Embed Size (px)
Citation preview

Total Market/2nd Tier Initiative
Phase 1
Research & Feasibility
April 2006

Study components
1.Baseline Studies – literature review and economic analysis
2.Dialogue with policymakers and stakeholders
3.Partnership Development4.Manufacturer Assessments
and regulatory review5. In country Market
Assessments and/or Business Plan development (for candidate markets)

3
15,5
00
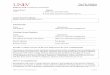
Morocco – basic family planning demographicsMorocco – basic family planning demographics‘000 women‘000 women
Source: Interviews with Moroccan Health Ministry 22-23 November 2005, Moroccan 2004 family planning survey; DHS
Other key facts:Historical CPR (any method): 1980: 19%1992:~40%2004: ~63%
Poverty% on <$1/day: 2.0%% on <$2/day 7.5%
63%
57%

4
Morocco – method mixMorocco – method mix% of married women 15-49% of married women 15-49
Source: DHS 2004 survey, Interviews with Moroccan Health Ministry 22-23 November 2005
63% % of married women 15-49
40.1% 2.1%5.4%
2.7%1.5%
3.0%8.0%
10.0%
27.0%
OCsIn
jecta
bles
IUDs
Condo
ms
Sterili
zatio
n
Other
mod
ern
Tradit
ional
Unmet
nee
d
No co
ntra
cept
ion –
free
choic
e

5
Morocco – method mix by urbanization/ wealthMorocco – method mix by urbanization/ wealth% of married women 15-49% of married women 15-49
*Including unmet need
Source: DHS 2004 survey, Interviews with Moroccan Health Ministry 22-23 November 2005
57% 53% 57% 51%
10%7%
13%7%
33% 40%30%
42%
Urban Rural Richest Poorest
None
Traditional
Modern
*

6
69%
15%11%
5%<1%
Low fertility Don't need/want
Healthconcerns
Religious/attitude
Lack of access
Morocco – reasons for non-use of contraceptivesMorocco – reasons for non-use of contraceptives% of married women 15-49 who do not use contraceptives% of married women 15-49 who do not use contraceptives
*Including lack of awareness/ knowledge (0.4%), too far/ difficult access (0.2%), too expensive (0.1%)
Source: DHS 2004 survey, Interviews with Moroccan Health Ministry 22-23 November 2005
*

7
Segmentation AnalysisSegmentation Analysis
Young Urbanites
Lower Middle
Poor
Tier/ Segment Description
Older Urbanites
Traditionals
Source: 1998 “Policy” segmentation analysis, interviews with Ministry of Health 22/11 2005
Proportion of married women 15-49
• Older, urban, wealthier, well educated, 80% <4 children, 65% think ideal # of children is 2 or less, all want to limit number of children
• 18% (1998 survey)
Urban Migrants
• Younger, urban, wealthier, well educated, 94% think ideal # of children is 4 or less, still want more children themselves
• 20% (1998 survey)
• Older, less wealthy, well educated, urban or rural, 40% with 7+ children, 80% wanted 4 children or less
• 30% (2005 estimate)
• Poorer, rural, in their 30’es, centre-south of country, 65% want 4 children or fewer
• 15% (2005 estimate)
• Rural, poor, no education, 45% have 7+ children, have never used contraception
• 7% (2005 estimate)
• Recent migrants to cities, “urban problems but rural attitudes”
• New segment, not included in 1998 survey
• ~10% (2005 estimate)

8
Older U
rban
ites
Youn
ger U
rban
ites
Lower
Midd
lePoo
r
Trad
itiona
ls
Urban
Migr
ants
Unmet Need
Traditional
Other Modern
OC
Segmentation AnalysisSegmentation Analysis % of married women 15-49% of married women 15-49
Source: 1998 “Policy” segmentation analysis, interviews with Ministry of Health 22/11 2005
?No
data

9
Market overview - MoroccoMarket overview - Morocco
[New Tier 2]
Social Marketing
NGO [IPPF/ AMPF]
Tier/ Segment Description Price/ cycle, USD
• TBD
• 2 products:– Microgynon– Minidril
• 5 products– Microgynon– Microlut– Exluton– Microval– Nordette
Private Sector
• 20+ products1
2
3
3
Government
• 3 products: – Microgynon– Minidril– Exluton
3
Cycles distributed p.a., m
$1.30++
TBD
$0.96
$0.54
Free
4.3
0
2.7
0.7
11.0
Pha
rmac
y di
strib
utio
n
Source: Morocco visit, interviews
Clin
ic d
istr
ibut
ion

10
Market overview HondurasMarket overview Honduras
[New Tier 2]
Social Marketing
NGO [IPPF/ ASHONPLAFA]
Tier/ Segment Description Price/ cycle, USD
• TBD
• 1 product:- La Perla
• 1 products– Lo Femenal
Private Sector
• 20+ products1
2
3
3
Government
• 1 product: – Lo Femenal
3
Cycles distributed p.a., m
$4.70++
TBD
$1
$0.30-$1
Free
0.8
0
0.3
0.9
0.7
Pha
rmac
y di
strib
utio
n
Source: Honduras visit, interviews
Clin
ic d
istr
ibut
ion

11
Key findings - HondurasKey findings - Honduras
Additional Tier 2 viability
• Tier 2 product exists in the form of ASHONPLAFA/IPPF La Perla BUT:– Only one product in this market segment and not favoured by doctors as
perceived as inferior quality– Opportunities exist to shift consumers from govt sector – Niche may exist between La Perla ($1) and Schering’s Microgynon (c.$5)– Tier 2 product with higher margins for ASHONPLAFA could allow them to
cross-subsidise rural programmes threatened by USAID budget cuts
Cost savings potential in free-to-market segment
• Potential exists for cheaper international bulk procurement– MoH would now like to focus on poorer/rural market segments (USAID pull-out and
economic hardship)– Government currently procuring via UNFPA – Potential exists for savings with generics, though perception of high quality should be
maintained– Dependence on Wyeth exists for lowest market segment (agreement restricts low-cost Lo-
Femenal for distribution only in govt, ASHONPLAFA clinics and outreach programmes)
General observations
• Currently 3 tiers of Honduran market are catered for and unmet need is estimated to be 7% BUT:– USAID contribution for commodities procurement diminishing by 25% per year until 2009– Secretaria de Salud still promising free commodities, but budget will be a challenge, and
new Liberal govt contains 2 Pro-Life MPs– Unmet need is mainly in the less accessible rural areas– Little product choice exists in the T2 segment– Injectables market share growing and 3 to 4 times more popular than OCs

12
No clear need for (additional) Tier 2
Tier 2 viability - summaryTier 2 viability - summary
Fully sustainable:• Self-funding (i.e. does not need donor funding), and•All key parties committed for long term (or easily replaceable)
Unsatisfactory availability:•Unaffordable product•Low quality product•Lack of access/ information•Lack of appropriate choice
Satisfactory availability:•Affordable product•Quality product•Good access/ information•Appropriate choice
Sustainability issues:• Not self-funding (i.e. needs substantial donor-funding) , or•Self-funding, but issues around longer term stability of self-funding arrangements
AVAILABILITY
SU
ST
AIN
AB
ILIT
Y
Urgent need for (additional) Tier 2
Urgent need for (additional) Tier 2
Future need for (additional) Tier 2
SatisfactoryUnsatisfactory
Hig
hLo
w
Peru
El Salvador
Morocco
Honduras
Jordan
Ukraine
Romania

Conclusions
•Business cases based on introduction into both free to client and T2 segments in smaller marketsBUT limited experience of simultaneous introduction•Significant interest in TM/T2 among governments facing sustainability challenges•No existing strategies for targeting free products to low income groups, and shifting wealthier clients•Limited experience in switching to generic brands (except Peru)•OCs widely available but key issue for TM/T2 is choice: increasing access to lower priced, newer products (BUT limited data)•Strong commercial competition likely•Potential IPPF MA management agencies, except in Jordan

Next Steps
1. Strengthen links with Govts and other procuring agencies; gather further intelligence and begin product registration, procurement procedures etc
2. Links with investors to identify financial start-up resources
3. Investigate business model for national management agencies, plus roles for advertising agencies, distributors; further develop selection procedures for management agencies
4. Research to understand the risks to CPR through brand substitution in the public sector
5. Investigate opportunities for promotion and brand communication to providers (especially medical professionals and pharmacists) and consumers (strategies depend on national regulation on direct to consumer product advertising)
6. Consumer research to better understand factors affecting consumer preferences, method and brand choices, and motivators to pay
7. Development of detailed costing to complete business and marketing plans

15
Specific objectives of sub-group
• To share information between agencies on companiesbeing used or identified for supply of RH products;
• to undertake a mapping exercise and qualitativeassessment of manufacturers of hormonal contraceptives in lower and middle income countries,using a common methodology.
• to identify a group of companies that could apply tobe prequalified by WHO.
• to develop to develop a common data base ofmanufacturers of contraceptives and other reproductivehealth commodities; and
• to identify gaps in knowledge and other activities to beundertaken.

16
Generic hormonal contraceptives
Mapping and initial assessment:• What manufacturers are found in which LMICs? • What products do they make and at what volumes?• What is their capacity, capability and
competence?• What would be needed to bring them up to
modern GMP?• What other capacity building would be required
before they could export product?

17
Generic hormonal contraceptives
Study 1. “Qualitative study” • Completed review of generic manufacturers of
hormonal contraceptives in: China, India, Indonesia,
Malaysia, Oman, South Africa, Taiwan, Thailand and Viet Nam.
• Review ongoing in: Argentina, Brazil, Chile,
Costa Rica, Mexico, and Uruguay.• Report to be completed by 31 July 2006.• Concept Foundation, Partners in Population and
Development, UNFPA.

18
Generic hormonal contraceptives
Study 2. “Quantitative study”• Assessment of the manufacturing competence of
five companies in China, India, Oman, Thailand
and South Africa.• Close link maintained between studies and
additional companies identified in Study 1 will be
assessed by 30 Sept 06. • Concept Foundation, IPPF/ICON, UNFPA

19
Conclusions
• Enormous capacity in China, India and Thailand.In China, most companies produce COCs over4-6 weeks, once receive government order. InThailand, except for one, most companiesmanufacture DMPA over 4-6 weeks/year.
• Although all factories visited have national GMP,there are still significant disparities and few would meet stringent GMP requirements.
Thailand has applied for PICS membership andwill apply PICS GMP in 2-3 years.

20
Conclusions
• Most companies are finding APIs from European sources to be expensive but that they cannot easily obtain material made to acceptable GMP nor with the necessary drug master files to allow completion of registration dossiers.
• Few companies have the capability of developing registration dossiers required for the export of products to countries with strict regulatory requirements.