Embed Size (px)
Citation preview

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
Dr Keith Holt
Types of replacement
There are many types of knee replacement available today, with most of these resembling each other very closely. With design coalition between manufacturers occurring, it is becoming clear that we have come close to stabilising a design, and that we are not searching for radical changes anymore. It suggests some consensus between all the companies who research and design these products. It also suggests that the product is quite good, and therefore, it is likely that future improvements will probably be small.
Total knee replacement - is the most common of the replacement operations, with partial replacements being less often used. This is not only because it is
more predictable in its outcome and survival, but also because most people have wear in more than one part of the knee, and hence need more than one part of the knee replacing. In this procedure, the worn out ends of the bone are replaced with metal, and a plastic tray is inserted between these to keep the friction low, and to absorb impact. The kneecap (patella) may also be re-lined with a plastic (or a metal and plastic) button.
A primary (first time) knee replacement is really just a resurfacing of each of the bone ends. How these surfaces interact with each other however, and how much ligament function is preserved, or is induced by the prosthetic design, is what ultimately makes the joint functional: and perhaps more like the normal knee. Over the last 50 years, many different designs have been tried. In the last few years, with prosthetic longevity becoming less of an issue, some design changes have been made to try and create more normal kinematics (the way the knee moves during use). What is becoming apparent, is that the nearer the kinematics approach those of the normal knee, the better the results seem to be; certainly in the short term, and hence perhaps, in the longer term.
Unfortunately, despite the above stated aim of modern designs, it does not mean that we can duplicate normal knee function yet; albeit that one or two designs are now very close to being able to do this. Because of some altered ligament function that occurs during insertion of a standard prosthesis (the ACL or anterior cruciate ligament is almost always lost, and the PCL or posterior cruciate ligament is often partly damaged), simulation of normal joint function does not really occur. There are however, prosthetic designs that now come very close to this ideal, either preserving these ligaments, or substituting for them. Whilst PCL function has long been able to be replicated by a prosthesis (a PS or posterior stabilised design), ACL function has not. Some more
TOTAL KNEE REPLACEMENTTechnical aspecTs - The WhaT, hoW, & Why
navigaTed and RoboTic suRgeRy included
Total Knee ReplacementA traditional resurfacing design on which all modern
designs are based.
Femoral Component
Polyethylene Tibial Component
Knee Replacement is a demanding procedure that requires a good working knowledge of knee kinematics, combined with experience. Optimal results require prostheses that mimic normal kinematics as close as possible: but also, implantation in good alignment, with acceptable ligamentous tension and balance. This is not an easy task as the knee is far from being just a hinge. It's motion is very much 3 dimensional.
This brochure contains technical information for those that are interested. It explains in some detail how the surgery is done, what sort of replacements are available and for what purpose, and why current replacement still only has 80-85% satisfaction rates in all joint registries. It is not intended to be read as a whole. Rather, you should select the portions that you think are relevant and read those first.
Tibial Tray

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
recent designs however, have been able to provide some ACL function. Such function then allows more normal kinematics to be replicated without the potential problem of instability that would occur in a design that was built to the exact same shape as a normal knee but was ACL deficient. As yet unfortunately, some of these more recent designs are not available in Australia.
Knee replacement - the procedure
The best surgery is carried out using computer navigation to optimize alignment correction. This involves putting 2 pins in the femur (usually within the incision), and 2 pins in the tibia (usually through separate holes). On each pair of pins is placed a tracking array which can be followed by a camera. By moving the thigh around, the centre of rotation of the hip can then be worked out, usually to within 2mm. Once this is done, the knee and ankle are plotted out with a pointing tool that also contains a tracking array. Using this information, the position of the individual bones, and the leg as a whole, can be worked out and depicted on a computer monitor, providing a 3D model of the knee, including a model of the femur and the tibia. This can then be used for the surgery.
Computer Screen showing alignment during computer
navigation
Positioning the cutting jigThe cutting jig (being held) is moved to a position
which corresponds to both the amount of bone resection required and to the correct alignment - i.e. degree of varus/valgus and slope. This is then
pinned, and the bonethen cut with a saw through the guide slot.
Computer Navigation at work Note infrared beams are generated and reflected off
the balls and back to the camera. This then sends information to the computer to determine both the
position and the alignment of the bones.
Determining the hip centreBy moving the femur around, the system will
determine the centre of rotation, that being the hip centre. This is usually accurate to within 2mm.
In addition to the above, the cutting guides that are used can also have arrays placed on them, thus allowing them to be tracked simultaneously with the bones. This information then allows the cutting guides (seen in real time on the animation) to be moved, and to be accurately pinned to the bones ready to make the cuts for the prosthesis. This process is, theoretically, degree and millimetre accurate, and is done by following the distances and angles that are displayed on the screen (all calculated by the computer). By doing this, the desired amount of bone to be resected, and the desired angle at which a cut is to be made (in both planes), can be determined.
At the end of the procedure, the computer will also tell us what the final alignment of the leg is: something that can be fine tuned during the cementation of the prosthesis by varying the thickness of the cement.

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
Mechanical versus Kinematic Alignment
Ideal alignment used to be thought of as a straight leg, with the tibial component being at 90º to the tibial axis, and therefore, parallel to the floor. This is known as Mechanical Alignment, and is depicted in the diagram on the right. The problem with this is that most people do not grow up with perfectly straight legs. Indeed, the majority are slightly varus (bow legged), but with a good number being valgus (knock kneed): and of course, there is a whole range in between.
Pre-
oper
ativ
e al
ignm
ent v
iew
Post
-ope
rativ
e al
ignm
ent v
iew
A li
ne fr
om th
e ce
ntre
of t
he h
ip sh
ould
pas
s th
roug
h th
e ce
ntre
of t
he k
nee
and
the
ankl
e
Mecahnical AlignmentRe-alignment from a varus (bow-legged) knee to a
straight knee.
If significant mal-alignment is corrected to re-establish the mechanical axis, which is what the prostheses were originally designed for, then in some instances the ligaments on one or other side of the knee will be too tight, and may therefore require some sort of release. The problem here, is that the leg is trying to be brought into an alignment that it has never been in: and whilst we know that 'Mechanical Alignment' provides good wear characteristics, it does not always provide the best function, or the best pain relief.
With the above in mind, and with the availability of computer technology to evaluate 3D CT scans of the knee, some companies have been trying to work out where the native axes of rotation of an individual's knee really is, thereby leading to computer derived cutting jigs which can be used to insert the prosthesis more anatomically. That is, to try and reproduce the leg alignment, and the axes of rotation, that existed prior to the arthritis and before any subsequent deformity set in. The end result of this is called 'Kinematic Alignment'.
The results of kinematically aligned knees have been mostly good, and in many cases excellent: but it has also produced some significant outliers - patients with knees that end up well outside the 0º - 3º varus range that is thought to provide the best compromise
Kinematic AlignmentNote that the joint line is not at right angles to the tibia, nor is it parallel to the floor. This has been
made to replicate the normal opposite knee.Most prostheses are not designed for this style of alignment, and using them like this can change patella tracking, and hence, may lead to other
problems.
Hip-Knee-Ankle AngleIn the normal population, the average is to be slightly bow legged: males being near 2º and
females nearer 1º
More varus(bow-legged)
More valgus(knock-kneed)
between function and cosmesis, but still with optimal wear characteristics of the prosthesis. Accordingly, current thought is that the knee should be somewhere within that range if possible, whilst still trying to make the knee well balanced with minimal releasing of any ligamentous structures. Clearly however, there are legs where the deformity is so great that some releases will need to be performed in order to get them close to this ideal range, and not every knee will be able to be corrected that far. If that is found to be the case, then a best compromise may be undertaken whereby the problems of releases are balanced against what is sometimes a slightly sub-optimal cosmetic result (e.g. a residual valgus or knock kneed deformity).
Males and females combined

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
Achieving balance
The above talks about correcting the leg alignment to provide optimal varus or valgus for function, and optimal wear characteristics: that is, a discussion of the leg alignment when the knee is straight. What it does not discuss, is the ligament tension balance through the flexion range (during knee bend). This is determined by the rotation of the prosthetic femoral component on the femur, and is achieved by attempting to make the flexion surface of the prosthesis parallel to the hinge line of the collateral ligaments. Mostly, this is still done by using the points of attachment of the collateral ligaments to the femur, the so-called femoral epicondylar axis. Hence, it is like getting a swing to be parallel to the ground by making the axis, the hinge point for the top of the ropes, parallel to the ground. The problem however, is that the points of attachment of the ligaments can sometimes be difficult to determine.
Right Knee - flexed 90º(Femur seen end on)
One of the ways of getting the rotation of the femoral component correct is to cut the flexed femur parallel to the Transverse Epicondylar
Axis (TEA). This should make the tension of the collateral ligaments equal given that they attach to
the epicondyles.Note that in a normal knee the joint is sloped (usually about 3º) because the lateral condyle is smaller than the medial. Standard prosthesis
however have the same radius of curvature on each side, so the joint has to be cut parallel to the TEA.
Trans EpicondylarAxis
Femoral Cut
Tibial Cut
LateralFemoralEpicondyle
MedialFemoral
Epicondyle
Lateral condyle
Medial condyle
Joint line
A - shows the knee flexed to 90º after cuts have been made as per the diagram on previous pageB - shows the cuts with the knee straight
If the knee is balanced the gap should be the same throughout the 0º - 90º range of motion.
Lateral Collateral Ligament
Medial Collateral Ligament
Knee flexed to 90ºView of the end of the
bone
Knee straightView of the front of
the bone
TibiaTibia
The latest generation computer navigation systems can define what is known as the ‘knee envelope’. That is, the range of alignments and balances that the knee can be put through without lengthening or releasing any of the collateral ligamentous structures. This can now be done through a nearly full range of knee motion; for the first time determining balance, not only in extension (with the knee straight), but also in flexion (with the knee bent).
Theoretically, the latest generation of computer navigation systems should allow optimal placement of a prosthesis, in accordance with a plan that is based on alignment and ligament tension information defined by taking the knee through its motions, with the navigation system in place, before the actual surgery begins . The problem however, is that such a plan can sometimes require alteration after the bone cuts are made. This is because, in the process of cutting out the worn out parts of the bones, some ligaments (usually the MCL and/or PCL) may be partly released or freed up, thus changing the balance of the knee. Hence, the original plan may need to be adjusted after the bones have been cut and trialling of the prosthesis has occurred.
The limiting factor in earlier navigation systems has been the difficulty of defining the Epicondylar Axis (TEA), and knowing that it does not always represent the isometric point of the collateral ligaments. To plan the alignment based purely on balance, without defining the TEA, requires the newer alignment systems as described above, and on screen modeling. Such alignment systems form the basis for robotically assisted surgery.
The skill of replacement is to insert the prosthesis such that it has the right tension (not too loose and not too tight), both with the knee in full extension (straight), and throughout the flexion range - yet being able to keep it within an acceptable alignment range [not too varus (bow legged), and preferably not valgus (knock kneed)].
Flexion Gap Extension Gap
Balancing the Knee in FlexionWith the femur bent at 90º, the back of the femoral
condyles are cut parallel to the axis of rotation. When the femoral component is inserted, this should lead to a knee where the collateral ligaments are of equal length, and hence equal tension in flexion.
Axis

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
Robotic Knee Surgery
Robotic surgery is now starting to be available. What this offers is a sophisticated navigation system to plan the placement of the prostheses, and to balance the ligaments. The robots themselves (at least the ones currently licensed for use in Australia) do not actually do any of the cutting of the bone, hence perhaps, it is a bit of a misnomer to call the process ‘Robotic Surgery’. Nevertheless, these systems do incorporate safeguards so that they prevent operation outside the designated limits of the surgery area.
The medial condyle ready for surgery to begin for a partial
replacementThe burr is used to remove all the coloured layers.
Each layer represents 1m of thickness.
The medial condyle - burring nearly finished
Once all the coloured area has been removed, the two pilot holes for the prosthetic stems are made.
The Finished Hemi-ArthroplastyThe tibia is cut similar to the femur. The prostheses
are then cemented in as shown.
Medial Condyle
The Navio burr is controlled by the computer using the navigation array
that is attached to it. The burr will retract into it's sheath, or will stop rotating, if it is used outside the planned area.
This sort of 'Robot' is currently classified as a 'Passive Robot', whereas an 'Active Robot' is classified as one that actually carries out some of the work. Such a classification has been created in order to use the word 'Robot' for activities that actually do not come under the definition of the term 'Robot'. This is of course is somewhat false advertising!
For partial knee replacement (hemi-arthroplasty), or patello-femoral joint replacement, these being the operations where it is hardest to get the component positioning right (and more so than in total knee replacement), robotically navigated surgery can be helpful to accurately define the area that needs to be burred out for the implant. It does this by modeling the knee on the computer, based on data that is input at the time of surgery (and sometimes from 3D CT scans).
As it also knows where the tip of the burr is, the system can allow the surgery to be performed on screen where it demarcates the area to be burred by colouring it in. The coloured area is actually layers of colour, each colour representing a 1mm thick layer. Essentially, each colour is then successively removed until the underlying white of the bone, representing the bottom of the resection area, is exposed. (Note however, that different systems do this in different ways.)
In addition to defining the area to be burred, the computer can actually restrict what bone is removed. It does this by turning off, or retracting, the burr (or saw) when it is outside the coloured area. As such, it prevents excessive removal of bone, leaving a well defined area on which to sit and cement the prosthesis.
For total knee replacement, whilst this can be done in a similar manner, it is currently too slow to be useful in that format. The volume of bone to be removed is too much for a burr to do alone, and thus it would take too long to make this a viable method of bony resection. For a total knee replacement therefore, the plan is different. Here, the aim is to use standard type cutting blocks

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
that will allow the use of a saw; this being much faster, and almost as accurate, as using a burr throughout. The upgraded navigation system that comes with the robot allows the positioning of some tapered holes, which then accept the blocks similar to those shown below. Once in place, the position is checked with the system, fine adjustments are made (to within 1mm and 1º of angulation), and further pins are inserted to definitively fix the block ready for the bone cuts to be made. The femur is cut first, and then the tibia.
The cutting block locks into the holes
The block position is then finely adjusted using the navigation tools, and then pinned into place ready
for the saw to be used.
Creating the tapered holes for the cutting block
There are two at the top of the bone and two at the end. These are defined and then burred out.
The reason to consider using the robotic system is not just to determine the position of the components on each bone (something that can be done well with standard computer navigation that we have been using for nearly 10 years), but to try and define the balance of the components on each other throughout the range of motion. Essentially, the aim is to have ligamentous tension that is roughly equal throughout the range of motion, being neither too tight, nor too loose, at any
one point of the flexion arc. So what the system does is to define what is referred to as the ligamentous envelope of the knee. By taking the knee through a range of motion when stressed into valgus (knock knee angulation with the medial collateral ligament tightly resisting) and then into varus (bow legged angulation with the lateral collateral ligament tightly resisting) the natural length and tension of each ligament can be determined for all angles of motion from full extension to over 100º of flexion.
Defining the Knee EnvelopeThe knee is taken through a range of motion
stressing it into both varus and valgus. This creates an envelope of laxity of the collateral ligaments.
Orange is varus (MCL) and purple is valgus (LCL). What is created is a view of the knee throughout
the motion range. This then allows a plan based on what alignment might work without making those
ligaments too tight or too loose.
Once the envelope has been established, the computer can overlay the prosthesis with best size and fit algorithms, and then display them on screen as it expects the knee to look after completion. Each individual prosthetic component is then manipulated on the model, altering the size of components, angles of bone cuts, position of bone cuts, and whatever else seems necessary, until an acceptable balance is achieved throughout the range of motion.
If the above procedure is carried out as described, implanting the prosthesis just based on balancing the ligaments, then what you end up with is kinematic alignment. The knee ends up being balanced, but no specific account of overall alignment (varus or valgus) is taken. Essentially, this methodology just restores the knee alignment back to where it was before the arthritis set in. For most people this is a reasonable position, and the average knee angle for normal knees is 1-2º varus.

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
That is, slightly bow legged. There is however, quite a range of 'normal', and there are concerns with leaving the alignment outside a certain range - one of the so called 'Outliers' that we have tried to avoid producing over the last few decades.
From most surgeons perspective, excessive valgus (knock knee deformity) is seen as cosmetically
Adjusting the component positionThis picture shows the femoral component position
in relation to the mapped out surfaces of the original bone (yellow areas). It shows alignment, rotation and so on. The prosthesis can be moved
in every direction to improve the position by using the controls (+/-/>..). The tibial component is then
adjusted the same way.
Adjusting the component positionThe graph at the bottom of the picture shows the
final gaps on each side of the knee for each degree of motion. With this information, adjustments can be made to component positioning to ensure that
the knee goes through to full extension, and that it is neither too tight, nor too loose, at any point in the
range.
VarusStraight Valgus
Normal variations in leg alignmentNote that: restoring normal ligamentous balance
(Kinetic Alignment) will restore this native alignment. It will not correct or adjust it.
unacceptable: and also, it can lead to a compromised gate because the knees can rub against each other during walking. Excessive varus (bow legged deformity) on the other hand, is less noticeable: but, if it exceeds 3º or 4º it may lead to premature prosthetic wear because it over stresses the medial (inside) half of the tibial polyethylene tray.
When adjusting the position of the prostheses on the model therefore, it is not just as simple as balancing the gaps throughout the flexion range. One also has to take into account the overall leg alignment to try and keep the majority of knees with in an optimal range of say 0º - 3º varus. Because there is some laxity in the ligaments, and because a millimeter or two gap is normal, there is some room for this adjustment. Hence, for example, if the knee has a range of laxity encompassing 2º varus to 7º varus when the knee is in near full extension (fully straight) before surgery, then the ideal final alignment to be aimed for may be in the range of 2º and 3º varus. On the other hand, if the knee cannot be brought into the acceptable range, being out by a degree or more, then some sort of ligamentous release may have to be done to achieve that final aim. Where possible however, current thinking is that we should consider less releases than previously, even if they are only partial releases: and this is achievable because we no longer go for a mechanical alignment of 0º varus / valgus with every knee.

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
Why consider robotically aided surgery for Total Knee Replacement?
The overall satisfaction rate for Total Knee Replacement, in almost every registry in the world, is only about 80-85% good to excellent. The remainder are less happy with their new knee, and often for reasons that are hard to define. The advent of computer navigation to improve alignment was thought to be the harbinger of better results, but that did not happen. Results in the Australian National Joint Registry are showing some early benefits of this, but the improvement is small and perhaps not statistically significant. (On the other hand, there is some early evidence of improvement in the results for hemi-arthroplasty.)
Changing away from mechanical alignment to more natural alignment ('Kinematic Alignment' as discussed above), is thought to be bringing better results, but it is still too early to know that. To now move to a system of Modified Kinematic Alignment, taking into account ligament tension balance throughout the range of motion is logical, but the evidence for it will be some years away; and perhaps 10 or more years away. Nevertheless, we think that the slightly increased accuracy over standard computer navigation, plus the ability to better plan component position before the bones are cut, will lead to better results. If so, then the additional cost of these techniques may become justified. Certainly, as Robotic systems become more user friendly, more helpful, and cheaper, we expect them to become the instrument of choice for this sort of procedure.
The 'Navio' Orthopaedic RobotThis one, designed by Blue Belt Technologies, and now owned by Smith & Nephew, comes with the
upgraded Navio computer alignment system. This is optimised for implantation of S & N prostheses.
The final AssessmentThe graphs here represent the end result of a knee plan. What it shows is the gaps on each side of the knee during a range of motion from 0º through to
about 120º. You will see here that the final planned alignment, based on balancing those gaps, is 8º
varus (that is: quite bowed). Some may accept that as being just 'Kinematic Alignment', but it probably
means that the Medial Collateral Ligament is too tight, so a release should probably be made to get
the knee into a less varus position ( say 2-3º).
More advanced robotic systems are already on trial. Some of these have the robot doing all the cutting of the bone based on a plan designed along the same lines as the current systems, but still with the surgeon adjusting and approving the plan before any cuts are made. There are various reasons why this sort of system will be not only more accurate (it doesn't need to use pins and cutting blocks for one thing), but also quicker. It is likely therefore, that these systems will eventually become used, albeit that they will require legislative change to allow this.
For now, all such machines require the surgeon to be in control throughout the procedure. In time however, as the machines get better, it is likely that they will be approved to actually do the bone cuts based on the surgically approved plan. This means that the knee will be exposed, the bone ends mapped out for the navigation system to recognise, and then the robot will make all the cuts. Components will then be placed in the knee by the surgeon and the alignment and balance checked to see if it matches that plan. Any adjustments required can then be made. Such robots (e.g. Rosa) have now been approved for trial in the USA, and it is expected that approval for this in Australia is not far away.

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
Robots with surgical arms (Rosa)This robot is part of the newer series of robots in development. These have arms that can not
only be controlled, but can actually carry out the surgery based on the same navigation systems that are described above. It is likely that these will be
approved for use in the not too distant future.
Further into the future, we think that navigation systems will not require pins to be put into the bones to hold the navigation arrays. Indeed, there are systems under development which have implantable devices that are very small but very accurate. These merely need to be placed into the bone and can stay there to provide information on wear and other parameters for the life of the prosthesis. Also, instead of hand mapping the ends of the bone to register that information onto the computer, there are cameras and laser devices which will do all this in seconds rather than minutes, and will be more accurate. Over the next 5 years therefore, it is expected that there will be quite a lot of changes which will make this sort of procedure more accurate and quicker, and hopefully this will lead to better satisfaction rates in the registries.
Evidence for Ligament balancing
Whilst the evidence for ligament balancing, and for 'Kinematic Alignment' and it's variations, is only just reaching the Australian National Joint Registry, there is some literature to support some of these changes.
We know that ever improving the accuracy of 'Mechanical Alignment', moving from alignment based on rods placed down the shafts of the femur and tibia, and advancing through various forms of computer based alignment, has not improved the results of the procedure. On the other hand, using that same alignment, but balancing the ligament tension, has shown early promise of improving results. Releases can now be done more selectively, and by degrees rather than all or nothing: and the pressures in each compartment can be measured throughout the full
range of motion.
The above can be done in a controlled fashion by using special pressure sensing trial prostheses which are inserted instead of the polyethylene components and, when in situ, give live pressure readings for both sides of the knee. The readings are sent to a monitor and can be used to progressively change alignment, or alter ligament tension by doing selective releases, until the correct balance is achieved.
A Verasens pressure sensorThese come in different sizes and can be put into the
knee instead of the tibial plyethylene component. These relay pressure information from both the
medial and the lateral sides. Pressures can be taken continuously throughout the whole range of motion.
A Verasens pressure readoutThe numbers shown refer to the pressures at a
given point of the flexion arc of the knee. The green spots locate the point from which the pressures are
measured. Linking these points provides an axis of contact and this can be measured against the
rotation of the component, thus conveying rotational information that may indicate a need for change.
Once the required balance has been obtained, the sensors can be removed and the real components can be inserted. This method of controlled adjustment is not routinely done, but is very helpful when learning to balance a knee. With the advent of the newer technologies however, including robotically assisted surgery with current generation alignment systems, this sort of technology should no longer be necessary. It's importance though, should still be recognised. It proved that ligament balance was crucial to success.

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
Patello-Femoral considerations
The patello-femoral joint has not yet been mentioned, but is a major cause of problems following total knee replacement. Indeed, it may actually be the largest cause of problems following this sort of surgery. The reason for this is that the current replacement types that are available in this country do not actually work like a normal knee. The ones that are available, mostly work more like a hinge than a normal knee, and the difference is important.
In the normal knee, the femur rotates externally (turns outwards) about 15º as it bends.
Femoral external rotation with flexion
This shows that as the knee is flexed (bent), the femur rotates about 15º with respect to the tibia.
Some of this actually occurs in the tibia because the act of pushing the foot up (dorsi-flexion) causes this bone to internally rotate. The cause of this effect is the crooked hinge phenomenon made by the sub-talar joint (the joint just below the ankle joint).
With flexion, the lateral condyle moves right off the back of the tibia
This then allows the femur to rotate externally (outwards)
Lateral Tibia
Lateral Femur
MRI of a normal knee
The crooked ankle effectAs the ankle is flexed the foot turns out. The
corollary of this is that, during squatting, when the foot is fixed to the ground, the tibia rotates inwards.
T h e e x t e n s o r mechanism consists of the quadriceps muscle and tendon, the patella, and the patella tendon. All the force of the quads muscle is directed through the patel la tendon and into the tibia via its attachment to that bone, the tibial tubercle.
The patella pushes the tendon away from the joint, thus providing leverage. The patella is 'V' shaped in cross section and, by being situated in the trochlear groove of the femur,
For this to occur in a normal knee, a number of design features must be present so that the following happens:
1. The tibia must internally rotate (turn in towards the opposite tibia) during the flexion. This is an effect that occurs at the ankle when the ankle is also bent during squatting and lunging type activities. It is due to the fact that the ankle joint complex is
crooked. That is, it is not aligned perpendicular to the direction of motion.
2. When the tibia rotates inwards, the lateral femoral condyle slides right back, indeed right over the back of the lateral tibia, such that the femur can then rotate externally (to face outwards from the centre of the body). This then changes the orientation of the trochlear groove such that it is more laterally placed (externally rotated) with increasing flexion.
which is a matching 'V' shape, stability is provided. Every normal extensor mechanism pulls through a small angle (the 'Q' angle - see below) with the knee straight, but this lessens with flexion as the tibia internally rotates and the femur externally rotates.
The change in the tibia whereby the tibial tubercle moves medially (towards the mid-line of the body), accompanied by the opposite (external – that is away from the mid-line) rotation of the femur (moving the attached quads muscles, and hence their line of action, more laterally), is such that, in the normal knee, the 'Q' angle essentially becomes abolished (0°) when the knee is flexed 20° to 30°. This then means that the
Qu
ad
ric
eps
Patella Tendon
Patella
Quads Tendon
Tibial Tubercle
The Extensor Mechanism

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
The 'Q' angle and Knee FlexionThe quadriceps force exerted during knee flexion
pushes the patella laterally because of the 'Q' angle. This forces the femur to externally rotate until the
angle is 0º and the lateral force is neutralised.
The patella is pushed laterally
because of the 'Q' angle between the
patella tendon and the quads
tendon
Patella tendon
Patella
Quads tendon
The medial side of the
knee acts just like a ball and socket during
knee flexion. It does not move
posteriorly
The lateral side of the
knee moves posteriorly as
the knee flexes
Lateral Medial
The femur externally
rotates to follow the patella until
the sideways force is gone
Q
The 'Q' angleThis is the angle that the quadriceps force pulls on the patella subtended on the patella tendon below. It causes a laterally directed force that pushes the patella sideways and loads up the lateral patella
groove (trochlear) on the femur. This in turn causes the femur to externally rotate as the knee bends and
the force increases.
Lateral force made by the
Q angle as the quadriceps
contract Q
Area of high pressure
as force is applied during
squatting
LateralTrochlear
Patella
patella tracks centrally without excessive force laterally, and hence without excessive pressure under the lateral side of the patella.
If during squatting, the patella is pushed laterally by the quadriceps force acting via the 'Q' angle, and this is not compensated for by tibial internal, and femoral external, rotation, then excessive forces can be generated under
the lateral facet of the patella. Knee replacements with standard 'hinge like' mechanics that do not compensate for this angle, can therefore be painful because of the repetitive shear forces that occur across the patella in flexion. These forces act upon the patella but are resisted by the patella being in the trochlear groove. If the patella has not been resurfaced, then it experiences high pressure under the lateral facet. If it has been resurfaced, then the resurfacing button is held in the trochlear and the patella is pushed laterally, thereby causing a shear stress at the interface of the patella and the resurfacing button. For this reason, bone scans looking at underlying bone stress, are often positive in the patella area in a painful Total Knee Replacement.
A standard Knee ReplacementUp until recently, all knee replacements acted like a hinge, not rotating as the knee goes into flexion. To cope with this, the trochlear groove is often made
crooked, an improvement on the older designs. This however, is not the same as the normal knee where the femur (and trochlear) rotate to keep in line with
the patella: thus decreasing shear forces.
'Q' angle pushes patella across
Shear forces created between the patella
and the implant
Right Knee flexed 90º
A Bi-Cruciate Stabilised Knee in flexion
Bi-cruciate function lets this knee function more like the normal one and hence it rotates in flexion.
The trochlear moves with the patella, thus
decreasing shear forces
The Trochlear has not rotated to meet the
patella
Femoral Component
Femur

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
Movement of the lateral femoral condyle
In order for the lateral femoral condyle to slide posteriorly, and then to slide right over the back of the lateral tibial plateau allowing it to externally rotate (turn outwards), a number of design features need to coexist: and most of these are difficult to replicate in a prosthetic joint without introducing instability that would normally be controlled by the anterior and posterior cruciate ligaments of the knee.
The Anterior Cruciate LigamentThis goes from the central tibia to attach to the
inside of the lateral femoral condyle. It thus prevents the condyle slipping completely off the back of the
lateral tibial plateau during flexion, and pulls it back as the knee is straightened again.
Left femur cut down
the middle
ACL
Inside of LFC
Central Tibia
These features are as follows:
1. The femoral condyle on the lateral side has to be smaller than the medial - with a slightly smaller radius of curvature.
2. As a consequence, the lateral joint line is usually 3mm above that on the medial side (i.e. the joint line is sloped - hence when you stand on 1 leg and balance, the leg may not be at right angles to the ground but the joint line is parallel to it. This happens in normal walking, and keeps the forces across the joint more nearly at right angles to it, which is better for force distribution. It also decreases shear forces that may occur with a sloping joint line).
3. The backward slope of the lateral joint line will be more than the medial, thus allowing the lateral condyle to slide off the back of the lateral tibia as the tibia internally rotates. This does not occur on the medial side where the femur stays centred in its
Looking down on the top of the tibiaThis diagram shows how each of the femoral
condyles move during flexion. Note that the Medial Femoral Condyle (MFC) just pivots around a fixed
point like a ball and socket whereas the Lateral Femoral Condyle (LFC) moves posteriorly. By
plotting those points, the axis of rotation is marked out and this can be seen gradually externally rotating
with flexion, thus neutralising the 'Q' angle - and hence decreasing shear forces on the patella.
MFC LFC
Axis of rotation
Knee Flexion Angle
Right Tibia
socket and does not exhibit any roll back. Indeed, the medial side of the knee behaves much like a ball and socket joint with the socket being made up of not only the tibial bone which is concave on that side, but by a stable meniscus which does not move back in flexion like the lateral one: and hence the meniscus deepens the socket for the medial femoral condyle.
4. The lateral tibial surface is flat/convex, not concave, so that as the knee bends, the lateral condyle can slide posteriorly down the slope. Because of that slope, the lateral ligament becomes looser as the lateral condyle moves posteriorly and, in turn, that looseness allows it to move even more posteriorly.
The driving force for this is the pressure under the lateral patella caused by the quadriceps pulling obliquely via the 'Q' angle. This pushes on the lateral side of the trochlear, hence pushing the femur into external rotation. As a consequence, the femur rotates, allowing the patella to go with it. When the knee reaches about 20º of flexion, the 'Q' angle then becomes neutralised such that it no longer acts to provide an external rotation force. This also means that there is no longer a shear force acting on the patella, all forces then being directly across the patello-femoral joint.
Anterior Cruciate Ligament (ACL) Function
To allow for this much freedom of movement of the lateral femoral condyle on the lateral tibia, there must be some ACL (Anterior Cruciate Ligament) function to provide some control to this so that the knee is not unstable in rotation. The ACL holds the lateral femoral condyle (LFC) to the anterior tibia and prevents the femur from just sliding in an uncontrolled fashion off the back of the lateral tibia as the knee flexes. It also acts to rotate the femur back to a stable, internally rotated position, as it extends (the screw-home mechanism).

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
The bottom line and the role of the prosthesis
The importance of all of the above is that, as the knee bends, the patella becomes much more in line with the trochlear groove and hence is not pushing it sideways. This then decreases any shearing force on the patella itself as the knee bends: and given that squatting can invoke a patello-femoral contact force of about 7 - 8 times body weight (say 500kg in a 70kg man), a force that progressively increases from standing through to full flexion, it is important to remove the associated shear force from early on in the flexion manoeuvre so as to decrease the risk of patella pain.
If the above could be achieved in knee replacement design, then some feel that this would eliminate, or at least greatly reduce, the patella problems that we still see. Hence, when associated with modern robotic techniques, such a prosthetic change may further reduce the dissatisfaction rate that currently exists. Of course this remains to be proven, but bi-cruciate stabilised knees, those with both ACL and PCL function, do exist (The Journey 11 BCS Knee or Bi-Cruciate Stabilised); and the number that have been implanted is now quite high. Although not available in this country due to regulation issues, we are starting to see encouraging outcome data from other international centres. Further information on this, and other prosthetic types, is described below.
In addition there are now some prostheses that actually preserve the cruciate ligaments. Of course these ligaments cannot be contracted or damaged to use this sort of knee, which means that such a knee is not suitable for use in very bad arthritis, but these are being implanted at research centres to see if the results are good enough to move towards general world wide release.
The next level down in terms of kinematics, is a knee that pivots on the medial side. These do not have ACL function but at least have the pivot in the right place. These knees tend to be unconstrained on the lateral side, which means that the patella can push the femur into some external rotation: hence, they may have better patello-femoral function than standard knees. This function however, is deliberately limited by the design in order to avoid creating instability.
Issues of size
The prosthesis is sized during the procedure. Each component comes in multiple sizes, all of which are available for every case. On the femoral side, depending on the make of the prosthesis, there may also be available both a standard width, and a narrow width, component for any given size. These have been available for a few years now, recognising that most females haver a narrower knee for the same depth than males. Indeed, over 90% of females will end up best suited to a narrow component (It is to be noted that some makes now only supply narrow components, but
usually in a larger range of sizes).
In addition to variations on the femoral and tibial component sizes, the polyethylene tibial tray which locks into the tibial component, comes is multiple thicknesses for any given size; there usually being a range from 9mm through to 25mm. This then allows a good deal of adjustment for any bone loss which might otherwise leave a large gap to be filled between the cut bone ends.
The longevity of a knee replacement
For most available prostheses, a 90% - 95% survivorship at 15 years is expected (as the results from the Australian National Joint Registry show). This means that most replacements will be functioning well at 15 years, and that some will go to 25 years or more before requiring revision. As expected, the analysis of results show that the heavier more active patients will wear out their knees earlier: and hence, the older, lighter and more sedentary patients are more likely to be in the 90% group that will go past 15 - 20 years.
Some of the current models are now tested out past 30 years (based on average use) in the laboratory, but only time will tell if these newer knees will really last that long.
The (theoretical) improvement in longevity over the prostheses that were implanted 20 years ago is due to several factors:
1. Component design has improved based on our ever increasing knowledge of how a normal knee functions, and based on the long term results of older designs.
2. The standard, highly polished, Chrome Cobalt (medical grade stainless steel if you like) femoral components can be made smoother by various ionic blasting techniques which fill in microscopic pores in the chrome cobalt surface. Instead of the more traditional polished chrome cobalt prosthesis, alternative metals can be used. Of these, Zirconium is now the leading contender, having been on the market for a decade or more. This is more expensive, and more difficult to produce, but the bearing surface can be subjected to a plasma spray that oxidizes the surface to Zirconium Oxide (patented as Oxinium). This ceramic surface is not only significantly smoother than the underlying metal surface can be made, it is also very much harder and less easily scratched. The Oxinium surface is not a coating, but rather a 5 micron layer on the surface of the component: hence, it is part of the component metal and does not need to be bonded to it. Compared to a Chrome Cobalt Femoral component, the Oxinium coated component has been shown

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
to be twice as hard and 49 times more abrasion resistant. This latter may be important if there are any minor (sometimes microscopic) bone or cement fragments remaining in the knee; something that may be reasonably common given how hard it is to wash out and remove all of these tiny fragments. As an added benefit, a zirconium component does not contain any nickel, that being a metal that some people react to. It also does not contain either cobalt or chrome, both ions of which can cause problems in a worn out Chrome Cobalt joint where metal on metal wear creates fine metal particles which can be absorbed. Although very rare in knee replacement, such absorption can cause 'heavy metal' toxicity.
3. The polyethylene tibial tray is harder and less subject to wear. This has been achieved by 'highly cross linking' the polyethylene molecules. The polyethylene is composed of very long monomers (single molecular chains) that are fused together to create a polymer. Those molecules then line up with the direction of stress in the component which, because the knee moves hinge like in line with the direction of walking, means that they line up with the direction of motion (i.e. front to back). By doing this, it allows some splitting of the molecules under extreme loads. By fusing these together, side to side, the plastic is made stronger. In addition it is made harder which, if done cautiously, does not harm its intrinsic strength. If made too hard however, it may become brittle, so the radiation dose used for this process has to be very carefully measured.
4. Vitamin E, an anti-oxidant, can also be added to the polyethylene tray. It is a difficult process to get this into the plastic, but it decreases oxidative degradation of the plastic over time. Some companies can supply polyethylene components that have been treated like this and, in the laboratory, these seem to have better wear characteristics.
The Australian National Joint Replacement Registry goes back over 15 years. Most data therefore relates to Chrome Cobalt and early polyethylene technology. Results from newer technologies are only just beginning to show up but, over the next 20 years, based on laboratory testing, better performance is anticipated.
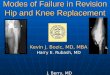
UKR Revision - rate by patient ageNote that Uni-Compartment Knee Replacement
(hemi-arthroplasty) has a higher revision rate compared to TKR. Again, the younger, heavier and
fitter your are, the sooner the knee wears out or fails. More use = faster wear.
TKR Revision - rate by patient ageThese graphs demonstrate that the younger, heavier and fitter your are, the sooner the knee wears out or
fails. More use = faster wear.
TKR Revision - rate by causeThis graph shows the reasons for failure of a Knee Replacement necessitating a revision in males. For
females it is similar except for a lower infection rate early on.
ANJRR 2017
ANJRR 2017
ANJRR 2017

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
to work to a variable degree. The best ingrowth surface is tantalum, and this can be made to have the same sort of structure as normal bone. This structure, with lots of small cavernous defects in it, is known as trabecular metal. When first introduced for the tibial component, it came bonded to the polyethylene. The advantage of this was that, in that configuration, it had the same stress/strain characteristics as normal bone. Ingrowth was excellent, loosening was never seen, and because stresses were distributed to the tibia physiologically, there were no areas of high or low stress. At 10 years, these components look as good as they did on day 1.
The disadvantage of the above is that these components did not allow the use of a separate tibial tray. This meant that the polyethylene component could not be changed if worn out. It also meant that more modern, hardened and/or vitamin E infused, polyethylene could not be used. With more recent technology, separate tantalum trays are now made, but the extra rigidity of these seems to have changed the nature of stress transfer such that they behave like other metal trays that are available.
Accepting all this variation, the literature is still unclear as to whether the long term outlook for a cemented joint is any different from an uncemented one. At this stage therefore, the choice remains the surgeons preference, and depends on his experience with the prosthesis he uses.
Finally, but importantly, and independent of its use to fix the prosthesis to the bone, cement can be used in varying thicknesses to adjust the final tightness of the joint. Too tight can make it sore, too loose can make it unstable. With increasing emphasis on this balance, this seems to be one of the best ways of providing a knee with optimised balance throughout the range of motion. Again, it is one reason why Dr Holt prefers cement; which thus can be used to fine tune alignment and tension to balance the ligaments, and to make the knee stable - neither too tight nor too loose.
Bone Cement (methyl methacrylate)
This comes with various antibiotics mixed into it, and in both slow (12 min) and fast (7 min) setting
versions. It is fully strong when set.
The problem with this approach is that bone is living and, unlike wood, bone is constantly being removed and replaced. Whether, during this cycle of constant rejuvenation, it grows back as strong as it was depends on a number of factors, including local forces through the bone.
On the tibial side it is usual for a rigid base plate to be used, this being a tray for the polyethylene bearing surface. Independent of how accurate the bone cuts are made, and how good the cementation is, the tray will always sit on some slightly high points putting extra pressure on those areas and hence lowering pressure on other areas. This leads to high stress areas where the bone builds up to support the tray, and low stress areas where the bone may just be resorbed (osteolysis). Generally, these variations of bone strength, whilst often seen on x-ray, are not a great clinical problem. Sometimes however, in high demand patients, the high stress areas can develop stress fractures and stress reactions which can be painful. The opposite effect, where bone that is shielded from stress and gets resorbed, can lead to prosthetic loosening: though this is unusual with today's prostheses.
For the above reasons, engineers continue in their quest for a reliable, cement free joint replacement. In most cases, this involves having a special porous surface on the back of the metal prosthesis which allows the bone to grow into it. If this occurs, then the stresses that go through the joint should be much more like normal, and hence, bone should theoretically build up evenly under the tibial plate, thus becoming stronger with time.
Many such surfaces have been developed, and all seem
Cement or no cement?
Traditionally, joint replacements have been cemented into the bone. Theoretically this would seem to be a good idea. It means that the prosthesis is solidly glued into the bone at the outset, and that recovery should therefore be fairly quick. In addition, the cement seals the ends of the bone which cuts down the bleeding. Hence, there is less bruising and swelling after surgery, so motion should return more quickly.
Cement used as a spacer to adjust tension / laxity between components
2 - 3mm cement space

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
Patella or no patella?
Resurfacing of the patella (kneecap) with a polyethylene button is one of the most controversial areas in knee replacement surgery. Most studies in the literature show that, at least in the first 5 years or so, there is no difference in the results whether the patella is replaced or not. In the last few years however, longer term results are starting to show that patella replacement may be advantageous. Kneecap pain is a not infrequent problem after replacement, whether or not it has been resurfaced. The incidence of this problem may be up to 25% in some designs when un-resurfaced, but in no designs is it completely avoided, even with a polyethylene button on the bearing surface.
Most big surveys of knee replacements are now showing that the ability to be able to climb and descend stairs is enhanced by having the patella resurfaced. Given the low complication rate of patella replacement therefore, it would seem reasonable to carry this out at the time of the initial procedure. Certainly the advantages of this versus leaving the patella alone, are now becoming more compelling. For this reason, Dr Holt resurfaces every patella with a polyethylene bearing surface (button). This then avoids the problem of having to comeback and resurface it later if there is on-going patella pain. It does not however, guarantee that there will be no patella pain.
Femoral Component
Patella
Patella Button
View of the patella button The polyethylene cannot be seen, but the cement
around it can be.
Cement (white)
Oval versus round patella buttonThis shows alterntives to patella resufacing. The left
one shows the usual round patella. The right one shows the same size patella top to bottom, but being
oval there is more coverage of the whole bone.
Patella buttons have traditionally come as round domes. Whilst these work quite well for the most part, the polyethylene does not cover all of the patella. This can cause pain if the patella does not quite sit square in the trochlear groove thus allowing some force to go through the un-resurfaced part of the bone. This has particularly been seen as a problem in posterior stabilised and constrained knees which have a box in the central femoral component where a peg on the tibial component sits to provide stability to the joint. The problem here is that the patella can slightly sink into the box in flexion, and the quads tendon above it can rub on its edges causing inflammation (synovitis): and sometimes this needs an arthroscopy and removal of that inflamed tissue to resolve that issue.
The peri-patella synovitis issue usually causes a
sensation of crepitus as the knee is flexed. When bad enough, and the tissue is thick enough, a lump of the tissue can get caught between the patella and the femur, only to be squeezed out during flexion. This is known as a 'Patella Clunk'. This usually requires surgery to remove the lump, and generally this is not recurrent.
Patella ClunkIn flexion the quads tendon rubs over the edge of the central box of the femoral component in a PS Knee.
Patella ClunkThis shows peri-patella synovitis which grows like seaweed in this condition and can catch beween the
patella and femoral components in flexion.
In recent times, and in response to these problems, some companies have re-introduced oval (or near oval) buttons like some that were used a couple of decades ago. These seem to reduce pain by completely removing direct contact of the femoral component on the bony patella, and they also seem to significantly reduce the synovitis that was associated with the use of the dome patella in some of the more stabilised designs; those which have a central femoral box construction (see below for details of these knees).
Femur
Tibia
Quads tendon
Quads tendonrubs on the edge of the central box
Patella Button
Synovitis

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
CR - (Posterior) Cruciate Retaining Knee
This has a smooth trochlear and no central box.
Types of Knee ReplacemenT
CR, PS, BCS, CP, Constrained, Medial Pivot, Mobile Bearing, Hinge, and the variants including Distal Femoral & Upper Tibial Replacement.
The prostheses come in different types which are used based on both the individual surgeon's preference, and the requirements of the knee concerned. Essentially, there are 8 main varieties which are made, of which, 6 are currently available in Australia. In all of these, except the CP (Cruciate Preserving), the ACL (Anterior Cruciate Ligament) is removed. Whilst in a normal knee this would cause instability, in a knee replacement, the intrinsic design is such that this does not occur. The prosthesis itself is stable and therefore does not require an ACL.
CR - Cruciate retaining knees, being updated versions of the original design of almost all modern day prostheses, still remain popular worldwide. They are called Cruciate Retaining because they preserve the PCL (Posterior Cruciate Ligament) not the ACL. The advantage of these is that they have the best longevity: at least as documented in the Australian Joint Registry reviewing knee designs that were implanted 20 years ago. The downside is that the PCL can be hard to preserve such that it remains fully functional and, in a good many of these knees, the PCL is at least partly damaged and loses at least some of its function. This occurs because the portion of the tibia that is removed to allow insertion of the tibial component, also contains some of the footprint of the PCL. Loss of PCL function causes the tibia to have increased laxity, allowing it to move back and forth on the femur during motion. This forwards and backwards motion, whilst usually not noticed can, if significant, be enough to cause some instability; albeit that this may actually
PS - Posterior Stabilised knees are a later development of the CR knee. In this version, the PCL is removed along with the ACL. The PCL is then substituted for, the prosthesis thereby replacing the function of the PCL. This is done by having a peg in the middle of the tibial tray which sits in front of a bar on the femoral component, thus stopping the tibia from sagging backwards. The advantage of this is that full PCL function is guaranteed, thus preventing so called 'flexion instability (instability or looseness of the knee when it is at about 45º of flexion). This, in turn, also decreases the force on the patella during bent knee activities: something that may be important given that the commonest site of residual pain in a replaced knee is the patello-femoral joint. One of the downsides of the PS knee has been premature wear of the peg. Early designs caused excessive pressure on the peg, and hence, earlier than expected failure. More modern designs however, have much better designed pegs which, at least in laboratory testing, exhibit much less wear. It is therefore expected, that these more recent designs will address that problem. In addition, better joint surfaces and tougher polyethylene should also help. Currently, the single biggest problem that is seen in the PS knee, relates to the box that is required to fit the peg, and therefore to make the PCL function work. The problem is referred to as 'patella clunk', and is descibed above. Whilst not often a problem, it can present as a painful grating of the knee during flexion, often beginning many months after surgery. If bad enough, the inflamed tissue that builds up around the patella can form a big enough lump of tissue that it can get caught between the patella and the femoral component, hence causing a clunk.
X-ray of a right CRTotal Knee Replacement
give rise to a feeling of pain rather than a feeling of looseness or giving way.

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
BCS - Bi-Cruciate Stabilised KneeThis uses the front and the back of the peg to provide
both ACL and PCL function.
The Journey 11 Knee
If mild it needs either no treatment, or occasionally, just a cortisone injection to settle the inflammation. Providing it is not sore, the grating is of no consequence, and it does not do any damage to the prosthesis. If significant however, and noting that it can worsen with time, an arthroscopy can be performed to remove the offending tissue. This is generally a minor, day case procedure, and recurrence is uncommon.
BCS - Bi-Cruciate Stabilised knees are relatively new. In this design, both the ACL and the PCL are substituted for, and the prosthesis is designed to replicate normal knee function rather than that of a simple hinge. This is very important as it causes the femur to rotate outwards (externally) as it flexes, thus aligning the patella groove on the femoral component with the patella much better, similar to the native knee. Because of this, there should be much less shear force on the patella in flexion, and it is thought that this should therefore provide not only better function, but significantly, less patella pain. If this proves to be the case, then this will solve the single biggest cause of residual problems in knee replacement: and it should significantly improve bending, squatting, climbing and so forth.
The archetypal BCS design, the Smith & Nephew 'Journey 1' knee, was introduced a decade or so ago, but never released for general use in this country. However, it was used in testing centres around the country, and more widely elsewhere. Subsequently though, it was withdrawn from the market because of mixed results. It turned out that this knee produced either excellent results, or poor results, with little in between. Further research suggested that this knee, whilst functioning the nearest to a normal knee in the laboratory, was hard to put in because there was not enough tolerance engineered into the design to provide some forgiveness in the placement of the components during insertion. Trying to get the exact centres of rotation and pivot points to be exactly the same as in a normal knee was too difficult, and remains so, even with computer navigation, computer planning and robotic assistance.
PS - Posterior Stabilised KneeThis has a central box and a peg which articulates
on a bar at the back of the box to replicate PCL function.
The Legion PS Knee
The bar at the back of the femoral component
will sit behind the peg and push the tibia forwards as the knee
bends
The peg on the tibial tray will sit in the slot, in front of the bar, on the femoral
component
The tibial tray will lock into the tibial component when
the prosthesis is put together
X-ray of a right PSTotal Knee Replacement
Central box
Some years on, the 'Journey 11' has been released, having addressed all of the design problems that were thought to be an issue with the original 'Journey 1' knee. The revised knee design has now been implanted since 2013 and is in widespread use elsewhere with excellent early results. Importantly, all of the problems

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
that were associated with the 'Journey 1' seem to have been resolved. To date, the 'Journey 11' has not been approved for use in this country, but it is expected to be available soon given the good results seen elsewhere.
CP - Cruciate Preserving knees are very new, and are still being inserted in testing centres only. Essentially, these preserve both the ACL and PCL. The current model, the 'Journey XR', is identical to the 'Journey 11', but rather than substituting for the cruciate ligaments with a peg, it uses the native ligaments. Of course, for this to work, the native ligaments need to be normal: not torn, stretched or contracted. This will therefore preclude many degenerate knees from being so replaced but, as it is essentially a 'Journey 11 knee', the latter can be implanted if it is thought that the knee in question is unsuitable for this style of replacement. Because of the difficulty in getting the joint line at the right level and getting the ligament tensions correct, it may be that advanced navigation systems, with the new robotic technology, will be required to get optimum results from this.
A Constrained ProsthesisA variation on PS and BCS. The difference is the
square peg on the tibial tray which prevents varus or valgus.
Constrained Prostheses knees are a modification of PS and BCS designs. Essentially, the peg in the middle of the knee is made in square cross section instead of round. This means that it can substitute for damaged collateral ligaments (medial or lateral) where necessary. The advantage of this is that it is just a matter of inserting a different polyethylene tibial tray (constrained rather than PS) onto the tibial component, hence straight forward. It just requires a central box, meaning that it can be used with either a standard PS, or BCS, femoral component.
To change from a CR (or an MP) knee to a stabilised knee however, requires a change of femoral component to one with a box. This then means that, in a revision situation, the old femoral component needs to be
removed: hence making this somewhat bigger surgery to do.
The major use of constrained knees is in the revision situation where there is often damage to the capsule and collateral ligaments because of the removal process involving the old prosthesis. It is also known that the results of revision surgery are better when this style of prosthesis is used in preference to insertion of another primary style of implant (CR or PS).
The downside of a constrained knee is that it puts extra forces on the femoral component because the varus / valgus (bow-legged / knock knee) stability that it exerts is provided by the peg in the femoral box. Accordingly, there is some evidence that this can occasionally produce premature loosening of one of the components. When necessary however, it provides a simple and reliable solution to what can be a difficult problem (one of medial or lateral ligament insufficiency).
CP - Cruciate Preserving KneeThis preserves both ACL and PCL for which reason
there is a cutout in the centre of the tibial component. It also needs a small cutout (but not a box) in the
femoral compnent.
The Journey 11 XR Knee
Medial Pivot knees are a relatively old design but which, with newer versions now available, have started to become popular. What these do is to provide front to back (sagittal) stability similar to a PS design knee, except that this is done by making the medial part (inside half) of the knee a ball and socket. Although this would at first seem a strange thing to do, it turns out that this is how the normal knee works. Essentially, in the normal knee, the medial condyle of the femur stays within a socket on the medial tibia which is formed by the meniscus and its ligamentous attachments. The lateral femoral condyle on the other hand, can slide backwards and forwards in an arc on the lateral tibia with flexion. This motion, sometimes called rollback, occurs because the tibia internally rotates (turns inwards towards the opposite tibia) during knee flexion: an effect caused by the ankle joint. The ankle and the subtalar joint below it, in combination, form what is

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
A Mobile Bearing Knee This separates the flexion component (above the poly
insert) from the rotation component (below). Note that there is complete conformity of the femoral
component to try and reduce wear.
Despite this, in some hands, these knees have given very good results. As a consequence therefore, they are still in widespread use today. The main aim of the design however, was to make the polyethylene wear less and for it to therefore last longer. Interestingly though, despite the theory, the long term follow up by the Australian National Joint Replacement Registry does not show this to be the case: and in any event, the current generation polyethylene is so good that premature wear in any of the above designs is rare. Accordingly, the reason to choose such a knee is now one of personal preference rather than one of component longevity.
'essentially' a crooked hinge. It is descibed in more detail above, but essentially, ankle flexion rotates the tibia inwards.
This so called 'rollback' is important in the knee, mostly for patella tracking and function. This is because the internal rotation of the tibia necessarily rotates the tibial tubercle with it, whereby decreasing the angle of force that occurs across the patella. That is, a reduction of the 'Q' angle. Although this could theoretically replicate normal knee function, it doesn't do that all that well because there is no ACL function remaining in the knee. Clearly, if full function was restored, the knee would be unstable just like in a normal knee that has had an ACL injury. Accordingly, whilst the design allows for some rotation of the femur during flexion of the knee, it is limited.
It seems that medial pivot knees are liked because of the stability they provide from the constrained ball and socket arrangement on the medial side of the knee. In addition, they do not require a box to house a peg for PCL and ACL function, which may therefore mean that they are less liable to develop a 'patella clunk' or related problem. Outcome studies suggest that medial pivot and bi-cruciate substituting designs feel the most normal.
A Medial Pivot KneeCreates a ball and socket mechanism on the medial
side which is conforming and provides good stability. The lateral side rotates about this.
Mobile Bearing knees, in various incarnations, have been around since the 1980's. These were originally designed to allow some rotation of the tibia at the knee whilst increasing constraint of the tibial and femoral components. It was thought that by increasing the contact area between the femoral component and the polyethylene tibial tray, that wear would be reduced. Indeed, this proved to be the case but the mechanics were not normal, and the design did not allow the femur to roll backwards on the tibia during flexion of the knee. As a consequence, these knees tended to have less flexion range than more conventional knees; that is, they do not bend as far.
Hinge Knees are the next step up in stability. Essentially, these link the femoral and tibial components by a hinge mechanism. These always require some sort of stem on each side so as to spread the forces over larger lengths of the tibia and femur. Whereas once these prostheses were prone to relatively early failure because of over-constraint, they now come with rotation available at the knee (a so called 'Rotating Hinge') and some vertical laxity which allows slight separation of the components during flexion; all of which goes towards decreasing the stresses put on the tibia and femur, hence providing better longevity as well as better function.
The most advanced hinge available, is based on the Smith & Nephew 'Journey 11' design. It not only allows some femoral rotation during flexion of the knee, it actually makes it happen: thus producing more normal knee function. This sort of freedom at the knee, coupled with excellent all round stability, can thus provide a very good solution to the very damaged knee with little remaining ligament function. It can also be used where there is moderate amounts of bone loss, including situations where there is substantial bone missing from previous failed replacement surgery.

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
The Legion Hinge Knee (HK)In this knee the components are linked together by a hinge mechanism which provides ultimate stability in all directions. It is for use in knees with extensive
ligament damage or bone loss.
Another use of a hinge is in the knee where there is poor quads muscle control thereby requiring the knee to be hyper-extended (over straightened) to provide stability when walking. This action gradually stretches out the tissues at the back of a normal knee so, over time, the knee becomes gradually looser and more hyper-extended. Only a hinge will prevent this. It is therefore indicated in arthritic knees where there is an associated muscular, or neurologic, problem which affects control of the knee.
Choosing a prosthetic knee is like choosing a car: one model might look best, another may last longest, another may have the best engine, and yet another may be the nicest to drive, etc. In other words - you can't have it all in one package. Hence, this means choosing a prosthesis on the values that seem to be most important at the time. There is no one best prosthesis, just better lasting ones - as shown in the Australian National Joint Replacement Registry. Outcome satisfaction measures however, are not part of the data collection, and may not correlate with longevity of a particular prosthesis.
The Link range of tumour prosthesesVarious companies make a range of prostheses which are expandable, thereby covering most
contingencies. Here is a range from Proximal Tibial Replacement through to Distal Femoral and Total
Femoral Replacement.
Given that Hinge Knees come with stems, it can be easily augmented with extra wedges of metal to fill any bone deficiencies. Such augments, which can be used on both sides of the joint, are off the shelf components, and hence, are freely available for use. Hospitals that do a reasonable amount of revision work will have all these extras on the shelf to cater for any such indications.
Standard prosthesis (CR, PS, BCS etc) can also accept stems and augments if required, but these are all meant for situations that require less stability than a hinge.
Proximal Tibial, Distal Femoral, and Total Femoral, Replacement are the domain of the tumour surgeon. Essentially, these are based on the hinge format but, instead of just filling up small areas of bone loss with augments and bigger polyethylene components, these simply replace the whole proximal tibia, the distal femur or, in the case of bone loss right up to the hip, or involving the hip joint as well, the whole femur. These latter prostheses have a hip joint at the top and a hinge knee at the bottom.
Use of so much metal and plastic significantly increases the infection risk, so some of these prostheses come with a silver coating (or similar) which leaches out into the nearby tissues. Silver is strongly anti-bacterial, and hence, such coating greatly reduces infection.
A Distal Femoral Replacement for a peri-prosthetic fracture
This represents a good sloution for situations where the likelihood of dealing with the pathology by repair
is unlikely to succeed.

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2019
Further information can also be obtained on this and other related topics, such as:
Knee Replacement - Total and PartialKnee Replacement - the hospital journey
Pain Management after Knee ReplacementRehabilitation after Knee Replacement
Knee Replacement after dischargeBilateral Knee Replacement
Infection after Knee ReplacementRobotic Surgery
and more
at: www.keithholt.com.au