Embed Size (px)
Citation preview

Total Knee Arthroplasty in Patients With Prior Ipsilateral Hip Fusion
D a v i d W. R o m n e s s , M D , a n d B e r n a r d F. M o r r e y , M D
Abstract: Sixteen total knee arthroplasties performed between 1977 and 1985 in 13 patients with prior ipsila~eral hip arthrodesis or ankylosis were studied to determine the preferred sequence and long-term follow-up of procedures in this clinical setting. Twelve of 16 underwem fusion takedown and total hip arthroplasty prior to knee replacement. The average age at total knee arthroplasty was 52.7 years and the average time from hip fusion to total knee arthroplasty was 36.3 years. Mean follow-up after total knee arthroplasty was 5.5 years (range, 2.3 to 10 years). The Hospital for Special Surgery knee score increased from a mean of 31.8 preoperatively to 72.2 after surgery. In patients who had conversion of the hip fusion prior to knee replacement, knee scores were 28 before and 72.5 after both procedures. Patients who retained their hip fusion had mean scores of 43.5 and 72.1, respectively. None of the knees has been removed and 14 of 16 had no pain at last follow-up. One had mild pain and one had moderate pain attributed to pes anserine bursitis. Although the numbers are small, this experience reveals that takedown of the fusion with total hip arthroplasty is an effective technique before performing the knee replacement. Though successful in some instances, the experience is too small to show that if hip fusion is in good position, knee replacement without fusion takedown is acceptable. Key words: total knee arthroplasty, hip fusion
The problem of the ipsilateral knee following hip arthrodesis has been addressed in previous reports. A biomechanical analysis by Gore et al. (7) has shown that the knee on the fused side is subject to different patterns of mot ion than knees in normal subjects. Other reports show an increased incidence of ligamentous laxity, knee pain, and degenerative arthritis. The incidence of degenerative changes in the knee after ipsilateral fusion of the hip is well known and has been reported as high as 68.2% (4, 8, 10, 13, 15). Conversion of a hip fusion to total hip arthroplasty has not been reliable in relieving symptoms at the knee (i, 3, 14, 16). Thus, some patients require reconstructive procedures on the
From the Department of Orthopedics, Maya Clinic and Mayo Foun- dation, Rochester, Minnesota,
Presented at the American Academy of Orthopaedic Surgery Annual Meeting, Anaheim, CA, March 1991.
Reprint requests: Bernard F. Morrey, MD, Mayo Clinic, 200 First Street SW, Rochester, MN 55905.
knee. However, the long-term success of technical considerations of this problem has not been primarily addressed. The purpose of this study was to deter- mine the preferred sequence of procedures in those with severe gonarthrosis and ipsilateral hip fusion and to assess the long-term outcome of total knee arthroplasty in this uncommon, but demanding, clinical setting.
Materials and Methods
Total knee arthroplasty (TKA) was performed on 4,642 knees at the Mayo Clinic between 1977 and 1985. Sixteen of these that were performed in 13 patients with prior ipsilateral hip fusion were stud- ied. There were five males and eight females. The mean age at the time of hip fusion was 17.3 years (range, 6 to 43 years). The mean time from fusion to total knee arthroplasty was 36 years (range, 4 to
63

Tab
le
1.
Cli
nic
al
Dat
a in
P
atie
nts
W
ith
K
nee
R
epla
cem
ent
and
Ip
sila
tera
l H
ip
Fu
sio
n
O~
-4
¢D
t- O
e-
Pro
- P
osi
tio
n
of F
usi
on
*
Kn
ee
Ag
e A
ge
Len
gth
H
SS
Sco
reK
nee
ced
ure
A
ge
at
Rea
son
In
vo
lve-
at
at
F
oll
ow
-up
N
o.
Sex
S
ide
Fu
sio
n
for
Fu
sio
n
+-A
bd
uct
F
lex
Ext
Rot
m
ent:
~
TH
A
TK
A
t(y
rs.)
P
reo
p
Po
sto
p
Har
ris
Hip
K
nee
RO
M
Sco
re
Pre
op
P
ost
op
P
reo
p
Po
sto
p
,.%
::3-
1 F
R
9 S
urg
ical
--
10
20
0 II
68
69
4.
3 40
94
.5
sept
ic h
ip
2 M
L
13
Su
rgic
al--
TB
-
5 25
0
I 64
64
6.
8 35
60
3
F R
6
Su
rgic
al--
TB
10
20
15
It
38
38
10
.0
29
76
4 F
L 19
A
nk
ylo
sis-
- l0
40
0
II
26
26
8.3
10
57
psor
iati
c ar
th.
5 F
R
27
An
ky
losi
s--
--
80
--
I 30
30
5.
3 23
.5
80.5
R
A
6 F
L 27
A
nk
ylo
sis-
- --
80
--
I
30
30
5.3
23.5
76
R
A
7 M
R
15
A
nk
ylo
sis-
- -
15
10
l0
II
57
57
3.4
27.5
70
R
A
8 M
L
18
An
ky
losi
s--
- 5
30
10
I1
58
58
2.3
i2
70
RA
9
F R
12
S
urg
ical
--
- I0
15
0
III
52
52
5.3
13
39
seps
is
10
M
R
12
An
ky
losi
s--
10
50
5 II
62
62
7.
3 37
79
T
B
(cas
ted)
11
F
R
14
Ank
ylos
is
l0
50
0 II
56
65
4.
5 46
81
(c
aste
d)-
se
psis
12
F
L 14
A
nkyl
osis
15
45
0
II
56
63
6.0
37.5
8I
(c
aste
d)-
se
psis
13
M
R
24
S
urg
ical
--
0 20
0
I N
on
e
28
3.4
51
80
trau
ma/
seps
is
I4
F R
42
S
urg
ical
--
10
30
0 I
No
ne
75
5.6
44
75
CD
H/D
JD
15
F R
10
A
nk
ylo
sis-
- 0
30
0 II
N
one
70
5.1
38
50.5
T
B
(cas
ted)
16
M
L
13
Su
rgic
al--
TB
10
20
0
II
No
ne
58
5.8
40
84
10
-90
0
-10
0
69
88
5-1
0
I0-3
5
56
72.7
1
0-8
5
0-9
0
67
78.3
3
0-3
0
0-5
0
33
55
80
-10
0
0-8
5
33
79
80
-10
0
10
-10
0
33
79
0-2
0
0-I
0
49
61.8
45
-60
0
-60
49
62
.3
20
-90
1
0-5
0
35
47.2
10
-60
0
-70
70
85
.8
10
-12
0
0-1
05
52
67
.8
15
-11
5
0-1
05
52
31
.5
10
-80
0
-85
N
A
--
15
-90
0
-65
N
A
--
10
-12
0
0-8
5
NA
--
10
-85
0
-10
0
NA
--
"o
< o "-.4
Z o ~o
cD
TB
, tu
ber
culo
sis;
R
A,
rheu
mat
oid
ar
thri
tis;
C
DH
, co
ng
enit
al
hip
d
ysp
lasi
a;
DJD
, d
egen
erat
ive
join
t d
isea
se.
* A
bd
uct
ion
, +
; A
dd
uct
ion
, -,
t
Fo
llo
w-u
p
sin
ce
kn
ee
rep
lace
men
t.
:1: S
ee t
ext
for
def
init
ion
.

TKA and Prior Ipsilateral Hip Fusion • Romness and Morrey 65
60 years) and the m e a n age at the time of total knee arthroplasty was 52.7 years (range, 26 to 75 years). Twelve of the 16 hip fusions underwent conversion to total hip arthroplasty a mean of 12.2 months prior to knee replacement (range, 6 days to 8 years). Three patients with bilateral hip fusion had the fusion con- vetted to a hip replacement prior to knee replace- ment.
The etiology of the hip fusions is shown in Table 1. Eight hips were surgically arthrodesed, four an- kylosed following casting for sepsis, and four un- derwent spontaneous ankylosis secondary to inflam- matory disease of the joint. The position of the fusion in the group that had the fusion converted to a total hip replacement as recorded by the examining sur- geon averaged 38.8 ° of flexion, 2.1 ° of abduction, and 3.3 ° of external rotation (Fig. 1). In the group that retained the hip fusion (cases 13-16) the po- sition of the hip was more desirable, averaging 22.5 ° of flexion, 5 ° of abduction, and no rotation (Fig. 2).
The indication for knee arthroplasty was severe pain and radiographic joint destruction in all cases. The ability to define the a l ignment of the knee ac- curately was limited because of the malposit ion of the extremity f rom the hip fusion. Furthermore, the type of forces imparted to the knee are so extensive in some instances that the knee is grossly distorted (Fig. 1). An at tempt was made to correlate in a qual- itative manne r the severity of the knee arthrosis and the position of the hip fusion (Table 1). Knee in- volvement was thus graded as mild (I) if arthrosis was associated with less than 10 ° varus or valgus alignment; modera te (II) if greater than 10 ° angular deformity was present; or severe (III) if ~,he joint was subluxed more than I cm or greater than 2 cm of joint depression had occurred.
Since this study covered m a n y years, several pros- thetic designs were used as shown in Yable 2. The prosthesis was secured with cement in ~4 cases and uncemented designs were used in 2. Surgeons did not note any particular technical difficulties related to the fused hip w h e n performing the knee replace- ment in patients w h o retained their fusion.
The mean fol low-up period was 5.5 years (range, 2.3 to 10 years). Nine patients (11 knees) were ex- amined with physical examinat ion and radiographs and four (5 knees) answered questionnaires and sent current radiographs. The questionnaire contains il- lustrations to approximate knee motion, thus allow- ing an accurate determinat ion of the knee score. Knees were graded before and after surgery with the Hospital for Special Surgery (HSS) knee score, which is based on pain, function, range of motion, muscle
Table 2. Prosthetic Types Use
Knee arthropIasty Kinematic 7 PCA 3
Cemented 2 Ingrowth 1
Kinematic 1 stabilized Stabocondytar 1 Tavernetti 1 Geomedic 1
Total 16 Hip arthroplasty
DF-80 4 Charnley 3 T-28 3 PCA ingrowth 1 Aufranc-Turner 1
Total 12
strength, flexion deformity, and stability (12). An excellent result was 8 5 - 1 0 0 points; good, 7 0 - 8 4 points; fair, 6 0 - 6 9 points; and failure, less than 60 points. Hips that underwent arthroplasty were also graded using the Harris hip score, which rates hips based on pain, function, deformity, and range of mo- tion (9).
Radiolucent lines were evaluated using standing anteroposterior and lateral radiographs according to zones described by Insall et al. (11).
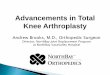
Fig. 1. (A) A 67-year-old woman with severe bilateral post- septic coxarthrosis, 51 years after spontaneous right hip arthrodesis, in excessive abduction (case 1). (Figure con- tinues)

66 The Journal of Arthroplasty Vol. 7 No. 1 March 1992
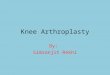
Fig. 1. (B, C) The knee is severely arthritic with subluxation. (D) The right hip was replaced to improve position and function. (E) The knee was replaced 6 months later, shown here with no pain and motion from 0 ° to 100 ° 10 years after surgery. (Figure continues)

TKA and Prior Ipsilateral Hip Fusion • Romness and Morrey 67
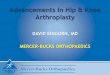
Fig. 2. (A) A 74-year-old woman, 23 years after right hip arthrodesis for congenital hip dislocation in good position (case 14). (Figure continues)
Fig. I. (F) The knee was replaced 6 montl',s later, shown here with no pain and motion from 0 ° to 100 ° lO years after surgery.
Results
The HSS knee score inc reased f rom a m e a n of 31.8 p reope ra t i ve ly to a pos tope ra t ive score of 72.2 (Table 1). Using this score, 1 knee was r a t ed excel lent , 11 were good, 1 was fair, a n d 3 we re poor . Of the p o o r results , one pa t i en t h a d psora t ic ar thr i t is l imi t ing h e r func t ion and h a d knee m o t i o n f rom 0 ° to 50 ° (case
Fig. 2. (B, C) The right knee is minimally symptomatic. (Figure continues)

68 The Journal of Arthroplasty Vol. 7 No. 1 March 1992
4); one had good function but had moderate pain that was thought to be secondary to persistent pes anserine bursitis (case 12); and one had mild pain, poor motion, and poor function for unknown rea- sons (case 9). The radiographs showed good pros- thetic fixation in all three of these cases.
Of the four patients who retained their hip fusion (cases 13-16) , the mean knee score increased from 43.5 preoperatively to 72.1 postoperatively. The se- verity of the gonarthrosis was less in these four, as indicated by the mean preoperative knee score (Table 1). Three of these knees were rated good and one was poor. The 12 patients who had their hip fusion converted to a prosthetic hip increased their mean knee score from 28 preoperatively to 72.5 postop- eratively. In this group, one was excellent, eight were good, one was fair, and two were poor (cases 4 and 9). Similarly, this group tended to have more exten- sive deterioration of the knee joint as evidenced by the preoperative knee scores (Table 1).
Preoperative knee motion averaged 22 ° to 78 ° . The mean range of motion at last follow-up was 2 ° to 75 ° . The mean arc of motion increased from 57 ° to 73 ° with knee arthroplasty. A comparison of motion between the two groups in this study is shown in Table 3.
Radiolucent lines were present with no progres-
T a b l e 3. Mean Knee Range of M o t i o n and Arc of Mot ion (°)
With All Arthrodesis Prosthetic
Knees Maintained Hip
Range of motion Preoperative 22-78 11-94 25-73 Postoperative 2-75 0-83 3-72
Arc of motion Preoperative 57 83 48 Postoperative 73 84 69
sion in two knees (zone A in one and zones A and E in the other). Neither patient had pain.
Complications and Reoperations
O n e patient underwent manipulation 12 days after knee surgery. There was one case of venous throm- bosis. There were no symptomatic pulmonary em- boli and no infections of the knee arthroplasty.
Patients who underwent conversion of the hip fu- sion to total hip arthroplasty had a mean Harris hip score of 50 before and 67 at last follow-up after sur- gery. One hip was revised due to aseptic loosening and one underwent resection arthroplasty due to deep infection.
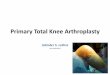
Fig. 2. (D) Nine years later the contralateral left hip has been treated with joint replacement. (E) The right knee is painful with progressive arthrosis. (Figure continues)

TKA and Prior Ipsilateral Hip Fusion • Romness and Morrey 69
Fig. 2. (F, G) The patient is asymptematic with motion from I5 ° to 90 ° 14 months after knee replacement.
Discussion
Ipsilateral knee pain and gonarthrosis often de- velop in patients with a hip fusion. Multiple studies have shown improvement in knee symptoms follow- ing conversion of the hip fusion to total hip arthro- plasty. Amstutz and Sakai (1) reported improvement in five of seven patients with preoperative knee pain after hip replacement for arthrodesis. Lubahn et al. (14) noted that all four of their patients with pre- operative knee pain had total relief of their knee pain following conversion to hip replacement. Brewster et al. (3) reported on 33 patients with hip fusion who showed improvement in knee symptoms after hip replacement, however, two of their patients went on to total knee arthroplasty. Strathy and Fitzgerald (16) reported knee pain as an indication for revision to a prosthetic hip, however, they did not report in- cidence or improvement in knee symptoms. None of these authors noted the detailed clinical or radio- graphic findings at the knee.
Knees with significant degenerative changes due to altered mechanics from a fused hip would not be expected to improve and many eventually go on to require total knee arthroplasty. An important con- sideration for the practicing surgeon is whether the
position of the hip fusion causes more extensive al- teration or destruction in the knee. If so, this would argue in favor of converting to a mobile hip before the knee surgery to decrease stresses on the knee implant and interface after replacement. While the numbers are not large enough to definitively address this question, our interpretation is that the extent of knee involvement is a function of the position of hip fusion. We, therefore, favor conversion to hip re- placement before knee surgery. However, the un- derlying disease process may also be the cause of primary knee arthrosis as well as the pathologic con- dition causing the hip fusion. There is virtually noth- ing published on the management of the combina- tion of hip fusion and knee arthritis. Hence information needed to direct a t r e a t m e n t program is lacking. In the only previously published report on ipsilateral total knee arthroplasty in patients with hip fusion, Garvin et al. (6) reported on nine cases in which the arthrodesis was maintained. At an average follow-up period of more than 7 years, their results were comparable to previously reported results of knee replacement in patients without a hip fusion from the same institution. However, they noted an increased incidence of stiffness and the need for post- operative manipulation.

70 The Journal of Arthroplasty Vol. 7 No. 1 March 1992
To the best of our knowledge the results of knee replacement following ipsilateral hip fusion conver- sion to a hip replacement has not been previously studied. The reason for this is the obvious rarity of the condition. The few cases wi th heterogenous pa- thology reported here do not al low the question to be resolved wi th complete certainty. However , suf- ficient data exist to al low some insight into this un- c o m m o n and difficuk problem.
All patients in the current study had improvement in their knee symptoms and function, the HSS knee score improved in all patients and overall improved by a m e a n of over 40 points. The am oun t of knee flexion was not improved after surgery, however , ex- tension and functional arc of mot ion were improved. Results reported in this study are not as good as pre- viously reported for routine total knee arthroplasty (2, 5, 11). This m a y be due to the severity of pre- operative knee problems and to patients in the study who had become severely debilitated by their un- derlying disease.
Comparison be tween patients w h o did and did not have prel iminary hip surgery is difficult because of the small num be r of cases in the later group. The postoperative knee score was similar but knee mo- tion was less in patients w h o underwent conversion to hip replacement. This m a y be related to the un- derlying disease of patients in this group, which in- cluded more debilitated patients (5 of 12 knees in this group were in patients wi th inf lammatory ar- thritis). More extensive use of manipula t ion may have improved knee flexion.
When the hip is arthrodesed in an op t imum po- sition, main tenance of the fusion was noted to still allow successful knee replacement, but the follow- up is relatively short. Knee replacement in patients who mainta in their hip fusion can be technically more demanding, but, in general, the knee is not as severely involved if the position of fusion is good. There is usually adequate flexion of the pelvis to allow proper knee positioning, however , flexion is not as good as with a functioning hip joint. Careful attention to al ignment is also important with an im- mobile hip. Because proper a l ignment is so essential to the long- term result of knee replacement and since this does correlate with the position of fusion, our preference is to replace the hip prior to knee replace- m e n t .
Conclusions
A satisfactory result can be expected w h e n per- forming total knee arthroplasty in patients who de- velop gonarthrosis after ipsilateral hip fusion. Func- tional outcome is partially dependent on severity of
preoperative knee symptoms and the underlying dis- ease process. Takedown of the fusion is preferred by the authors but the few cases in which this was not done show equally successful results wi th relatively short- term follow-up.
References
1. Amstutz HC, Sakai DN: Total joint replacement for ankylosed hips: indications, technique, and prelimi- nary results. J Bone Joint Surg 57A:619, 1975
2. Bourne MH, Rand JA, Ilstrup DM: Posterior cruciate condylar total knee arthroplasty: five year results. Clin Orthop 234:129, 1988
3. Brewster RC, Conventry MB, Johnson EW Jr: Con- version of the arthrodesed hip to a total hip arthro- plasty. J Bone Joint Surg 57A:27, 1975
4. Callaghan J J, Brand RA, Pedersen DR: Hip arthro- desis: a long term follow-up. J Bone Joint Surg 67A: 1328, 1985
5. Ewald FC, Jacobs /VIA, Miegel RE, et al: Kinematic total knee replacement. J Bone Joint Surg 66A: 1032, 1984
6. Garvin KL, Pellicci PM, Windsor RE, et ah Contra- lateral total hip arthroplasty or ipsilateral total knee arthroplasty in patients who have a long-standing fu- sion of the hip. J Bone Joint Surg 71A:1355, 1989
7. Gore DR, Murray MP, Sepic SB, Gardner GM: Walk- ing patterns of knee with unilateral surgical hip fusion. J Bone Joint Surg 57A:759, 1975
8. Greiss ME, Thomas R, Freeman MAR: Sequelae of arthrodesis of the hip. J Soc Med 73:497, 1980
9. Harris WH: Traumatic arthritis of the hip after dislo- cation and acetabular fractures: treatment by molded arthroplasty: an end-result study using a new method of result evaluation. J Bone Joint Surg 51 A: 737, 1969
10. Hauge MF: The knee in patients with hip joint an- kylosis: clinical survey and biomechanical aspects. Acta Orthop Scand 44:485, 1973
11. InsaU JN, Hood RW, Flawn LB, Sullivan D J: The total condylar knee prosthesis in gonarthrosis: a five to nine year follow-up of the first one hundred consecutive cases. J Bone Joint Surg 65A:619, 1983
12. Insall JN, Ranawat CS, Aglietti P, Shine J: A com- parison of four models of total knee replacement prostheses. J Bone Joint Surg 58A:754, 1976
13. Lipscomb PR, McCaslin FE: Arthrodesis of the hip: a review of 371 cases. J Bone Joint Surg 43A:923, 1961
14. Lubahn JD, Evarts CMCC, Fekner JB: Conversion of ankylosed hips to total hip arthroplasty. Clin Orthop 153:146, 1980
15. Sponseller PD, McBeath AA, Perpich M: Hip arthro- desis in young patients: a long-term follow-up study. J Bone Joint Surg 66A:853, 1984
16. Strathy GM, Fitzgerald RH Jr: Total hip arthroplasty in the ankylosed hip: a ten year follow-up. J Bone Joint Surg 70A:963, 1988