Embed Size (px)
Citation preview

Topographic Inventories of VagalAfferents in Gastrointestinal Muscle
FENG BIN WANG AND TERRY L. POWLEY*
Department of Psychological Science, Purdue University, West Lafayette, Indiana 47907
ABSTRACTTo inventory and characterize the two types of vagal afferents (both putative mechano-
receptors) in the muscle of the gastrointestinal tract, the authors injected wheat germagglutinin-horseradish peroxidase into the nodose ganglia of rats that had received unilateralventral rhizotomies to eliminate efferents. The gut, from the oral esophagus to the distalcolon, was divided into wholemounts, processed with tetramethylbenzidine, and surveyed toestablish normative topographic maps of afferents. Vagal intraganglionic laminar endings(IGLEs) were ubiquitous, with concentrations varying on a longitudinal gradient (higherrostrally). This overall gradient was punctuated by denser condensations of endings in theoral esophagus, gastric corpus, and distal ileum. In regional specializations, IGLEs werefused into conspicuous, dense networks in the laryngeal esophagus and the antrum. Intra-muscular arrays (IMAs) had restricted distributions, including the walls of the stomach andthe sphincters throughout the gut. In the forestomach, a singular concentration of orthogo-nally crossed IMAs was organized into a lattice or “fovea.” IMAs displayed variations inmorphology, with one specialization consisting of short, terminal processes associated withsphincters and a more widespread form consisting of long, rectilinear processes in theforestomach, along the greater curvature, and in limited intestinal regions. On the basis oftheir topographic patterns and structural specializations, the two putative mechanoreceptorsmay have different functions: IGLEs appear situated to integrate intramural tension, andperhaps myenteric neuronal activity, into rhythmical, propagated motor programs, such asswallowing, peristalsis, and emptying. IMAs are distributed strategically and appear tosatisfy structural requirements for stretch receptors tuned to tonic or more aperiodic eventsthat may affect central nervous system processing as well as local gastrointestinal coordina-tion. J. Comp. Neurol. 421:302–324, 2000. © 2000 Wiley-Liss, Inc.
Indexing terms: autonomic nervous system; mechanoreceptors; vagus nerve; visceral afferents
The vagus nerve supplies at least two types of afferentendings to the muscle coat of the gastrointestinal (GI)tract. Both of these afferents in the gut wall are assumedto be mechanoreceptors on the basis of their respectivelocations in muscle, their morphologies, and their prelim-inary electrophysiologic characterizations. Despite thisgeneral formulation, however, neither the functional char-acteristics nor the adequate stimuli of either ending havebeen delineated.
One of these processes is the intraganglionic laminarending (IGLE). The ending was described first by Nonidez(1946) and then was characterized more fully by Rodrigoand coworkers (1975, 1982). Rodrigo and colleagues alsoprovided the commonly used name of IGLE for the ending(Rodrigo et al., 1975), a designation that emphasizes boththe location of the ending (i.e., in myenteric ganglia) andits characteristic morphology (i.e., laminae of puncta dis-tributed primarily on either or both ganglionic boundaries
or poles abutting the muscular layers). The ending hasbeen characterized thoroughly (Rodrigo et al., 1975, 1982;Neuhuber, 1987; Neuhuber and Clerc, 1990; Berthoud andPowley, 1992), and its general distribution throughout theesophagus, stomach, and intestines has been described(Berthoud and Powley, 1992; Wang and Powley, 1994;Powley and Wang, 1995; Berthoud et al., 1997; Dutsch etal., 1998).
Grant sponsor: National Institutes of Health; Grant number: DK27627.F.B. Wang’s current affiliation: National Chung Cheng University, Tai-
wan.*Correspondence to: T.L. Powley, Department of Psychological Science,
165 Peirce Hall, Purdue University, West Lafayette, IN 47907.E-mail: [email protected]
Received 19 July 1999; Revised 25 January 2000; Accepted 26 January2000
THE JOURNAL OF COMPARATIVE NEUROLOGY 421:302–324 (2000)
© 2000 WILEY-LISS, INC.

The other vagal afferent process is the intramusculararray (IMA). The ending was distinguished by Berthoudand Powley (1992). Its name, which was introduced morerecently (Wang and Powley, 1994; Powley and Wang,1995), describes the site in which it is found (i.e., withinthe muscle sheets) and part of its structure (i.e., typically,it consists of an array of rectilinear terminals parallelingthe muscle fibers). The structure of the ending has beencharacterized partially (Berthoud and Powley, 1992), andits distribution in the stomach and sphincters of the GItract also has been described (Berthoud and Powley, 1992;Kressel et al., 1994; Phillips et al., 1997; Neuhuber et al.,1998).
Although relatively detailed structural profiles of thetwo types of endings (particularly IGLEs) are available,only general descriptions of the regional distributions ofthe two endings have emerged (Neuhuber, 1987; Wangand Powley, 1994; Berthoud et al., 1997; Phillips et al.,1997; Phillips and Powley, 1998). The current experimentwas performed to extend these characterizations. Morespecifically, quantitative descriptions of the distributionsof the vagal afferent endings in the GI tract were estab-lished to yield information pertaining to three sets ofissues. First, a characterization of region-by-region pat-terns of terminal densities and comparisons of these pat-terns with the physiological roles of the different regionsmay provide information relevant to the functional spe-cializations of the different endings. Second, systematicinventories of different loci throughout the GI tract mayidentify either additional types of vagal afferent terminalsor structural variants in the broad classes already recog-nized. Both more detailed information on regional organi-zation (the first set of issues) and specification of differentmorphologic specializations of the endings (the second setof issues) should facilitate correlations with electrophysi-ological profiles. Third, quantitative descriptions of thetopographic patterns of afferents in the GI tract shouldprovide indices for measuring alterations in this innerva-tion such as might occur during development, with neu-ropathies, over the course of regeneration, or during theaging process. To date, little progress has been made inassessing potential reorganizations of vagal projections insuch circumstances (see, e.g., Villalta et al., 1989; Ka-neoke et al., 1995; Fazan and Lachat, 1997; Zanone et al.,1998), due in part to the lack of normative baselines thatmay provide sensitive measures of changes or differences.
Traditionally, surveys of GI innervation have been com-plicated by several technical limitations. Most descrip-tions have been based on necessarily limited samples ofsectioned tissues, making it difficult to extrapolate or gen-eralize to the entire GI tract. In addition, because thedifferent organs of the GI tract can vary substantially indiameter (and length, in the case of the stomach and thececum) as a function of diet composition, feeding schedule,and many other factors, comparisons of precise sites fromanimal to animal frequently have been problematic atbest. Furthermore, because the viscera receive innerva-tion from mixed nerves and contain the different elementsof the enteric nervous system as well, distinguishing par-ticular types of fibers (e.g., vagal afferents) requires selec-tive labeling or staining strategies compared with morecommonly applied, panneuronal strategies.
The current experiment adapted protocols that werechosen to minimize the limitations described above: 1) Theanterograde tracer wheat germ agglutinin-horseradish
peroxidase (WGA-HRP), which appears to be bound andincorporated by all nodose neurons, was used to label theentire population of vagal afferents innervating the gut. 2)A selective motor rhizotomy procedure was used to ex-clude vagal efferent axons that otherwise may have beenlabeled. 3) To make it practical to compare and to combinespecimens from different animals as well as to surveylarge regions of the gut more efficiently, wholemountstaken from the entire GI tract were divided and preparedfollowing a standardized protocol. 4) Tissue boundariesand landmarks were used as fiducial points, and elasticsampling grids were fitted individually to specimens, sothat counts of endings could be normalized in the same GIcoordinate system for all animals.
The results demonstrate characteristic gradients in re-ceptor densities, describe regional concentrations of vagalafferent terminals, document novel structural variationsof both IGLEs and IMAs at particular locations in the GItract, and establish the normative patterns of vagal inner-vation that can be used to evaluate the development,regeneration, or dissolution of the visceral afferent inner-vation of the gut wall.
MATERIALS AND METHODS
Subjects
Male Sprague-Dawley rats (Harlan, Indianapolis, IN)weighing 215 6 35 g when they received their first surgery(rhizotomy) were used. The animals were housed individ-ually at 23°C on a 12:12 hour light:dark schedule. Solidchow (laboratory diet no. 5001; PMI Feeds, Inc.) and tapwater were available ad libitum. All rats received a wetchow supplement for 1–3 days postsurgery. All protocolswere approved by the Purdue University Animal Care andUse Committee and were conducted in accordance withthe Guidelines of the American Association for Accredita-tion of Laboratory Animal Care.
Surgeries
Each animal underwent two surgeries separated by21 6 10 days. In both interventions, each rat receivedNembutal (50 mg/kg, i.p.) as an anesthetic, atropine sul-fate (1.0 mg/kg, s.c.) to reduce secretions, and Demerol (10mg/kg, s.c.) as a postsurgical analgesic. Incisions weretreated with the antibiotic powder Nitrofurazone beforeand after the skin was sutured.
Rhizotomy. In the first surgery, each animal under-went a unilateral (left in 9 animals, right in 13 animals)intracranial vagal ventral rhizotomy (i.e., motor rhizot-omy; cf. Walls et al., 1995). Briefly, the caudal skull wasexposed from a dorsal approach, and an operative windowwas drilled (no. 6 round dental bit) in the angle formed inthe occipital bone by the dorsolateral part of the occipitalcondyle. The meninges covering the vagal roots were ex-posed and incised, and the ventral rootlets were cut witha sharpened microhook.
Nodose tracer injection. After a 3-week interval thatallowed the motor fibers to degenerate, each animal re-ceived a pressure injection (53 pounds of pressure for 3–4msec; 20–40 mm micropipette inner diameter; Pico-spritzer II; General Valve Corporation, Fairfield, NJ) ofWGA-HRP (3 ml; 2.5% in distilled H2O; Vector Laborato-ries, Burlingame, CA) into the nodose ganglion ipsilateralto the de-efferentation.
303VAGAL AFFERENTS TO GI WALL

Rhizotomy verification and tissue counterstaining.
Each animal was injected with FluoroGold (2.0 mg/1.0 ml0.9% saline, i.p.) 2 days before perfusion to yield both anindex of completeness of the rhizotomy (Powley et al.,1987; Walls et al., 1995) and a counterstain of the entericnervous system (Powley and Berthoud, 1991).
Tissue preparation
Each animal was injected with a lethal intraperitonealdose of Nembutal. Five minutes later, the animal receivedinjections of Regitine (25 mg/kg, i.p.) to facilitate vasodi-lation and of heparin (0.2 ml; 1,000 units/ml in the leftventricle). The rat was then perfused transcardially withsaline (300 ml for 5 minutes at 37°C) followed by 3%paraformaldehyde in 0.1 M phosphate buffer, pH 7.3–7.5(500 ml for 15 minutes at 4°C), and then 10% sucrosephosphate buffer, pH 7.3–7.5 (500 ml for 15 minutes at4°C).
The GI tract was removed, divided into organs, washedwith tap water, and stored in phosphate buffer, pH 7.3–7.5, at 4°C. To facilitate comparisons or combinations ofcounts from different animals, all organs were trimmedand divided in the same fashion. Stomachs were separatedinto dorsal and ventral walls by making longitudinal cutsalong the lesser and greater curvatures. Intestines weredivided into longitudinal segments and then opened intoflat sheets with longitudinal cuts along the mesentericattachment. Esophagi were prepared similarly with lon-gitudinal cuts along the tracheal attachment. The sheetsof muscle wall of the alimentary canal were prepared assets of wholemounts after the submucosal/mucosal layerswere separated from the various specimens with a forceps(Powley et al., 1994). Some of the submucosal/mucosalpeels of the GI tract, particularly from the esophagus, alsowere prepared and examined.
Wholemounts were processed according to the tetram-ethylbenzidine (TMB) protocol of Mesulam (1978). Pro-cessed specimens were mounted with the circular musclelayer up on gelatin-coated slides, covered immediately with asecond slide coated with Sigmacote (Sigma, St. Louis, MO),and then pressed with weights. Thirty minutes later, theSigmacote-coated top slides were removed, and the flat-tened tissue was exposed overnight to air at room temper-ature to dry. The specimens were then dehydratedthrough ascending alcohol solutions (70%, 95%, 100%, and100%) for 10 seconds each, cleared with xylene (twochanges for 5 minutes each), and coverslipped with DPX(Aldrich, Milwaukee, WI). For additional perspectives, fro-zen serial transverse sections (112 mm or thicker) of the GItract from other animals were prepared similarly.
The brainstem also was removed; stored in 15% sucrosebuffer, pH 7.3–7.5, at 4°C; and then sectioned into serialcoronal thick sections (112 mm; throughout the dorsal vagalcomplex). Animals were classified as having a complete ven-tral rhizotomy only if the dorsal motor nucleus of the vagusipsilateral to the surgery was devoid of FluoroGold-labeledneurons (#10 cells/entire side), whereas the contralateralnucleus was well labeled ('3,000–4,000 cells/side; for de-tails, see Powley et al., 1987; and Walls et al., 1995).
Inventory strategy for vagal afferentterminals
Twenty-two rats with verified complete unilateral ven-tral rhizotomies were included in the current surveys. Theinventories proceeded in two steps. In a first stage, all
tissues from all animals were screened systematically forregional variations in IGLE and IMA morphology andwere checked for any additional classes of endings labeledby nodose injections. For a quantitative inventory, i.e., asecond step, specimens were excluded if they 1) were tornor partially stripped during processing, 2) had excessivelyheavy endogenous peroxidase activity from mast cells orresidual erythrocytes that could obscure elements, or 3)exhibited weak HRP-TMB reactions.
Counting analyses
All counts were made with darkfield illumination at350 (objective 36.3, eyepiece 38) with a Leitz widefieldOrthoplan II microscope (Leitz, Wetzlar, Germany). Fortopographic surveys, a counting grid displayed in the mi-croscope field was used (Fig. 1, upper left). This countinggrid, in turn, was positioned with sampling grids (seebelow; see also Fig. 1) fitted to the different organ whole-mounts. A distinct cluster 1) of terminal puncta, 2) arisingfrom a single axon, and 3) encapsulating a myentericganglion (or pole of a ganglion) was defined as an “IGLE”(for examples, see Figs. 3, 4). Each separate IGLE termi-nal within (i.e., .50% of its surface area inside) the count-ing grid was counted as an IGLE.
An array 1) of two or more parallel terminal processes,2) originating from a single axon, 3) interconnected bybridging elements, and 4) coursing in either the circularmuscle layer or the longitudinal muscle layer was consid-ered an “IMA” (for examples, see Figs. 4C, 9). Two group-ings of such linear processes that did not originate from acommon fiber and/or were separated by significant dis-tances were considered separate IMAs. For counting, be-cause the fiber of origin or other elements of an IMA werenot always visible within the counting grid field and, thus,it was not always practical to distinguish separate affer-ents, the intersections of parallel terminal processes withthe lines of the counting grid IMAs were counted.
For the topographic surveys, individual labeled neuriteswith the caliber of a single axon were judged “fibers,” andgroups of profiles consisting of two or more fibers coursingtogether were counted as “bundles.” For each countinggrid sample, in addition to counting the number of each ofthe different elements, the orientation (i.e., circular orlongitudinal) of IMAs, fibers, and bundles also was re-corded.
The counting grid was moved systematically over thewholemounts, so that comparable regions were sampledfrom each animal. Two sampling grid versions, one for themore tubular organs (i.e., esophagus, duodenum, jejunum,ileum, and colon) and a second for the more saccularorgans (stomach and cecum), were used (Fig. 1).
Esophageal, duodenal, jejunal, ileal, andcolonic sampling
In these structures, the densities of the different WGA-HRP-labeled vagal afferents were determined in 1.7-mm-wide, transverse strips situated every 5 mm along thelength of the wholemount (Fig. 1). By using this algo-rithm, '35% of the area of a gut wholemount was sampleddirectly.
Stomach and cecum sampling
Whereas the esophagus and intestines were relativelyconstant in length and varied primarily in their degree of
304 F.B. WANG AND T.L. POWLEY

dilation, the stomach and cecum, the organs with promi-nent reservoir functions, varied substantially from case tocase in both the circular dimension and the longitudinaldimension. To normalize these organs to a standard tem-plate, an elastic sampling grid was devised and fitted toeach wholemount (see Fig. 1). Because the cecum had amuch lower density of vagal afferents, it proved practicalto scan and count the entire organ rather than to workwith the elastic grid and sample only intersections.
With the elastic sampling grid strategy used for differ-ent wholemounts, it was then practical to combine com-
parable sites of the ventral and dorsal walls of the stom-ach as well as to combine sampling sites of stomachs andintestines from animal to animal. In addition, designatingthose intersections that fell in gastric regions (forestom-ach, corpus, and antrum) made it possible to combinecounts for the samples from each of the gastric areas. Forthese pooled regional estimates, those intersections over-lapping or very near boundaries (Fig. 1, shaded intersec-tions) were not included in the pooled samples (consistingof 15 intersections for the forestomach, 15 for the corpus,and 4 for the antrum on each side of the stomach).
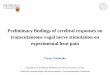
Fig. 1. The counting and sampling grids used for topographicsurveys. The counting grid (top left) consisted of an 8 3 8 reticlecovering 2.89 mm2 when projected into a 350 field of view in themicroscope. Each field sampled was scanned and ambiguous elementswere classified before the counting was done. By rotating the countinggrid so that its lines were parallel to the fibers of the two musclesheets, it was possible to separately inventory bundles, fibers, andintramuscular arrays (IMAs) coursing parallel to circular muscle fi-bers versus those running with longitudinal fibers. All vagal intra-ganglionic laminar endings (IGLEs), IMAs, fibers, and bundles werethen counted in four separate z-scans as well as x-scans and y-scansof the reticle. The same counting grid was used for inventorying allwholemounts. A sampling grid was used to position the counting gridat specific coordinate sites. One version of sampling grid, illustratedon the right, was designed for the tubular organs (esophagus, smallintestine, and large intestine), whereas another version, representedat the bottom left, was developed for the more saccular organs (stom-ach and cecum). In the case of tubular organ wholemounts, a series oftransverse or circular bands separated at 5-mm intervals along thelength of the organ were counted. The midline (antimesentery) of theorgan at the level of each sampling strip was determined by measur-ing from the lateral (mesenteric) boundaries. Left and right halves ofthe viscus were distinguished. The counting grid was aligned imme-diately lateral to the midline, and the four elements (i.e., bundles,fibers, IGLEs, and IMAs) were inventoried. The grid was movedradially in 1.7-mm steps, and the process was repeated until theentire circular strip had been surveyed. To adjust for differences in
circumference along the organs as well as for animal-to-animal dif-ferences in organ diameter (wholemount width), counts obtained atthe peripheral cut edges of the wholemounts were expressed in termsof the actual area or portion of the grid sampled and then were scaledup to a full counting-grid equivalent for analyses and data presenta-tion. To fit a sampling grid to a saccular organ, and to the stomach inparticular, the distance between one “longitudinal” line at the limit ofthe lesser curvature and a second at the limit of the greater curvaturewas measured and divided by 6 to yield a unit distance that wouldproduce 6 equal, longitudinal rows fitted to the stomach. Similarly,the distance between one “circular” line at the proximal limit of the(fore)stomach and a second at the distal limit of the corpus/antrumwas measured and divided by 10 to yield a unit distance that wouldproduce 10 circular columns fitted to the organ. The 45 intersectionsof the lines defining this elastic grid were designated the samplingsites. The counting grid was then centered on each intersection orsampling point, and this reticle was rotated so that one of its axesparalleled the circular muscle at that location, and the other axisparalleled the longitudinal muscle. Intersections and fields of viewfalling outside the wholemount (black fields in the schematic) wereexcluded. For quantitative summaries in which the sampling siteswere pooled into forestomach, corpus, and antrum groupings, thoseintersections occurring on or near regional boundaries (gray fields inthe schematic) were excluded. The samples obtained by positioningthe counting grid at the 45 intersections of the stomach covered 10%of the total area of the wholemount.
305VAGAL AFFERENTS TO GI WALL

Statistics
The selection criteria for quantification yielded samplesets of six (stomach and ileum) or five (each of the otherorgans) complete and low-artifact specimens that werecounted. Three animals with left rhizotomies and nodoseinjections and two animals with right rhizotomies andnodose injections provided complete wholemount sets.
Because the final sets of specimens quantified for thedifferent organs were not obtained from exactly the samesubset of animals, statistical comparisons generally weredone within organs and not between organs. For the pur-poses of general discussion, however, a limited number ofbetween-organ comparisons also were performed. Re-gional densities and percentages were analyzed with arepeated-measures two-way analysis of variance. Deter-minations for left and right (or ventral and dorsal) halveswere evaluated separately and then combined for somedescriptions, except where asymmetries occurred. Thesymmetry or asymmetry of each class of vagal elementswas assessed with regression analyses: The respectivesampling grid points were translated into series, and theseries for the right nodose was then correlated with thecorresponding series for the left nodose. A high correlationcoefficient (r . 0.60) was used as an index of symmetry.
All counts were considered relative measures and wereevaluated without the application of a correction factor. Inaddition, a stereologic approach was not used. These strat-egies were based on several considerations: We preservedthe whole muscular wall and did not section it eithermechanically or optically. Wholemounts of the GI tractlike those used here essentially are monolayers. Becauseof issues of labeling completeness and other sources ofvariability, we deemed it more appropriate to consider ourcounts relative estimates (e.g., for comparing density inthe corpus vs. density in the antrum) rather than asprecise estimates of absolute number.
Photomicrographs were taken with TMAX 400 black-and-white film and Kodak Gold 25 color film (Eastman-Kodak, Rochester, NY). Extraneous lint or artifact wastouched up with Spotone.
RESULTS
Esophagus
General survey of vagal afferents. IGLEs were themore prominent and ubiquitous vagal endings observed inthe esophageal muscle coat. They formed several consis-tent patterns and assumed characteristic shapes: 1) Indi-vidual vagal axons innervating the esophagus issued mul-tiple IGLEs clustering in adjacent ganglia; theseterminals varied in shape from round, club-like, or leaf-like to thickened, free nerve endings (Figs. 3, 4). 2) Theywere distributed both longitudinally and radially through-out the entire esophagus. 3) The IGLEs were lateralizedwith little overlap: The right nodose ganglion innervatedthe right side of the esophagus, and the left nodose gan-glion innervated the left side of the esophagus. 4) In thetransverse plane, IGLEs were distributed most denselynear the tracheal attachment rostrally and the mesentericline caudally (Fig. 2). 5) Longitudinally, IGLEs were dis-tributed more densely orally and less densely aborally. 6)Within the general longitudinal gradient of ending den-sity, IGLEs were distributed particularly densely in tworegions, one at the level of the upper esophageal sphincter
and the other at the level of the esophageal hiatus,roughly a centimeter above the lower esophageal sphinc-ter.
In addition to such overall distributions of traditionallyshaped IGLEs, a conspicuous specialization of these end-ings appeared at the level of the upper esophageal sphinc-ter. In this region, the innervation was so dense that theIGLEs and bundles of vagal afferent fibers fused ormerged into a characteristic compact network or denseplexus (Fig. 5A,B).
In the esophagus, IMAs virtually were confined to thelower esophageal sphincter (Fig. 4C). The IMAs were lo-cated in and parallel to the circular muscle of the loweresophageal sphincter. They were numerous in the deeperpart of the circular muscle, i.e., nearer to submucosa.These esophageal IMAs were composed of multiple, short,terminal processes (100–200 mm).
In addition to the esophageal muscle afferents invento-ried in the wholemount series, other elements were ob-served in the submucosa in transverse sections and insubmucosal wholemounts. A striking network of termi-nals coursed longitudinally in the submucosa at the levelof larynx. This laryngeal submucosal network consisted oflong elements traveling rostrocaudally for about 8 mmthat were interconnected by shorter elements bridgingtransversely (Fig. 5C,D).
Fig. 2. Camera lucida tracing of the afferent innervation of theesophagus supplied by the right nodose ganglion. This tracing from acomplete montage illustrates the lateralized pattern of innervation ofthe esophagus. The rostral (left) and caudal (right) halves of theesophagus are separated at the level of the aortic arch. Part of therostral esophagus traced here is represented in the photomicrographin Figure 5. Note that the region of the upper esophageal sphincterhas more dense processes than the rest of the esophagus. At this scale,only bundles and especially prominent intraganglionic laminar end-ings (IGLEs; a few of which are indicated by arrowheads) can be seen;individual fibers, small IGLEs, and intramuscular arrays (IMAs) aretoo fine to appear. Lt, left side of the esophagus; Rt, right side of theesophagus. Scale bar 5 2.0 mm.
306 F.B. WANG AND T.L. POWLEY

Topographic mapping of afferent elements. Figure6 summarizes the density of IGLEs at successive longitu-dinal levels of the esophagus. The esophageal IGLEs sup-plied by the left and right nodose ganglia were distributedwith significant density gradients running both longitudi-nally (P , 0.001 for both left and right vagi) and circularly(P , 0.001 for both left and right vagi). Longitudinally, thedensity (endings per mm2) of IGLEs was greatest in themore rostral esophagus (first 1 mm or so); then, it declinedprogressively along the length of the esophagus, with asecondary peak in density oral to the lower esophagealsphincter. More globally, the wholemount of the rostralhalf of the esophagus averaged twice the density of IGLEsobserved in the wholemount of the caudal half of the organ(rostral:caudal density was 2:1 for left nodose innervationand 2:1 for right nodose innervation; P , 0.05). Circularly,the highest densities of IGLEs in the esophageal wall werenear the tracheal attachment rostrally, and near the mes-enteric line caudally (Fig. 6A9,B9). This circular gradientwas most pronounced at the oral end of the esophagus and
gradually became flatter at the gastric end of the organ.The radial gradients also were lateralized insofar as theright nodose ganglion provided IGLEs predominantly tothe right half of the esophagus (75%; P , 0.001), and theleft nodose ganglion provided IGLEs predominantly to theleft side of the esophagus (74%; P , 0.001). The projectionfields of the left and right vagi were symmetrical.
Fig. 3. Darkfield photomicrographs of wheat germ agglutinin-horseradish peroxidase (WGA-HRP)-stained intraganglionic laminarendings in the esophagus. For illustration, a small (single arrow),medium (double arrows), and large (triple arrows) IGLE are desig-nated. This sample specimen of endings is located in the thoracicesophagus caudal to the aortic level. Scale bar 5 100 mm.
Fig. 4. Darkfield photomicrographs illustrating the types of vagalafferent endings observed in the caudal esophagus. A: Low-powerview illustrating a number of individual vagal fibers forming IGLEs inthe caudal esophagus. B: Higher power view of three club-like orthickened IGLEs issued by a single fiber. C: Field of IMAs (severalexamples are indicated by arrowheads) in the circular muscle of thelower esophageal sphincter. Scale bars 5 300 mm in A; 100 mm in B,C.
307VAGAL AFFERENTS TO GI WALL

Fig. 5. Vagal afferent specializations in the esophagus. A: Low-power view from a wholemount of the region of the upper esophagealsphincter (for location, see Fig. 2). B: Enlargement from the upperright-hand corner of A. The dense network of fused IGLEs and bun-dles that are characteristic of the oral esophagus is indicated byarrowheads. Simple, singular IGLEs are indicated by small arrows.
C: Submucosal endings in a wholemount at the level of the upperesophageal sphincter. D: Photomicrograph of a frontal section of theesophagus at the level of the upper esophageal sphincter. Arrowheadsdesignate the plexus of endings in the submucosa (see C), and arrowsin the obliquely sectioned muscle indicate IGLEs. Scale bars 5 800mm in A; 400 mm in B; 200 mm in C; 100 mm in D.

Fig. 6. Topographic maps and plots of the vagal afferent innerva-tion of the esophagus. Similar plots are employed throughout thearticle for the different gastrointestinal (GI) organs. A: Surface-and-contour plot of the esophageal innervation (IGLE) density contributedby the right nodose ganglion. Viewer’s perspective is from the oral (tothe left) and lateral (down) sides of the esophagus. The x-axis (0–70mm) is the length of the esophagus (data for the two wholemountscombined), the y-axis (5 to 25 mm) is the circular dimension of thewholemount, and the z-axis is IGLE density. A*: Full frontal perspec-tive of the same topographic map that illustrates most simply theextent to which the right nodose issued a lateralized projection to theesophagus. B: Surface-and-contour plot of the esophageal IGLE in-
nervation contributed by the left nodose ganglion (the same perspec-tive as A). B*: Full frontal perspective of the left nodose projection tothe esophagus. A comparison of A9 and B9 illustrates the symmetry ofthe lateralized projections to the esophagus. C: The innervation den-sity of IMA projections from the right (solid circles) and left (opencircles) nodose ganglia sampled on the circular axis at the level of thelower esophageal sphincter (70 mm). Note that the concentration ofIMAs in the sphincter occurs distal to the secondary peak of IGLEs inthe caudal esophagus. A comparison of the left and right nodoseprojections illustrates a peak in the radial distribution of IMAs andindicates a symmetry in the projections of the two ganglia.
309VAGAL AFFERENTS TO GI WALL

In the esophagus, IMAs were observed regularly only inthe lower esophageal sphincter. These IMAs at the caudallimit of the esophagus were distributed in the circularmuscle (see Fig. 6, lower right). Both the right and leftnodose contributed equally to the field of IMAs. The pro-jections of the two vagi to the sphincter were organizedalong a striking circular gradient, with the greatest den-sity of endings rotated essentially 90° from the two vagaltrunks (i.e., the 21.7 mm sampling point of the grid inFig. 6).
Level-by-level analyses of the counts of both vagal af-ferent bundles and fibers demonstrated that these ele-ments had the same distribution patterns (i.e., longitudi-nal gradients, circular gradients, laterality of projection,etc.; details not shown) that were observed for IGLEs.Figure 7 summarizes the longitudinal patterns of axonbundle and fiber densities for the esophagus collapsedacross the circular axis, with the counts for esophagealIGLEs expressed similarly (Fig. 7, top row) for compari-son.
Stomach
General survey of vagal afferents. The stomach wasinnervated richly, with conspicuous bundles of afferentfibers fanning out radially from the gastroesophagealjunction. Figure 8 is a montage of a wholemount of aventral wall of one stomach. As individual axons ap-proached their targets, they separated from the bundles offibers, which occupied the connectives of the myentericplexus, to course into local ganglia in the case of IGLEs orinto muscle sheets in the case of IMAs. Both IGLEs andIMAs were found throughout the stomach, although theyboth varied dramatically in density and morphology fromregion to region.
IGLEs occupied most myenteric ganglia throughout thestomach. Individual afferent axons formed multiple ter-minal IGLEs, typically innervating several neighboringganglia of the myenteric plexus.
IMAs also were found throughout the stomach, al-though they varied quite substantially in packing density(see below), orientation (i.e., predominately circular orprimarily longitudinal), and size. Regional differences inIMA lengths were particularly characteristic. IMAs com-prised of short ('200 mm) terminal elements paralleledmuscle fibers in the pylorus (see Fig. 10B,C) and in thecircular muscle of the lesser curvature; in contrast, IMAswith extensive terminal elements ('1,000 mm) paralleledmuscle fibers in the forestomach (see Fig. 9) and thegreater curvature.
Although they probably are best considered to be simplyvariants of the two general types of vagal afferent termi-nals, two local gastric specializations or receptor concen-trations of the vagal afferent innervation that have notbeen described previously were particularly conspicuousand, arguably, could be considered separate types of end-ings. One of these local variants consisted of a densenetwork or plexus of afferent terminals in the antrum (seeFig 10A). In this local antral network, fiber bundles andIGLEs were packed so closely and densely that they pro-duced a meshwork apparatus with a honeycomb appear-ance. The pattern was similar morphologically to the spe-cialized network observed in the laryngeal region of theesophagus (see above). The other local variant consisted ofa dense field of IMAs organized with a conspicuous latticepattern in the forestomach (Fig. 9E,F). In this particular
Fig. 7. Two-dimensional plots of the longitudinal distributions ofdifferent elements counted, illustrating density gradients along theesophagus, for right (solid circles) and left (open circles) nodose pro-jections. At each level of the esophagus, counts have been collapsedover the circular dimension. From top to bottom, plots representsequentially the density of IGLEs, counts of circularly coursing fiberbundles, counts of longitudinally coursing fiber bundles, counts of allfiber bundles, counts of the circularly directed individual axons,counts of the longitudinally coursing single axons, and counts of allindividual axons. Horizontal axis: rostrocaudal position of the sam-pling strip as designated in each plot. C, circular direction; L, longi-tudinal direction; Lt, samples from five animals with left nodoseinjections of WGA-HRP; Rt, samples from five rats with right nodoseinjections of tracer.
310 F.B. WANG AND T.L. POWLEY

region, long, prominent, rectilinear IMAs in the circularmuscle were crossed orthogonally (in different planes)with similarly extensive IMAs in the longitudinal musclesheet. In contrast to this dense, three-dimensional latticepattern in the middle of the wall of the forestomach, mostregions of stomach not only had fewer IMAs: they alsopredominantly had IMAs located primarily in one or theother muscle sheet. For example, excluding the latticeregion described above, circular IMAs predominatedthroughout much of the forestomach, whereas longitudi-nal IMAs predominated along the greater curvature of theforestomach and the corpus.
Topographic distributions of vagal elements. Thequantitative analysis of the stomach confirmed thatIGLEs were distributed most densely in the corpus (seeFig. 11A,B). When the sampling grid points were groupedby conventional stomach regions, the average density of
IGLEs in the corpus (6.3 IGLEs per mm2) was signifi-cantly greater than their concentration in the forestomach(2.8 IGLEs per mm2; P , 0.005). The antrum had anintermediate number (3.8 IGLEs per mm2) of the termi-nals (this is an overall value for the antrum and not avalue for the dense network area only). The distributionsof vagal IGLEs in the stomach also were lateralizedstrongly. The ventral or “left” stomach wall contained 97%of the IGLEs originating from the left nodose ganglion,whereas the dorsal or “right” half stomach contained 96%of the IGLEs issued by the right nodose ganglion (P ,0.001). The small minority of IGLEs found contralateral totheir nodose of origin tended to be just over the greatercurvature, where they could be interpreted either as form-ing short wrap arounds or as resulting from experimentalerror in separating the organ into precisely symmetricalhalves. Regression analysis indicated that the patterns of
Fig. 8. Vagal afferent innervation of the stomach. A montage of aventral stomach wholemount from an animal that received a leftnodose injection of WGA-HRP. The pylorus is at the upper right, andthe forestomach is at the left. The fiber bundles enter from the loweresophageal sphincter (excised at the top) and radiate over the stomachto the greater curvature. At this scale, fiber bundles are the mostconspicuous elements, although larger IGLEs can be seen, and prom-
inently elongated, longitudinal IMAs at the greater curvature of theforestomach also can be seen. In the antrum (upper right), the fasci-cles of the gastric branch of the vagus that course across the pylorus(the vertical cut in the extreme upper right) to innervate the initialsegment of the duodenum also can be observed. The organ measures42 mm on the long axis.
311VAGAL AFFERENTS TO GI WALL

projections from the left and right nodose were symmet-rical.
IMAs were distributed predominately, although not ex-clusively, in the forestomach rather than in the antrum orthe corpus (see Fig. 11C,D). This concentration in theforestomach peaked in a dramatic receptor concentrationor “fovea” at the forestomach site where the lattice ofcircular and longitudinal IMAs occurred. When the sam-
pling grid points counted were combined into the conven-tional regions of the stomach, the average density of IMAsin the forestomach overall (17.3 IMAs per mm2) greatlyexceeded that in the corpus (2.9 IMAs per mm2; P , 0.001)or the antrum (0.6 IMAs per mm2). IMAs had the samestrongly lateralized pattern that was noted for IGLEs. Theventral gastric wall received 98% of the IMAs from the leftnodose ganglion, whereas the dorsal stomach received
Fig. 9. Darkfield photomicrographs of the vagal afferent ending inthe wall of the stomach. A,B: Examples of long and multiple-armedIMAs (arrowheads) in the circular muscle of the ventral stomach wall.Profiles of IGLEs also can be seen. The small, white, oval cells seen inmany of the darkfield views (including A–D) are mast cells thatexpress endogenous peroxidase activity. C,D: Low-power examplesillustrating the typical patterns and densities of IMAs observed in the
circular (C; greater curvature, forestomach) and longitudinal (both Cand D) muscle wall. E,F: Still lower power views of the lattice of IMAsfound in the forestomach (ventral and dorsal, respectively). The fineindividual processes are elements of IMAs; the dense white profilesare fiber bundles and IGLEs also found in the forestomach. Scalebar 5 500 mm for A–D; 800 mm for E,F.
312 F.B. WANG AND T.L. POWLEY

94% of the IMAs from the right nodose ganglion. Like thelateralized distribution of IGLEs, the few contralateralIMAs were found primarily along the midline or cuttingedge. The distributions of the fields of IMAs on the ventraland dorsal walls of the stomach were symmetrical (based
on the regression calculation). The local densities of vagalbundles and separate fibers generally conformed to a com-posite distribution of the two types of terminals, i.e., thedistributions of IGLEs and IMAs combined (details of thebundle and fiber distributions not shown).
Intestines
General survey of vagal afferents. Vagal afferentfibers and terminals also were found throughout the mus-cle wall of the small and large intestines (Figs. 12, 13). Theterminals consisted of IGLEs (predominantly) and IMAs.The densest innervation occurred in the initial segment(or bulb) of the duodenum, and the afferents became pro-gressively more sparse moving distally. This overall pro-gression was punctuated by a somewhat denser fieldfound just oral to the ileocecal junction. With the excep-tion of innervation of the proximal duodenum, vagal af-ferents in the intestines were sparser distal to the pylorusthan they were in any region of the stomach (Figs. 14–16).
IMAs in the intestines were limited to a few notableconcentrations. The most conspicuous field of IMAs wasobserved regularly in the large intestine at the junctionbetween the proximal and midcolon segments, '55 mmdistal to the cecum (Fig. 17A). In this colonic field of IMAs,several afferents with between two and eight long ele-ments innervated the circular muscle (for reference to asimilar group of IMAs located in the distal duodenum in aregion that was not included in one of the standard whole-mount samples in the current experiment, see Discussion,below). In addition, another afferent element that mayrepresent a variant of the IMA pattern also was observedoccasionally in the proximal duodenum and the distalileum. This element consisted of a single terminal processor free ending. Without qualifying as an array of parallelprocesses and without bridging elements, such elementswere not counted as IMAs, although it is possible that theyrepresent one extremely simplified variant of the IMAmorphology. IMAs were sufficiently sparse in the intes-tines that no attempt was made to plot them topographi-cally for the quantitative inventory described below.
In addition to the two types of vagal afferents in themuscle coat of the intestine, mucosal afferents as far distalas the distal colon also were observed in the current ex-perimental series (i.e., in the transverse sections of theintestines that were used as adjuncts). These vagal affer-ent endings in the colonic mucosa were free endings at thebase of epithelial cells (Fig. 17) that branched from indi-vidual fibers and appeared very similar morphologically tothe vagal mucosal endings described previously in theproximal small intestine (see Discussion).
Topographic distribution of the afferent elements in
the small and large intestines. Organ-by-organ or re-gional comparisons confirmed that IGLEs were moredense orally and less dense anally. On average, the duo-denum had more (78 IGLEs per circular sampling strip)and denser (3.3 IGLEs per mm2) terminals than the mid-jejunum (12 IGLEs per sampling strip; 0.5 IGLEs permm2) or the distal ileum (14 IGLEs per strip; 0.7 IGLEsper mm2). Within the ileum, the gradient of decreasingdensity was reversed by a characteristic field of endingsthat peaked at a maximum concentration (45 IGLEs in thesampling strip) at the ileocecal junction (Fig. 18; see alsoFig. 20). On the circular axis, intestinal IGLEs consis-tently were more concentrated more near the mesenteric
Fig. 10. Darkfield photomicrographs of vagal afferent endings inthe muscular wall of the antrum and pylorus. A: Part of the denseapparatus of club-like IGLEs and afferent bundles that comprise thespecialized antral network described in the text. B: The band of IMAs(coursing left and right in this view) in the pyloric circular muscle ina gastric wholemount. Afferent bundles and fibers can be seen cours-ing from the antrum (below) into the ring of IMAs. C: Higher magni-fication view of the middle region of B. Scale bar 5 300 mm for A,B;200 mm for C.
313VAGAL AFFERENTS TO GI WALL

attachment and less concentrated near the antimesen-tery.
In contrast to a generally symmetrical pattern of inner-vation from the right and left vagi observed in all sites
rostral to the intestines, a notable asymmetry in innerva-tion occurred for the duodenum. The proximal duodenumwas innervated much more densely by the left vagus. Theleft nodose ganglion provided 3.2 times more IGLEs to the
Fig. 11. Topographic maps and plots of the vagal afferent inner-vation of the stomach. A: Surface-and-contour plot of the gastric IGLEinnervation density contributed by the left nodose ganglion. Viewer’sperspective is from the greater curvature of the forestomach.B: Surface-and-contour plot of the gastric IGLE innervation providedby the right nodose ganglion (same perspective as A). C,D: Illustra-
tions of the corresponding surface-and-contour plots for IMAs fromthe respective nodose sources. The sharp peak in receptor innervationproduced by the conspicuous lattice of IMAs in either side of theforestomach is clear in the surface plots, and the associated contourplots illustrate the location of this gastric “fovea.”
314 F.B. WANG AND T.L. POWLEY

proximal duodenum (119.37 IGLEs per sampling strip;P , 0.0001) than the right nodose ganglion (see Figs.18, 20).
IGLEs were located throughout the entire colon, andthere were significant gradients of terminal densities inboth the longitudinal direction (P , 0.001) and the circu-lar direction (P , 0.001). The proximal and midcolon haddensities of 0.7 IGLEs per mm2 and 0.9 IGLEs per mm2,higher (P , 0.001) than the density found in the distalcolon (0.2 IGLEs per mm2; Figs. 19, 20). The colon imme-diately rostral to the rectum had only sparse numbers ofIGLEs (two to four IGLEs per sampling strip). Circularly,IGLEs were distributed consistently more densely in themesenteric band and less densely in the antimesentericportion of the viscus (Fig. 19). Statistical analyses of thecounts of both bundles of axons and individual fibers in-dicated that these elements had significant longitudinaland circular gradients through the intestines and thattheir distributions were very similar to the topographicpatterns of IGLEs at the same sites (Fig. 20).
DISCUSSION
Overview
The current experiments characterize the topographicpatterns of the vagal afferent innervation of the musclecoat of the GI tract and indicate that this innervationconsists of two general types of endings, namely, IGLEsand IMAs, that have been described previously. Localspecializations of vagal afferent function may be producedby 1) regional differences in the densities of the two typesof terminals as well as perhaps in their relative propor-tions and 2) distinctive differences in the morphology of
IGLEs and IMAs from region to region. Before consideringthe details of this innervation, some of its local specializa-tions, and the implications of these patterns for function,a few issues pertaining to the protocols we used should beconsidered.
Issues of labeling all vagal afferents
The current experiments employed a tracing strategydesigned simultaneously to 1) avoid false positive re-sults from the inadvertent labeling of vagal motor fibersthat course through the nodose and 2) to label all nodoseganglion projections to the GI tract. The prospect ofinadvertent labeling of efferent fibers effectively waseliminated by the use of the intracranial ventral vagalrhizotomies that were verified as complete. Further-more, the conclusion that the experiment was not sam-pling motor fibers is reinforced by the fact that vagal
Fig. 12. Camera lucida tracings of the afferent fiber bundles in-nervating samples of the small intestine. A segment of duodenumappears on the left, and the distal jejunum and proximal ileum appearon the right. Vagal afferent bundles enter the intestines from themesenteric line (the lateral edges of the wholemounts) and coursepredominately toward the antimesentery (longitudinal midlines ofwholemounts). Examples of a few exceptionally large IGLEs are des-ignated with arrowheads. Scale bars 5 2 mm.
Fig. 13. Camera lucida tracing of the afferent fiber bundles inner-vating the large intestine. A wholemount of the cecum appears above,and a wholemount from the transverse colon is shown below. In thececum, afferent bundles enter at the lesser curvature (region of theileocecal and colonic junctions) and radiate centrifugally toward thegreater curvature. In the colon, bundles enter at the mesenteric lineand course to the antimesentery. A few of the particularly largeIGLEs are indicated by arrowheads. Scale bars 5 2 mm.
315VAGAL AFFERENTS TO GI WALL

preganglionic projections to the gut wall have differentmorphologies and sites of termination (Berthoud et al.,1990; Holst et al., 1997) than the fibers described in thecurrent report. The strategy chosen to achieve completelabeling of vagal afferents involved administeringWGA-HRP, which appears to be bound and incorporatedby all neurons in the nodose (Robertson and Grant,1985; Robertson et al., 1992), in a volume that effec-tively infiltrated the entire ganglion.
Comparisons with previous experiments buttress theconclusion that the current labeling for IGLEs and IMAswas particularly complete. In previous series, by usingdifferent anterograde tracers, our laboratory group hasfound that cholera toxin HRP (Phillips et al., unpub-lished), dextran (Jarvinen et al., 1998), 1,19dioctadecyl-
3,3,39-tetramethylindocarbocyanine perchlorate (DiI;Berthoud and Powley, 1992; Powley et al., 1994), andPhaseolus vulgaris-leucoagglutinin (PHA-l; Powley et al.,unpublished results) yield less dense labeling of IGLEsand IMAs than that yielded by using WGA-HRP. Anotherexperiment illustrates the point: Berthoud and his co-workers (1997) recently reported a semiquantitative studyemploying DiI injections and estimating the density ofIGLEs in selected regions. Their estimates were lower(250–500%) than the current WGA-HRP counts. Thoseinvestigators addressed the fact that several features ofthe DiI protocol may have led to an underestimation ofIGLEs (this same underestimate also would have biasedthe investigators’ extrapolations that only one-third ofgastric myenteric ganglia receive IGLE innervation). At
Fig. 14. Vagal IGLEs in the small intestine. IGLEs were distrib-uted throughout the intestines, although they exhibited characteristicregional variations in morphology. A,B: IGLEs in the proximal duo-denum (examples are indicated by arrows). Duodenal IGLEs tendedto be relatively rounded, and multiple IGLEs were formed by a singlevagal afferent. In shape, they were similar to gastric IGLEs, althoughthey appeared to have somewhat smaller field sizes than those in thestomach. C: IGLE profiles in the midjejunum. Arrows indicate one
case. Intestinal IGLEs distal to the duodenum typically were morenarrowly club-like or digit-like, with an individual axon issuing fromone to perhaps five of these separate terminals (see Figs. 15 and 16).D: Vagal IGLE pattern in the rostral ileum. Arrows indicate oneexample. E: Ileal IGLE distribution immediately proximal to theileocecal junction. One profile is indicated by an arrow. Scale bar 5100 mm for A,C–E; 160 mm for B.
316 F.B. WANG AND T.L. POWLEY

any rate, a comparison of previous observations and thecurrent survey suggests that the WGA-HRP protocol usedin the current series produced more inclusive labeling ofvagal afferents than any other common anterograde trac-ing strategy.
In observing that vagal afferents of the gut musclewall from the pharynx through the descending colonapparently consist of only two types of endings, wecannot exclude the possibility that there is a populationof nodose neurons that does not express binding sites forthe lectin WGA and, thus, was not labeled in the currentexperiment. In addition to the observations of Robert-son and coworkers (1992) indicating that all nodoseneurons bind WGA-HRP, however, another set of obser-vations also suggests that the current survey did notmiss a population of vagal afferents: Although the stud-ies have not been complete, the anterograde tracingexperiments (i.e., cholera toxin HRP, dextran, DiI, andPHA-l) mentioned above did not identify a novel class ofvagal afferents in the gut wall. Additional types of no-dosal afferents, of course, do innervate the submucosaand mucosa of the GI tract (Holst and Powley, 1992;Powley et al., 1994; Berthoud et al., 1995b; currentresults) and liver paraganglia (Prechtl and Powley,1987; Berthoud et al., 1992, 1995a).
Topographic distribution of IGLEs andIMAs in the GI tract
The current experiments establish that there are ma-jor gradients in vagal receptor density along both lon-gitudinal and circular axes of the gut; furthermore,orally, but not aborally, vagal projections to the GI tractare largely unilateral and uncrossed. Generally, vagal
Fig. 15. Cecal IGLEs. These club-like or thickened profiles arecharacteristic of vagal IGLEs in the cecum. This particular arbor ofIGLEs is supplied by an individual vagal afferent fiber. Scale bar 5200 mm.
Fig. 16. Pattern of vagal IGLEs in the colon that, particularly inthe more distal colon, tended to be more rounded or leaf-shaped thanthose in the distal small intestine. A: Proximal colon. B: Transversecolon. C: Distal descending colon. Small, isolated oval profiles aremast cells. Scale bar 5 200 mm.
317VAGAL AFFERENTS TO GI WALL

Fig. 18. Topographic distribution of vagal IGLEs in the small intes-tine. All plots are oriented with the oral end of the wholemounts to theleft and the long x-axis corresponding to the longitudinal dimension ofthe organ. A,B: Surface-and-contour plots of the duodenal innervationsupplied by the left and right nodose (left and right, respectively). Theasymmetry, consisting of a considerably more dense concentration of
IGLEs produced by the left nodose compared with the right nodose,can be seen. C,D: The jejunal distributions with symmetrical inputsfrom left and right nodose ganglia. E,F: The ileal distributions ofIGLEs. The increase in concentration of the endings can be seen at thedistal end of the ileum (just rostral to the ileocecal junction).
Fig. 17. Vagal afferent endings (IMAs and mucosal endings) in thecolon. A: Photomicrograph from a wholemount of colonic muscularisexterna at the junction between the proximal colon and the midcolon.A band of colonic IMAs running circularly is indicated by arrowheads.The longitudinally coursing elements are individual afferent axons inthe muscle wall. B: Darkfield photomicrograph from a transversesection through the wall the proximal colon. The muscle wall appears
as a bright band at the bottom of the view. The profiles of one completecrypt (right) and a partial crypt (left) are defined by the large numbersof peroxidase-reactive mast cells occupying the crypt. A single afferentvagal fiber (indicated by arrowheads) courses into the crypt andramifies to produce free endings associated with the epithelium,which does not appear in this darkfield image but was seen withdifferential contrast optics. Scale bars 5 500 mm in A; 50 mm in B.
318 F.B. WANG AND T.L. POWLEY

Figure 18

afferent projections are more dense rostrally and lessdense caudally within the same organ (e.g., esophagusor intestines). There also is a general progression be-tween the organs of the GI tract, with more dense in-nervation occurring rostrally (esophagus, stomach, andproximal duodenum) and less dense innervation occur-ring caudally (distal small and large intestines). Theselongitudinal gradients also have been noted byBerthoud and coworkers (1997; see also Kuramoto and
Kuwano, 1994). In addition, the gut exhibits circulargradients of vagal innervation density. IGLEs as well asvagal bundles and fibers tend to be concentrated mostdensely at the line of attachment where vagal bundlesenter the organ (tracheal attachment, esophagus; mes-enteric attachment, intestines). In the stomach, theendings are distributed most densely between the lessercurvature, where bundles enter, and a midpoint on thecircular axis.
Fig. 19. Topographic distribution of vagal IGLEs in the colon.A: Surface-and-contour plot of colonic IGLEs contributed by the rightnodose. The oral end of the combined wholemounts is on the left, andthe long x-axis of the plot corresponds to the longitudinal dimension ofthe colon. A*: Surface plot from A rotated to a full frontal perspective.
B: Surface-and-contour plot of the left nodose IGLEs in the colon(same orientation as A). B*: Surface plot from B rotated to a fullfrontal perspective. A9 and B9 show that the vagal afferent innerva-tion of the colon is bilateral, and there is little evidence of anyasymmetry.
320 F.B. WANG AND T.L. POWLEY

The current results indicate that the overall longitudi-nal and circular gradients of receptor density in the GItract are punctuated by regional concentrations of each ofthe two endings at strategic locations in the GI tract.IGLEs occur in their highest densities in the oral esoph-agus and in the gastric corpus, with additional concentra-tions in the duodenal bulb and in the ileal wall immedi-ately proximal to the ileocecal junction. IMAs occur indramatic concentrations in the local lattice region of theforestomach and in the major sphincters, i.e., the loweresophageal and pyloric sphincters. Relative to the densi-ties in the local surrounds, concentrations of IMAs alsoseem to occur at special junctures in the duodenum (Phil-lips et al., 1997; unpublished observations) and the colon(current observations).
Vagal afferent fibers and endings exhibit a lateraliza-tion of their projection patterns in the proximal GI tractfrom the esophagus to the duodenum, but they are distrib-uted bilaterally below that level. This pattern means thatthe esophageal and gastric branches of the vagus main-tain a lateralized organization, whereas the celiacbranches form bilateral projections. Although they arelateralized, the vagal afferent projection fields of the prox-imal gut generally are symmetrical. The conspicuous ex-ception is the proximal duodenum, which is innervateddisproportionately by the left vagus (see also Berthoud etal., 1997). This asymmetrical projection, as described re-cently (Phillips et al., 1997), is supplied by the gastrodu-odenal division of the common hepatic branch, whicharises from the left vagus, and it appears that this un-paired hepatic branch accounts for a major part of thevagal innervation of the duodenal bulb. [Because the semi-quantitative survey of DiI-labeled afferents by Berthoudet al. (1997) suggested several left/right vagus asymme-tries in organ innervations, it should be noted that thecurrent topographic inventories throughout the GI tractidentified a statistically reliable asymmetry only in theinnervation of the duodenal bulb. The strategy adopted byBerthoud and colleagues of basing quantitative inferenceson a single animal exemplar for each side did not permitchecks for statistical reliability and cannot substantiategeneral claims of asymmetry.]
Local specializations in IGLE and IMAmorphology
The current experiments suggest that regional special-izations of the vagal afferent innervation are formed notonly by local variations in the density of the innervation ofthe muscle coat but also by regional structural adapta-tions of the two general categories of endings. IGLEs ex-hibited characteristic variants in structure. The densenetworks found both in the oral or laryngeal esophagusand in the gastric antrum appeared to be comprised of anumber of small, densely packed IGLEs and fiber bundlesthat were fused. In contrast, in other regions, IGLEs con-sisted of larger plates of puncta that were distributed lessdensely in neighboring ganglia. The suggestion that theIGLEs vary in extent, density, and other features fromregion to region also was substantiated by a more formalanalysis: Jarvinen and colleagues (1998) employed multi-variate analysis to decide how many basic categories offibers occurred in a digitized sample of 92 vagal afferentsthat formed IGLEs in the stomach and the duodenum.Although the fibers had important distinguishing differ-ences in the stomach compared with the duodenum [e.g.,
Fig. 20. Overall, two-dimensional summary of the longitudinal dis-tributions of the different vagal afferent elements in the intestine. Ateach rostrocaudal level, the counts of the circular sampling strip havebeen collapsed. From top to bottom, the graphs represent sequentiallythe density of IGLEs, counts of circularly coursing bundles, tallies oflongitudinally coursing bundles, combined counts of all bundles, countsof circularly coursing individual fibers, tallies of longitudinally coursingfibers, and counts of all fibers. The contribution of the right nodose (solidcircles) and the left nodose (open circles) are plotted separately. Coinci-dence of the distributions from the right and left nodose reflect symmet-rical patterns of innervation. The conspicuous asymmetry of innervationin the duodenum (left nodose projections . right nodose projections) isapparent. The overall rostral-to-caudal gradient in density of the differ-ent elements also can be seen as well as more local increases in concen-trations in the distal ileum (i.e., near the ileocecal junction) and aroundthe transition between the proximal colon and the midcolon. Verticalaxes, IGLEs/sampling strip or intersections/sampling strip (dependingon element); horizontal axes: longitudinal position of the sampling stripat 5-mm intervals within each segment of the intestine.
321VAGAL AFFERENTS TO GI WALL

stomach fibers averaged larger receptive fields (3.0 mm2
vs. 1.7 mm2) and more IGLEs per fiber ('9 vs. '6)], allfibers appeared to belong to a single general class of af-ferents with receptive fields and other features that maybe adapted to the local tissue conditions.
In a similar fashion, IMAs seem to establish variantsthat characterize different regions by variations in thelength and number of the terminal elements and the num-ber of cross bridges. For example, the three-dimensionallattice generated by a multiplicity of IMAs in the longitu-dinal muscle crossing orthogonally with similar numbersin the circular muscle was a conspicuous feature of theforestomach. In addition, IMAs located in this lattice or“fovea,” as well as in the region of the greater curvaturetended to be composed of long and extensive terminalelements. In contrast, IMAs found in the sphincters and inthe circular muscle near the lesser curvature were com-posed of much shorter elements. IMA clusters in the smalland large intestines tended to be composed of elongatedparallel elements in the circular muscle: We have notobserved IMAs in intestinal longitudinal muscles of intactanimals.
Is there only one general type ofmechanoreceptive afferent?
The principle that the two classes of endings, IGLEs andIMAs, form the basic categories of innervation of the mus-cularis externa needs to be reconciled with a previousobservation. In the original description of IMAs in theforestomach, Berthoud and Powley (1992) observed indi-vidual vagal axons that were polymorphic, with some col-laterals terminating in IGLEs and others forming IMAs.This hybrid morphology raises the possibility that vagalafferents to the muscle wall may be extensions of a com-mon type of neuron that is capable of forming either ter-minal. Such an assessment may be correct at some funda-mental level, but there seem to be sound heuristic reasonsfor considering IGLEs and IMAs as distinct major catego-ries, even if they can be combined into a single, higherorder category of “mechanosensitivity” fibers or “mechano-receptor” fibers. A two-category classification is consistentwith the fact that distributions of IGLEs and IMAs are notcorrelated strongly. In the current findings, the clearestdissociations were observed in the esophagus and the in-testines: IMAs were found in sphincters, the stomach, anda few specialized regions of the intestines, but the esoph-agus and extensive zones of intestine contained essen-tially only IGLEs. Although they were less dramatic, therealso were dissociations within the stomach. The highestdensity of IMAs occurred in the forestomach and sphinc-ters, whereas the highest density of IGLEs was found inthe corpus.
There is a corresponding dissociation of the two termi-nal types at the level of the individual fiber as well. Thehybrid that was characterized originally in the forestom-ach is confined largely to this area. In most regions of theGI tract, one observes axons forming either exclusivelyIMAs or exclusively IGLEs (Phillips et al., 1997; currentresults). In the multivariate analysis of IGLE variantsmentioned above (Jarvinen et al., 1998), .90% of ran-domly selected dextran-labeled vagal afferents issuing atleast one IGLE were composed exclusively of IGLE termi-nals and, thus, were not hybrid.
Functional inferences based on thedistributions of vagal afferents
The two types of vagal endings in the muscle wall pre-viously have suggested general inferences about theirphysiologic functions. For example, Neuhuber (1987; seealso Neuhuber and Clerc, 1990; Neuhuber et al., 1995)postulated that IGLEs may be tension receptors thattransduce shearing forces occurring between the musclesheets on the basis of the superficial location of theseendings within myenteric ganglia and their connectivetissue interconnections with the neighboring musclelayer. Similarly, Berthoud and Powley (1992) suggestedthat IMAs may function as the “in series tension receptorsfound in an in parallel location” that have been postulatedfrom electrophysiologic analyses of gastric afferents (see,e.g., Iggo, 1955; Blackshaw et al., 1987), on the basis of 1)these endings’ locations within muscle sheets, 2) theirlong processes running parallel to the muscle fibers of therespective sheet, and 3) their close association with thenetwork of interstitial cells of Cajal in the muscle. Thecurrent detailed inventories of IGLE and IMA densitiesand distributions offer several possible refinements ofthese ideas.
First, IGLEs, with their ubiquitous distribution andassociation with myenteric ganglia, may be particularlycritical for transducing contractions, migrating motor pat-terns, and local distortion (including tension, whethercaused by contractions or distensions) and for translatingthese stimuli into reflexes that phase propagated andrhythmic motor programs, such as peristalsis and migrat-ing motor potentials. This inference is consistent with theregional variations in IGLEs and their associated myen-teric ganglia. For example, the specialized IGLE networkor complex, which we have observed in the laryngealesophagus, appears to correspond with the dense plexus ofmyenteric ganglia in the region (Neuhuber et al., 1998)and may coordinate swallowing as well as other oropha-ryngeal and tracheal programs (cf. Fischer et al., 1998).The similarly specialized network apparatus of IGLEs inthe antrum may coordinate antral pumping and othergastric emptying activity. This general hypothesis ofIGLE function also would be consistent with the finding(Neuhuber et al., 1995; Dutsch et al., 1998) that IGLEs, atleast those in the esophagus, express calbindin (Kuramotoand Kuwano, 1994; Kressel and Radespiel-Troger, 1999)and calretinin (Kressel and Radespiel-Troger, 1999). Be-cause these proteins are found in rapidly adapting mech-anosensors (Duc et al., 1994), they seem to be well adaptedas a system for following and organizing the relatively fastchanges of the transient motor contractions (measured inseconds) of programs of rhythmic GI motility (periodsmeasured in seconds or minutes). This hypothesis is by nomeans exclusionary—the previously mooted ideas thatIGLEs may be able to mediate axon responses and may bemodulated by neurohumoral signals (see, e.g., Berthoudand Powley, 1992) are potentially complementary. Giventhe structure of IGLEs, including their synaptic contactswith enteric neurons (Neuhuber, 1987) and substanceP-containing vesicles in their terminals (Kressel andRadespile-Troger, 1999), these afferent effects could oper-ate both locally in axon responses or reflexes as well as inconventional vago-vagal reflexes with a central relay. Acapacity to change in response to the local humoral milieuand to operate through local as well as classical reflex
322 F.B. WANG AND T.L. POWLEY

pathways would make IGLEs dynamic mechanisms forcross-coupling motor rhythmicities or response-phase re-lations. In summary, IGLEs appear to be organized tooperate as tension receptors, endings that are capable oftransducing both active and passive changes in force.
Second, IMAs, with their more limited distributions andelongated processes complexed with interstitial cells, maybe tuned more selectively to detect stretch or dilation asopposed to distortions related to periodic motor activity.The local morphologic specializations of IMAs and theirconcentrations at strategic sites also are suggestive. Mostparticularly, the density and crossed or latticed organiza-tion of circular and longitudinal IMAs in the forestomachsuggest analogies with other receptor concentrations inother afferent modalities (e.g., the cone-dense fovea of theretina). Both the density and the distinctive orthogonalorganization of the endings in the two muscle sheetswould be consistent with an exceptional sensitivity to themechanical factors produced by stretch. Because the ratforestomach primarily has a reservoir function, and in-gested nutrients are pocketed in this region in which thehighest density of IMAs is found, it seems reasonable tocorrelate this lattice with stretch detection. Although suchinformation presumably may be integrated into the rhyth-mic motor programs of the stomach, it also may be cou-pled, through various central relays, to responses of recep-tive relaxation or accommodation as well as responsesrelated to ingestion and volume monitoring. BecauseIMAs are associated with the interstitial cell of Cajalnetwork, which is involved in pacemaker activity, IMAsalso may transduce or effect an integration of stretchstimuli and pacemaker signaling.
In addition to the forestomach, IMAs are found in highdensities in sphincters (Kressel et al., 1994; Phillips et al.,1997; Neuhuber et al., 1998; current findings). Such alocation is consistent with the working hypothesis thatIMAs are mechanoreceptors that, compared with IGLEs,are tuned less to rhythmic, coordinated motor activity andare tuned more to relatively static stretch (interrupted byinfrequent phasic changes, such as sphincter opening).Recording the emptying and the redistribution of nutrientboluses at critical sites may apply not only to the IMAsthat are found in exceptional density in the lower esoph-ageal sphincter and the pylorus but also to the relativelyisolated fields of IMAs in circular muscle that we noted inparticular sites along the GI tract. These regular fields ofIMAs in the colon (see Fig. 17) and in the duodenum(Phillips et al., unpublished observations), because of flex-ures and ligamentous attachments at the sites, may besituated at “functional sphincters or valves.” In summary,IMAs appear to be organized to operate as stretch recep-tors that are capable of transducing changes in the lengthof their respective muscle sheets.
Using the topographic profiles to evaluatereorganizations of vagal projections
One of the aims of the current experiment was thedevelopment of a sampling strategy that could be “fitted”to different animals’ GI tracts so that data from differentanimals could be combined or compared. The current re-sults establish that the elastic-grid protocols combinedwith standardized wholemount preparation make suchsurveys practical. The identification of areas of high den-sity, such as the lattice field of IMAs in the forestomach,indicates that data from different animals can be com-
bined effectively without case-to-case variability blurringthe topographic patterns.
Although the details are presented elsewhere, it shouldbe noted that this topographic mapping strategy has beenvalidated by several recent surveys of the GI innervationand its plasticity. For example, the protocol has illumi-nated the patterns of regeneration of vagal afferents ob-served after axotomy (Powley et al., 1997; Phillips et al.,2000) as well as detecting changes during development(Swithers et al., 1999) and the aging process (Phillips etal., 1998). It also has been proven to have good utility incomparing neuronal distributions within the enteric ner-vous system (Phillips et al., 1998; Jarvinen et al., 1999). Inaddition, the sampling protocol has been adapted to themouse not only to provide a comparative inventory of thevagal afferent innervation of another species (Powley etal., 1998) but also to evaluate a specific reorganization ofthe IMA fields associated with a mutation that disruptsthe interstitial cell network of the forestomach (Fox et al.,1998, 1999).
ACKNOWLEDGMENTS
The authors especially acknowledge Robert Phillips forhis expert and particularly extensive help in data analy-sis, graphing, and photography. Joshua Kelly (color pho-tography) and Jeff Mitchell (artwork) also contributedextensively to the project. Helpful comments on earlierdrafts of the material were provided by Elizabeth Bar-onowsky, Charles Bracker, Edward Fox, Michael Jarvi-nen, Robert Meisel, Robert Phillips, Elwood Walls, andGerald Wasserman. This report is based on work submit-ted in partial fulfillment of the Ph.D. requirement(F.B.W., 1995) at Purdue University. Preliminary reportsof portions of the work appeared abstract form at theannual meetings of the Society for Neuroscience (Wangand Powley, 1994) and at the American Gasteroenterologi-cal Association (Powley and Wang, 1995).
LITERATURE CITED
Berthoud H-R, Powley TL. 1992. Vagal afferent innervation of the ratfundic stomach: morphological characterization of the gastric tensionreceptor. J Comp Neurol 319:261–276.
Berthoud H-R, Jedrzejewska A, Powley TL. 1990. Simultaneous labeling ofvagal innervation of the gut and afferent projections from the visceralforebrain with DiI injected into the dorsal vagal complex in the rat.J Comp Neurol 301:65–79.
Berthoud H-R, Kressel M, Neuhuber WL. 1992. An anterograde tracingstudy of the vagal innervation of rat liver, portal vein and biliarysystem. Anat Embryol 186:431–442.
Berthoud H-R, Kressel M, Neuhuber WL. 1995a. Vagal afferent innerva-tion of rat abdominal paraganglia as revealed by anterograde DiI-tracing and confocal microscopy. Acta Anat 152:127–132.
Berthoud H-R, Kressel M, Raybould H, Neuhuber WL. 1995b. Vagal sen-sors in the rat duodenal mucosa: distributions and structure as re-vealed by in vivo DiI-tracing. Anat Embryol 191:203–212.
Berthoud H-R, Patterson LM, Neumann F, Neuhuber WL. 1997. Distribu-tion and structure of vagal afferent intraganglionic laminar endings(IGLEs) in the rat gastrointestinal tract. Anat Embryol 195:183–191.
Blackshaw LA, Grundy D, Scratcherd T. 1987. Vagal afferent dischargefrom gastric mechanoreceptors during contraction and relaxation of theferret corpus. J Auton Nerv Syst 18:19–24.
Duc C, Barakat-Walter I, Droz B. 1994. Innervation of putative rapidlyadapting mechanoreceptors by calbindin- and calretinin-immunoreactive primary sensory neurons in the rat. Eur J Neurosci6:264–271.
Dutsch M, Eichhorn U, Worl J, Wank M, Berthoud H-R, Neuhuber WL.
323VAGAL AFFERENTS TO GI WALL

1998. Vagal and spinal afferent innervation of the rat esophagus: acombined retrograde tracing and immunocytochemical study with spe-cial emphasis on calcium-binding proteins. J Comp Neurol 398:289–307.
Fazan VPS, Lachat J-J. 1997. Qualitative and quantitative morphology ofthe vagus nerve in experimental chagas’ disease in rats: a light micro-scopic study. Am J Trop Med Hygiene 57:672–677.
Fischer A, Canning BJ, Undem BJ, Kummer W. 1998. Evidence for anesophageal origin of VIP-IR and NO Synthase-IR nerves innervatingthe guinea pig trachealis: a retrograde neuronal tracing and immuno-histochemical analysis. J Comp Neurol 394:326–334.
Fox EA, Baronowsky EA, Phillips RJ, Martinson FA, Powley TL. 1998.Selective loss of gastric tension receptors in c-kit mutant mice. SocNeurosci Abstr 24:1124.
Fox EA, Baronowsky EA, Phillips RJ, Powley TL. 1999. Selective loss ofIMA-type mechanoreceptors in mice mutant for steel factor, the c-kitreceptor ligand. Soc Neurosci Abstr 25:1556.
Holst M-C, Powley TL. 1992. Vagal afferent innervation of the proximalduodenum [abstract]. Dig Dis Sci 37:974.
Holst M-C, Kelly JB, Powley TL. 1997. Vagal preganglionic projections tothe enteric nervous system characterized with PHA-L. J Comp Neurol381:81–100.
Iggo A. 1955. Tension receptors in the stomach and the urinary bladder.J Physiol 128:593–607.
Jarvinen MK, Powrozek TA, Wollmann WJ, Powley TL. 1998. Specializa-tions of vagal intraganglionic laminar endings (IGLEs) in the rat stom-ach and duodenum: a quantitative analysis. Soc Neurosci Abstr 24:1123.
Jarvinen MK, Wollmann WJ, Powrozek TA, Schultz JA, Powley TL. 1999.Nitric oxide synthase-containing neurons in the myenteric plexus ofthe rat gastrointestinal tract: distribution and regional density. AnatEmbryol 199:99–112.
Kaneoke Y, Koike Y, Sakurai N, Washimi Y, Hirayama M, Hoshizyama M,Takahashi A. 1995. Gastrointestinal dysfunction in Parkinson’s dis-ease detected by electrogastroenterography. J Auton Nerv Syst 50:275–281.
Kressel M, Radespiel-Troger M. 1999. Anterograde tracing and immuno-histochemical characterization of potentially mechanosensitive vagalafferents in the esophagus. J Comp Neurol 412:161–172.
Kressel M, Berthoud H-R, Neuhuber WL. 1994. Vagal innervation of therat pylorus: an anterograde tracing study using carbocyanine dyes andlaser scanning confocal microscopy. Cell Tissue Res 275:109–123.
Kuramoto H, Kuwano R. 1994. Immunohistochemical demonstration ofcalbindin-containing nerve endings in the rat esophagus. Cell TissueRes 278:57–64.
Mesulam M-M. 1978. Tetramethyl benzidine for horseradish peroxidaseneurohistochemistry: a non-carcinogenic blue reaction-product for vi-sualizing neural afferents and efferents. J Histochem Cytochem 26:106–117.
Neuhuber WL. 1987. Sensory vagal innervation of the rat esophagus andcardia: a light and electron microscopic anterograde tracing study. JAuton Nerv Syst 20:243–255.
Neuhuber WL, Clerc N. 1990. Afferent innervation of the esophagus in catand rat. In: Zenker W, Neuhuber WL, editors. The primary afferentneuron: a survey of recent morpho-functional aspects. New York: Ple-num Press. p 93–107.
Neuhuber WL, Kressel M, Dutsch M, Worl J, Berthoud H-R. 1995. Rela-tionships of IGLEs to enteric glia and neurons in the rat esophagus:further indications of a mechanosensor-local effector role. Soc NeurosciAbstr 21:1633.
Neuhuber WL, Kressel M, Stark A, Berthoud H-R. 1998. Vagal efferentand afferent innervation of the rat esophagus as demonstrated byanterograde DiI and DiA tracing: focus on myenteric ganglia. J AutonNerv Syst 70:92–102.
Nonidez JF. 1946. Afferent nerve endings in the ganglia of the intermus-cular plexus of the dog’s oesophagus. J Comp Neurol 85:177–189.
Phillips RJ, Powley TL. 1998. Gastric volume detection after selectivevagotomies in rats. Am J Physiol 274:R1626–R1638.
Phillips RJ, Baronowsky EA, Powley TL. 1997. Afferent innervation of
gastrointestinal tract smooth muscle by the hepatic branch of thevagus. J Comp Neurol 384:248–270.
Phillips RJ, Baronowsky EA, Powley TL. 1998. Regional effects of aging onvagal endings and myenteric neurons in the GI tract of the Fischer rat.Soc Neurosci Abstr 24:1123.
Phillips RJ, Baronowsky EA, Powley TL. 1999. Vagal afferent reinnerva-tion of the rat GI tract smooth muscle forty-five weeks after completesubdiaphragmatic vagotomy. Soc Neurosci Abstr 25:1688.
Phillips RJ, Baronowsky EA, Powley TL. 2000. Regenerating vagal affer-ents reinnervate gastrointestinal tract smooth muscle of the rat.J Comp Neurol 421:325–346.
Powley TL, Berthoud H-R. 1991. A fluorescent tracer strategy for stainingthe enteric nervous system. J Neurosci Methods 36:9–15.
Powley TL, Wang FB. 1995. Mapping regional distributions of vagal pro-jections to the gastrointestinal tract [abstract]. Gastroenterology 108:A670.
Powley TL, Fox EA, Berthoud H-R. 1987. Retrograde tracer technique forassessment of selective and total subdiaphragmatic vagotomies. Am JPhysiol 253:R361–R370.
Powley TL, Holst M-C, Boyd DB, Kelly JB. 1994. Three-dimensional re-constructions of autonomic projections to the gastrointestinal tract.Microsc Res Tech 29:297–309.
Powley TL, Baronowsky EA, Wollmann WJ, Phillips RJ. 1997. Regenerat-ing vagal afferents reinnervate GI tract smooth muscle of the rat. SocNeurosci Abstr 23:430.
Powley TL, Phillips RJ, Martinson FA, Baronowsky EA, Fox EA. 1998.Vagal afferent terminals in the mouse stomach: types and topographicmaps. Soc Neurosci Abstr 24:1124.
Prechtl JC, Powley TL. 1987. A light and electron microscopic examinationof the vagal hepatic branch of the rat. Anat Embryol 176:115–126.
Robertson B, Grant G. 1985. A comparison between wheat germagglutinin- and choleragenoid-horseradish peroxidase as antero-gradely transported markers in central branches of primary sensoryneurons in the rat with some observations in the cat. Neuroscience14:895–905.
Robertson B, Lindh B, Aldskogius H. 1992. WGA-HRP and choleragenoid-HRP as anterogradely transported tracers in vagal visceral afferentsand binding of WGA and choleragenoid to nodose ganglion neurons inrodents. Brain Res 590:207–212.
Rodrigo J, Hernandez CJ, Vidal MA, Pedrosa JA. 1975. Vegetative inner-vation of the esophagus. II. Intraganglionic laminar endings. Acta Anat92:79–100.
Rodrigo J, De Felipe J, Robles-Chillida EM, Perez Anton JA, Mayo I,Gomez A. 1982. Sensory vagal nature and anatomical access paths toesophagus laminar nerve endings in myenteric ganglia. Determinationby surgical degeneration methods. Acta Anat (Basel) 112:47–57.
Sengupta JN, Kauvar D, Goyal RK. 1989. Characteristics of vagal esoph-ageal tension-sensitive afferent fibers in the opossum. J Neurophysiol61:1001–1010.
Swithers SE, Baronowsky EA, Powley TL. 1999. Presence and distributionof vagal IGLEs and IMAs in stomach of pre-weanling rat pups. SocNeurosci Abstr 25:1555.
Villalta J, Estruch R, Antunez E, Valls J, Urbano-Marquez. A. 1989. Vagalneuropathy in chronic alcoholics: relation to ethanol consumption. Al-cohol Alcoholism 24:421–428.
Walls EK, Wang FB, Holst M-C, Phillips RJ, Voreis JS, Perkins AR,Pollard LE, Powley TP. 1995. Selective vagal rhizotomies: a new dorsalsurgical approach used for intestinal deafferentations. Am J Physiol269:R1279–R1288.
Wang FB. 1995. Inventory and distribution of vagal afferent projections inthe gastrointestinal tract of rat [dissertation]. West Lafayette, IN:Purdue University.
Wang FB, Powley TL. 1994. Taxonomy of vagal afferent projections to thegastrointestinal tract. Soc Neurosci Abstr 20:1375.
Zanone MM, Burchio S, Quadri R, Pietropaolo M, Sacchetti C, Rabbone I,Chiandussi L, Cerutti F, Peakman M. 1998. Autonomic function andantibodies to autonomic nervous structures, glutamic acid decarboxyl-ase and islet tyrosine phosphate in adolescent patients with IDDM.J Neuroimmunol 87:1–10.
324 F.B. WANG AND T.L. POWLEY