Embed Size (px)
Citation preview
Topical Timolol Therapy in Pregnancy:Is It Safe for the Fetus?A.M. WAGENVOORT,1 J.M.G. VAN VUGT,1* M. SOBOTKA,2 AND H.P. VAN GEIJN1
1 Division of Prenatal Diagnosis and Therapy, Department of Obstetrics and Gynecology, University Hospital ‘‘VrijeUniversiteit,’’ 1007 MB Amsterdam, The Netherlands2Department of Pediatric Cardiology, University Hospital ‘‘Vrije Universiteit,’’ 1007 MB Amsterdam, The Netherlands
ABSTRACT At 21 weeks of gestation, a 37-year-old woman was referred to our hospital. The fetusshowed bradycardia and arrhythmia. Because of glau-coma the woman had previously been treated withtimolol eye drops. In this paper a possible associationbetween the timolol eye drops and the fetal cardiacarrhythmia is discussed. Teratology 58:258–262,1998. r 1998 Wiley-Liss, Inc.
Pregnancy in association with treated glaucoma isconsidered to be an unusual entity (Samples and Meyer,’88). The drugs, mostly beta-blockers, that are used totreat glaucoma are topical. Side effects such as bradycar-dia, arrhythmia, myocardial infarction, and congestiveheart failure have been reported following ocular admin-istration of timolol in adults (Munroe et al., ’85;Schneider and Proegler, ’88). Kooner and Zimmerman(’88) advised against the use of beta-blockers in the firsttrimester of pregnancy because one must consider theirpossible harmful effects on the fetus. Because fractionsof ophthalmically applied solutions will be absorbed bydrainage through the nasopharyngeal mucosa, all oph-thalmic topical medication should be considered toproduce systemic blood levels. This paper describes theeffect on the fetal heart rhythm in a case with topicalapplication of timolol, a beta-blocker.
CASE REPORT
A 37-year-old woman was referred to the UniversityHospital ‘‘Vrije Universiteit’’ at 21 weeks of gestation inher second pregnancy because of fetal bradycardia.Before the 21st week of gestation the fetal heartbeatwas regular, as stated by her referring midwife. Herfirst pregnancy 8 years earlier had been uneventful,and she had a spontaneous delivery near term of a girl,with birth weight of 3,100 g.
The woman had been diagnosed with elevated intra-ocular pressure in both eyes, at age 34. She had had nocomplaints then but was examined since her motherhad developed acute glaucoma. She was diagnosedhaving primary glaucoma. Timolol eye drops 0.5%, onedrop in each eye, one time daily, were prescribed. Shehad not applied any compression of the punctum afteradministration. Before and after the start of timololmedication, there were no signs of cardiac problems.
She had a normal ECG. Her pulse rate was 80 beats permin. This medication was continued during her preg-nancy. Chorionic villus sampling at 11 weeks of preg-nancy, because of advanced maternal age, showed anormal female karyotype.
At 21 weeks, a targeted ultrasound examination ofthe fetus was performed. A heart frequency of 74 beatsper min (bpm) was found, with an irregularity of twonormal beats followed by a pause, as shown by M-modeultrasound (Fig. 1). There was no suspicion of struc-tural anomalies, including absence of fetal hydrops.The family history revealed no cardiac diseases. Anti-SSA (anti-Ro) and Anti-SSB (anti-La) was negative inthe blood of the mother.
At 25 weeks and 5 days, the timolol medication wasreduced to 0.25% times daily on our request. Three dayslater the heart rate of the fetus increased to 96 bpmwith the irregularity as described before, and 1 weeklater, the fetal heart rate was 120 bpm and the irregu-larity had disappeared, except for occasional ectopicbeats (Fig. 2).
At 29 weeks and 4 days, the medication was stoppedafter consulting the ophthalmologist. The rising intra-ocular pressure was acceptable. Three days after com-plete withdrawal of the medication, the fetal heart ratewas around 130 bpm. This frequency with occasionalectopic beats remained until delivery.
At 39 weeks and 6 days, a girl of 3,025 g was born,with Apgar scores of 8 and 10 after 1 and 5 min,respectively, and with an umbilical arterial pH of 7.30.Directly after the baby was born, blood was taken fromthe umbilical cord to evaluate if the genotype CYP2D6A and CYP2D6 B belonged to the ‘‘wild type,’’ to excludean oxygenation capacity problem in the liver andbecause of this accumulation of the drug. After birththe baby demonstrated cardiac arrhythmia with heartfrequencies over 200 bpm, diagnosed as right ventricletachycardia with atrial extra systole (Fig. 3). A cardiacanomaly was not present on ultrasound. Becauseof the risk that the heart frequency might persist,
*Correspondence to: J.M.G. van Vugt, M.D., Division of PrenatalDiagnosis and Therapy, Department Obstetrics and Gynecology, Uni-versity Hospital ‘‘Vrije Universiteit,’’ P.O. Box 7057, 1007 MB Amster-dam, The Netherlands. E-mail: [email protected]
Received 7 May 1998; Accepted 26 August 1998
TERATOLOGY 58:258–262 (1998)
r 1998 WILEY-LISS, INC.
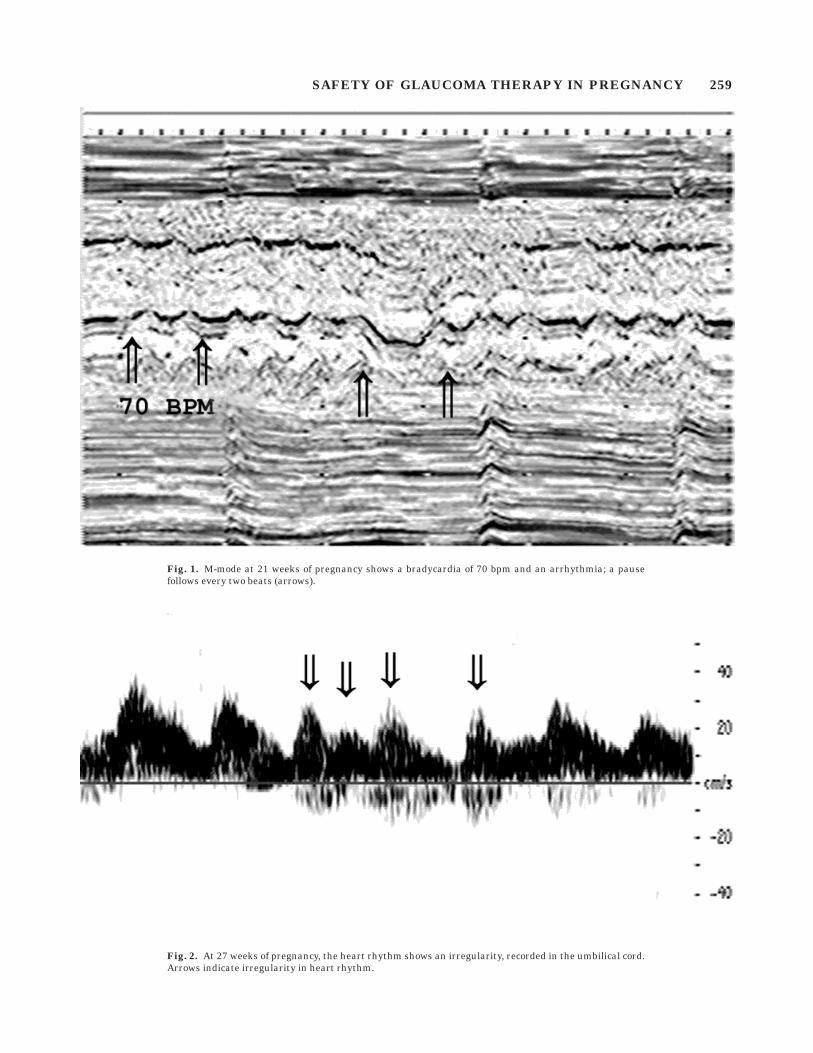
Fig. 2. At 27 weeks of pregnancy, the heart rhythm shows an irregularity, recorded in the umbilical cord.Arrows indicate irregularity in heart rhythm.
Fig. 1. M-mode at 21 weeks of pregnancy shows a bradycardia of 70 bpm and an arrhythmia; a pausefollows every two beats (arrows).
SAFETY OF GLAUCOMA THERAPY IN PREGNANCY 259
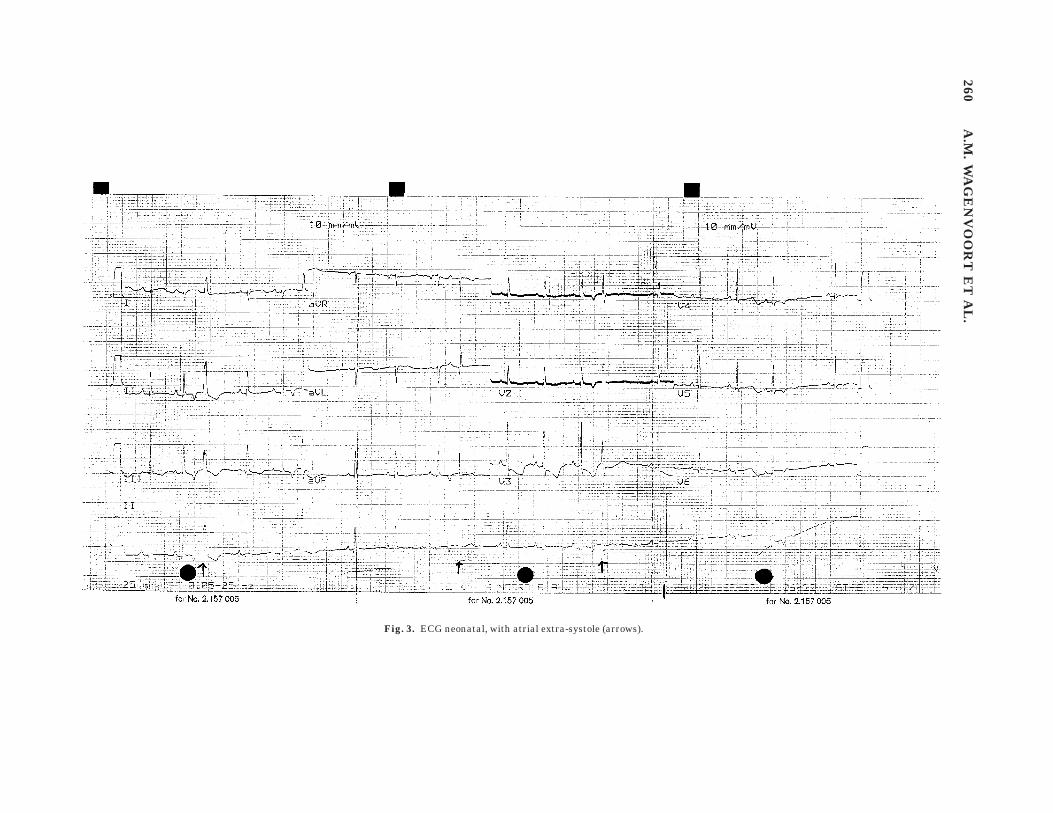
Fig. 3. ECG neonatal, with atrial extra-systole (arrows).
260A
.M.
WA
GE
NV
OO
RT
ET
AL
.
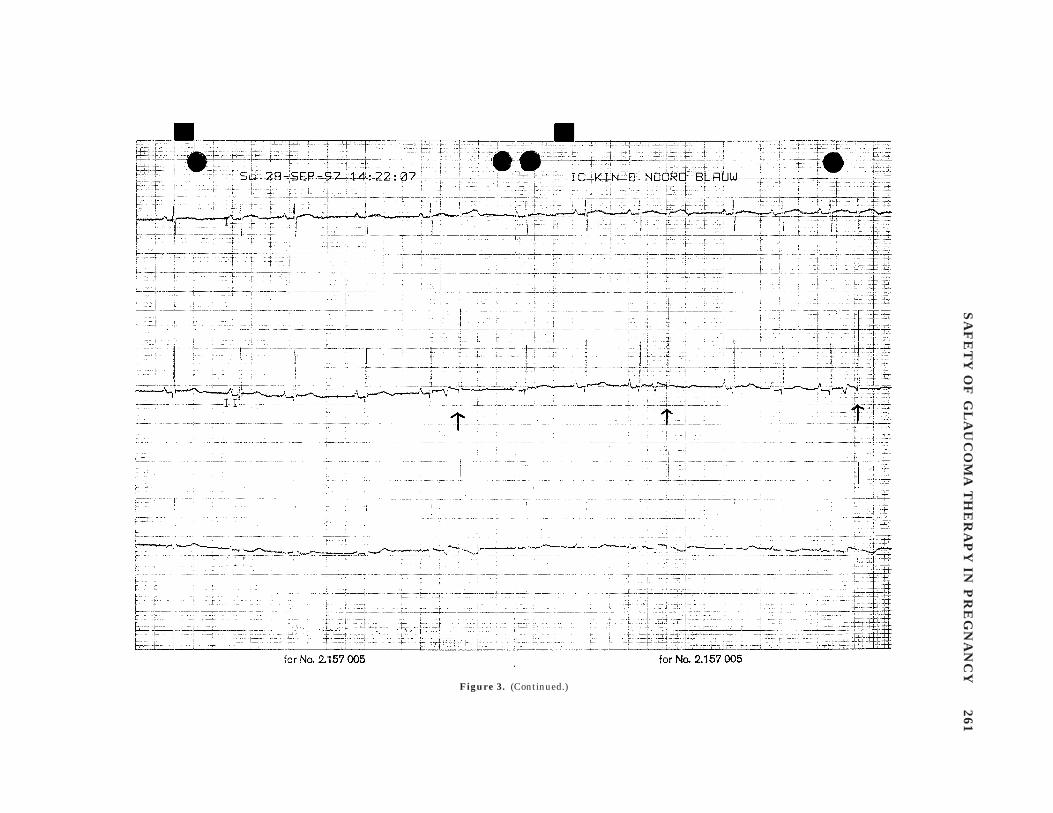
Figure 3. (Continued.)
SA
FE
TY
OF
GL
AU
CO
MA
TH
ER
AP
YIN
PR
EG
NA
NC
Y261

the neonate was digitalized. Two months after birththe baby is developing well. The patient started hermedication again 1 month after giving birth to herdaughter.
DISCUSSION
The observed bradycardia and arrhythmia at 21weeks of pregnancy cannot be explained by cardiacabnormalities or a known genetic syndrome. There-fore, the observed abnormal heart rhythm may beexplained as an adverse effect of the topically adminis-tered timolol, as described in adults. Timolol is anonselective beta-blocker. It is said to be 10–12 timesmore potent than propanolol in blocking cardiac chro-notropic and inotropic effects (Van Petten, ’80). An-other report (Akingbehin and Sunder Raj, ’90) showedthat in adults systemic side effects of the heart havebeen reported, such as bradycardia, arrhythmia, andheart failure. From the topically administered eyedrops 80% of the volume drains through the nasolacri-mal duct and is absorbed systemically. Because theocular instillation is very similar to intravenous admin-istration, the topical timolol bypasses the hepaticmetabolism. Orally administered beta-blockers haveto undergo the first-pass effect, and most of the drugmay be inactivated. This may be explain the sideeffects of topical beta-blockers despite the lower oculardose.
Studies by Touw and Breimer (’97) reveal anotherexplanation, which could be the deficiency of theCYP2D6A and CYP2D6B enzymes. If these two en-zymes are not present, the normal oxidation capacityfor timolol in the liver will than be disturbed, andaccumulation of the drug could occur. The genotype ofthis baby is the normal ‘‘wild type.’’ This means thatthe oxidation capacity of drugs in the liver was normal.Van Petten (’80) showed in sheep that timolol crossesthe placenta and blocks the usual rebound fetal tachy-cardia which follows cord occlusion. Kooner and Zim-merman (’88) revealed that drugs that are given to thepregnant woman may cross the placenta and harm thefetus. Only the unbound drug is active and available topass through the placenta. During pregnancy thematernal blood volume increases and alphafetoproteinmay interfere with normal drug-binding profiles. Thedrugs that pass through the placenta will depend ondrug characteristics. Lipid-soluble, nonionized, lowmolecular weight drugs will readily cross the placentaand enter the fetal circulation.
Timolol (C13 H24N 4 O3 S) has a low molecular weightof 316.4 Daltons. Timolol is excreted into breast in milkand may cross membranes as well. Once the drug hasentered the fetal circulation, it may be excreted intothe amniotic fluid from the kidneys, the lungs, or theskin. The length of fetal exposure to an administereddrug may be much longer than it will be in adults
because of recirculation through the swallowing andbreathing movements of the fetus and reexcretion bythe fetal kidneys (Kooner and Zimmerman, ’88). Thehalf-life of timolol in adults will be 4–5 hr. Because ofthe mechanism mentioned before, the smaller bloodvolumes, and immature metabolic systems of the fetus,the plasma levels of timolol may exceed the therapeuticrange, which leads to an increased risk of adversesystemic effects and a half-life that will be 4–6 timeslonger than that of adults (Akingbehin and SunderRaj, ’90).
Because of the preconceptional intake of the eyedrops, it is possible that the drugs interfere with thedevelopment of the embryonic heart. In the secondtrimester, the dose of timolol (0.5%) has been enough toblock conduction (Cottle et al., ’83). When the dose oftimolol had been halved, there was an increase in fetalheart rate. After the drug had been stopped, the brady-cardia disappeared. This baby had bradycardia, arrhyth-mia, and postpartum paroxysmal tachycardia withremaining arrythmia. There is always the possibilitythat the cardiac conduction disorder had nothing to dowith the use of timolol. One could speculate, however,that because of relatively high dose of timolol early inpregnancy, the cardiac conduction in the embryo or thefetus, may have changed, so a conduction disorder hasremained.
When a woman on glaucoma therapy becomes preg-nant, most of the time it is possible to interrupt thetherapy during pregnancy. Young pregnant womenoften will tolerate slight increases in intraocular pres-sure well, and treatment may be deferred until deliveryof the infant (Samples and Meyer, ’88), so that theeventual harm to the fetus can be reduced as much aspossible.
LITERATURE CITED
Akingbehin T, Sunder Raj P. 1990. Ophthalmic topical beta blockers:review of ocular and systemic adverse effects. J Toxicol Cutan Ocul9:131–147.
Cottle MKW, Van Petten GR, Van Muyden P. 1983. Maternal and fetalcardiovascular indices during fetal hypoxia due to cord compressionin chronically cannulated sheep. Am J Obstet Gynecol, 146:678–685.
Kooner KS, Zimmerman TJ. 1988. Antiglaucoma therapy duringpregnancy—Part 1. Ann Ophthalmol 20:166–169.
Munroe WP, Rindone JP, Kershner RM. 1985. Systemic side effectsassociated with the ophthalmic administration of timolol. DrugIntell Clin Pharm 19:85–89.
Samples JR, Meyer SM. 1988. Use of ophthalmic medications inpregnant and nursing woman. Am J Ophthalmol 106:616–623.
Schneider H, Proegler M. 1988. Placental transfer of b-adrenergicantagonists studied in an in vitro perfusion system of humanplacental tissue. Am J Obstet Gynecol 159:42–47.
Touw DJ, Breimer DD. 1997. Het cytochroom P450-enzymsysteem.Pharm Weekbl [Sci] 28:948–963.
Van Petten GR. 1980. Cardiovascular effects of timolol in the unanaes-thetized pregnant ewe and fetus. Proc West Pharmacol Soc 23:191–195.
262 A.M. WAGENVOORT ET AL.







![T J Journal of Clinical Toxicology · myopic shift [8,9]. In most cases of TiACG, symptoms resolved soon aftercessation of the drug. Topical timolol, dorzolamide, brimonidine, and](https://img.pdfslide.us/doc/110x75/5ebd358e4668e26a432d4319/t-j-journal-of-clinical-toxicology-myopic-shift-89-in-most-cases-of-tiacg-symptoms.jpg)