Embed Size (px)
Citation preview

Top 10 Prescribing Mistakes Providers Frequently Make
Lara Groetzinger, PharmD, BCCCP
Unit-based clinical pharmacist
Medical ICU

Objectives
• Identify mistakes commonly made when ordering and prescribing medications, including high-alert medications
• Evaluate the impact of prescribing errors on patient outcomes
• Develop strategies on how to mitigate prescribing errors and avoid pharmacist phone calls
2

Prescribing Errors • Common but preventable events • Account for 70% of medication errors that could potentially result in
adverse events– More frequently made by junior prescribers
• Medication errors can occur during various stages of the medication use process– Ordering– Prescribing– Interpreting – Dispensing – Administering
3Pharm J. 2019;302(7922)Tariq RA, Vashisht R, Scherbak Y. Medication Errors. [Updated 2020 Jun 15]. Br J Clin Pharmacol. 2009 Jun;67(6):624-8.
~50%

4
ISMP High Alert Medication– Drugs that bear a heightened
risk of causing significant patient harm when used in error
– Mistakes may or may not be more common but consequences of an error are clearly more devastating
http://www.ismp.org/Tools
=ISMP high alert medication
10. Ordering errors
5

“It’s not what you know, its how you order it!”
Common ordering mistakes
Wrong drug
Wrong dose
Wrong time
Wrong frequency
Wrong route
Real ordering mistakes
6

Strategies to Avoid Ordering Errors
• Wrong drug – Tall Man Letters (Look-alike-sound-alike medications)
• Wrong dose/frequency – Computerized advice to guide the prescription of
optimal dosages
– Dose range warnings
• Wrong timing – Know your hospital’s standard medication administration times
(SMAT)
• Electronic methods – Computerized physician order entry (CPOE)
– Clinical decision support system (CDSS)
• Other strategies – Minimize verbal orders
– Utilize your pharmacist
7 Br J Clin Pharmacol. 2009 Jun;67(6):624-8.

Wrong Route
8

9. Wrong Dosage Form
9

Dosage Forms : which do you pick?
10
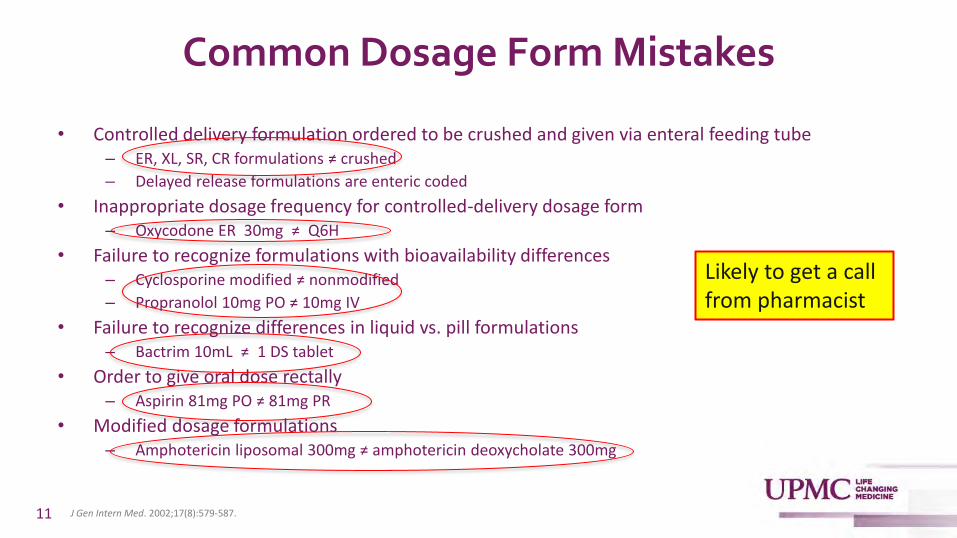
Common Dosage Form Mistakes
• Controlled delivery formulation ordered to be crushed and given via enteral feeding tube – ER, XL, SR, CR formulations ≠ crushed
– Delayed release formulations are enteric coded
• Inappropriate dosage frequency for controlled-delivery dosage form– Oxycodone ER 30mg ≠ Q6H
• Failure to recognize formulations with bioavailability differences– Cyclosporine modified ≠ nonmodified
– Propranolol 10mg PO ≠ 10mg IV
• Failure to recognize differences in liquid vs. pill formulations – Bactrim 10mL ≠ 1 DS tablet
• Order to give oral dose rectally – Aspirin 81mg PO ≠ 81mg PR
• Modified dosage formulations – Amphotericin liposomal 300mg ≠ amphotericin deoxycholate 300mg
11 J Gen Intern Med. 2002;17(8):579-587.
Likely to get a call from pharmacist

Immunosuppressant Dosage Form Considerations
Cyclosporine • Non-modified: SandImmune®
– More erratic and incomplete absorption= lower bioavailability
• Modified: Gengraf® and Neoral® – Increased absorption and
bioavailability (~30%) compared to non-modified
– More commonly used in practice
• NOT bioequivalent and cannot be used interchangeably
• No specific dose conversion– Monitor plasma concentrations
frequently
Mycophenolate • Mycophenolate mofetil (CellCept®)
– Liquid formulation available for enteral feeding tubes
• Mycophenolate sodium enteric-coated (Myfortic®) delayed-release – DO NOT CRUSH– May have less gastrointestinal side effects
• NOT bioequivalent and cannot be used interchangeably
• Myfortic® 180mg = CellCept® 250mg
12 Lexicomp Online 2020. Cyclosporine: Drug information. UpToDate.Lexicomp Online 2020. Mycophenolate: Drug information. UpToDate.

Trimethoprim (TMP) /Sulfamethoxazole (SMX) Bactrim®
Tablet (mg/tab) Oral Liquid IV (undiluted)
SS DS SS (10mL) DS (20mL)
Sulfamethoxazole 400mg 800mg 400mg 800mg 80mg/mL
Trimethoprim 80mg 160mg 80mg 160mg 16mg/mL
Dose for 5mg/kg Q8H in 70kg patient
2 DS tablets by mouth Q8H 40mL by mouth Q8H 350mg IV Q8H
13
SS= single strengthDS=double strength
• 5:1 Ratio (SMX:TMP)• Weight-based doses based on TMP component• DS= 160mg TMP
Lexicomp Online 2020. Trimethoprim-sulfamethoxazole: Drug information. UpToDate.

14
Divalproex Sodium, Sodium Valproate, Valproic Acid
• Valproic acid– Protonated form
– Immediate release (IR): 250mg IR capsule
• Valproate sodium – Sodium salt of valproic acid
– Ex: 250mg/5mL oral solution, 100mg/mL IV solution
• Divalproex sodium – Compound containing sodium valproate and
valproic acid
– Delayed release (DR): Depakote® 125mg DR sprinkle capsule; Depakote® 125mg,DR tablet
– Depakote ER® 250mg, 500mg ER tablet (24-hour)
• All expressed in terms of valproic acid activity
• Not AB-rated so NOT interchangeable – IR = 3-4x/day
– DR= 2-3x/day
– ER= 1x/day
• Convert to IV→ use same oral TDD and divided every 6 hours – Ex: patient on 1000mg ER at
bedtime, now NPO→ convert to 250mg IV Q6H
TDD= total daily dose Lexicomp Online 2020. Valproate: Drug information. UpToDate, Inc.

8. Drug Monitoring Errors
15

Common Drug Monitoring Mistakes
• Ordering of drug levels just because they exist
• Inappropriate timing of drug level
– Not at steady state
• Wrong type of level (trough vs peak)
• Unfamiliarity with therapeutic target
• Total vs. free levels
• Failure to take into consideration the clinical context
– Treat the patient not the number
• Failure to recognize drug-lab interactions 16
Phenobarbital
Vancomycin
Voriconazole
Aminoglycosides
Digoxin
Phenytoin
DOACs/DTIs

17
Drugs with Ability to Utilize Therapeutic Drug Monitoring (TDM)*
• Antibiotics– Aminoglycosides – Vancomycin
• Azole antifungals – Voriconazole – Posaconazole– Itraconazole– Isavuconazole
• Cardiovascular – Digoxin – Lidocaine – Procainamide
• Immunosuppressants – Tacrolimus – Cyclosporine – Sirolimus
• Anticonvulsants– Phenytoin/Fosphenytoin– Carbamazepine – Valproic acid – Phenobarbital/primidone– Lamotrigine– Levetiracetam– Oxcarbazepine
• Other– Lithium– Theophylline
Clinical Pharmacokinetic and Pharmacodynamic Concepts. In: Bauer. Applied Clinical Pharmacokinetics, 3e New York, NY: McGraw-Hill
*Not comprehensive

TDM Steps
18
1. Obtain drug level
• Is this drug a candidate for TDM?
• What will I do with the level?
2. Interpret drug level
• PK/PD
• Timing
• Therapeutic range
• Clinical context
3. Adjust dosing regimen (if necessary)
• Ask your clinical pharmacist 🙂
• Linear PK calculation
• Bayesian PK programs
4. Repeat (only if necessary)

Time
Co
nce
ntr
atio
n
TDM Terminology
CMAX (Peak)
CMIN (Trough)
Random
AUC
AUC= area under curve
Aminoglycosides
Vancomycin
AminoglycosidesVancomycinImmunosuppressantsPhenytoinAzoles
19

Steady-State
Time
Co
nce
ntr
atio
n
Steady-state
12
34
5
Number of doses
Time to steady state: (without a loading dose)
➢ Vancomycin: 4-5 doses➢ Digoxin: 5-7 days ➢ Phenytoin: 3-5 days ➢ Valproic acid: 2-4 days➢ Phenobarbital: 2-3 weeks ➢ Voriconazole: 5-7 days
20 Clinical Pharmacokinetic and Pharmacodynamic Concepts. In: Bauer. Applied Clinical Pharmacokinetics, 3e New York, NY: McGraw-Hill

7. Errors in Opioid Prescribing
21

Common Opioid Prescribing Errors
• Failure to consider drug-specific factors – Lack of knowledge about equianalgesic dosing – Inappropriate dosing – Confusion between dosage forms – Lack of understanding of pharmacokinetic properties
• Failure to consider patient-specific characteristics– Risk factors for adverse drug reactions (ADRs)– Organ failure– Opioid tolerance vs. opioid naïve
• Patient controlled analgesia (PCA) errors• Allergies and cross-tolerance
22

Equianalgesic Dosing
• Fentanyl is 100x more potent than morphine*
• 1mg IV hydromorphone ~7mg IV morphine~20mg PO morphine*– >1mg contributed to 70% of preventable ADR reports involving hydromorphone submitted to PA patient safety authority
23
Equianalgesic Dosing Table (mg)*
Drug Oral IV
Buprenorphine 0.4 (SL) 0.3
Codeine 100 -
Fentanyl - 0.1
Hydrocodone 30 -
Hydromorphone 7.5 1.5
Morphine 30 10
Oxymorphone 10 -
Oxycodone 20 -
Simple Opioid Conversion Steps:1. Calculate total 24-h opioid dose of each different opioid2. Convert total 24-h dose of each opioid to an equivalent
dose in oral morphine equivalents using the table. 3. Add equivalent doses of each opioid together to get the
total daily oral morphine equivalent (OME) dose4. Determine the dose of the new opioid regimen equal to
the calculated daily OME using the table5. Reduce calculated dose of new opioid by 25–50% to
prevent overdose from incomplete cross-tolerance between opioid
*doses are approximate and intended to be used as a general guide
https://accesspharmacy.mhmedical.com/content.aspx?bookid=667§ionid=43490030.McPherson, MLM. In: Demystifying Opioid Conversion Calculations: A Guide for Effective Dosing. Bethesda, MD: American Society of Health-System Pharmacists;2009:chap 5
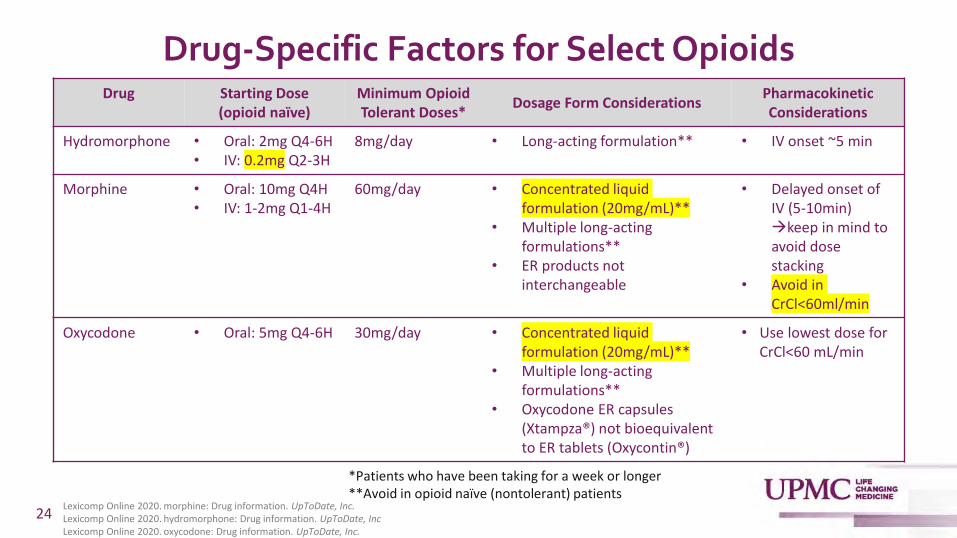
Drug-Specific Factors for Select OpioidsDrug Starting Dose
(opioid naïve)Minimum Opioid Tolerant Doses*
Dosage Form ConsiderationsPharmacokinetic Considerations
Hydromorphone • Oral: 2mg Q4-6H• IV: 0.2mg Q2-3H
8mg/day • Long-acting formulation** • IV onset ~5 min
Morphine • Oral: 10mg Q4H• IV: 1-2mg Q1-4H
60mg/day • Concentrated liquid formulation (20mg/mL)**
• Multiple long-acting formulations**
• ER products not interchangeable
• Delayed onset of IV (5-10min) →keep in mind to avoid dose stacking
• Avoid in CrCl<60ml/min
Oxycodone • Oral: 5mg Q4-6H 30mg/day • Concentrated liquid formulation (20mg/mL)**
• Multiple long-acting formulations**
• Oxycodone ER capsules (Xtampza®) not bioequivalent to ER tablets (Oxycontin®)
• Use lowest dose for CrCl<60 mL/min
24
*Patients who have been taking for a week or longer**Avoid in opioid naïve (nontolerant) patients
Lexicomp Online 2020. morphine: Drug information. UpToDate, Inc.Lexicomp Online 2020. hydromorphone: Drug information. UpToDate, IncLexicomp Online 2020. oxycodone: Drug information. UpToDate, Inc. .

25
Patient-Specific Factors to Consider • Comorbid risk factors for respiratory
depression – Age >65
– Cardiac disease
– Obstructive sleep apnea
– Obesity
– COPD
• Opioid naïve – Avoid fentanyl patch
– Avoid long-acting agents initially
• Treatment of acute pain – Avoid fentanyl patch
• Allergies– Fentanyl does not cross-react with morphine
or codeine derivatives
• Renal failure – Avoid morphine
• Metabolites can accumulate, lower seizure threshold and cause neurotoxicities
• Codeine is metabolized to morphine
• Opium tincture contains morphine
– Avoid meperidine
• Metabolite accumulation may cause seizures
• Patient controlled analgesia (PCA)– Avoid the use of basal rates with PCA for
pain control of an opioid-naïve patient
– Utilize standardized PCA order sets
– Limit verbal orders
Am J Health-Syst Pharm. 2008; 65:1184-91JAMA Intern Med. 2015 Apr;175(4):608-15. BMJ Open. 2018; 8(12): e024086.

6. Errors in Anticoagulation Prescribing
26
Common Anticoagulation Prescribing Mistakes
• Inappropriate dosing – Direct oral anticoagulants (DOACs)
• Inappropriate dose adjustment
• Drug-food interactions
• Mistakes when transitioning between agents
• Inappropriate prescribing of heparin protocols
• Monitoring errors
27

Inappropriate DOAC Dosing is Common and Leads to Worse Outcomes
Inappropriate DOAC Dosing
• Described in up to 39% of patients
– Underdosing >overdosing
• Risk factors for underdosing
– Older age
– Renal failure
– Outpatient prescriptions (vs. inpatient)
– Higher CHA2DS2VASc score
– Higher HAS-BLED score
Associated Outcomes • Increased cardiovascular
hospitalization– HR: 1.26 (95% CI: 1.07 to 1.5)
• Higher rate of VTE recurrences– HR: 10.5 (95% CI: 1.28 to 85.9)
• Composite stroke, MI– HR: 1.57 (95% CI: 1.34 to 1.83)
• Higher bleeding rates– HR: 1.63 (95% CI: (1.14-2.34)
• All-cause mortality – HR: 1.91 (95% CI: 1.02-3.6)
28J Am Coll Cardiol. 2016;68(24):2597-2604.Thromb Haemost. 2017;117(2):382-389.Am J Med. 2019;132(7):847-855.e3
J Am Heart Assoc. 2020;9(6):e014108.J Pharm Health Care Sci. 2020;6:2.Front Pharmacol. 2018;9:1220

Appropriate Apixaban Dosing for Select Indications
Indication Usual Dose Dose Adjustment Indications
Hemodialysis Clinical Trial Data
Atrial Fibrillation 5mg BID
2.5 mg BID iftwo of the following
three are met:• SCr > 1.5 mg/dL• Age ≥ 80 years• Weight ≤ 60 kg
No dosage adjustment
necessary unless:• Age ≥ 80 years OR• Weight ≤ 60 kg→ reduce to 2.5 mg
BID
Excluded patients with:
• SCr>2.5 mg/dL OR
• CrCl <25 mL/minute
Deep Venous Thrombosis or Pulmonary Embolism
10mg BID x 7 days→ 5mg BID
No dosage adjustment is recommended by the manufacturer for any degree of reduced kidney function.
29
BID= twice dailySCr- serum creatinineCrCl= creatinine clearance
Lexicomp Online 2020. Apixaban: Drug information. UpToDate, Inc.

Appropriate Rivaroxaban Dosing for Select Indications
30
Indication Usual Dose Dose Adjustment Indications
Hemodialysis Clinical Trial Data
Atrial Fibrillation
20mg daily CrCl >50 mL/min: • No dosage
adjustmentCrCl 15 to 50 mL/min:• 15 mg once daily
with foodCrCl <15 mL/min:• Avoid use
Avoid use
Patients with CrCl<15 mL/min were excluded
Deep Venous Thrombosis or Pulmonary Embolism
15mg BID x 21 days → 20mg daily
CrCl ≥30 mL/min:• No dosage
adjustment CrCl <30mL/min:• Avoid use
Patients with CrCl<30 mL/min were excluded
Lexicomp Online 2020. Rivaroxaban: Drug information. UpToDate, Inc.
BID= twice dailyCrCl= creatinine clearance

31
Transitioning Between Select Agents
From Heparin (UFH)– Apixaban/rivaroxaban/
enoxaparin should be started immediately after discontinuing the UFH infusion
To Heparin (UFH)– Initiate UFH at the time the
next dose of apixaban/ rivaroxaban/ edoxaban is due
– Initiate UFH 6-12 hours after last enoxaparin injection (24 hours if Q24H dosing)
– Initiate UFH 18-24 hours after the last fondaparinux injection
From Warfarin– Apixaban/dabigatran can be
started once warfarin has been stopped and INR is < 2
– Rivaroxaban can be started once warfarin has been stopped and the INR is < 3
– Edoxaban can be started once the INR is ≤ 2.5
To Warfarin – Discontinue DOAC and initiate
warfarin at the time the next dose would have been given (6pm)
– Consider initiation of parenteral anticoagulant if indicated
From Enoxaparin – Initiate apixaban/rivaroxaban/
edoxaban/ dabigatran 0-2 hours before the next dose of enoxaparin is due
To Enoxaparin – Initiate enoxaparin at the time
the next dose of apixaban/ rivaroxaban/edoxaban is due
Lexicomp Online 2020. Apixaban: Drug information. UpToDate, Inc.Lexicomp Online 2020. Rivaroxaban: Drug information. UpToDate, Inc.Lexicomp Online 2020. Edoxaban: Drug information. UpToDate, Inc.

UPMC Heparin Protocols: No DOAC Interference
32
Nomogram Bolus Dosing(Maximum)
Initial Dosing(Rate not to exceed)
Goal aPTT (seconds)
Goal Anti-Xa activity (units/ml)
Stroke/EP/VAD/High-Risk Bleed
N/A 8 units/kg/hr (1600 units/hr)
59-72 0.25-0.35
Afib/Post-Op 60 units/kg(10,000 units)
10 units/kg/hr (1600 units/hr)
68-82 0.3-0.45
UA/NSTEMI 60 units/kg(4,000 units)
12 units/kg/hr (1000 units/hr)
68-96 0.3-0.6
DVT/PE 80 units/kg(10,000 units)
18 units/kg/hr (1600 units/hr)
68-106 0.3-0.7
Lowest dose and goal anti-Xa, never a bolus
Highest Anti-Xa goal
Clin Appl Thromb Hemost. 2018;24(2):310-316.

Wait 72 hours before obtaining anti-Xa levels
Select DOACs cause falsely elevated anti-Xa reading
Order: Heparin IV (DOAC Interference) PowerPlan
A fixed weight-based IV UFH infusion (without bolus) based upon indication
Patient receiving an interacting DOAC in prior 72 hours
…patient needs interim anticoagulation…heparin is selected…
UPMC Heparin Protocols: DOAC Interference
Formulary DOACs that interact with anti-Xa:• Apixaban (Eliquis®)• Edoxaban (Savaysa®)• Rivaroxaban (Xarelto®)
No titration of the drip or Anti-Xalevels within first 72 hours!
Ann Pharmacother. 2020. [published online ahead of print, 2020 Sep 4] doi:10.1177/1060028020956271

5. Drug Allergy Errors
34

Mistakes Involving Drug Allergies
Common Mistakes
• Inaccurate history or documentation • Inadvertently overlooking a patient’s
drug allergy • Bypass of CPOE and Clinical decision
support system (CDSS) alerts– Failure to document reason for CDSS
override– Inappropriate bypass
• Failure to understand cross-reactivity – Inappropriate substitution of:
• Less effective agent • More toxic agent• More costly agent
• Failure to investigate reaction– True allergy vs. side effect
PA Patient Safety Reporting System
• Total of 854 allergy-related preventable events – 37% Anti-infectives – 15% Opioid analgesics – 10% Non-opioid analgesics
• Over half (56%) reached the patient – 87% of these passed through two or
more stages • Patient history→ allergy
documentation→ ordering→verifying→ administering
35
76%
Pharmacotherapy. 2003;23(7):855-860.PA-PSRS https://patientsafetyj.com/index.php/patientsaf/article/view/med-allergies/19

Bypass of Clinical Decision Support Alerts
36
Failure to document override reason:
Potentially inappropriate bypass:
Likely to get a call from pharmacist
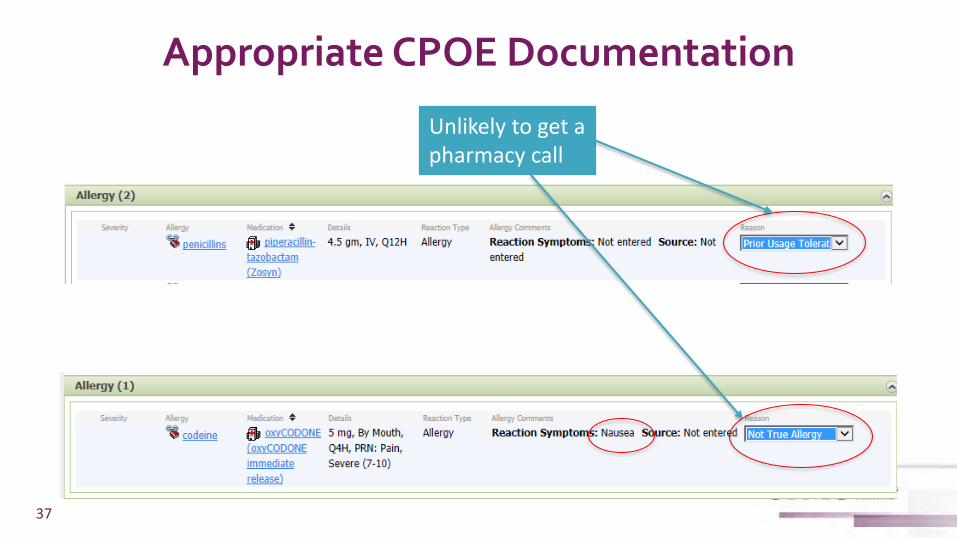
Appropriate CPOE Documentation
37
Unlikely to get a pharmacy call

A Penicillin-Allergy Label has Serious Consequences
• Most common drug allergy reported in medical records – >95% of patients labeled with penicillin allergy can safely receive penicillin when they are
appropriately and safely evaluated
• Individual patient implications – Prescribed less effective therapies – Receive more toxic therapies – Use of broad-spectrum antibiotics – More postoperative surgical-site infections
• Public health implications – Antibiotic resistance – Higher rates of C. difficile infection – Use of more costly agents – Increased length of hospital stays
38 N Engl J Med 2019;381:2338-51.
Vancomycin
Vancomycin, Clindamycin, Fluoroquinolones
Carbapenems
Carbapenems, Aztreonam
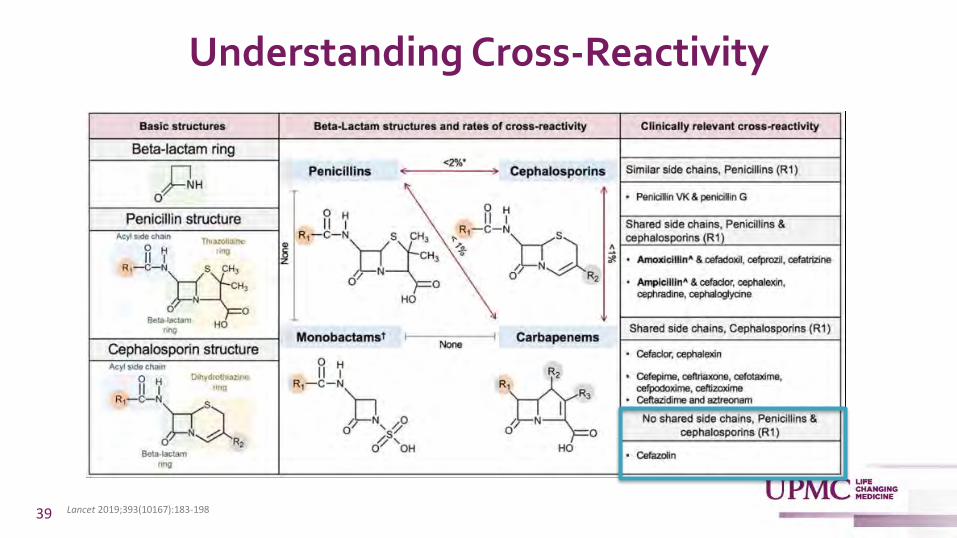
Understanding Cross-Reactivity
39 Lancet 2019;393(10167):183-198

What About Cefazolin?
• Study of 131 patients with IgE-mediated reactions to penicillin (mostly anaphylaxis) + positive skin test – One patient (0.8%) had a positive
skin test to cefazolin • Also had a positive result to all
other reagents tested including aztreonam and carbapenems
– Authors conclude possible allergy to β-lactam ring
• Cefazolin hypersensitivity is a selective allergy – Not expected to cross-react with
other cephalosporins and/ or penicillins
– See allergy management pathway
40J Allergy Clin Immunol Pract 2020;8:1989-93.Allergy 2018, 73, 1833–1841.J. Allergy Clin. Immunol. Pract. 2016, 4, 1232–1236.

41
UPMC Pathway for Evaluation and Management of Penicillin Allergy

UPMC Data: Impact of a Beta-Lactam Allergy Evaluation and Management Pathway on Aztreonam Utilization
42
~$363,000 cost savings
Adapted with permission from McCreary et al

4. Drug-Drug Interactions
43
Common Medications with Significant Drug-Drug Interactions (DDIs)
• DOACs
• Warfarin
• Azole antifungals
• Antiepileptics
44

Pharmacokinetic Drug-Drug Interactions
Metabolism• Cytochrome P450 (CYP) are enzymes
that play a major role in drug metabolism
• CYP450 inhibitors– Decrease metabolism of other drugs
(substrates) metabolized by the same enzyme
– Increase substrate levels→ potential toxicity
• CYP450 inducers– Increase metabolism of other drugs
(substrates) metabolized by the same enzyme
– Decrease substrate levels→ potential therapeutic failure
Absorption• P-glycoprotein (P-gp) is an efflux
transporter located in the small intestine and other sites
• P-gp inhibitors– Inhibit efflux of substrate and increases
bioavailability– Increase substrate levels→ potential
toxicity
• P-gp inducers – Promote efflux of substrate and decreases
bioavailability– Decrease substrate levels→ potential
therapeutic failure
45
Takeaway: Inhibitors Increase & inDucers Decrease
Hematology Am Soc Hematol Educ Program. 2018;2018(1):339-347.Horn JR. Important Drug Interactions & Their Mechanisms. In: Katzung BG. eds. Basic & Clinical Pharmacology, 14e. McGraw-HillBlood. 2018;132(21):2230-2239.
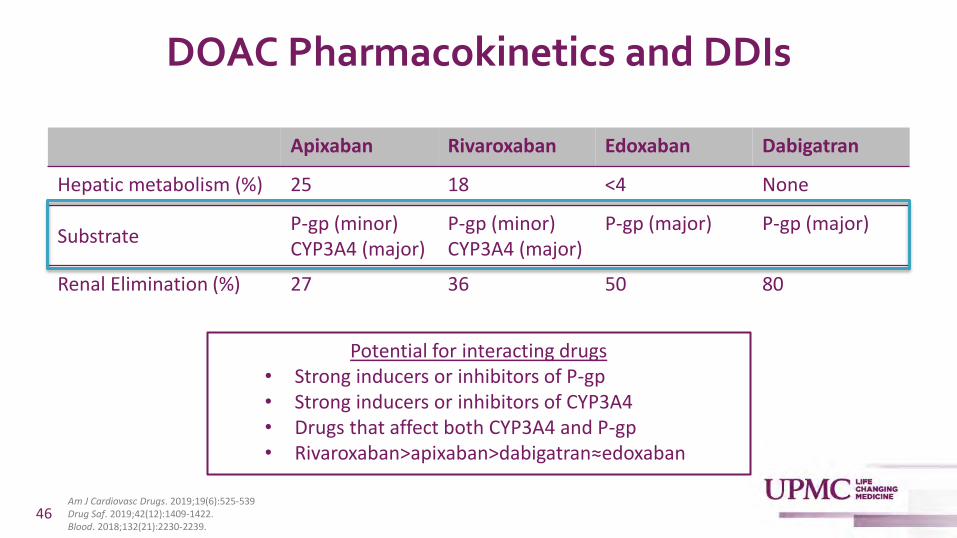
DOAC Pharmacokinetics and DDIs
46
Apixaban Rivaroxaban Edoxaban Dabigatran
Hepatic metabolism (%) 25 18 <4 None
Substrate P-gp (minor) CYP3A4 (major)
P-gp (minor) CYP3A4 (major)
P-gp (major) P-gp (major)
Renal Elimination (%) 27 36 50 80
Potential for interacting drugs • Strong inducers or inhibitors of P-gp• Strong inducers or inhibitors of CYP3A4• Drugs that affect both CYP3A4 and P-gp• Rivaroxaban>apixaban>dabigatran≈edoxaban
Am J Cardiovasc Drugs. 2019;19(6):525-539Drug Saf. 2019;42(12):1409-1422.Blood. 2018;132(21):2230-2239.

Drug Interaction Potential*
Strong Inhibitors Strong Inducers
CYP3A4 P-glycoprotein CYP3A4 P-glycoprotein
KetoconazoleItraconazole RitonavirErythromycin^
KetoconazoleItraconazole RitonavirErythromycin^
Dronedarone^
Verapamil^
Rifampin Carbamazepine Phenytoin Phenobarbital Primidone St. John’s wort
Rifampin Carbamazepine Phenytoin St. John’s wort
Apixaban• 5-10mg BID→ reduce dose by 50%• 2.5mg BID→ avoid
Avoid
RivaroxabanAvoid^Avoid if CrCl <80mL/min
Avoid
47
*Not comprehensiveBID=twice dailyCrCl=creatinine clearance
Lexicomp Online 2020. Apixaban: Drug information. UpToDate, Inc.Lexicomp Online 2020. Rivaroxaban: Drug information. UpToDate, Inc Am J Cardiovasc Drugs. 2019;19(6):525-539.

Warfarin Pharmacokinetics and DDI
• Warfarin is a substrate of– Major: CYP2C9
– Minor: CYP3A4, CYP2C19, CYP1A2
• Mechanisms for DDI– Inhibition/ induction of CYP450 enzymes (mostly 2C9)
– Competition for plasma protein binding
– Alteration in intestinal bacteria that synthesize vitamin K
• Strong CYP inducers
• The “FAB-Four” inhibitors – Fluconazole (and other azoles)
– Amiodarone
– Bactrim
– Flagyl 48 Hematology Am Soc Hematol Educ Program. 2018;2018(1):339-347.

Summary of Recommendations for DDI Involving Anticoagulants
49
Substrate
Inhbitor/InducerAntiarrhythmics Antibiotics Antiepileptics Antifungals Other
amio
dar
on
e1
,2,3
dro
ned
aro
ne
1,3
dilt
iaze
m1
vera
pam
il1
,3
azit
hro
myc
in3
clar
ith
rom
ycin
1,3
eryt
hro
myc
in1
,3
trim
eth
op
rim
/su
lfa
met
ron
idaz
ole
rifa
mp
in1
,2,3
carb
amaz
epin
e1
,2,3
ph
eno
bar
bit
al1
,2,3
pri
mid
on
e1
,2,3
ph
enyt
oin
1,3
flu
con
azo
le1
,2
isav
uco
naz
ole
1
itra
con
azo
le1
,3
keto
con
azo
le1
,3
po
saco
naz
ole
1
vori
con
azo
le1
,2
rito
nav
ir1
,3
St. J
oh
n's
Wo
rt1
,3
cycl
osp
ori
ne
1,2
,3
Apixaban1,3 ↑ ↑ ↑ ↑* ↑ ↓ ↓ ↓ ↓ ↓ ↑ ↑ ↑* ↑* ↑* ↑* ↑* ↓
Rivaroxaban1,3 ↑ ↑* ↑* ↑* ↑* ↓ ↓ ↓ ↓ ↓ ↑ ↑ ↑ ↑ ↑ ↓
Edoxaban3 ↑ ↑ ↑ ↑ ↑ ↑ ↓ ↓ ↓ ↑ ↑ ↑ ↓ ↑
Dabigatran3 ↑* ↑* ↑* ↑* ↑* ↑* ↓ ↓ ↓ ↓ ↓ ↑* ↑* ↑* ↓ ↑*
Warfarin1,2 ↑ ↑ ↑ ↑ ↑ ↑ ↑ ↓ ↓ ↓ ↓ ↑ ↑ ↑ ↑ ↑ ↑ ↓ ↓
Avoid
Dose adjust
Caution/Increased monitoring
No interaction
*Avoid in certain patients with reduced renal function1 CYP3A42 CYP2C93 P-gp↑ Increase in DOAC exposure↓ Decrease in DOAC exposure
Drug Interactions. Micromedex Solutions. Truven Health Analytics, Inc. Ann Arbor, MI. Available at: http://www.micromedexsolutions.com. Accessed August 2020Lexicomp® Drug Interactions. Available at https://www.uptodate.com/drug-interactions/?source=responsive_home#di-druglist. Accessed August 2020.
Other Significant DDI
• Carbapenems and valproic acid – All carbapenems decrease valproic acid concentrations – Avoid combination
• Azole antifungals and calcineurin inhibitors (CNI)– Azoles increases tacrolimus/cyclosporine due to CYP3A4 inhibition– Potency of CYP3A4 inhibition
• Ketoconazole*> itraconazole*= voriconazole*> posaconazole* > fluconazole= isavuconazole
– Dose reduction of CNI required • *Reduce CNI to one-half to one-third
– i.e. tacrolimus 3mg BID→ 1mg BID
• Utilize clinical pharmacist
50 Drug Metab Rev. 2007;39(4):647-657Pharmacotherapy 2010;30(8):842–854
Likely to get a call from pharmacist

3. Errors in Medication Reconciliation and Transitions of Care
51

Common Medication Reconciliation Mistakes
Med History/Rec• Inaccurate or incomplete documentation of
drug, dose, route, frequency, dosage form
• Continuing a medication the patient is no longer taking
• Continuing a medication that is not clinically appropriate
• Not continuing an appropriate medication a patient is taking
• Discontinuing medications appropriately on admission but not restarting upon discharge
• Confusion with formulary interchanges
Transitions of Care
Discharge
• Inappropriate continuation from transition from ICU to ward– PPI
– Antipsychotics
– Sedation
• Inappropriate continuation of medications at hospital discharge– Opioids
– Insomnia medications
– Benzodiazepines 52
54%
71%
Arch Intern Med. 2005;165(4):424.Ann Pharmacother. 2010;44(12):1887.Arch Intern Med.2012:1-13.Ann Pharmacother. 2008;42(10):1373.J Gen Intern Med. 2007;22(7):1024.
62%

Inappropriate Continuation of ICU Medications is Common
Proton Pump Inhibitors (PPIs)
• Patients often discharged on stress ulcer prophylaxis with no clear indication
• Hospitalized patients commonly on PPIs without clear indication
• Potential risks of PPIs– Diarrhea, impaired B12
absorption, hypomagnesemia,Clostridium difficile infection, hip fractures, and pneumonia
– Poly pharmacy consequences– Economic consequences
Antipsychotics
• Often prescribed for new onset agitation or delirium
• Many continued upon hospital discharge
• Potential risks of antipsychotics – Metabolic disturbances– Somnolence– Dry mouth– Extrapyramidal symptoms – Consequences of polypharmacy– Increased risk of death in elderly
53
Up to 44%
Up to 65%
21%
Gastroenterology. 2020; 159 (2):e23-e24.Crit Care Resusc. 2016;18(4):270-274Crit Care. 2012;16(3):R84J Crit Care. 2016;33:119-124Ther Adv Drug Saf. 2018;10:2042098618809933.

Strategies to Avoid Medication Reconciliation Errors
Accurate med history
• Communication with patient, caregiver, pharmacy, outpatient prescriber
• Utilization of pharmacy fill database to check accuracy
– Investigate noncompliance
• Check on drugs/ formulations/ doses you are not familiar with
Accurate med reconciliation
• What medications are important to continue in-patient? – Corticosteroids, anticoagulation,
immunosuppressants, thyroid
• What medications should I think about holding?– Diuretics/ anti-hypertensives (if in
shock)
– Sedatives/psych meds (if altered)
• Always take into consideration current renal function!
54

Strategies to Avoid Errors upon Transfer and Discharge
• At transfer– Look at home medication list and current medication orders– Ensure that medications are appropriately continued, resumed, or
discontinued• Appropriately continued: new IV antibiotics • Appropriately resumed: anticoagulation after procedure • Appropriately discontinued: stress ulcer prophylaxis, sedation, antipsychotics
• Upon discharge – Consult the home medication list, current medication orders, compare them
with the discharge medication orders – Ensure that medications are appropriately continued, resumed, or
discontinued
• Multidisciplinary teamwork is key!55

2. Failure to Renally Dose
56

Inappropriate Prescribing of Renally Cleared Drugs is Common
• ~30% of prescriptions inpatient • Up to half of patients with CKD in the outpatient setting• 12-43% elderly patients in long term care • Drug classes most likely to be inappropriately renally dosed
– Antibacterial agents– Antivirals – Anticoagulants– Analgesics – Antihyperglycemics
57
Annals of Pharmacotherapy 2020, Vol. 54(7) 625–632.Drugs Aging (2015) 32:391–400.J Pharm Bioallied Sci 2013 Apr – Jun; 5 (2): 136-40.Intern Med J 2003;33:10–13.Gen Intern Med 2007;23:423–8.

Factors Contributing to Renal Dosing Errors
• Many medications are renally cleared
• Failure to recognize chronic kidney disease (CKD)
• Failure to adjust after acute kidney injury (AKI)
• Failure to adjust after resolution of AKI
• Knowledge about dose-adjustment requirements
• Failure to recognize age as an important contributing factor
• Failure to adjust when transitioning between RRT modalities
• Unfamiliar with forms of renal replacement therapies (RRT)
– Hemodialysis (HD)
– Continuous renal replacement therapy (CRRT)
– Peritoneal dialysis (PD)
• Inappropriate or inadvertent override of clinical decision support system (CDSS) alerts
• Lack of CDSS interventions in the ambulatory care setting
58 Pharmacotherapy 2011;31(4):346–356.J Gen Intern Med. 2008;23(8):1125–30.

Strategies to Avoid Renal Dosing Errors: Inpatient
59
Electronic documentation of AKI Electronic documentation of resolved AKI
Think about dose adjustment! Antibiotics
Anticoagulants Electrolytes
Opiates

How to Access UPMC Renal Dosing Guidelines for Antimicrobials
60

Strategies to Avoid Renal Dosing Errors: Outpatient
61
eGFR Ranges (mL/min/1.73m2)Medication Class <15 15-29 30-44 45-59
AntibioticsCiprofloxacinLevofloxacinNitrofurantoinTMP/SMX
AnticoagulantsApixabanDabigatranEdoxabanEnoxaparinRivaroxaban
AnticonvulsantsGabapentinLevetiracetemPregabalin
Oral hypoglycemicsCanagliflozinDapaglifozinEmpaglifozinGlyburideMetformin
OtherBaclofenDigoxinColchicineLithium
Avoid
Dose-adjust
No dose adjustment Ann Pharmacother. 2020;54(7):625-632.

1. Polypharmacy and Failure to
Deprescribe
62

Polypharmacy • Technical definition: Regular use of at least 5 medications
– More common in elderly • By age 70, three out of four people take > 5 medications daily
• Functional definition: Use of multiple medications that are unnecessary and have the potential to do more harm than good
• Many negative consequences – Increased burden on health care system – Decreased quality of life– Increased risk of adverse drug events – Increased medication errors – Increased fall risk – Increased mortality
63 Am Fam Physician. 2019 Jul 1;100(1):32-38.Fam Pract Manag. 2018 May-June;25(3):28-32
One study: only 19% of office visits to general internists included a medication review!

Polypharmacy and the Prescribing Cascade
Newly prescribed med A
Side effect to med A
Prescribe med B to treat side effect of
med AADE to med B
Prescribe med C to treat ADE of med B
64
Amlodipine for hypertension
Patient develops peripheral edema
Furosemide prescribed Patient develops urinary incontinence
Anticholinergic prescribed
1.4% of patients prescribed a calcium channel blocker were subsequently prescribed a loop diuretic within 90 days compared with 0.7% of patients prescribed a different antihypertensive (p<0.001).
JAMA Intern Med. 2020;e197087.Fam Pract Manag. 2018 May-June;25(3):28-32.

Deprescribing
Definition
• Set of interventions to identify inappropriate or unnecessary medications
• Act of tapering, reducing, or stopping a medication
• Goal: to reduce medication burden and harm while maintaining or improving quality of life
Common Target Medications
• Antipsychotics
• PPIs
• Benzodiazepines
• Aspirin
• NSAIDs
• Statins
• Antihypertensives65 Fam Pract Manag. 2018 May-June;25(3):28-32.
Can Fam Physician. 2017;63(5):354-364.

66Can Fam Physician. 2017;63(5):354-364.

Appropriate Select Indications for PPIIndication Duration Barrett’s Esophagus Lifelong
Erosive esophagitis Lifelong
Zollinger-Ellison syndrome Lifelong
GERD without erosive esophagitis 4-8 weeks then re-assess
Active upper GIB secondary to PUD Determined by underlying etiology of bleed
H. pylori 14 days
PUD: Gastric ulcers 8-12 weeks
PUD: Duodenal ulcers 4-8 weeks
PUD: NSAID-induced Minimum 8 weeks
Prevention of PUD in high risk patients Until risk factors absent
DAPT or triple therapy in high risk patients Duration of DAPT/ anticoagulation
H2RA failure or intolerance Depends on indication
PUD= peptic ulcer diseaseNSAID=nonsteroidal anti-inflammatoryDAPT=dual antiplatelet therapyH2RA= histamine receptor antagonist67
Am J Gastroenterol 2016; 111:30–50.Gastroenterology 2016;151:822–835Am J Gastroenterol 2013; 108:308 – 328Can Fam Physician. 2017 May;63(5):354-364.J Am Coll Cardiol. 2016;67(14):1661-71
When to Consider Deprescribing Aspirin
• Routine use for Primary prevention– Especially if >75 years old
• Atrial fibrillation without coronary artery disease – Use anticoagulation (OAC) alone
• Atrial fibrillation with acute coronary syndrome/stent– Use P2Y12 inhibitor (clopidogrel) + OAC
– Avoid long term triple therapy (DAPT +OAC)
• When long term OAC is needed – Exception: history of mechanical heart valve
• Triple therapy (DAPT +OAC)– Use for shortest duration possible
68
Clin Cardiol. 2020;43(2):137-144.Circulation. 2019;140(11):e596-e646.N Engl J Med 2019;380:1509-24.
Takeaway:If you newly prescribe an oral anticoagulant →investigate whether your patient still has an indication for aspirin
69
Tips for deprescribing
✓ Discontinue unnecessary therapy
✓ Consider adverse drug reactions (ADR) as a possible cause for any new symptom
✓ Avoid treating side effects with another drug
✓ Consider nonpharmacologic options
✓ Decrease the dose if ADR suspected but drug is essential
✓ Don’t avoid drugs with known benefits just to minimize number of drugs
Resources to aid in deprescribing
– The Anticholinergic Burden Calculator • http://anticholinergicscales.
es/calculate
– The Beers List • https://bit.ly/2GQhM2Y
– Deprescribing.org
– MedStopper• http://medstopper.com

70
Top 10 Prescribing Mistakes Providers Frequently Make
1. Polypharmacy
2. Failure to renally dose
3. Med rec and transitions of care
4. Drug-drug interactions
5. Drug allergies
6. Anticoagulants
7. Opioids
8. Drug monitoring
9. Dosage form errors
10. Ordering errors

Acknowledgements
• Peg Verrico, BS Pharm, RPh
• Erin McCreary, PharmD, BCPS, BCIDP
• Adrienne Szymkowiak, PharmD
71

Top 10 Prescribing Mistakes Providers Frequently Make
Lara Groetzinger, PharmD, BCCCP
Unit-based clinical pharmacist
Medical ICU





























