Embed Size (px)
Citation preview
Special Article June 1999: 177-181
Too Much Versus Too Little: The Implications of Current Iodine Intake in the United States Kelly Lee, M.S., R.D., Robert Bradley, M.S., R.D., Johanna Dwyer, D.Sc., R.D., and Stephanie L. Lee, M.D., Ph.D.
lodine intake influences the health of Americans todaH but in different ways than it has in the past. In the early 7900s, iodine deficiency was respon- sible for widespread endemic goiter in the United States. The incidence of goiter was markedly re- duced by the introduction of iodine supplementa- tion of salt and other foods in the 7920s. By the middle of this century iodine-related problems in the Unites States were more likely to be aasoci- ated with too much rather than too little of this essential nutrient. Recent and disturbing new data suggest that there has been a sharp decline in iodine intake during the last 20 years, especially in women of reproductive age. A brief compari- son of thyroid response to insufficient and exces- sive intakes in normal and diseased thyroid tissue is presented. The population affected and the im- plications for therapy are also reviewed.
Introduction
At the turn of this century iodine deficiency disorders (IDD) were epidemic in many parts of the United States, with consequent morbidities that included endemic goi- ter.' Iodine deficiency occurs in regions where the topsoil has been depleted of iodine by erosion caused by glacier movement, rain, wind, and flooding. The most profound iodine deficiency and goiter occurred in several regions of the United States including the length of the Appala- chian range, the states bordering the Great Lakes, and
~~ ~~
Ms. Lee and Mr. Bradley are with the Frances Stern Nutrition Center, New England Medical Center, and Tufts University School of Nutrition Science and Policy; Dr. Dwyer is Director of the Frances Stern Nutrition Center, New England Medical Center, and Professor of Medicine and Community Health, Tufts University School of Medicine and School of Nutrition Science and Policy; Dr. Lee is Assistant Professor of Medicine, Tufts University School of Medicine, and Director of the Thyroid Disease Center, Division of Endocrinology, New England Medical Center, Boston, MA 021 11, USA. Reprint requests should be directed to Dr. Stephanie Lee.
westward to the Northwest and Rocky Mountain regions of the United States.
In the 1920s David Marine conducted initial studies of iodine supplementation in adolescent girls and demon- strated that sodium iodide supplementation reduced thy- roid enlargement from 21% to 0.2%.2 Salt iodination has never been mandatory in the United States because salt manufacturers readily iodized their products to achieve marketing advantages over their competitors who did not add iodine. By the mid-1 900s preventive efforts had been so successful that IDD was no longer considered a public health problem in America. For the last 50 years the aver- age American iodine intake3 exceeded the Recommended Dietary Alloyance (RDA)4 and the recommended level based on a consensus statement by UNICEF, the Interna- tional Council for the Control of Iodine Deficiency Disor- ders (ICCIDD), and the World Health Organization (WHO).' The importance of iodine in the prevention of goiter has nearly disappeared from the collective American con- sciousness owing to the widely held but erroneous belief that iodine deficiency has been permanently eliminated.
Iodine intake still influences the health ofAmericans today but in different ways than in past years. Today, iodine-related problems occur in subsets ofthe U.S. popu- lation that have either excessive or deficient intake of this essential nutrient.6 For most individuals the level of io- dine in the American diet today is appropriate for good health, but small but significant groups of persons with disparate pathologies of the thyroid gland suffer adverse health effects from current iodine intake. Depending on underlying thyroid pathology, excessive iodine may cause hypothyroidism, goiter formation, or hyperthyroidism in these persons. Also, excessive iodine in the diet may im- pede the diagnosis and treatment of individuals with dis- eases of the thyroid who are about to undergo radioactive iodine administration. Iodine deficiency, especially in women, will cause an increase in goiter formation, with additional special concerns during pregnancy.
This article provides a review of the biologic effects of the spectrum of iodine intakes, which range from toxic- ity to deficiency, and their public health implications to- day.
Nutrition Reviews@, Vol. 57, No. 6 177

Current Intakes more than 20% of the population should have a urinary
Virtually all iodine intake occurs via dietary ingestion. The effects of low iodine intakes and the prevalence of IDD have not been considered a major public health issue in this country for the last 50 years because of a well-estab- lished voluntary program of fortification of table salt with iodine. Iodized salt in the United States contains one part iodine to 10,000 parts salt (sodium chloride) by weight. Therefore, 1 g iodized salt contains approximately 100 pg iodine. Also, there is a relatively high level of iodine in the American food supply from other sources: Iodine prod- ucts are commonly used as ingredients in or in the pro- cessing of bread and dairy products, and the diets of cattle and chickens are often supplemented with kelp, resulting in significant but variable amounts of iodine in meats, milk, and eggs. As a result, iodine intake in the United States in the recent past has been higher than both mini- mal average requirements and the RDA l e ~ e l . ~ . ~ - ~
Previously published data regarding iodine consump- tion in the United States is from the Food and Drug Ad- ministration Total Diet Study 1991. The estimated daily intake of iodine from food is between 150 and 550 &day, with many people getting more than the dietary allow- ances of 150 pglday for adolescents and adults and 200 &day for pregnant or lactating w0men~9~ recommended by the Food and Nutrition Board ofthe U.S. National Re- search Council. The Total Diet Study underestimates io- dine intake because it does not include the contributions of iodine from iodized salt, drinking water, prepared or “fast” foods, and medications. Some but not all daily mul- tiple vitamins contain 150 pg iodine per tablet. Kelp or seaweed supplements available at natural food or nutri- tion stores may contain many thousands of micrograms of iodine per tablet. It is impossible to analyze every food on the market, and there is considerable variation in io- dine content by region and by processing technique. Therefore, it is possible that significant sources of iodine have yet to be identified and that intakes may be higher than current estimates. Iodine intake levels of this magni- tude are not a problem for the general population. How- ever, high intake levels in those with previous iodine defi- ciency, diffuse or nodular nontoxic goiter, thyroiditis and hyperthyroidism, and in those who require radioactive iodine (I131) treatment for thyroid cancer or thyrotoxicosis are at risk for complications.
Trends in dietary habits and food selection were not taken into account in the Total Diet Study. Iodine excre- tion data from the first National Health and Nutrition Ex- amination Survey (NHANES I)’ collected across the coun- try fiom 197 1 to 1974 confirmed the Total Diet Study data showing that the average urinary iodine concentration was relatively high at 293.3 pgfg creatinine. The median urinary iodine concentration of an iodine-sufficient popu- lation should be greater than 100 pglg creatinine, and no
iodine concentration below 50 pgfg creatinine. Significant iodine deficiency occurs with urinary iodine excretion of less than 50 pgfg creatinine. At the end of 1998, data from NHANES I11 (1 988-1 994) demonstrated a surprising and significant reduction in the average American dietary io- dine intake to 124.6 pg/g ~reatinine.~ Although this aver- age intake is considered sufficient, the size of the popula- tion with iodine deficiency (urinary iodine concentration less than 50 pg/g creatinine) rose 1 0-fold from NHANES I to 8.1 % of men and 15.1 % of women. At high risk are Caucasian females between ages 40 and 49 years, who had the highest incidence of iodine deficiency (25.5%). In fact, approximately 19-23% of women between ages 30 and 60 years were iodine deficient. Thus, iodine deficiency is again becoming significant, especially in women in the United States. This observed reduction in iodine intake must be monitored carefully and confirmed with additional independent studies because iodine deficiency is associ- ated with goiter formation, with increased risk of miscar- riages, and possibly with reduced intelligence in offspring of iodine-deficient mother^.^,^^^^
The recent reduction in dietary iodine may be owing to several factors, including the dairy industry’s effort to reduce iodine in milk, the replacement of iodine with bro- mine salts as the dough conditioner in commercial bread production, reduced intake of eggs (especially the iodine- rich yolks) for cholesterol concerns, reduced use of table salt for hypertension concerns, and the use of salt not supplemented with iodine in manufactured foods. Another factor that must be taken into account is the low public awareness of the importance of using iodized salt to main- tain an adequate iodine intake for good thyroid health.
Iodine Metabolism
The only known function of iodine in the human body is as an essential component of the thyroid hormones thy- roxine (T,) and triiodothyronine (T3). T, contains four at- ums (59% by weight) and T, contains three atoms (65% by weight) of iodine per molecule. Severe iodine deficiency results in reduced thyroid hormone levels and hypothy- roidism. The biologic functions of the thyroid hormones include binding to nuclear receptors to influence gene expression in target tissues resulting in biologic effects on neuronal development, adrenergic receptor sensitiv- ity, oxygen consumption, resting metabolic rate, heat pro- duction, and fatty acid release from adipose tissue.
Iodine is absorbed completely and rapidly from the gut in the form of iodide, which is the most common form of dietary iodine. Once iodine is in the blood stream, it is transported both as free and protein-bound iodine and is distributed throughout the body’s extracellular compart- ments. A sodium-iodate symporter concentrates the io- dine in a saturable and energy-dependent process into
178 Nutrition Reviews@, Vol. 57, NO. 6
High iodine intake
Normal thyroid Pathology: Thyroiditis
Graves’ thyrotoxicosis Hashimoto’s hypothyrodism
Wolff-Chaikoff Shut down
.1 Escape and return
to normal
.1 Wolff-Chaikoff
Shut down
-1 No escape and hypothyroidism
Pathology: Thyroid autonomy
Toxic adenoma Toxic and non-toxic multinodular goiter
-1 lodineinduced
Hyperthyroidism (Jod-Basedow thyrotoxicosis)
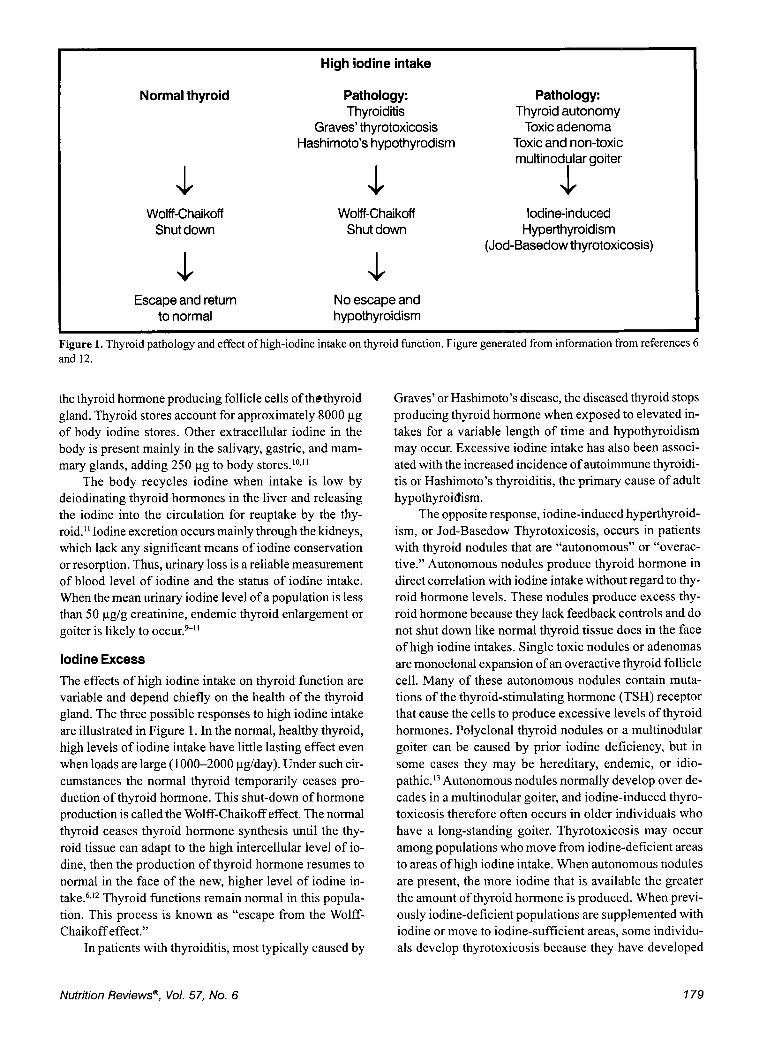
Figure 1. Thyroid pathology and effect of high-iodine intake on thyroid function. Figure generated from information from references 6 and 12.
the thyroid hormone producing follicle cells of thethyroid gland. Thyroid stores account for approximately 8000 pg of body iodine stores. Other extracellular iodine in the body is present mainly in the salivary, gastric, and mam- mary glands, adding 250 pg to body stores.lO.”
The body recycles iodine when intake is low by deiodinating thyroid hormones in the liver and releasing the iodine into the circulation for reuptake by the thy- roid.” Iodine excretion occurs mainly through the kidneys, which lack any significant means of iodine conservation or resorption. Thus, urinary loss is a reliable measurement of blood level of iodine and the status of iodine intake. When the mean urinary iodine level of a population is less than 50 pg/g creatinine, endemic thyroid enlargement or goiter is likely to o c c ~ r . ~ - ~ I
Iodine Excess
The effects of high iodine intake on thyroid function are variable and depend chiefly on the health of the thyroid gland. The three possible responses to high iodine intake are illustrated in Figure 1. In the normal, healthy thyroid, high levels of iodine intake have little lasting effect even when loads are large (1 000-2000 pdday). Under such cir- cumstances the normal thyroid temporarily ceases pro- duction of thyroid hormone. This shut-down of hormone production is called the Wolff-Chaikoff effect. The normal thyroid ceases thyroid hormone synthesis until the thy- roid tissue can adapt to the high intercellular level of io- dine, then the production of thyroid hormone resumes to normal in the face of the new, higher level of iodine in- take.6,12 Thyroid functions remain normal in this popula- tion. This process is known as “escape from the Wolff- Chaikoff effect.”
In patients with thyroiditis, most typically caused by
Graves’ or Hashimoto’s disease, the diseased thyroid stops producing thyroid hormone when exposed to elevated in- takes for a variable length of time and hypothyroidism may occur. Excessive iodine intake has also been associ- ated with the increased incidence of autoimmune thyroidi- tis or Hashimoto’s thyroiditis, the primary cause of adult hypothyroidism.
The opposite response, iodine-induced hyperthyroid- ism, or Jod-Basedow Thyrotoxicosis, occurs in patients with thyroid nodules that are “autonomous” or “overac- tive.” Autonomous nodules produce thyroid hormone in direct correlation with iodine intake without regard to thy- roid hormone levels. These nodules produce excess thy- roid hormone because they lack feedback controls and do not shut down like normal thyroid tissue does in the face of high iodine intakes. Single toxic nodules or adenomas are monoclonal expansion of an overactive thyroid follicle cell. Many of these autonomous nodules contain muta- tions of the thyroid-stimulating hormone (TSH) receptor that cause the cells to produce excessive levels of thyroid hormones. Polyclonal thyroid nodules or a multinodular goiter can be caused by prior iodine deficiency, but in some cases they may be hereditary, endemic, or idio- pathic.13 Autonomous nodules normally develop over de- cades in a multinodular goiter, and iodine-induced thyro- toxicosis therefore often occurs in older individuals who have a long-standing goiter. Thyrotoxicosis may occur among populations who move from iodine-deficient areas to areas of high iodine intake. When autonomous nodules are present, the more iodine that is available the greater the amount of thyroid hormone is produced. When previ- ously iodine-deficient populations are supplemented with iodine or move to iodine-sufficient areas, some individu- als develop thyrotoxicosis because they have developed
Nutrition Reviews@, Vol. 57, No. 6 179

autonomous thyroid nodules.l”16 This condition, a toxic multinodular goiter, is a common diagnosis in the United States among immigrants from iodine-deficient areas in Asia, for example. By interfering with the synthesis of thyroid hormone, antithyroid thionamide drugs such as propylthiouracil and methimazole are used to treat thyro- toxicosis caused by conditions such as Graves’ disease and toxic multinodular g0iter.I’
Iodine Deficiency
There are three levels of iodine deficiency based on uri- nary iodine levels: mild (50-100 pg/g creatinine), moder- ate (20-49 pg/g creatinine), and severe (< 20 pg/g creati- nine). The average urinary excretion of creatinine is ap- proximately 1 g/day in adults but depends on the renal function and muscle mass of the person. In areas with severe deficiency, side effects in addition to goiter forma- tion are observed, including hypothyroidism, endemic mental retardation, cretinism, and decreased fertility. Io- dine deficiency is the most common preventable cause of mental retardation in the world.
When iodine intake is even just mildly deficient, the first sign is thyroid enlargement or goiter formation. The body is not able to produce adequate levels of T,. In re- sponse, TSH is released from the pituitary gland and the thyroid gland produces increased numbers of thyroid fol- licle cells and it enlarges.I0The enlarged gland is able to trap available iodine more efficiently and thus can pro- duce more thyroid hormone. Mild to moderate iodine defi- ciency results in endemic goiter without hypothyroidism. The thyroid hormone levels remain in the normal range but at the expense of developing an enlarged thyroid gland or goiter.
Although there are many causes of goiter, adaptation to chronic low iodine intakes is one common cause of formation in large populations. Over time the goitrous thy- roid develops autonomous nodules, which increase the risk of hyperthyroidism from a high iodine intake. When several autonomous nodules form in a goiter, the patient may become thyrotoxic from a “toxic multinodular goiter” even with a normal iodine intake. These patients may ex- perience a marked worsening of thyrotoxicosis if exposed to large amounts of iodine.
Goitrogens may worsen the effects of iodine defi- ciency. Cassava meal, a dietary staple in many areas of the world, contains linamarin which is metabolized to thiocy- anate that can interfere with iodine trapping and thyroid hormone production. Goitrogens are also found in millet, kelp, maize, bamboo shoots, sweet potatoes, lima beans, and vegetables of the genus Brassica, including cabbages, turnips, kale, rutabaga, and mustard. Selenium deficiency worsens iodine deficiency because of the decrease in the activity of enzymes required for thyroid hormone synthe- sis.
4
Also, dietary iodine may influence the type and inci- dence of thyroid carcinoma. It has been observed that aggressive follicular thyroid cancer is common in areas of iodine deficiency, whereas the more indolent papillary thy- roid cancer is more common in areas of iodine sufficiency. The causal relationship is supported by the observation that in regions of iodine deficiency that have been supple- mented with iodine, the incidence of follicular thyroid car- cinoma falls concomitant with a rise in papillary thyroid carcinoma.
Implications for Therapy
The public health implications of iodine intake in the United States have moved from the historical problem of endemic iodine deficiency to concerns about the health effects of high levels of iodine in some individuals, with specific risks of either increased or insufficient intake on different thyroid pathologies. As the new millennium arrives there are new public health concerns about a trend of iodine deficiency in certain subsets of the U.S. population. Of particular concern is iodine deficiency in young women of reproductive age, which could lead to goiter formation and potentially reduced mental intellect of children born to mothers with severe iodine deficiency. It is predicted that mild iodine deficiency contributes to thyroid enlarge- ment and goite? formation. During the last decade, it has been recognized that thyroid nodules occur in 50% of the elderly, which may reflect goiter formation from insuffi- cient iodine intake. It is important for health care profes- sionals to consider iodine deficiency as a cause of nodu- lar goiter in the United States and to watch for an increas- ing incidence, especially in women. It is very important that the public understand that the use of iodized salt is necessary for normal thyroid function.
More than 14,000 patients are diagnosed with thyroid cancer each year.I8 In addition, approximately 1% of the U.S. population-2.7 million people4evelop thyrotoxi- cosis during their lifetime. Patients with this diagnosis are often treated with radioactive iodine. The main concern for them is that the uptake of radioactive iodine will be decreased when dietary iodine intake is high.I9”O There is good reason to believe that this is so. In the United States, uptake of II3’ by the thyroid has progressively decreased during the last 50 years. By the late 1960s the normal 24- hour thyroid uptakes had already decreased from approxi- mately 20-30% to between 5 and 10% of the administered dose of radioactive iodine.2I To increase the uptake of for radioiodine therapy it is customary to prescribe a low- iodine diet to patients to increase iodine uptake by the thyroid tissue, thereby creating a temporary dietary defi- ciency state.
A major challenge for clinicians is to make sure that medical nutrition therapy prior to radioactive iodine therapy maximizes II3I uptake by the diseased thyroid tissue. Be-
180 Nutrition Reviews@, Vol. 57, No. 6
cause iodine intake in the United States is very high in some patients, 5- to 14-day low-iodine diets are prescribed for patients prior to radioactive iodine therapy. The goal is to create a temporary dietary deficiency of iodine so the thyroid tissue will avidly take up the administered radio- active iodine and will receive a maximally effective radia- tion dose.
Conclusion
Food processing practices and the use of iodized salt since the 1920s have created a food supply in the United States that can be high in iodine. Health care providers must be aware of the interaction of high-iodine intakes with sus- ceptible individuals with thyroid dysfunction. Iodine in- take, although sufficient on average, has decreased dra- matically during the last 20 years, as illustrated by recent NHANES I11 data. Although the reduction in iodine intake in subsets of the population is moderate, there is no con- cern for severe deficiency associated with cretinism and growth and mental retardation. It therefore appears that, similar to the start of the 20th century, the UnitedStates at the start of the 2 1 st century is again faced with iodine deficiency, at least in certain subsets of the population. It is unclear whether the trend toward use of prepared foods that do not contained iodized salt or avoidance of added iodized salt at the table is responsible, but until it is deter- mined what dietary pattern or patterns have contributed to this change clinicians must be aware of the effects of too little and too much iodine on thyroid physiology. The United States has a unique set of public health concerns regarding both iodine deficiency, especially in women, which may result in goiter formation, and the effects of too much iodine on certain individuals who are at risk because of pre-existing thyroid pathology.
Acknowledgments. This research was funded in part by contract number 53/3-K06-5-10 ofthe U.S. Department of Agriculture and by the Gerber Foundation, which pro- vided partial salary support to Dr. Dwyer for preparation of this manuscript. Support was also provided through the General Clinical Research Center, funded by the Divi- sion of Research Resources of the NIH under grant num- ber MO 1 -RR00054.
1. Food and Nutrition Board, Institute of Medicine. lo- dine nutrition in the United States: summary of a conference. Washington, DC: National Academy Press, 1970 Marine D. Prevention and treatment of simple goi- ter. Atlantic Med J 1923;26:437-43
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
Hollowell JG, Staehling NW, Hannon WH, et al. Iodine nutrition in the United States. Trends and public health implications: iodine excretion data from National Health and Nutrition Examination Surveys I and Ill (1971-1974 and 1988-1994). J Clin Endocrinol Metab 1998;83:3401-8 Food and Nutrition Board, Institute of Medicine. Recommended dietary allowances, 10th ed. Wash- ington, DC: National Academy Press, 1989 WHO, UNICEF, ICCIDD. Indicators for assessing iodine deficiency disorders and their control through salt iodization. Geneva: World Health Organiza- tion, 1994;6:36 Vagenakis AG, Braverman LE. Adverse effects of iodides on thyroid function. Med Clin North Am
Pennington JAT, Schoen SA. Contributions of food groups to estimated intakes of nutritional elements: results from the FDA Total Diet Studies, 1982-1 991. Int J Vitam Nutr Res 1996;66:350-62 * Pennington JAT, Young BE. Total Diet Study nutri- tional elements, 1982-1 989. J Am Diet Assoc
Hetzel BS. The story of iodine deficiency: an inter- national challenge in nutrition. New York: Oxford University Press, 1989 Linder MC, ed. Nutritional biochemistry and me- tabolism: with clinical applications, 2nd ed. New York: Elsevier, 1991 ;252-5 Hunt S, Groff J. Advanced nutrition and human metabolism. New York: West Publishing Co, 1990;
Bravelman LE. Effects of iodine on thyroid function in man. Trans Am Clin Climatol Assoc 1990;102:
Dremier S, Coppee F, Delange F, et al. Thyroid au- tonomy: mechanism and clinical effects. J Clin Endocrinol Metab 1996;81:4187-93 Todd CH, Allain T, Gomo ZAR, et al. Increase in thyrotoxicosis associated with iodine supplements in Zimbabwe. Lancet 1995;346:1563-4 Fradkin JE, Wolff J. Iodide-induced thyrotoxicosis. Medicine 1983;62:1-20 Anonymous. Iodine fortification and thyrotoxicosis. Nutr Rev 1970;28:212-4 Cooper DS. Antithyroid drugs. N Engl J Med 1984;
Parker SL, Tong T, Bolden S, et al. Cancer statis- tics. CA Cancer J Clin 1996;65:5-27 Park YK, Harland BF, Vanderveen JE, Shank FR. Estimation of dietary iodine intake of Americans in recent years. J Am Diet Assoc 1981 ;79:17-24 London Wr, Vought RL, Brown FA. Bread: a dietary source of large quantities of iodine. N Engl J Med 1965;273:381 Oddie TH, Fisher DA, McConahey WM, Thompson LS. Iodine intake in the United States: a reassess- ment. J Clin Endocrinol Metab 1970;30:659-65
1975;59:1075-88
1991 191 :I 79-83
3 1 8-22
143-52
31 1 1 353-62
Nutrition Reviews@, Vol. 57, No. 6 181