Embed Size (px)
DESCRIPTION
Article
Citation preview

International Journal of Cardiology xxx (2012) xxx–xxx
IJCA-14827; No of Pages 10
Contents lists available at SciVerse ScienceDirect
International Journal of Cardiology
j ourna l homepage: www.e lsev ie r .com/ locate / i j ca rd
Review
Measurement accuracy of non-invasively obtained central blood pressure byapplanation tonometry: A systematic review and meta-analysis
Hao-Min Cheng a,b,c,⁎, Dora Lang a,d, Catalin Tufanaru a, Alan Pearson a
a The Joanna Briggs Institute, Faculty of Health Sciences, The University of Adelaide, Adelaide, Australiab Department of Medical Research and Education, Taipei Veterans General Hospital, Taipei, Taiwanc Department of Medicine, National Yang-Ming University, Taipei, Taiwand Centre for Evidence Based Nursing, Singapore National University Hospital, Singapore
⁎ Corresponding author at: The Joanna Briggs InstituThe University of Adelaide, 5005, Australia. Tel./fax: +6
E-mail address: [email protected] (H-
0167-5273/$ – see front matter © 2012 Elsevier Irelanddoi:10.1016/j.ijcard.2012.04.155
Please cite this article as: Cheng H-M, et al,etry: A systematic review and meta-analys
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 17 December 2011Received in revised form 20 April 2012Accepted 28 April 2012Available online xxxxKeywords:Central blood pressureApplanation tonometryTransfer functionSphygmoCorLate systolic peakSphygmomanometer
Background and objectives: Non-invasive methods based on applanation tonometry have been proposed to es-timate central blood pressure. However, the accuracy of these methods hasn't been systematically examined.Methods: We performed a systematic review and meta-analysis of studies comparing estimated andinvasively measured central BP.Results: Sufficient data were available in 22 studies for meta-analysis (857 subjects and 1167 measurements).Acquired arterial pressure waveforms in these studies were directly measured, calibrated to match invasiveaortic mean BP and diastolic BP or calibrated to match brachial BP measured with a sphygmomanometer, cuffBP. Of the former 2 conditions, the errors of estimated central BP were small with a mean and standard de-viation of difference −1.1±4.1 mm Hg (95% limits of agreement −9.1–6.9 mm Hg) for central systolic BP;−0.5±2.1 mm Hg (−4.6–3.6 mm Hg) for central diastolic BP; and −0.8±5.1 mm Hg (−10.8–9.2 mmHg) for central pulse pressure. However, the errors inflated to −8.2±10.3 mm Hg (−28.4–12.0 mm Hg)for central systolic BP, 7.6±8.7 mm Hg (−9.5–24.6 mm Hg) for central diastolic BP, and −12.2±10.4 mm
Hg (−32.5–8.1 mm Hg) for central pulse pressure, when calibrated to cuff BP. The findings were still evidentin subgroup analysis conducted with different central BP estimating methods and validated cuff BP monitors.Conclusion: Present tonometry-based central BP estimating methods are acceptable in theory, with small er-rors. However, based on current available evidence, there is substantial room for improvement in measure-ment accuracy of central BP when cuff BP is used to calibrate the peripheral waveforms.© 2012 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Blood pressure measurement has been used extensively in dailyclinical practice to manage cardiovascular disease. However, BP de-termined at different sites can vary considerably and may be differ-ently affected by antihypertensive drugs [1,2].
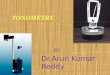
The gold standard of central BP measurements is aortic root BP,using a saline-filled catheter or an external pressure transducerwith tip in situ [3], which is not suitable for routine clinical practice.Recently, some noninvasive methods for estimating central BP areavailable [4–6]. Current common methods for the noninvasive esti-mation of central BP utilize applanation tonometry to acquire an arte-rial pressure waveform [7], which is then subject to calibration and/ormathematical calculation (Fig. 1, Appendix I).
te, Faculty of Health Sciences,1 8 84104809.M. Cheng).
Ltd. All rights reserved.
Measurement accuracy of nois, Int J Cardiol (2012), doi:1
The discrepancy between the central and peripheral BP may mag-nify with administration of vasoactive agents [6,8–12]. Growing evi-dence from epidemiological studies [13,14] and clinical observation[15] suggests that central BP may be more relevant than peripheralBP in predicting target organ damage and cardiovascular outcomes.Recent randomized controlled trials have also given impetus to theclinical application of central BP by demonstrating differential impactsof anti-hypertensive drugs on central and peripheral BP [16,17]. As aconsequence, the concept of central BP measurement was addressedin The 2007 ESH-ESC Practice Guidelines for the Management of Arte-rial Hypertension [18]. However, before recommending central BPmeasurement as a useful clinical tool, the accuracy of current centralBP estimatingmethods should be systematically examined. Moreover,a recent meta-analysis of longitudinal studies suggested that elevatedcentral BP was not significantly associated with a higher relative riskof clinical events as compared to elevated brachial BP [19]. This maycast doubt on the accuracy of the noninvasively estimated centralBP. Therefore, the aim of this systematic review and meta-analysiswas to synthesize the available research evidence on the accuracy ofcurrent noninvasive measurement methods for central BP. Throughour systematic review, professional societies can assess the accuracy
n-invasively obtained central blood pressure by applanation tonom-0.1016/j.ijcard.2012.04.155

Transfer function
CarotidSBP
A. Carotid tonometry
B. Radial tonometry
C. Radial tonometry
Central aortic SBP
RadialSBP2
Invasive calibration
Non-invasive calibration
Cather-measured central BP (MBP, DBP)
Invasivecentral MBP
Invasivecentral DBP
Mean
Minimum
Mean
Minimum
Raw wave Calibrated wave
Sphygmomanometers-measured cuff BP (SBP, DBP, MBP)
Cuff MBP
Cuff DBP
Maximum
Minimum
Maximum
Minimum
Raw wave Calibrated wave
Cuff SBP
(mmHg)
(mmHg)
Fig. 1. Illustrations of different methods used to estimate central blood pressure and the calibration procedures. The tonometry-recorded waveforms (raw wave) are adjustedaccording to either the catheter-measured invasive central BP or sphygmomanometer-measured cuff BP. The characteristics of the raw wave (maximum, mean, and minimum)are calculated first and then matched to the relevant BP values measured by invasive catheters or non-invasive BP monitors (i.e. mean and minimum correspond to MBP andDBP or maximum and minimum correspond to SBP and DBP, respectively). Panel A: use of carotid artery applanation tonometry to obtain calibrated carotid pressure waveform;panel B: use of radial artery applanation tonometry and a generalized transfer function to reconstruct an aortic pressure waveform; panel C: identification of the late systolic shoul-der of a tonometric radial pressure waveform (radial SBP2) to approximate central SBP. The calibration process may produce measurement errors when inaccurate cuff BP is usedfor non-invasive calibration.
2 H-M. Cheng et al. / International Journal of Cardiology xxx (2012) xxx–xxx
of these central BP-estimating methods and identify potential barriersto this concept and possible areas for future research.
2. Methods
2.1. Inclusion criteria
There was no restriction placed on language or year of publication. Studies wereconsidered eligible if they satisfied the following criteria.
2.1.1. Type of studyThe study had extractable data regarding measurements between estimated and
measured central BP.
2.1.2. Types of phenomena of interestThe study investigated the accuracy of noninvasive central BP-estimating methods
using applanation tonometry in comparison with invasively obtained correspondingvalues. To provide reference of measurement accuracy, studies using invasive BP forpressure waveform calibration or obtaining peripheral pressure waveform by directmeasurements of catheter were deemed eligible but meta-analyzed separately.
2.1.3. Types of participantStudies with adult subjects were considered, regardless of clinical diagnosis, co-
morbidities, and treatments. The participants had to have been receiving paired mea-surements of estimates and invasively measured central BP.
2.1.4. Types of outcomesThis review included the following types of outcome measures: systematic bias
and random error of estimates comparing with measured central BP.
2.2. Reference standard
The gold standard of central BP is aortic root BP measured with a saline-filled cath-eter or an external pressure transducer with tip in situ.
2.3. Search strategy (Appendix I)
The search strategy aimed to find both published and unpublished studies. Wesearched PubMed, CINAHL, Cochrane Library (including Cochrane DSR, DARE, andCCTR), Scopus, Web of Science, EMBASE, and Google Scholar by using all identified
Please cite this article as: Cheng H-M, et al, Measurement accuracy of noetry: A systematic review and meta-analysis, Int J Cardiol (2012), doi:1
keywords and index terms. Reference lists of identified studies were also searchedfor further studies.
2.4. Assessment of methodological quality/critical appraisal
Research papers selected for retrieval were assessed by 2 reviewers for methodo-logical validity prior to inclusion in the review using an original specific critical ap-praisal tool designed for the review. The methods and results of critical appraisalwere summarized in Appendix II.
2.5. Data extraction
Data were extracted from papers using an original data extraction form for this re-view developed by consensus and based on the previous systematic reviews for mea-surement accuracy [20]. Differences in data extraction were resolved by consensus.
2.6. Data synthesis
Study characteristics were extracted and summarized in Table 1. For quantitativesynthesis, we used the method developed by Dr Paula R Williamson for meta-analysis of method comparison studies [21], which has been used to examine the accu-racy of devices for measuring body temperature in children [20]. In brief, the pooledestimates of systematic bias and random errors were obtained using an inverse vari-ance weighted approach and the random effects model [20]. The former, also knownas Mantel–Haenszel weighted method, is a weighted sum of the estimates from eachof the primary studies. The weights are calculated by the inverse of the variance ofthe individual study estimates, which were the mean differences (MD) and standarddeviation of differences (SDD) between the paired measurements in method compar-ison studies. Homogeneity was assessed using a standard large sample test [22]. Meta-analysis based on DerSimonian–Laird weights for the random effects model [22],which incorporates a between-study variance, was also used for statistical poolingfor MD and SDD in the presence of significant heterogeneity across studies. To accountfor the source of heterogeneity, further subgroup analysis according to different centralBP estimating methods was also performed. On Forest plots, the individual and pooled95% limits of agreements combining systematic and random errors between pairedmeasurements of different central BP parameters were presented by subgroup analysisas well as in total.
n-invasively obtained central blood pressure by applanation tonom-0.1016/j.ijcard.2012.04.155

Table 1Population characteristics in individual studies about methods of estimation of central blood pressure.
Study Year Setting Attrition number Samplesize
Mean age(range)
Male(%)
CAD(%)
Central BPinvasivereferencemethoda
Sensor type and quality Central BP indexestimating methodb
Calibrationmethodc
Type of BP monitor
Karamanoglu et al. 1993 [4] CAG NS 14 53.7 (36–70) 92.9 85.7 HF 5F Millar Custom-made GTF D NAKaramanoglu andFeneley
1996 [43] CAG NS 13 58.5 92.3 84.6 HF 6F Millar SPC 360 Carotid tonometry CI NA
Chen et al. 1997 [23] CAG NS 20 59 (36–78) 80 60 HF SPC-320 Custom-made GTF(ARX model)
CI NA
Pauca et al. 2001 [25] Cardiacsurgery
NS 62 61 72.6 96.8 SF Spectramed model T36AD-R withdamping coefficient >0.3 andresonant frequency >20 Hz
GTF from SphygmoCor D NA
Van Bortel et al. 2001 [26] CAG NS 19 57 (40–79) 89.5 NS SF NS Carotid tonometry CI DinamapSoderstrom et al. 2002 [36] PTCA NS 12 67.3 (62–76) 66.7 100 SF Siemens Sircus 1281 with damping
coefficient 0.35–0.5 and resonantfrequency 25 Hz
GTF from SphygmoCor D NA
Davies et al. 2003 [30] CAG NS 28 60 71.4 82 SF Siemens Recor GTF from SphygmoCor CC1 HEM-705CPd
Hope et al. 2003 [39] CAG NS 78 63 78.2 NS SF NS Custom-made GTF (saline-filled system)
CI NA
Cloud et al. 2003 [29] CAG NS 30 63.7 (27–84) 60 57 SF NS GTF from SphygmoCor CC1 HEM-70 CPd
Smulyan et al. 2003 [24] CAG NS 50 54 (33–82) NS NS HF 6f Millar SPC 350 GTF from SphygmoCor CC1 Colin?Hope et al. 2004 [32] CAG NS 42 64 66.7 NS HF Millar Microtip Custom-made GTF CI/CC2 DinamapTM XL 9301
Portable MonitorPauca et al. 2004 [33] Cardiac
Surgery24 21 64 (41–87) 81 100 SF Spectramed model T36AD-R with
damping coefficient >0.2 andresonant frequency >20 Hz
SBP2 D NA
Hope et al.e,f 2004 [37] CAG NS 19 DM/38non-DMpatients
66/65 NS 84/87 SF NS Custom-made GTF (saline-filled system)
CI NA
Sharman et al. 2006 [38] CAG 13 30 56 (37–76) 70 70 HF Millar model SSD-1008 GTF from SphygmoCor CI NATakazawa et al. 2007 [27] CAG 2 18 61 (47–78) 83.3 NS HF Pressure Wire RADI SBP2 CC1 Colin TM 2740Hope et al. 2007 [28] CAG NS 93 61 63 NS HF Millar Microtip Custom-made GTF CI NARajani et al.e 2008 [40] Moderate
aortic stenosisundergoingCAG
NS 14 74 (54–81) 71.4 NS HF SPC-464D GTF from SphygmoCor CI/CC1 Omron 705CPd
Hickson et al. 2009 [31] CAG NS 38 60 NS NS HF 5f Millar SPC-454E GTF from SphygmoCor/SBP2 CI HEM-711A-ECheng et al. 2010 [34] CAG NS 100 61.6 78 42 HF 2f Millar SPC 320 SBP2 D Omron VP2000Zuo et al. 2010 [35] CAG 2 45 62 (33–79) 73.3 71.1 SF XDY-2003 with damping coefficient
>0.3 and resonant frequency >30 HzGTF from SphygmoCor CC1 Omron 705 CPIId
Shih et al.g 2011 [41] CAG NS 40 64.1 80.4 52.2 HF Dual sensor 2f Millar model SSD-1059 Custom-made GTF D/CC1 Microlife Watch BPOfficed
Ding et al.e 2011 [42] CAG 11 33 60.1 (45–83) 63.6 51.5 SF GE Mac-Lab System with dampingcoefficient >0.3 and resonantfrequency >20 Hz
GTF from SphygmoCor/SBP2e CC1 Omron HEM9000-AI
CAG = diagnostic cardiac catheterization for risk assessment; PTCA = percutaneous transluminal coronary angioplasty; attrition number = number of participants satisfying inclusion but not in the study; SBP = systolic blood pressure;MBP =mean blood pressure; DBP = diastolic blood pressure; NS = not stated; NA= not applicable, which indicates central BP was estimated by invasive methods (see texts of Calibration methods) in the studies without the use of sphyg-momanometers.
a HF = high fidelity catheter tip transducer; SF = saline filled system with external transducer.b GTF = generalized transfunction; SBP2 = late systolic shoulder on peripheral pressure waveforms; cuff = sphygmomanometer.c CC1 = calibrated to cuff SBP/DBP; CC2 = calibrated to cuff MBP/DBP; CI = calibrated to invasive aortic MBP/DBP; D = direct measurement.d Studies used BP monitors fulfilling the requirement of validation standards.e The estimated central BP by Omron HEM 9000-AI in this study was not included in meta-analysis because it was estimated from SBP2 and a regression equation and could confound the combined estimates of errors.f Hope et al. [37] examined GTF in 19 DM patients and 38 non-DM patients, respectively.g Hope et al. [32] and Rajani et al. [40] conducted both invasive and non-invasive calibration; Shih et al. [41] acquired peripheral waveforms by direct measurements and then recalibrated them using cuff SBP/DBP.
3H-M
.Chenget
al./InternationalJournalofCardiology
xxx(2012)
xxx–xxx
Pleasecite
thisarticle
as:ChengH-M
,etal,Measurem
entaccuracy
ofnon-invasivelyobtained
centralbloodpressure
byapplanation
tonom-
etry:Asystem
aticreview
andmeta-analysis,Int
JCardiol(2012),doi:10.1016/j.ijcard.2012.04.155

4 H-M. Cheng et al. / International Journal of Cardiology xxx (2012) xxx–xxx
3. Results
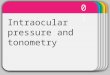
3.1. Description of search process (Fig. 2)
Fig. 2 shows the details of search process. Twenty-one out of 30 el-igible studies had extractable and sufficient outcome data from thepapers [4,23–42] or from correspondence with the authors [43].Twenty-two studies (857 subjects; mean age, 61.4 years; 69.2%male subjects) with a total of 1167 measurements were eligible forinclusion and subjected to meta-analysis in this review.
3.2. Summary of included studies
These studies were all conducted invasively in a catheterizationlaboratory or operating room and small in sample size (numberrange 12–100, mean 37.2). The majority of studies applied general-ized transfer function on peripheral pressure waveform (Fig. 1,panel B) to obtain the estimated central BP (n=17). Of the 17 studiesusing transfer function, 10 studies performed the analysis using thesoftware program and transfer function from SphygmoCor (AtCorMedical, Sydney).
3.3. Calibration methods
Current central BP estimation relies on the acquisition of peripher-al pressure waveform, mostly by applanation tonometry. If the ac-quired peripheral waveforms were not directly measured, they weresubject to calibration and then used for central BP estimation. The cal-ibration methods in these studies were detailed in Table 1.
One common approach is to calibrate peripheral waveforms tomatch the aortic mean and diastolic BP (Fig. 1, left upper panel)based on the widely accepted approach whereby mean and diastolicpressures from the central aorta to the peripheral artery have nearlythe same values [1].
Records identified through database searching
(n = 1110 )
Scr
een
ing
Incl
ud
edE
ligib
ility
Iden
tifi
cati
on Additio
identified ts
(n =
Records after duplicates removed and examined with title screening
(n = 934 )
Studies included in quantitative synthesis (n = 22) with 857 subjects
and 1167 measurements)
Records examined with abstract screening
(n = 193)
Full-text articles assessed for eligibility
(n = 40 )
Studies included in the systematic review
(n = 30)
Fig. 2. Flow chart of th
Please cite this article as: Cheng H-M, et al, Measurement accuracy of noetry: A systematic review and meta-analysis, Int J Cardiol (2012), doi:1
The other calibrating method in these primary studies is to cali-brate the peripheral waveform to match the arm BP measured bysphygmomanometers (Fig. 1, left lower panel). Peripheral waveformscould be calibrated to cuff SBP and DBP [30] or cuff MBP and DBP [32].The calibration process could become a source of measurement errorswhen cuff BP, which is not error-free, is used for calibration.
In real world clinical practice, the direct invasive measurement ofperipheral BP or calibration by invasive aortic MBP/DBP (invasivemethods) is impractical. It is essential to perform separate meta-analyses according to calibration methods (invasive methods vs.non-invasive method). Fifteen studies used invasive methods (6 bydirect measurements and 10 by invasive calibration with one con-ducted both) and 9 studies used non-invasive calibration. Two studiesconducted both invasive and non-invasive calibration for pulse wave-forms [32,40]. One study directly acquired peripheral waveforms andthen recalibrated them using cuff BP [41].
3.4. Meta-analysis of systematic bias and random error between differentBP parameters and corresponding invasive measured central BP
The 22 studies for quantitative synthesis included 857 individuals.Subjects in 4 studies [25,34,36,38] underwent repetitive measurementsafter changes in hemodynamics by exercise or medication to provokeblood pressure changes with results presented separately. The resultsof meta-analysis for systematic and random errors of different BP pa-rameters compared with corresponding invasively measured centralBP values are summarized in Table 2. Most comparisons were charac-terized by significant heterogeneity in terms of MD and SDD. Residualheterogeneity was still evident in both MD and SDD between studieswithin the subgroup of different estimating methods.
Not all studies provided comprehensive reporting on all central BP pa-rameters. Formeta-analysis, appropriate and extractable outcome data toexamine agreement between invasively measured reference central BPparameters and corresponding estimated values were available frompart of these studies as shown in Table 2 and respective Forest plots.
nal records hrough other ources 1087 )
Records excluded after evaluation of abstract (n = 153)
Flow Chart of the Search Process
Papers excluded after review of full paper(n=10), with reasons:
duplicate publication (n=2); irrelevant phenomenon of interest (n= 3), irrelevant
comparator (n= 3), irrelevant outcome (n=1) to the inclusion criteria; inconsistent results
shown in the article (n=1)
Insufficient outcome data for further meta-analysis after attempts to contact
corresponding authors (n= 8)
e search process.
n-invasively obtained central blood pressure by applanation tonom-0.1016/j.ijcard.2012.04.155

Table 2Meta-analysisa of mean difference and standard deviation of differences between different BP parameters and corresponding invasively measured central aortic BP with the het-erogeneity test across studies.
MD(systematic bias)
SDD(random error)
95% Limits ofagreementb
Chi-squareda
(MD)P value ofheterogeneitya
(MD)
Chi-squared(SDD)
P value ofheterogeneity(SDD)
df
Estimated CSBP by invasive methods(16 studies, 21 comparison, 764 measurements)c
−1.1 4.1 −9.1–6.9 424.7 b0.0001 341.8 b0.0001 20
Estimated CDBP by invasive methods(9 studies, 13 comparison, 501 measurements)
−0.5 2.1 −4.6–3.6 1792 b0.0001 207.1 b0.0001 12
Estimated CPP by invasive methods(8 studies, 10 comparison, 395 measurements)
−0.8 5.1 −10.8–9.2 148.8 b0.0001 88.1 b0.0001 9
Invasive peripheral SBP(6 studies, 9 comparison, 336 measurements)
9.1 6.9 −4.5–22.7 192.4 b0.0001 47.7 b0.0001 8
Invasive peripheral DBP(5 studies, 8 comparison, 309 measurements)
0.1 2.3 −4.4–4.6 45.8 b0.0001 53.7 b0.0001 7
Invasive peripheral PP(4 studies, 6 comparison, 285 measurements)
12.2 7.1 −3.6–24 106.1 b0.0001 8.2 0.14 5
Noninvasively estimated CSBP(9 studies, 10 comparison, 384 measurements)
−8.2 10.3 −28.4–12 112.5 b0.0001 58.9 b0.0001 9
Noninvasively estimated CDBP(8 studies, 8 comparison, 348 measurements)
7.6 8.7 −9.5–24.6 215.5 b0.0001 52.57 b0.0001 7
Noninvasively estimated CPP(5 studies, 5 comparison, 276 measurements)
−12.2 10.4 −32.5–8.1 51.3 b0.0001 89.8 b0.0001 4
Cuff SBP(11 studies, 13 comparison, 415 measurements)
5.4 11.7 −17.6–28.3 41 0.0001 54.9 b0.0001 12
Cuff DBP(8 studies, 9 comparison, 349 measurements)
7.5 8.7 −9.5–24.5 57.1 b0.0001 51.8 b0.0001 8
Cuff PP(5 studies, 6 comparison, 277 measurements)
−0.7 13.2 −26.6–25.2 25.2 0.0001 33.9 b0.0001 5
MD = mean difference; calculated by averaging differences (BP parameters in the left column−corresponding invasively measured central BP) between paired measurements.SDD = standard deviation of difference between paired measurements; SBP = systolic blood pressure; DBP = diastolic blood pressure; PP = pulse pressure; CSBP = central sys-tolic blood pressure; CDBP = central diastolic blood pressure; CPP = central pulse pressure.
a Meta-analysis and Chi-square test for method comparison studies were based on DerSimonian–Laird weights for the random effects model and homogeneity was assessedusing a standard large sample test [21,22].
b 95% limits of agreement was calculated by MD±1.96*SDD.c Number of studies, comparisons at baseline and after hemodynamic interventions from all primary studies, and total measurements for corresponding BP values were included
in parenthesis.
5H-M. Cheng et al. / International Journal of Cardiology xxx (2012) xxx–xxx
Of the invasive methods for estimation, the mean pressure differ-ences of the estimated central BP were small with MD and SDD−1.1±4.1 mm Hg (95% limits of agreement −9.1–6.9 mm Hg) forcentral SBP (Fig. 3), −0.8±5.1 mm Hg (−10.8–9.2 mm Hg) for cen-tral pulse pressure, and −0.5±2.1 mm Hg (−4.6–3.6 mm Hg) forcentral DBP, as shown in Table 2 and Forest plots. Not only the sys-tematic bias (MD) but also the random error (SDD) of the estimatedcentral SBP and pulse pressure was reduced by applying invasivemethods as compared to the differences between invasive brachialand central SBP and pulse pressure (Table 2). This suggests that thepressure amplification from the central aorta to peripheral arteriescan be treated effectively with current theoretical frameworks of cen-tral BP estimation.
However, the errors inflated to −8.2±10.3 mm Hg (−28.4–12.0 mm Hg) for estimating central SBP (Fig. 4), −12.2±10.4 mmHg (−32.5–8.1 mm Hg) for central pulse pressure, and 7.6±8.7 mm Hg (−9.5–24.6 mm Hg) for central DBP (Table 2), whenthe pressure waveform was calibrated by cuff BP. Similarly, large dif-ferences between cuff and invasive central BP have been demonstrat-ed in our meta-analysis (Table 2). As compared to cuff SBP and pulsepressure, the random error of noninvasively estimated central SBPand pulse pressure was slightly reduced. The disagreement was stillconsiderable in the subgroup analysis by different central BP methodsas well as in studies using validated cuff BP monitors. When wepooled the studies reporting the use of validated cuff BP monitorsfor measurements, the errors were found to be similar: −6.7±10.6 mm Hg (−27.4–14.1 mm Hg) for noninvasively estimated cen-tral SBP, −15.0±11.1 mm Hg (−36.7–6.6 mm Hg) for central pulsepressure, and 10.8±8.5 mm Hg (−5.9–27.6 mm Hg) for centralDBP. Likewise, the cuff BP measured with validated sphygmomanom-eters had large MD and SDD with reference to corresponding
Please cite this article as: Cheng H-M, et al, Measurement accuracy of noetry: A systematic review and meta-analysis, Int J Cardiol (2012), doi:1
invasively measured central BP: 2.8±11.4 mm Hg (−19.7–25.3 mmHg) for cuff SBP, −1.6±12.0 mm Hg (−25.1–21.9 mm Hg) for cuffpulse pressure, and 9.7±8.5 mm Hg (−7.0–26.5 mm Hg) for cuffDBP. In contrast to the considerably reduced systematic bias and ran-dom error of the invasive methods for estimating central SBP andpulse pressure, the measurement accuracy of noninvasively obtainedcentral BP is suboptimal, even when the cuff BP monitors have passedthe requirements according to international validation standards.
3.5. Device-specific results
Through comprehensive systematic search, there have been onlytwo devices which utilize applanation tonometry to estimate centralBP and had undergone invasive validation (i.e. comparing centralSBP estimates with invasively measured central BP). The two devicesare SphygmoCor using generalized transfer function approach, andHEM-9000 AI using SBP2 method, respectively, which have beenunder patent protection for estimating central hemodynamics.
3.5.1. SphygmoCor (AtCor Medical, Sydney)Of the 10 studies performing the analysis by the software program
and GTF from SphygmoCor, 4 and 5 studies used invasive method andnon-invasive calibration, respectively, and one study was conductedwith both calibration methods. Of the studies with the invasive meth-od, the errors were −2.4±3.4 mm Hg (−9.1–4.3 mm Hg) for esti-mating central SBP, −2.6±4.0 mm Hg (−10.4–5.3 mm Hg) forcentral pulse pressure, and 1.9±1.5 mm Hg (−1.2–4.9 mm Hg) forcentral diastolic BP. Again, the errors of SphygmoCor system soaredto −8.2±11.6 mm Hg (−30.9–14.5 mm Hg) for estimating centralSBP, −15.4±10.2 mm Hg (−35.3–4.6 mm Hg) for central pulse
n-invasively obtained central blood pressure by applanation tonom-0.1016/j.ijcard.2012.04.155

Generalized Transfer Function
#Karamanoglu,1993 (n=27)
Chen,1997 (n=34)
#Pauca,2001 (n=62)
*#Pauca,2001 (n=62)
#Soderstrom,2002 (n=12)
*#Soderstrom,2002 (n=12)
Hope,2003 (n=78)
&Hope,2004 (n=19)
@Hope,2004 (n=38)
Hope,2004 (n=42)
Sharman,2006 (n=30)
*Sharman,2006 (n=30)
Hope,2007 (n=63)
Rajani,2008 (n=14)
Hickson,2009 (n=38)
Shih,2011 (n=40)
Subtotal (Mantel-Haenszel weighted)
Subtotal (Random Effect Model)
SBP2
#Pauca,2004 (n=21)
Hickson,2009 (n=29)
#Cheng,2010 (n=50)
*#Cheng,2010 (n=50)
Subtotal (Mantel-Haenszel weighted)
Subtotal (Random Effect Model)
Carotid Tonometry
Karamanoglu,1996 (n=13)
Total (Mantel-Haenszel weighted)
Total (Random Effect Model)
-40 -30 -20 -10 0 10 20 30 40
2.4 (-7.8,12.6)
0 (-7.3,7.3)
0 (-8.6,8.6)
-0.2 (-8.6,8.2)
-8 (-11.9,-4.1)
-7 (-10.9,-3.1)
-0.8 (-14.3,12.7)
-6 (-19.7,7.7)
-2 (-17.7,13.7)
1 (-14.7,16.7)
-1.3 (-7.6,5)
-4.7 (-11.2,1.8)
-2 (-23.6,19.6)
-2 (-13.8,9.8)
-1 (-18.6,16.6)
-0.6 (-6.3,5.1)
-2.2 (-10,5.5)
-2.2 (-10.5,6.1)
0.6 (-2.3,3.5)
2 (-9.8,13.8)
2.5 (-6.1,11.1)
3.5 (-8.1,15.1)
1.3 (-4,6.7)
1.5 (-4.4,7.3)
1.1 (-5,7.2)
-1.1 (-8,5.9)
-1.1 (-9.1,6.9)
Mean difference (mmHg)
Mean difference(95% limits)
*:Measurements after hemodynamic transients#:Peripheral waveforms were invasively acquired
&:Measurements in patients with DM;@:Measurements in patients without DM
Fig. 3. A Forest plot of the estimated central aortic SBP obtained with invasive methods vs. measured central SBP. The invasive method indicates that the peripheral pulse waveformswere either directly acquired or calibrated to invasive aortic MBP and DBP. Subtotal pooled point estimates are shown in the Forest plot within different subgroups categorizedaccording to various methods for central SBP measurements (generalized transfer function, SBP2, and carotid tonometry). The square (or diamond for pooled point estimates)and horizontal line indicate the mean difference and 95% limits of agreement, respectively. The mean difference and 95% limits were extracted and calculated from primary studies(shown on right side), which were then pooled as subtotal or total point estimates of mean difference and its limits.
6 H-M. Cheng et al. / International Journal of Cardiology xxx (2012) xxx–xxx
pressure, and 9.3±9.8 mmHg (−9.9–28.4 mmHg) for central DBP instudies conducted with non-invasive calibration.
3.5.2. HEM-9000AI (Omron Healthcare, Kyoto, Japan)Only one invasive validation study of non-invasive central BP as-
sessment was found for HEM-9000AI [42]. HEM-9000 AI only pro-vides central SBP, which was estimated by SBP2 method with aregression equation. The error in this study for central SBP estimationwas −2.0±10.2 mm Hg (−21.9–17.9 mm Hg).
Please cite this article as: Cheng H-M, et al, Measurement accuracy of noetry: A systematic review and meta-analysis, Int J Cardiol (2012), doi:1
4. Discussion
4.1. Summary of findings
The present review has shown that although current central BP es-timating methods are acceptable by using invasive calibration, theerror of these methods was large when cuff BP was used for non-invasive calibration. The invasive methods refer to applying thesecentral BP estimating methods on the peripheral pulse waves whichare directly measured or non-invasively acquired but calibrated
n-invasively obtained central blood pressure by applanation tonom-0.1016/j.ijcard.2012.04.155

7H-M. Cheng et al. / International Journal of Cardiology xxx (2012) xxx–xxx
using invasive aortic MBP and DBP. This calibrating practice is basedon the widely accepted notion that MBP and DBP alter minimallyalong the arterial tree [1]. The findings from invasive methods suggestthat the systematic bias and random error between peripheral BP andcentral BP could be reduced considerably (Table 2 and Fig. 3) by apply-ing thesemethods to estimate central BP [4,6,43]. Nevertheless, the ef-fect of the above application diminished as for noninvasive calibration.As shown in studies conducted with noninvasive calibration by cuffBP, the errors of central BP estimation soared considerably (Table 2,
Generalized Transfer Function
#Davies,2003 (n=28)
#Cloud,2003 (n=30)
#Smulyan,2003 (n=50)
Hope,2004 (n=42)
#Rajani,2008 (n=14)
#Zuo,2010 (n=45)
#Shih,2011 (n=40)
Ding,2011 (n=99)
Subtotal (Mantel-Haenszel
weighted)
Subtotal (Random Effect Model)
SBP2
Takazawa,2007 (n=18)
*Takazawa,2007 (n=18)
Subtotal (Mantel-Haenszel
weighted)
Subtotal (Random Effect Model)
Total (Mantel-Haenszel
weighted)
Total (Random Effect Model)
-50 -40 -30 -20 -10
Mean differ*Measurements after hemodynamic transients
#Measurements using validated BP monitors
Fig. 4. A Forest plot of the noninvasively estimated central aortic SBP vs. measured central Sibrated to non-invasive cuff BP. Individual primary studies are sorted by subgroups of generidation studies of central BP measurement, none study with cuff BP-calibrated carotid tonomin this Forest plot.
Please cite this article as: Cheng H-M, et al, Measurement accuracy of noetry: A systematic review and meta-analysis, Int J Cardiol (2012), doi:1
Fig. 4), even in studies using validated sphygmomanometers. In addi-tion, there is substantial room for quality improvement in reportingand conducting primary studies according to critical appraisal results(Appendix II).
4.2. Strengths of this study
This systematic review is in response to the long-lasting debates onthe validity of current central BP measures between the hypertensive
0 10 20 30 40 50
-7.2 (-27,12.5)
-13.3 (-42.9,16.3)
-1.5 (-23.6,20.6)
-7 (-30.5,16.5)
-8 (-21.7,5.7)
-4.2 (-36.9,28.5)
-2.2 (-14.7,10.3)
-15 (-34.9,4.9)
-7.5 (-26.3,11.4)
-7.3 (-28.7,14.2)
-11.7 (-25.6,2.2)
-12.3 (-28.8,4.2)
-12 (-26.9,3)
-12 (-26.9,3)
-8.1 (-26.4,10.1)
-8.2 (-28.4,12)
ence (mmHg)
Mean difference(95% limits)
BP. The non-invasive method indicates that the peripheral pulse waveforms were cal-alized transfer function and SBP2. Through our comprehensive search for invasive val-etry has ever been reported. Therefore, no subgroup of carotid tonometry is displayed
n-invasively obtained central blood pressure by applanation tonom-0.1016/j.ijcard.2012.04.155

8 H-M. Cheng et al. / International Journal of Cardiology xxx (2012) xxx–xxx
society and request for an independent systematic review [44]. Becausewe comprehensively searched many databases, it is unlikely that weoverlooked important pertinent studies. This systematic review alsosystematically and critically appraised the study quality based on previ-ous consensus guidelines (Appendix II and Table S2).
4.3. Process of central BP estimation
The tonometry-based central BP estimating methods using gener-alized transfer function may suffer from serial errors that challengetheir applicability [41], including the robustness of the mathematicalmodeling between the peripheral and central aortic pressure wave-form [28], the quality of the acquired pressure waveform [24], vari-able pulse pressure amplification between the brachial and radialarteries when brachial blood pressure values are used for calibratingradial pressure waveform [45], and intrinsic discrepancy betweenthe invasive brachial blood pressure values and those estimatedwith cuff-based sphygmomanometers [29,30]. Therefore, carotidwaveform [4] and radial waveform with the SBP2 method [2] wereused as alternatives. However, according to subgroup analysis dem-onstrated in Figs. 3 and 4, the major source of estimation error is ap-parently not from pressure waveforms or estimating methods.
4.4. Calibration issues
We have demonstrated in a previous study that major source oferror in estimating central BP by generalized transfer function maybe from inaccurate cuff BP used for waveform calibration [41]. Inthis study, simultaneous high-fidelity brachial and central aortic pres-sure waveforms were both obtained invasively. It concluded thatmore than 96% of error in estimating central BP resulted from inaccu-rate cuff BP for calibration. The study, however, hasn't examinedother possible sources of errors, such as generalizability [28], wave-form quality [24], and brachial-to-radial pulse pressure amplification[45] based on its study design.
Current sphygmomanometers appear to be a substantial barrier tothe clinical application of the central BP concept as demonstrated inour meta-analysis results even when validated BP monitors are usedfor calibration. In real world clinical practice, all non-invasive centralBP estimating methods can only calibrate peripheral waveforms bycuff BP. As shown in the left lower panel of Fig. 1, one common cali-brating practice is to adjust the peripheral waveform to make itspeak and trough in correspondence with cuff SBP and DBP, respec-tively. However, the notion that mean and diastolic pressures fromthe central aorta to the peripheral artery have nearly the same valuesholds true only when both central and peripheral BP are measuredinvasively. It has been well recognized that there are large variationsbetween indirect and direct blood pressure measurements [46]. TakeDBP as an example, large systematic bias and random error werenoted between non-invasively estimated and measured central DBP(7.6±8.7 mm Hg) and between cuff DBP and measured central DBP(7.5±8.7 mm Hg) as shown in Table 2. It is apparent that cuff DBPconsiderably overestimates measured central DBP, which should cor-respond to invasive peripheral DBP, and introduces substantial errorsinto the estimated central DBP through the non-invasive calibratingprocess. The reason behind this is that the international standardsfor BP monitors request manufacturers to validate tested BP monitorsagainst the mercury cuff method using Korotkoff sounds [3,47], whichis actually not an accurate method to measure arm BP when it is com-pared with intra-arterial pressure [46].
A variety of calibrating methods have been proposed to improvethe non-invasive waveform calibration [45,48–50]. The calibratingmethod used in two large-scale studies, Framingham [51] andAsklepios [2], is adhered to the notion that mean BP and diastolic BPalmost remain unaltered along the arterial tree. To calibrate carotidpressure waveforms, brachial mean BP is derived from integrated
Please cite this article as: Cheng H-M, et al, Measurement accuracy of noetry: A systematic review and meta-analysis, Int J Cardiol (2012), doi:1
mean of a signal-averaged brachial pressure waveform obtained bytonometry. However, throughout our comprehensive search, thereis no invasive validation study investigating the accuracy of thismethod against invasively measured central BP. Moreover, as shownin Fig. 4, the random error of noninvasively estimated central SBP inone study using brachial mean and diastolic BP for peripheral wave-form calibration was similar to other studies [32].
4.5. Precision and accuracy
As discussed in an editorial [52], precision (random error) is im-portant for a method to be applied in clinical research, and accuracy(systematic and random error) is mandatory for clinical application.Compared with the true gold standard of invasively measured centralBP, the Achilles tendon of current central BP estimating methods isactually the random error, because systematic bias may be correctedby statistical normalization [52].
4.6. Alternative methods
Our systematic review included studies conductedwith applanationtonometry and excluded studies using different methods such as echotracking [26], finger pressure cuff [53], and brachial cuff-basedmethods[34,54]. However, these methods may suffer from similar sources oferror as discussed above and have comparable ranges of errors shownin their primary invasive validation studies.
4.7. Limitations of this review
Inadequate reporting is a common problem for systematic re-views, and this limitation also exists for method comparison studies.For several studies, even after attempts were made to obtain resultsfrom corresponding authors, direct estimates of agreement betweenindex and reference central BP measures remained unavailable.
We have shown in Appendix Table S1 that all included studieshave different degrees of methodological weakness or lack ofreporting clarity. For example, current popular techniques used to es-timate central BP rely on good waveform acquisition by applanationtonometry, which is operator dependent and a less experienced oper-ator may inevitably render the estimates less reliable or valid. Wehave examined all included studies whether the measurement is sub-ject to “reliability checking” and performed by “trained professionals”(Appendix Table S1). However, as demonstrated in the Forest plot(Figs. 3 and 4) and our previous study [41], the major influence onmeasurement accuracy may be still resulting from calibrationmethods.
The aim of this review was to systematically review all eligiblestudies and meta-analyze the results of agreement between pairedcentral BP measurements presented in these studies. Our conclusionmight be confounded by the heterogeneity of study characteristics,estimation methods, and their conduction processes. However, weobtained the same trend across studies, as presented in Forest plots.
Moreover, our conclusion for invasive calibration is probably lim-ited by the characteristics of participants enrolled in these validationstudies, such as the high percentage of males and cardiovascular dis-eases. Most studies included in this review used radial-tonometry toestimate central BP in contrast to only two studies conducted withcarotid-tonometry. More evidence from invasive validation studiessupporting the use of carotid tonometry and the calibration methodby brachial-tonometry is warranted.
4.8. Conclusion
The current tonometry-based central BP estimating methods areacceptable by using invasive calibration because they have small sys-tematic and random errors. However, the errors were evident in the
n-invasively obtained central blood pressure by applanation tonom-0.1016/j.ijcard.2012.04.155

9H-M. Cheng et al. / International Journal of Cardiology xxx (2012) xxx–xxx
validation studies when cuff BP was used for noninvasive calibration.To implement central BP concept in clinical practice, evidence of im-proved measurement accuracy of these noninvasive methods by ei-ther more accurate cuff BP or better calibration methods should bedemonstrated.
5. Perspectives
The BP amplification from central aorta to peripheral arteries,which varies substantially between subjects, causes conceivable dis-crepancy between central and peripheral BP. Noninvasive methodsfor estimating central BP are available and make it an attractive targetfor management of hypertension. We comprehensively searched andsynthesized current available evidence on measurement accuracy ofcentral BP estimating methods in this systematic review and dis-closed the existing gaps of practice and research evidence, whichmay guide future research in this area. Although the difference be-tween central and peripheral BP can be reduced considerably by ap-plying these tonometry-based estimating methods with invasivecalibration, random error of these central BP estimates conductedwith non-invasive calibration only slightly decreased as comparedwith those of cuff BP. The non-invasive calibration process using inac-curate cuff BP appears to be one of the gaps between practice and the-ory. Moreover, despite being adopted in large-scale studies, carotidtonometry and/or the calibration method by brachial-tonometryhasn't been supported by any invasive validation study, which is anapparent evidence gap. In the era of evidence-based medicine, effortsshould be made to fill the above gaps in order to facilitate possible ap-plication of the attractive central BP concept in clinical practice.
Acknowledgments
The reviewers are grateful to the following: Mr. Michael Draper,for formulating search strategies; and Dr. Mustafa Karamanoglu, forproviding his data for our review synthesis. This work was supportedby the scholarship for 2011 oversea training from Executive Yuan, Re-public of China (0980004399) and IPRS-APA 2011 Scholarship(1214836) at the University of Adelaide from Australian Government.
The authors of this manuscript have certified that they complywith the Principles of Ethical Publishing in the International Journalof Cardiology [55].
Appendix A. Supplementary data
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.ijcard.2012.04.155.
References
[1] Nichols WW, O'Rourke MF. McDonald's blood flow in arteries: theoretic, experi-mental and clinical principles. 6th ed. London: Arnold; 2011.
[2] Segers P, Mahieu D, Kips J, et al. Amplification of the pressure pulse in the upperlimb in healthy, middle-aged men and women. Hypertension 2009;54:414–20.
[3] Association for the Advancement of Medical Instrumentation. American NationalStandard. Electronic or automated sphygmomanometers. Arlington, VA: AAMI;2009.
[4] Karamanoglu M, O'Rourke MF, Avolio AP, Kelly RP. An analysis of the relationshipbetween central aortic and peripheral upper limb pressure waves in man.Eur Heart J 1993;14:160–7.
[5] Benetos A, Tsoucaris-Kupfer D, Favereau X, Corcos T, Safar M. Carotid artery to-nometry: an accurate non-invasive method for central aortic pulse pressure eval-uation. J Hypertens 1991;9(Suppl. 6):S144–5.
[6] Takazawa K, Tanaka N, Takeda K, Kurosu F, Ibukiyama C. Underestimation of vaso-dilator effects of nitroglycerin by upper limb blood pressure. Hypertension1995;26:520–3.
[7] Kelly RP, Hayward C, Ganis J, et al. Noninvasive registration of the arterial pressurepulse waveform using high-fidelity applanation tonometry. J Vasc Med Biol1989;1:142–9.
[8] Kelly RP, Gibbs HH, O'Rourke MF, et al. Nitroglycerin has more favourable effectson left ventricular afterload than apparent from measurement of pressure in a pe-ripheral artery. Eur Heart J 1990;11:138–44.
Please cite this article as: Cheng H-M, et al, Measurement accuracy of noetry: A systematic review and meta-analysis, Int J Cardiol (2012), doi:1
[9] Jiang XJ, O'Rourke MF, Jin WQ, et al. Quantification of glyceryl trinitrate effectthrough analysis of the synthesised ascending aortic pressure waveform. Heart2002;88:143–8.
[10] Mackenzie IS, McEniery CM, Dhakam Z, et al. Comparison of the effects of antihy-pertensive agents on central blood pressure and arterial stiffness in isolated sys-tolic hypertension. Hypertension 2009;54:409–13.
[11] Protogerou AD, Stergiou GS, Vlachopoulos C, Blacher J, Achimastos A. The effect ofantihypertensive drugs on central blood pressure beyond peripheral blood pres-sure. Part II: evidence for specific class-effects of antihypertensive drugs on pres-sure amplification. Curr Pharm Des 2009;15:272–89.
[12] London GM, Asmar RG, O'Rourke MF, Safar ME. Mechanism(s) of selective systolicblood pressure reduction after a low-dose combination of perindopril/indapamidein hypertensive subjects: comparison with atenolol. J Am Coll Cardiol 2004;43:92–9.
[13] Roman MJ, Devereux RB, Kizer JR, et al. Central pressure more strongly relates tovascular disease and outcome than does brachial pressure: the Strong HeartStudy. Hypertension 2007;50:197–203.
[14] Wang KL, Cheng HM, Chuang SY, et al. Central or peripheral systolic or pulse pres-sure: which best relates to target organs and future mortality? J Hypertens2009;27:461–7.
[15] Jankowski P, Kawecka-Jaszcz K, Czarnecka D, et al. Pulsatile but not steady com-ponent of blood pressure predicts cardiovascular events in coronary patients. Hy-pertension 2008;51:848–55.
[16] Williams B, Lacy PS, Thom SM, et al. Differential impact of blood pressure-loweringdrugs on central aortic pressure and clinical outcomes: principal results of the Con-duit Artery Function Evaluation (CAFE) study. Circulation 2006;113:1213–25.
[17] De Luca N, Asmar RG, London GM, O'Rourke MF, Safar ME. Selective reduc-tion of cardiac mass and central blood pressure on low-dose combinationperindopril/indapamide in hypertensive subjects. J Hypertens 2004;22:1623–30.
[18] Mancia G, De Backer G, Dominiczak A, et al. Guidelines for the management of ar-terial hypertension: the Task Force for the Management of Arterial Hypertensionof the European Society of Hypertension (ESH) and of the European Society ofCardiology (ESC). Eur Heart J 2007;28:1462–536.
[19] Vlachopoulos C, Aznaouridis K, O'Rourke MF, et al. Prediction of cardiovascularevents and all-cause mortality with central haemodynamics: a systematic reviewand meta-analysis. Eur Heart J 2010;31:1865–71.
[20] Craig JV, Lancaster GA, Taylor S, Williamson PR, Smyth RL. Infrared ear thermom-etry compared with rectal thermometry in children: a systematic review. Lancet2002;360:603–9.
[21] Williamson PR, Lancaster GA, Craig JV, Smyth RL. Meta-analysis of method com-parison studies. Stat Med 2002;21:2013–25.
[22] DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177–88.
[23] Chen CH, Nevo E, Fetics B, et al. Estimation of central aortic pressure waveform bymathematical transformation of radial tonometry pressure: validation of general-ized transfer function. Circulation 1997;95:1827–36.
[24] Smulyan H, Siddiqui DS, Carlson RJ, London GM, Safar ME. Clinical utility of aorticpulses and pressures calculated from applanated radial-artery pulses. Hyperten-sion 2003;42:150–5.
[25] Pauca AL, O'Rourke MF, Kon ND. Prospective evaluation of a method for estimat-ing ascending aortic pressure from the radial artery pressure waveform. Hyper-tension 2001;38:932–7.
[26] Van Bortel LM, Balkestein EJ, van der Heijden-Spek JJ, et al. Non-invasive assess-ment of local arterial pulse pressure: comparison of applanation tonometry andecho-tracking. J Hypertens 2001;19:1037–44.
[27] Takazawa K, Kobayashi H, Shindo N, Tanaka N, Yamashina A. Relationship be-tween radial and central arterial pulse wave and evaluation of central aortic pres-sure using the radial arterial pulse wave. Hypertens Res 2007;30:219–28.
[28] Hope SA, Meredith IT, Tay D, Cameron JD. ‘Generalizability’ of a radial-aortictransfer function for the derivation of central aortic waveform parameters.J Hypertens 2007;25:1812–20.
[29] Cloud GC, Rajkumar C, Kooner J, Cooke J, Bulpitt CJ. Estimation of central aorticpressure by SphygmoCor requires intra-arterial peripheral pressures. Clin Sci(Lond) 2003;105:219–25.
[30] Davies JI, Band MM, Pringle S, Ogston S, Struthers AD. Peripheral blood pressuremeasurement is as good as applanation tonometry at predicting ascending aorticblood pressure. J Hypertens 2003;21:571–6.
[31] Hickson SS, Butlin M, Mir FA, et al. The accuracy of central SBP determined fromthe second systolic peak of the peripheral pressure waveform. J Hypertens2009;27:1784–8.
[32] Hope SA, Meredith IT, Cameron JD. Effect of non-invasive calibration of radialwaveforms on error in transfer-function-derived central aortic waveform charac-teristics. Clin Sci (Lond) 2004;107:205–11.
[33] Pauca AL, Kon ND, O'Rourke MF. The second peak of the radial artery pressurewave represents aortic systolic pressure in hypertensive and elderly patients.Br J Anaesth 2004;92:651–7.
[34] Cheng HM, Wang KL, Chen YH, et al. Estimation of central systolic blood pressureusing an oscillometric blood pressure monitor. Hypertens Res 2010;33:592–9.
[35] Zuo JL, Li Y, Yan ZJ, et al. Validation of the central blood pressure estimation by theSphygmoCor system in Chinese. Blood Press Monit 2010;15:268–74.
[36] Soderstrom S, Nyberg G, O'Rourke MF, Sellgren J, Ponten J. Can a clinically usefulaortic pressure wave be derived from a radial pressure wave? Br J Anaesth2002;88:481–8.
[37] Hope SA, Tay DB, Meredith IT, Cameron JD. Use of arterial transfer functions forthe derivation of central aortic waveform characteristics in subjects with type 2diabetes and cardiovascular disease. Diabetes Care 2004;27:746–51.
n-invasively obtained central blood pressure by applanation tonom-0.1016/j.ijcard.2012.04.155

10 H-M. Cheng et al. / International Journal of Cardiology xxx (2012) xxx–xxx
[38] Sharman JE, Lim R, Qasem AM, et al. Validation of a generalized transfer functionto noninvasively derive central blood pressure during exercise. Hypertension2006;47:1203–8.
[39] Hope SA, Tay DB, Meredith IT, Cameron JD. Use of arterial transfer functions forthe derivation of aortic waveform characteristics. J Hypertens 2003;21:1299–305.
[40] Rajani R, Chowienczyk P, Redwood S, Guilcher A, Chambers JB. The noninvasiveestimation of central aortic blood pressure in patients with aortic stenosis.J Hypertens 2008;26:2381–8.
[41] Shih YT, ChengHM, Sung SH, HuWC, Chen CH. Quantification of the calibration errorin the transfer function-derived central aortic blood pressures. Am J Hypertens2011;24:1312–7.
[42] Ding FH, Fan WX, Zhang RY, et al. Validation of the noninvasive assessment ofcentral blood pressure by the SphygmoCor and Omron devices against the inva-sive catheter measurement. Am J Hypertens 2011;24:1306–11.
[43] Karamanoglu M, Feneley MP. Derivation of the ascending aortic-carotid pressuretransfer function with an arterial model. Am J Physiol Heart Circ Physiol1996;271:H2399–404.
[44] Khoshdel AR. Time to end a doubt: is pulse wave analysis a valid measure for cen-tral arterial blood pressure and arterial stiffness? J Hypertens 2007;25:724–5.
[45] Verbeke F, Segers P, Heireman S, et al. Noninvasive assessment of local pulsepressure: importance of brachial-to-radial pressure amplification. Hypertension2005;46:244–8.
[46] Smulyan H, Safar ME. Blood pressure measurement: retrospective and prospec-tive views. Am J Hypertens 2011;24:628–34.
Please cite this article as: Cheng H-M, et al, Measurement accuracy of noetry: A systematic review and meta-analysis, Int J Cardiol (2012), doi:1
[47] O'Rourke MF, Adji A. Noninvasive studies of central aortic pressure. Current Hy-pertension Reports 2012;14(1):8–20.
[48] Bos WJ, Verrij E, Vincent HH, et al. How to assess mean blood pressure properly atthe brachial artery level. J Hypertens 2007;25:751–5.
[49] Dart AM, Cameron JD, Gatzka CD, et al. Similar effects of treatment on central andbrachial blood pressures in older hypertensive subjects in the Second AustralianNational Blood Pressure Trial. Hypertension 2007;49:1242–7.
[50] Mahieu D, Kips J, Rietzschel ER, et al. Noninvasive assessment of central and pe-ripheral arterial pressure (waveforms): implications of calibration methods.J Hypertens 2010;28:300–5.
[51] Mitchell GF, Hwang SJ, Vasan RS, et al. Arterial stiffness and cardiovascular events:the Framingham Heart Study. Circulation 2010;121:505–11.
[52] Boutouyrie P, Alivon M, Herbert A. Precision, accuracy and added value of centralpressure measurement. J Hypertens 2011;29:1059–60.
[53] Munir S, Guilcher A, Kamalesh T, et al. Peripheral augmentation index defines the re-lationship between central and peripheral pulse pressure. Hypertension 2008;51:112–8.
[54] Weber T, Wassertheurer S, Rammer M, et al. Validation of a brachial cuff-basedmethod for estimating central systolic blood pressure. Hypertension 2011;58:825–32.
[55] Coats AJ, Shewan LG. Statement on authorship and publishing ethics in the inter-national journal of cardiology. Int J Cardiol 2011;153:239–40.
n-invasively obtained central blood pressure by applanation tonom-0.1016/j.ijcard.2012.04.155