Embed Size (px)
Citation preview

Journal of Neurology, Neurosurgery, and Psychiatry 1993;56:125-134
NEUROLOGICAL EMERGENCY
Tonic clonic status epilepticus
Simon Shorvon
Tonic clonic status epilepticus can be definedas a condition in which prolonged or recur-rent tonic clonic seizures persist for 30 min-utes or more. From indirect studies, theannual incidence of tonic clonic status hasbeen estimated to be approximately 18-28cases per 100 000 persons (9-14 000 newcases each year in the UK, or 45-70 000cases in the USA).'2 It is most frequent inchildren, the mentally handicapped, and inthose with structural cerebral pathology(especially in the frontal areas). In establishedepilepsy, status may be precipitated by drugwithdrawal, intercurrent illness or metabolicdisturbance, or the progression of the under-lying disease, and is more common in symp-tomatic than in idiopathic epilepsy. About 5%of all epileptic adult clinic patients will have atleast one episode of status in the course oftheir epilepsy,'2 and in children the propor-tion is higher (10-25%).'-' Most statusepisodes, however, do not develop in knownepileptic patients, and in such cases arealmost always due to acute cerebral distur-bances; common causes are cerebral infec-tion, trauma, cerebrovascular disease,cerebral tumour, acute toxic or metabolicdisturbance, febrile illness (in children).Recent studies have shown status to accountfor about 3-5% of admissions to neurologicalintensive care,4 and 0>13% of all visits to auniversity hospital casualty department.5 Themortality of tonic clonic status is about5-10%, most patients dying of the underlyingcondition, rather than the status itself or itstreatment.' 2 Permanent neurological andmental deterioration may result from status,particularly in young children, the risks ofmorbidity being greatly increased the longerthe duration of the status episode.36 Tonicclonic status is only one of the forms of statusepilepticus (see table 1), and indeed is not themost common. Nevertheless, unlike othertypes, it is a medical emergency. Treatment isurgent because the longer seizures continue,the worse the outcome and the more haz-ardous is therapy. Successful management is abalance between the conflicting requirementsof controlling seizure activity as quickly aspossible, and minimising physiologicalchanges and medical complications.
Pathophysiology of tonic clonic statusepilepticusThe pattern of seizures in tonic clonic status
evolves over time. There is often a premoni-tory stage of minutes or hours, during whichepileptic activity increases in frequency orseverity from its habitual level. This clinicaldeterioration is an augury, often stereotypic,of impending status, and urgent therapy maywell prevent its full development. At the onsetof status, the attacks typically take the form ofdiscrete grand mal seizures. As time passes,however, the convulsive motor activity oftenevolves, first to become continuous, and thenclonic jerking becomes less pronounced andless severe, and finally ceases altogether. Thisis the stage of "subtle status epilepticus",7 bywhich time, the patient will be deeply uncon-sciousness, and the prognosis is poor. In par-allel to this clinical evolution, there is alsosometimes a progressive change in the EEG,9although how consistently such a progressiveclinical and EEG pattern occurs is notknown. Autonomic changes in status can beprofound, and dominate the clinical picture,These include hyperpyrexia, tachycardia, car-diac arrhythmia, blood pressure changes,apnoea, sweating, hypersecretion and massivenoradrenalin and adrenalin release. Otherprofound endocrine changes also occur.The physiological changes in status are
often divided into two phases, the transitionfrom phase 1 to 2 occurring after about 30-60minutes of continuous seizures.2 10-12 Whilstthis is a generally useful concept, it must be
Table 1 Classification of status epilepticus (derivedfromShorvon 2)
STATUS EPILEPTICUS CONFINED TO THENEONATAL PERIODNeonatal statusStatus in neonatal epilepsy syndromesSTATUS EPILEPTICUS CONFINED TO INFANCYAND CHILDHOODInfantile spasm (West syndrome)Febrile status epilepticusStatus in childhood myoclonic syndromesStatus in benign childhood partial epilepsy syndromesElectrical status during slow wave sleep (ESES)Syndrome of acquired epileptic aphasiaSTATUS EPILEPTICUS OCCURRING INCHILDHOOD AND ADULT LIFETonic clonic statusAbsence statusEpilepsia partialis continua (EPC)Myoclonic status in comaSpecific forms of status in mental retardationMyoclonic status in other epilepsy syndromesNonconvulsive simple partial nonconvulsive statusComplex partial statusBoundary syndromesSTATUS EPILEPTICUS CONFINED TO ADULT LIFEDe Novo absence status of late onset
Institute ofNeurology,National Hospital forNeurology andNeurosurgery, Londonand the NationalSociety for Epilepsy,Chalfont, Bucks, UKS ShorvonCorrespondence to:Dr. Shorvon, Institute ofNeurology, Queen Square,London WC1N 3BG, UKReceived 4 November 1992.Accepted 5 November 1992
125 on M
arch 25, 2022 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.2.125 on 1 February 1993. D
ownloaded from

Shorvon
recognised that there is great variation. Boththe rate and extent of physiological changeare dependent on many other factors, includ-ing the anatomical site of the epileptic focus,the severity of the seizures, the underlyingaetiology and the treatment employed.Nevertheless, this staging of changes is help-ful in devising a rational plan for therapy.
Phase 1From the onset of status, seizure activitygreatly increases cerebral metabolism.Physiological mechanisms are initially suffi-cient largely to compensate for this pertuba-tion. Cerebral blood flow is greatly increased,and initially the delivery of glucose to theactive cerebral tissue is maintained. Latersystemic and cerebral lactate levels rise, and aprofound lactic acidosis may develop."3 Thereare massive cardiovascular and autonomicchanges. Blood pressure rises, as does cardiacoutput and rate. The autonomic changesresult in sweating, hyperpyrexia, bronchialsecretion, salivation and vomniting, and adren-alin and noradrenalin release. Endocrine andautonomic changes also cause an early rise insugar levels.
Phase 2As the seizure activity progresses, the com-pensatory physiological mechanisms begin tofail. Cerebral autoregulation breaks downprogressively, and thus cerebral blood flowbecomes increasingly dependent on systemicblood pressure."'"2 Hypotension develops dueto seizure-related autonomic and cardiores-piratory changes and drug treatment, and interminal stages may be severe. The fallingblood pressure results in falling cerebralblood flow and cerebral metabolism. Thehigh metabolic demands of the epileptic cere-bral tissue cannot be met and ischaemic ormetabolic damage may ensue.'1'6 The ten-dency to hypotension can be greatly exacer-bated by intravenous antiepileptic drugtherapy, especially if infusion rates are toofast. Pressor agents are often necessary inprolonged therapy.
Systemic and cerebral hypoxia are com-mon in status, due to: central respiratory fail-ure (greatly exacerbated by drug medication);the increased oxygen requirements of convul-sions; and later pulmonary artery hyperten-sion and pulmonary oedema.23" Because ofthis, assisted ventilation is often requiredearly in the course of status.
Intracranial pressure may rise precipitouslyin status. The combined effects of systemichypotension and intracranial hypertensioncan result in a compromised cerebral circula-tion and cerebral oedema, particularly in chil-dren.'2 Intracranial pressure monitoring isadvisable in prolonged severe status, especial-ly in children, when raised intracranial pres-sure is suspected; the need for active medicalor surgical therapy is, however, largely deter-mined by underlying pathology.
Cardiovascular changes in late status canalso be serious. Pulmonary hypertension andoedema are frequent, even in the presence of
systemic hypotension. Pulmonary artery pres-sures can rise to dangerous levels, well inexcess of the osmotic pressure of blood, caus-ing oedema and stretch injuries to lung capil-laries.'7 Cardiac arrhythmias in status are theresult of direct seizure-related autonomicactivation, catecholamine release, hypogly-caemia, lactic acidosis, electrolyte distur-bance, or cardiotoxic therapy. The autonomiceffects are sometimes caused by simultaneousdischarges in sympathetic and parasympa-thetic pathways. Intravenous sedativesdepress cardiac function, and the drug effectscan be potentiated by pre-existing compro-mise of cardiac function. Inspite of the greatlyincreased demand, cardiac output can falldue to decreasing left ventricular contractilityand stroke volume,'8 causing cardiac failure.The prodigious noradrenalin and adrenalinrelease also contribute to the cardiac dysfunc-tion, arrhythmia and tachycardia. Measuresto control cardiac failure and arrythmia areoften needed.
Spectacular hyperpyrexia can also developin status,7 1" and may also require specifictreatment.
There are many metabolic and endocrinedisturbances in status, the commonest andmost important are: acidosis (includinglactic acidosis), hypoglycaemia, hypo/hyper-kalaemia, and hyponatraemia. Lactic acidosisis almost invariable in major status epilepti-cus,"3 from its onset, due to neuronal andmuscle activity, the acceleration of glycolysis,tissue hypoxia, impaired respiration, and cat-echolamine release. Acute tubular necrosisdue to myoglobinuria or dehydration, andoccasionally fulminant renal failure mayoccur. Hepatic failure is a not uncommon ter-minal event in status, due to other physiologi-cal disturbances, drug treatment orunderlying disease. Rhabdomyolysis, result-ing from persistent convulsive movements,can develop early in status and precipitaterenal failure if severe, and can be preventedby artificial ventilation and paralysing drugs.Disseminated intravascular coagulation isanother rare but serious development in sta-tus which will require urgent therapy. Othermedical complications in status are listed intable 2, and are usually due to the autonomicactivity, seizures or drug treatment.
Aniepileptic drug pharmacologyAs fast drug absorption is essential in status,all drugs are administered parenterally.Midazolam and paraldehyde can be givenintramuscularly, diazepam midazolam andparaldehyde by the rectal route, but all othersmust be given by intravenous injection. It isdesirable in status for drugs to have a rapid-onset and a prolonged duration of action.Unfortunately, rapidly-acting drugs areusually highly lipid soluble (for example,diazepam, midazolam, chlormethiazole,propofol), tending to redistribute quicklyfrom cerebral tissue to accumulate in the larg-er peripheral lipid compartments (fat stores).Because of this, after a single intravenous
126 on M
arch 25, 2022 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.2.125 on 1 February 1993. D
ownloaded from

Tonic clonic status epilepticus
Table 2: Medical complications in tonic clonic statusepilepticus (derivedfrom Shorvon2)
Cerebral:
Hypoxic/metabolic cerebral damageSeizure-induced cerebral damageCerebral oedema and raised intracranial pressureCerebral venous thrombosisCerebral haemorrhage and infarction
Cardiovascular, respiratory and autonomic:
HypotensionHypertensionCardiac failure, tachy- and brady-arrhythmia, arrestCardiogenic shockRespiratory failureDisturbances of respiratory rate and rhythm, apnoeaPulmonary oedema, hypertension, embolismPneumonia, aspirationHyperpyrexiaSweating, hypersecretion, tracheo-bronchial obstructionPeripheral ischaemia
Metabolic:
DehydrationElectrolyte disturbance (especially hyponatraemia,
hyperkalaemia, hypoglycaemia)Acute renal failure (especially acute tubular necrosis)Acute hepatic failureAcute pancreatitis
Other:
Disseminated intravascular coagulopathy/multi-organfailure
RhabdomyolysisFracturesInfections (especially pulmonary, skin, urinary)Thrombophlebitis, dermal injury
injection, there is a rapid fall in cerebral druglevels; the initial injection has therefore a
short-lived effect. Repeated dosing of suchlipid-soluble drugs results in progressive drugaccumulation in the fat stores. The clinicaleffect of subsequent doses will therefore differgreatly from that of the first injection, asredistribution to the already drug-rich fatstores will not readily occur. In this situation,new drug administration can cause very highcerebral levels which persist for long periodsof time. These high levels may precipitatehypotension, sedation or cardiorespiratoryfailure; a serious risk with the repeatedadministration of diazepam, midazolam,chlormethiazole, clonazepam, pentobarbi-tone, or thiopentone. Less lipid soluble drugsare relatively slower to act, but have a muchlonger-lasting effect without a high risk ofaccumulation (for example, phenytoin,lorazepam, phenobarbitone). For lipid-solu-ble drugs, the rate of injection must also becarefully monitored, as too rapid a rate ofadministration will cause very high cerebrallevels, and the risk of sudden cardio-respira-tory arrest or hypotension. For less lipid solu-ble drugs (such as, lorazepam), the rate ofinjection is not critical. An ideal antiepilepticdrug: should have no active metabolites(diazepam, midazolam, lignocaine andthiopentone have active metabolites); shouldnot interact with other medication; shouldnot have saturable metabolism (both pheny-toin and thiopentone have saturable pharma-cokinetics at therapeutic levels); should notbe unduly affected by hepatic or renal bloodflow or disease (chlormethiazole is an exam-
ple of a drug whose metabolism is greatlyeffected by both hepatic disease and changesin hepatic blood flow); should show no ten-dency to autoinduction (thiopentone, pheno-barbitone and phenytoin are all subject to
strong autoinduction); should have strongantiepileptic action (the non-barbiturateanaesthetics have little or no intrinsicantiepileptic action, a conundrum for theiruse in status which has not been fullyexplored); should be stable in solution andunreactive with giving sets (a problem withparaldehyde, diazepam, thiopentone).
General measuresFor the new patient presenting as an emer-gency in status, it is helpful to plan therapy ina series of progressive phases (table 3).
First stage (0-10 minutes):1) Oxygen and cardio-respiratory resuscitation:It is first essential to assess cardio-respiratoryfunction, to secure the airway and resuscitatewhere necessary. Oxygen should always toadministered, as hypoxia is often un-expectedly severe.
Second stage (1-60 minutes):1) Monitoring Regular neurological obser-vations, measurements of pulse, blood pres-sure, ECG and temperature should beinitiated. Metabolic abnormalities may causestatus, or develop during its course, and bio-chemical, blood gasses, pH, clotting andhaematological measures should be moni-tored.2) Emergency anticonvulsant therapy: shouldbe started (see below)3) Intraveous lines should be set up for fluidreplacement and drug administration (prefer-ably with 0 9% sodium chloride (normalsaline) rather than 5% glucose solutions).Drugs should not be mixed, and if twoantiepileptic drugs are needed (for example,phenytoin and diazepam), two intravenouslines should be sited. The lines should be inlarge veins, as many antiepileptic drugs causephlebitis and thrombosis at the site ofinfusion. Arterial lines must never be used fordrug administration.4) Emergency investigations: Blood should
Table 3 General measures (derivedfrom Shorvon2)
1 (0-10 minutes):Assess cardiorespiratory functionSecure airway and resuscitateAdminister oxygen
2 (0-60 minutes):Institute regular monitoring (see text)Emergency antiepileptic drug therapy (see text)Set up intravenous linesEmergency investigations (see text)Administer glucose (50 ml of 50% solution) and/orintravenous thiamine (250 mg) as HPIV parenterovite)where appropriateTreat acidosis if severe
3 (0-60/90 minutes)Establish aetiologyIdentify and treat medical complicationsPressor therapy where appropriate
4 (30-90 minutes)Transfer to intensive careEstablish intensive care and EEG monitoring (see text)Initiate seizure and EEG monitoringInitiate intracranial pressure monitoring where appropriateInitiate long-term maintenance antiepileptic therapy
These 4 stages should be followed chronologically; the firstand second withi 10 minutes, and stage 4 (transfer to ITU) inmost settings within 60/90 minutes of presentation.
127 on M
arch 25, 2022 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.2.125 on 1 February 1993. D
ownloaded from

Shorvon
be drawn for the emergency measurement ofblood gases, sugar, renal and liver function,calcium and magnesium levels, full haemato-logical screen (including platelets), bloodclotting measures, and anticonvulsant levels.50 ml of serum should also be saved forfuture analysis especially if the cause of thestatus is uncertain. Other investigationsdepend on the clinical circumstances.5) Intravenous glucose and thiamine: Fifty mlof a 50% glucose solution should be givenimmediately by intravenous injection if hypo-glycaemia is suspected. If there is a history ofalcoholism, or other compromised nutritionalstates, 250 mg of thiamine (for example, asthe high potency intravenous formulation ofParenterovite, 10 ml of which contains250 mg) should also be given intravenously.This is particularly important if glucose hasbeen administered, as a glucose infusionincreases the risk of Wernicke's encephalopa-thy in susceptible patients. Intravenous highdosage thiamine should be given slowly (forexample, 10 ml of high potency Parenterovite(over 10 minutes), with facilities for treatingthe anaphylaxis which is a potentially seriousside effect of parenterovite infusions. Routineglucose administration in non-hypoglycaemicpatients should be avoided as there is someevidence that this can aggravate neuronaldamage.6) Acidosis: If acidosis is severe, the admin-istration of bicarbonate has been advocated inthe hope of preventing shock, and mitigatingthe effects of hypotension and low cerebralblood flow. In most cases, however, this isunnecessary and more effective is the rapidcontrol of respiration and abolition of motorseizure activity.
Third stage (1-60190 minutes)1) Establish aetiology: The ranges of causesof status depend primarily on age, the pres-ence or absence of established epilepsy, andthe investigations required depend onclinical circumstances. CT scanning and CSFexamination are often necessary, the lattershould be carried out only with facilities forresuscitation available as intracranial pressureis often elevated in status.
If the status has been precipitated by drugwithdrawal, the immediate restitution of thewithdrawn drug, even at lower doses, willusually rapidly terminate the status.2) Physiological changes and medical complica-tions: The physiological changes of uncom-pensated status, listed above, may requirespecific therapy. Active treatment is mostcommonly required for: hypoxia, hypoten-sion, raised intracranial pressure, pulmonaryoedema and hypertension, cardiac arryth-mias, cardiac failure, lactic acidosis,hyperpyrexia, hypoglycaemia, electrolyte dis-turbance, acute hepatic or renal failure, rhab-domyolysis, disseminated intravascularcoagulation.3) Pressor therapy: Dopamine is the mostcommonly used pressor agent, given by con-tinuous intravenous infusion. The doseshould be titrated to the desired haemody-
namic and renal responses (usually initiallybetween 2-5,pg/kg/minutes, but this can beincreased to over 20 pug/kg/minutes in severehypotension). Dopamine should be given intoa large vein as extravasation causes tissuenecrosis. ECG monitoring is required, asconduction defects may occur, and particularcare is needed in dosing in the presence ofcardiac failure.
Fourth stage (30-90 minutes):1) Intensive care: If seizures are continuinginspite of the measures taken above, thepatient must be transferred to an intensivecare environment, and the usual intensivecare measures instituted.2) Intensive care monitoring: In severe estab-lished status, intensive monitoring may berequired, including: intra-arterial blood pres-sure, capnography, oximetry, central venouspressure and Swan-Ganz monitoring.3) Seizure and EEG monitoring: In pro-longed status, or in comatose ventilatedpatients, motor activity can be barely visible.In this situation, continuous EEG monitoringusing a full EEG or a cerebral functionmonitor is necessary. The latter must becalibrated individually, and then can registerboth burst suppression and seizure activity.Burst suppression provides an arbitrary physi-ological target for the titration of barbiturateor anaesthetic therapy. Drug dosing is com-monly set at a level which will produce burstsuppression with interburst intervals ofbetween 2-30 seconds.4) Intracranial pressure (ICP) monitoring andcerebral oedema: Continuous ICP monitor-ing is advisable, especially in children in thepresence of persisting, severe or progressiveelevated intracranial pressure. The need foractive therapy is usually determined by theunderlying cause rather than the status.Intermittent positive pressure ventilation,high-dose corticosteroid therapy (4 mg dex-amethasone every 6 hours), or mannitol infu-sion may be used (the latter is usuallyreserved for temporary respite for patients indanger of tentorial coning). Neurosurgicaldecompression is occasionally required.5) Long-term anticonvulsant therapy: Long-term maintenance anticonvulsant therapymust be given in tandem with emergencytreatment. The choice of drug depends onprevious therapy, the type of epilepsy and theclinical setting. If phenytoin or phenobarbi-tone have been used in emergency treatment,maintenance doses can be continued orally(through a nasogastric tube) guided by serumlevel monitoring. Other maintenanceantiepileptics can be started also, giving oralloading doses.
Stages in drug treatmentThe drug treatment of tonic clonic statusepilepticus can also be usefully divided intostages2 (table 4). A suggested regime for atypical new case presenting as an emergencyis given in table 5.
128 on M
arch 25, 2022 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.2.125 on 1 February 1993. D
ownloaded from
Tonic clonic status epilepticus
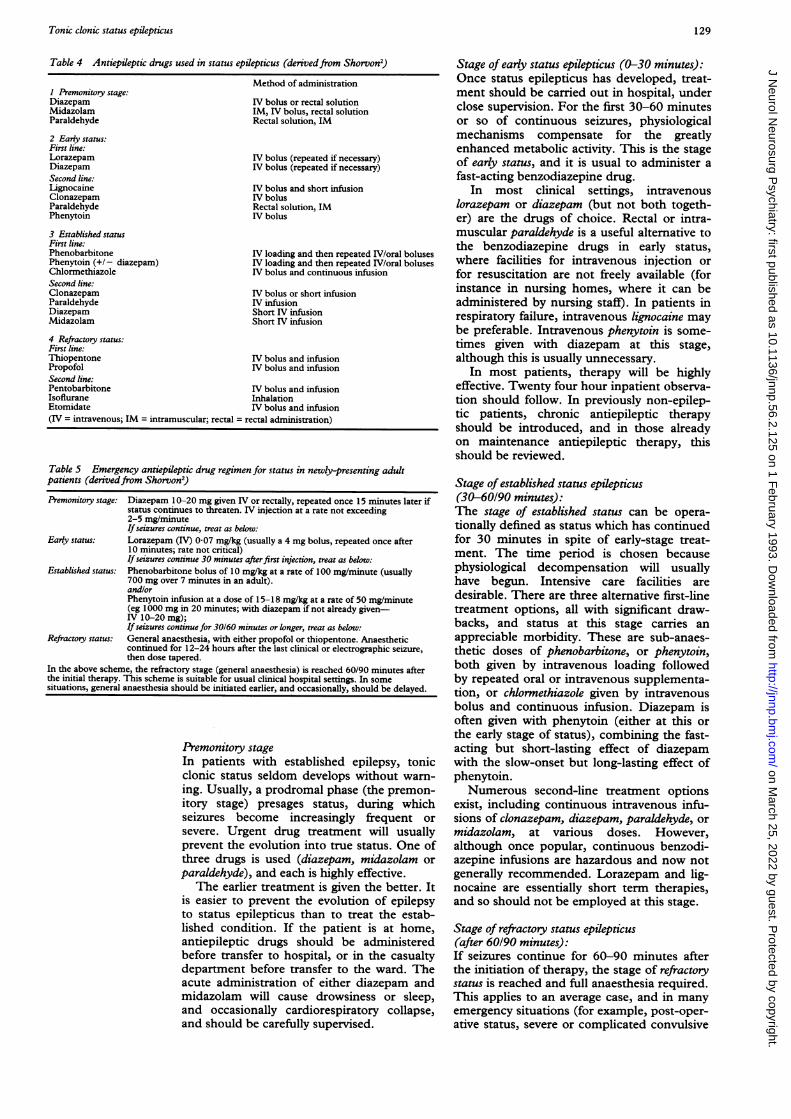
Table 4 Antiepileptic drugs used in status epilepticus (derivedfrom Shorvon')
I Premonitory stage:DiazepamMidazolamParaldehyde
2 Early status:First line:LorazepamDiazepamSecond line:LignocaineClonazepamParaldehydePhenytoin
3 Established statusFirst line:PhenobarbitonePhenytoin (+/- diazepam)ChlormethiazoleSecond line:ClonazepamParaldehydeDiazepamMidazolam
Method of administration
IV bolus or rectal solutionIM, IV bolus, rectal solutionRectal solution, IM
IV bolus (repeated if necessary)IV bolus (repeated if necessary)
IV bolus and short infusionIV bolusRectal solution, IMIV bolus
IV loading and then repeated IV/oral bolusesIV loading and then repeated IV/oral bolusesIV bolus and continuous infusion
IV bolus or short infusionIV infusionShort IV infusionShort IV infusion
4 Refractory status:First line:Thiopentone IV bolus and infusionPropofol IV bolus and infusionSecond line:Pentobarbitone IV bolus and infusionIsoflurane InhalationEtomidate IV bolus and infusion(IV = intravenous; IM = intramuscular; rectal = rectal administration)
Table 5 Emergency antiepileptic drug regimen for status in newly-presenting adultpatients (derivedfrom Shorvon2)
Premonitory stage: Diazepam 10-20 mg given IV or rectally, repeated once 15 minutes later ifstatus continues to threaten. IV injection at a rate not exceeding2-5 mg/minuteIf seizures continue, treat as below:
Early status: Lorazepam (IV) 0-07 mg/kg (usually a 4 mg bolus, repeated once after10 minutes; rate not critical)If seizures continue 30 minutes afterfirst injection, treat as below:
Established status: Phenobarbitone bolus of 10 mg/kg at a rate of 100 mg/minute (usually700 mg over 7 minutes in an adult).and/orPhenytoin infusion at a dose of 15-18 mg/kg at a rate of 50 mg/minute(eg 1000 mg in 20 minutes; with diazepam if not already given-IV 10-20 mg);If seizures continue for 30160 minutes or longer, treat as below:
Refractory status: General anaesthesia, with either propofol or thiopentone. Anaestheticcontinued for 12-24 hours after the last clinical or electrographic seizure,then dose tapered.
In the above scheme, the refractory stage (general anaesthesia) is reached 60/90 minutes afterthe initial therapy. This scheme is suitable for usual clinical hospital settings. In somesituations, general anaesthesia should be initiated earlier, and occasionally, should be delayed.
Premonitory stageIn patients with established epilepsy, tonicclonic status seldom develops without warn-ing. Usually, a prodromal phase (the premon-itory stage) presages status, during whichseizures become increasingly frequent orsevere. Urgent drug treatment will usuallyprevent the evolution into true status. One ofthree drugs is used (diazepam, midazolam orparaldehyde), and each is highly effective.
The earlier treatment is given the better. Itis easier to prevent the evolution of epilepsyto status epilepticus than to treat the estab-lished condition. If the patient is at home,antiepileptic drugs should be administeredbefore transfer to hospital, or in the casualtydepartment before transfer to the ward. Theacute administration of either diazepam andmidazolam will cause drowsiness or sleep,and occasionally cardiorespiratory collapse,and should be carefully supervised.
Stage of early status epilepticus (0-30 minutes):Once status epilepticus has developed, treat-ment should be carried out in hospital, underclose supervision. For the first 30-60 minutesor so of continuous seizures, physiologicalmechanisms compensate for the greatlyenhanced metabolic activity. This is the stageof early status, and it is usual to administer afast-acting benzodiazepine drug.
In most clinical settings, intravenouslorazepam or diazepam (but not both togeth-er) are the drugs of choice. Rectal or intra-muscular paraldehyde is a useful alternative tothe benzodiazepine drugs in early status,where facilities for intravenous injection orfor resuscitation are not freely available (forinstance in nursing homes, where it can beadministered by nursing staff). In patients inrespiratory failure, intravenous lignocaine maybe preferable. Intravenous phenytoin is some-times given with diazepam at this stage,although this is usually unnecessary.
In most patients, therapy will be highlyeffective. Twenty four hour inpatient observa-tion should follow. In previously non-epilep-tic patients, chronic antiepileptic therapyshould be introduced, and in those alreadyon maintenance antiepileptic therapy, thisshould be reviewed.
Stage of established status epilepticus(30-60/90 minutes):The stage of established status can be opera-tionally defined as status which has continuedfor 30 minutes in spite of early-stage treat-ment. The time period is chosen becausephysiological decompensation will usuallyhave begun. Intensive care facilities aredesirable. There are three alternative first-linetreatment options, all with significant draw-backs, and status at this stage carries anappreciable morbidity. These are sub-anaes-thetic doses of phenobarbitone, or phenytoin,both given by intravenous loading followedby repeated oral or intravenous supplementa-tion, or chlormethiazole given by intravenousbolus and continuous infusion. Diazepam isoften given with phenytoin (either at this orthe early stage of status), combining the fast-acting but short-lasting effect of diazepamwith the slow-onset but long-lasting effect ofphenytoin.Numerous second-line treatment options
exist, including continuous intravenous infu-sions of clonazepam, diazepam, paraldehyde, ormidazolam, at various doses. However,although once popular, continuous benzodi-azepine infusions are hazardous and now notgenerally recommended. Lorazepam and lig-nocaine are essentially short term therapies,and so should not be employed at this stage.
Stage of refractory status epilepticus(after 60/90 minutes):If seizures continue for 60-90 minutes afterthe initiation of therapy, the stage of refractorystatus is reached and full anaesthesia required.This applies to an average case, and in manyemergency situations (for example, post-oper-ative status, severe or complicated convulsive
129 on M
arch 25, 2022 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.2.125 on 1 February 1993. D
ownloaded from

Shorvon
status, patients already in ITU), anaesthesiacan and should be introduced earlier.Prognosis will now be much poorer, andthere is a high mortality and morbidity.
Anaesthesia can be induced by barbiturateor non-barbiturate drugs. A number of anaes-thetics have been administered, although fewhave been subjected to formal evaluation andall have drawbacks. The most commonlyused anaesthetics are: the intravenous barbi-turate thiopentone, or the intravenous non-barbiturate propofol. Other drugs in currentuse include the infusional anaesthetic isoflu-rane, and intravenous anaesthetics pentobarbi-tone (not available in the UK) and etomidate.
Patients require the full range of intensivecare facilities, including EEG monitoring,and care should be shared between anaes-thetist and neurologist. Experience with long-term administration (hours or days) of thenewer anaesthetic drugs is very limited. Thenon-barbiturate anaesthetics have little intrin-sic antiepileptic activity (indeed some are pro-convulsant), but it is not clear to what extent(if any) this is a disadvantage. The modemanaesthetics, on the other hand, have impor-tant pharmacokinetic advantages over themore traditional barbiturates.
Antiepileptic drugsDiazepam:Diazepam192" has a time honoured place as adrug of first choice in premonitory or earlystages of status. Its pharmacology and clinicaleffects have been extensively studied inadults, children and the newborn, and it hasbeen shown to be highly effective in a widerange of status types. Diazepam can be givenby intravenous bolus injections or by the rec-tal route in the premonitory stage, and has arapid onset of action. Sufficient cerebral lev-els are reached within one minute of a stan-dard intravenous injection, and rectaladministration produces peak levels at about20 minutes. The drug is rapidly redistributed,and has a relatively short duration of actionafter a single intravenous injection. Afterrepeated dosing, as drug concentrations inthe peripheral compartments (lipid stores)increase, this redistribution does not occur.Thus repeated bolus injections produce highpeak levels which persist, carrying an atten-dant risk of sudden and unexpected CNSdepression and cardiorespiratory collapse.Diazepam is metabolised by hepatic microso-mal enzymes. Respiratory depression,hypotension and sedation are the principalside-effects. Sudden apnoea can occur, espe-cially after repeated injections or if the injec-tion is administered at too fast a rate.
Bolus intravenous doses of diazepamshould be given in an undiluted form at a ratenot exceeding 2-5 mg/minute, using theDiazemuls formulation. Diazepam may begiven rectally, either in its intravenous prepa-ration infused from a syringe via a plasticcatheter, or as the ready made proprietaryrectal tube preparation Stesolid, the latter is aconvenient and easy method. Diazepam sup-
positories should not be used, as absorption istoo slow. The adult bolus intravenous or rec-tal dose in status is 10-20 mg, and additional10 mg doses can be given at 15 minute inter-vals, to a maximum of 40 mg. In children, theequivalent bolus dose is 0-2-0-3 mg/kg. Acontinuous infusion of benzodiazepine hasalso been used, but there is now little placefor this mode of administration. The solutionshould be freshly prepared, and no drugsshould be admixed.The usual IV formulation is as an emulsion
(Diazemuls) in a 1 mL ampoule containing5mg/mL or as a solution in 2 mL ampoulescontaining 5 mg/mL. Stesolid is the usual rec-tal formulation, 2-5 mL rectal tube contain-ing 2 mg/mL 4 mg/mL. The IV solution canalso be instilled rectally.
Midazolam:Midazolam2427 has only recently been recent-ly introduced in status, and clinical experi-ence is limited. Unique amongst the drugs instatus, it can be given by intramuscular injec-tion, as well as by the rectal or intravenousroutes. Bioavailability after intramuscularinjection is about 80-100%, and peak levelsare reached after about 25 minutes althoughthere is marked individual variation. Its elimi-nation kinetics are dependent on hepaticblood flow. The lipid solubility of the drug,and hence its cerebral action, is reduced aspH falls. Action is short-lived, and there is astrong tendency to relapse following a singlebolus injection. It is cleared from the bodyfaster than diazepam, and there is thus lesstendency to accumulate. Midazolam exhibitsthe same toxic effects as other benzodi-azepines, including sedation, hypotensionand cardiorespiratory depression. Respiratoryarrest may occur occasionally even after intra-muscular injection so careful monitoring isimperative. Intramuscular use in premonitorystatus, where immediate facilities for intra-venous injection are often not available, is agreat advantage. This is the main current rolefor midazolam in status, but further experi-ence may widen its indications.
Midazolam is usually given intramuscularlyor rectally in premonitory status, at a dose of5-10 mg (in children 0 15-0-3 mg/kg), whichcan be repeated once after 15 minutes or so.A 5-10 mg intravenous bolus injection canalso be given (repeated to a maximum of0-3 mg/kg in adults), and there is limitedexperience of an intravenous infusion.Midazolam is available in 5 mL ampoulescontaining 2 mg/mL or 2 mL ampoules con-taining 5 mg/mL.
Paraldehyde:Paraldehyde2830 is a thoroughly old fashionedmedication, but is still widely used in thetreatment of status epilepticus. Its main indi-cation is as an alternative or sequel to theadministration of diazepam in the stage ofpremonitory or early status. It is especiallyuseful in situations where intravenous admin-istration is difficult, or where conventionalantiepileptic drugs are contra-indicated or
130 on M
arch 25, 2022 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.2.125 on 1 February 1993. D
ownloaded from

Tonic clonic status epilepticus
have proved ineffective. The drug is usuallygiven rectally (or less often intramuscularly),and absorption by both routes is fast andcomplete. The onset of action is rapid andparaldehyde is effective for many hours.Seizures tend to recur less after control isachieved than with the shorter acting benzo-diazepines, anaesthetic drugs or chlormethia-zole. Paraldehyde has no strong tendency toaccumulate, and the risks of hypotension orcardiorespiratory depression are low. Toxicityis unusual providing: the correct dose is notexceeded; the solution is freshly made; theparaldehyde is not decomposed; is dilutedsatisfactorily. Inappropriately diluted ordecomposed paraldehyde is highly toxic byany route of administration. The intramuscu-lar injection must be into deep (usuallygluteal) muscle, well away from the sciaticnerve. In established status, paraldehyde canbe given by intravenous infusion, but this is acomplicated and fraught procedure, and onewhich is now very rarely recommended. Thedrug also reacts with rubber and plastic, andso if infused, must be given via glass givingsets and syringes. An injection using a plasticsyringe, however, is acceptable if given rapid-ly after drawing the solution up.
In early status, paraldehyde can be given ata dose of 10-20 mL of 50% solution rectallyor intramuscularly (children 0-07-0 35 mLikg),which can be repeated once after 15-30 min-utes.
In established status in adults, it can begiven by continuous infusion, as a solution of15 mL ampoules in 500 mL of 5% dextrosefreshly made up every three hours, given at adose of 15-30 mL every three hours (that is,approximately 100-200 mg/kg/h). There isnow no place for the bolus injection of undi-luted paraldehyde even into a fast runningdrip. In neonatal status, an infusion of200 mg/kg/h can be given for at least threehours, or an initial infusion of 200 mg/kg/hfollowed by 16 mg/kg/h for 12 hours.
Paraldehyde is supplied in 1OmL ampoules(approximately 10 grams) in darkened glassto prevent decomposition. For rectal or intra-muscular administration, it is diluted in equalmeasure with 0-9% sodium chloride (normalsaline) or arachis oil. For intravenous admin-istration, it should be given as a 5% infusionin 5% dextrose, freshly made up every threehours.
Chlormethiazole:Chlormethiazole3'-34 is widely used at thestage of established status, by continuousintravenous infusion. Distribution is veryrapid, and there is a large volume of distribu-tion. A single intravenous injection has a veryrapid effect, which is very short lived.Chlormethiazole is thus best given as a con-tinuous infusion, and the dose can be titratedaccording to effect on a moment to momentbasis, without inducing deep anaesthesia.This ability to titrate the dose is very useful,and unique amongst the drugs used in status.On longer-term therapy, however, as the drugconcentrations in peripheral lipid com-
partments approach saturation levels, thisproperty is lost. Sudden accumulation'maycause persistingly high blood levels, resultingin sudden cardiorespiratory collapse, cardiacarrhythmia, hypotension or deep sedation. Inview of this risk, prolonged use of the drugshould be avoided where possible. If a long-term infusion (> 12 hours) is judged neces-sary, it is wise to reduce the dose every fewhours to minimise accumulation. There is atendency for seizures to recur as chlormethia-zole is weaned, and longer-term oral supple-mentation is sometimes required. Onprolonged therapy there is a danger of fluidoverload, and electrolyte supplementationmay be required as the infusion fluid is elec-trolyte-deficient. The elimination of chlorme-thiazole is markedly affected by changes inhepatic blood flow and by hepatic disease.The drug is absorbed by PVC on prolongedcontact. Although its pharmacokinetics arewell studied, there have been no formal clini-cal trials of chlormethiazole in status, andpublished experience of its use, especially inthe long-term and in children or the newbornis very limited.
In status, an initial intravenous infusion of40-100 mL of the 0-8% solution is given(that is, 320-800 mg) at a rate of5-15 mL/minute. The infusion is continuedat a minimum dose which will controlseizures (commonly 0-5-4 mL/minute, maxi-mum 20 mL/minute in adults). Whenseizures are controlled (for 12 hours in a caseof adult status), the rate of infusion should beslowly reduced. It is not uncommon forseizures to recur on chlormethiazole with-drawal, in which case the minimum effectivedose should again be determined and contin-ued. Sometimes, switching from the intra-venous to oral form (1-3 capsules of 192 mgchlormethiazole base a day, or 1-3 500 mgtablets of chlormethiazole edisylate, or5-15 mL of chlormethiazole edisylate syrup)is necessary as status resolves. An infusionrate of 0-01 mlikg/minute (0-08 mg/kg/minute)in children has been recommended, increas-ing every 2-4 hours until seizures are abol-ished or drowsiness intervenes. The drug isusually supplied in 500 mL bottles of a 0-8%solution of chlormethiazole edisylate(8 mg/mL) in dextrose and sodium hydrox-ide.
Lorazepam:Lorazepam2" 35-39 is indicated in the early stageof status only, where its lack of accumulationin lipid stores, its strong cerebral binding andlong duration of action are very significantadvantages over diazepam. The pharmacolo-gy and clinical effects of lorazepam have beenwell characterised in adults, in children andin the newborn, and the drug has been thesubject of large scale clinical trials.Lorazepam is remarkably effective in control-ling seizures in the early stage of status. Itsmain disadvantage is the rapid developmentof tolerance. Initial injections of lorazepamare effective for about 12 hours (longer thanwith diazepam), but repeated doses are much
131 on M
arch 25, 2022 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.2.125 on 1 February 1993. D
ownloaded from

Shorvon
less effective, and the drug has no place aslong-term therapy. Lorazepam has sedativeeffects shared by all the benzodiazepine drugsused in status, but sudden hypotension orrespiratory collapse are less likely because ofits relative lipid-insolubility and the lack ofaccumulation after single bolus injections.
Lorazepam is administered by intravenousbolus injection. As distribution is slow, therate of injection is not critical. In adults, abolus dose of 0-07 mg/kg (to a maximum of4 mg) is given, and this can be repeated onceafter 20 minutes if no effect has beenobserved. In children under 10 years, bolusdoses of 01 mg/kg are recommended. Long-term infusion of lorazepam should not beused. It is usually available as a 1 mLampoule containing 4 mg of lorazepam.
Phenytoin:Phenytoin40'4 is a drug of first choice inestablished status. Its pharmacology and clin-ical effects are well documented, and there isextensive experience in status in adults, chil-dren and the newborn. It is a highly effectiveanticonvulsant, with the particular advantageof a long duration of action. It can also becontinued as chronic therapy. Phenytoincauses relatively little respiratory or cerebraldepression, although hypotension is morecommon. The initial infusion of phenytointakes 20-30 minutes in an adult, and theonset of action is slow. It is therefore oftenadministered in conjunction with a short-act-ing drug with a rapid onset of action such asdiazepam. The notorious saturable pharma-cokinetics of phenytoin cause less problems inthe emergency setting than in chronic thera-py, but careful serum level monitoring isessential. The usual phenytoin solutions havea pH of 12, and if added to bags containinglarge volumes of fluid at lower than physio-logical pH (for example, 5% glucose) precipi-tation may occur in the bag or tubing; use ina solution of 0'9% sodium chloride (normalsaline) (5-20 mg/mL) is safer. There is alsoa serious risk of precipitation if other drugsare added to the infusion solution.Administration via a side arm, or- directlyusing an infusion pump is preferable.Phenytoin should not be given by either rectalor intramuscular injection. ECG monitoringis advisable whilst administering phenytoin.The rate of infusion of phenytoin solution
should not exceed 50 mg/minute, and it isprudent to reduce this to 20-30 mg/minute inthe elderly. The adult dose is 15-18 mg/Kg;usually about 1000 mg, therefore taking atleast 20 minutes to administer. Regrettably, alower dose is too often given, which results insuboptimal cerebral levels. This is a commonand potentially serious mistake. Phenytointherapy can be continued after intravenousloading by oral or further intravenous dailydosages of 5-6 mg/kg individual doses, guid-ed by blood level measurements. For olderchildren, the dose of phenytoin is as foradults. For the newborn a dose of15-20 mg/kg, injected at a rate not exceeding1 mg/kg/minute, should be given. Phenytoin
is usually available as 5 mL ampoules con-taining phenytoin sodium 250 mg.
Phenobarbitone:Phenobarbitone43-46 is a drug of choice for thetreatment of established status. It is highlyeffective, has a rapid onset of action and pro-longed anticonvulsant effects. It has stableand non-reactive physical properties, andconvenient pharmacokinetics. Wide experi-ence has been gained of its use in adults andin children, and few drugs are as well tried inthe newborn. It has stronger anticonvulsantproperties than most other barbiturates, andmay be preferentially concentrated in meta-bolically active epileptic foci. As well as excel-lent anticonvulsant properties, it may alsohave cerebral-protective action. Acute toler-ance to the antiepileptic effect is unusual, incontrast to the benzodiazepines, and oncecontrolled, seizures do not tend to recur. Themain disadvantages of phenobarbitone are itspotential to cause sedation, respiratorydepression and hypotension; although inpractice these effects seem slight except athigh levels or with rapidly rising levels, and itssafety at even high doses is well established.The well-known chronic side-effects of phe-nobarbitone in long-term therapy are of norelevance in the emergency situation of sta-tus. The drug is eliminated slowly, and whilstthis is of no importance on initial phenobarbi-tone loading, on prolonged therapy there is adanger of accumulation, and blood levelmonitoring is essential. In the newborn peri-od dosing is more difficult than in adults, asthe pharmacokinetics change rapidly duringthe first weeks and months of life. The drughas a strong tendency to auto-induction.Phenobarbitone is a stable preparation whichdoes not easily decompose, nor is the drugabsorbed by plastic. It should not be used ina solution containing other drugs (for exam-ple, phenytoin), as this may result in precipi-tation.The usual recommended adult intravenous
loading dose is 10 mg/Kg, given at a rate of100 mg/minute (that is, a total of about600 mg in six, minutes). This should be fol-lowed by daily maintenance doses of1-4 mg/kg. The initial maximum adult doseshould not exceed 1000 mg as the drug is notvery lipid soluble and in obese patients, themg/kg guide may be unreliable. In neonates,initial phenobarbitone loading doses ofbetween 12-20 mg/kg have been recommend-ed to produce therapeutic levels, with subse-quent supplementation of 3-4 mg/kg per day,to a maximum dose of 40 mg/kg. In olderchildren, loading dose of between 5-20 mg/kgare recommended and maintenance doses of1-4 mg/kg, although much higher doses havebeen safely given. After loading, maintenancedoses can be given by the oral, intravenous orintramuscular route. Phenobarbitone is usual-ly presented in 1 mL ampoules containing200 mg of phenobarbitone sodium.Thiopentone:Thiopentone47-50 is the compound traditional-ly used for barbiturate anaesthesia in status
132 on M
arch 25, 2022 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.2.125 on 1 February 1993. D
ownloaded from

Tonic clonic status epilepticus
epilepticus, at least in Europe. It is an effec-tive antiepileptic drug, and may have addi-tional cerebral-protective effects. In the dosesused in status it has anaesthetic action, andall patients require intubation and most artifi-cial ventilation. The most troublesome side-effect is persisting hypotension and manypatients require pressor therapy. Thiopentonehas saturable pharmacokinetics, and a strongtendency to accumulate. Thus if large dosesare given, blood levels may remain very highfor protracted periods, and days may passbefore consciousness is recovered after drugadministration is discontinued. Blood levelmonitoring, both of the thiopentone and itsactive metabolite pentobarbitone, is thereforeessential on prolonged therapy. Other toxiceffects on prolonged therapy include pancre-atitis and hepatic disturbance, and thiopen-tone may cause acute hypersensitivity. Itshould be administered cautiously in theelderly, and in those with cardiac, hepatic orrenal disease. Although it has been in usesince the 1960s in status, formal clinical trialsof its safety and effectiveness in either adultsand children are few. A full range of ITUfacilities are required during thiopentoneinfusions. Central venous pressure should bemonitored, and blood pressure via an arterialline. Swan-Ganz monitoring is sometimesadvisable, and EEG or cerebral functionmonitoring is essential if thiopentone infu-sions are prolonged. A concomitantdopamine infusion is frequently needed tomaintain blood pressure. Thiopentone canreact with polyvinyl infusion bags or givingsets. The continuous infusion should bemade up in 09% sodium chloride (normalsaline). The intravenous solution has a pH of10-2-11-2, is incompatible with a large num-ber of acidic or oxidising substances, and nodrugs should be added. The aqueous solutionis unstable if exposed to air.The dose regime commonly used is as fol-
lows: thiopentone is given as a 100-250 mgbolus over 20 seconds, with further 50 mgboluses every 2-3 minutes until seizures arecontrolled, with intubation and artificial ven-tilation. The intravenous infusion is then con-tinued at the minimum dose required tocontrol seizure activity (burst suppression onthe EEG), usually between 3-5 mg/kg/hour,and at thiopentone blood levels of about40 mg/L. After 24 hours, the dose should becontrolled by blood level monitoring. After2-3 days or so, metabolism may be near satu-ration, and daily or twice daily blood levelestimations should be made to ensure thatlevels do not rise excessively. The doseshould be lowered if systolic blood pressurefalls below 90 mm Hg, or if vital functions areimpaired. Thiopentone should be continuedfor no less than 12 hours after seizure activityhas ceased, and then slowly discontinued.The usual preparation is as a 2-5 g vial with100 mL of diluent to produce a 2-5% solu-tion.
Propofol:In recent times, there has been a vogue for
the use of non-barbiturate anaesthesia in sta-tus; of the currently available compounds,propofol51-54 is probably the drug of choice.Published experience, however, is very limit-ed of its use in status, or indeed of its long-term administration in any clinical situation.Propofol is a highly effective and nontoxicanaesthetic. Although, in experimental mod-els, it has intrinsic anticonvulsant properties,it has caused seizures in anaesthetic practice.Propofol is extremely soluble in lipid, and hasa high volume of distribution. It thus actsextremely rapidly in status. Its effects aremaintained whilst the infusion is continued,and recovery following discontinuation of thedrug is also very quick; in marked contrast tothiopentone. Theoretically, there is a dangerof accumulation on very long-term therapy,but this has been reported in practice.Propofol administration causes profound res-piratory and cerebral depression, requiringthe use of assisted respiration, the fullpanoply of intensive care and monitoring, butonly mild hypotension, and has few cardio-vascular side effects. Long term administra-tion causes marked lipaemia and may resultin acidosis. It may cause involuntary move-ments which should not be mistaken forseizures. Although propofol has been the sub-ject of only a few case reports, it is widelyused in status, and warrants further formalstudy. Its safety in young children has notbeen established.
In status, the following regime can be used:initially a 2 mg/kg bolus dose is given, whichcan be repeated if seizures continue, succeed-ed by an infusion of 5-10 mg/kg/hour guidedby EEG. The dose should be graduallyreduced, and the infusion tapered 12 hoursafter seizure activity is halted. In the elderly,doses should be lower. It is available as20 mL ampoules containing 10 mg/mL, as anemulsion.
Other drugs:A wide variety of other drugs have been usedin status, including clonazepam, lignocaine,pentobarbitone, etomidate, magnesium sul-phate, clorazepate, corticosteroids, valproate,lamotrigine. Few of these (or indeed the first-line) drugs have received adequate formalclinical study in status, and their relative mer-its are largely uncertain. An exciting area offuture research is the use of cerebro-protec-tive agents, to prevent status-induced cerebraldamage. A more detailed discussion of the
Table 6 Common reasons for the failure ofemergencydrug therapy to control seizures in status epilepticus
Inadequate emergency antiepileptic drug therapy (especiallythe administration of drugs at too low a dose)
Failure to initiate maintenance antiepileptic drug therapy(seizures will recur as the effect of emergency drugtreatment wears off)
Hypoxia, hypotension, cardiorespiratory failure, metabolicdisturbance
Failure to identify the underlying causeFailure to identify other medical complications (including
hyperthermia, disseminated intravascular coagulation,hepatic failure)
Misdiagnosis (pseudostatus is more common than epilepticstatus at least in specialist neurological practice)
133 on M
arch 25, 2022 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.2.125 on 1 February 1993. D
ownloaded from

Shorvon
drugs used in status can be found in largerreviews.2 1655
Failure of antiepileptic treatmentThe antiepileptic drugs used in status are
highly effective. If seizures continue despiteemergency therapy, it is important to reassessthe clinical circumstances, as there are oftencomplicating remediable factors influencingthe response to treatment. The most commonof these are listed in table 6.
1 Hauser WA. Status epilepticus: epidemiological consider-ations Neurology 1990;40(suppl 2):9-12.
2 Shorvon SD. Status epilepticus: its clinicalfeatures and treat-ment in children and adults. Cambridge: CambridgeUniversity Press, 1993.
3 Aicardi J, Chevrie Jj. Convulsive status epilepticus ininfants and children. A study of 239 cases. Epilepsia1970;11:187-97.
4 Goulon M, Levy-Alcover MA, Nouailhat F. Etat de malepileptique de l'adulte. Etude epidemiologique et clin-ique en reanimation. Rev EEG Neurophysiol 1985;14:277-85
5 Pilke A, Partinen M, Kovanen J. Status epilepticus andalcohol abuse: an analysis of 82 status epilepticusadmissions. Acta Neurol Scand 1984;70:443-50.
6 Aicardi J, Chevrie Jj. Consequences of status epilepticusin infants and children. In: Delgado-Escueta AV,Wasterlain CG, Treiman DM, Porter RJ, eds. Statusepilepticus: mechanisms of brain damage and treatment.Advances in Neurology, Vol 34. New York: Raven Press,1983:115-125.
7 Bourneville DM. Recherches cliniques et therapeutiquessur l'epilepsie et l'hysterie. Progres Medical. Paris:Delahaye, 1876.
8 Roger J, Lob H, Tassinari C. Status epilepticus. In:Vinken PJ, Bruyn GW, eds. Handbook of clinical neurolo-gy, Vol 15. New York: Elsevier, 1974:145-188.
9 Treiman DM, Walton NY, Kendrick C. A progressivesequence of electroencephalographic changes duringgeneralised convulsive status epilepticus EpilepsyResearch 1990;5:49-60.
10 Lothman E. The biochemical basis and pathophysiologyof status epilepticus. Neurology 1990;40(suppl 2): 13-22.
11 Simon RP. Physiological consequences of status epilepti-cus. Epilepsia 1985;26(Suppl 1):S58-66.
12 Brown JK, Hussain IHMI. Status epilepticus: 1: Patho-genesis. Develop Med Child Neurol 199 1;33:3-17
13 Aminoff MJ, Simon RP. Status epilepticus: causes, clini-cal features and consequences in 98 patients. Am ofMed 1980;69:657-66.
14 Meldrum BS. Metabolic factors during prolonged seizuresand their relation to cell death. In: Delgado EscuetaAV, Wasterlain CG, Treiman DM, Porter RJ, eds.Status epilepticus: mechanisms of brain damage and treat-ment. Advances in neurology, vol 34. New York: RavenPress, 1983:261-75.
15 Delgado-Escueta AV, Ward AA, Woodbury DM, PorterRJ, eds. Basic mechanisms of the epilepsies; molecular andcellular approaches. Advances in neurology, vol 44. NewYork: Raven Press, 1986
16 Delgado-Escueta AV, Wasterlain CG, Treiman DM,Porter RJ, eds. Status epilepticus: mechanisms of braindamage and treatment. Advances in neurology, vol 34.New York: Raven Press, 1983.
17 Benowitz NL, Simon RP, Copeland JR. Status epilepti-cus: divergence of sympatlhetic activity and cardiovas-cular response. Ann Neurol 1986;19:197-199.
18 Young RSK, Fripp RR, Yagel SK, Werner JC, McGrathG, Schuler HG. Cardiac dysfunction during statusepilepticus in the neonatal pig. Ann Neurol1985;18:291-7.
19 Schmidt D. Diazepam. In: Levy R, Dreifuss FE, MattsonR, Meldrum B, Penry JK, eds. Antiepileptic drugs, 3rded. New York: Raven Press, 1989:735-64.
20 Schmidt D. Benzodiazepines- an update In: Pedley TAand Meldrum BS, eds. Recent advances in epilepsy, vol 2.Edinburgh: Churchill Livingstone, 1985:125-135.
21 Delgado-Escueta AV, Enrile-Bacsal F. Combination ther-apy for status epilepticus: intravenous diazepam andphenytoin. In: Delgado Escueta AV, Wasterlain CG,Treiman DM, Porter RJ, eds Status epilepticus: mecha-nisms of brain damage and treatment. Advances in neurolo-gy, vol 34. New York, Raven Press 1983:477-85.
22 Remy C, Jourdil N, Villemain D, Favel P, Genton P.Intrarectal diazepam in epileptic adults. Epilepsia
1992;33:353-8.23 Leppik IE, Derivan AT, Homan RW, Walker J, Ramsay
RE, Patrick B. Double-blind study of lorazepam anddiazepam in status epilepticus. I Am Med Assoc
1983;249: 1452-4.24 Dundee JW, Halliday NJ, Harper KW, Brogden RN.
Midazolam: a review of its pharmacological propertiesand therapeutic uses. Drugs 1984;28:519-43.
25 Galvin GM, Jelinek GA. Midazolam: an effective intra-venous agent for seizure control. Archives of EmergencyMedicine 1987;4:169-172.
26 Ghilain S, Van Rijckevorsel-Harmant K, de Barsy TH.Midazolam in the treatment of epileptic seizures. JI ofNeurol, Neurosurg Psychiatry 1988;51:732.
27 Jawad S, Oxley J, Wilson J, Richens A. A pharmacody-namic evaluation of midazolam as an antiepileptic com-pound. J Neurol, Neurosurg Psychiatry 1986;49: 1050-4.
28 Koren G, Butt W, Rajchgot P, Mayer J, Whyte H, PapeK, MacLeod SM. Intravenous paraldehyde for seizurecontrol in newborn infants. Neurology 1986;36:108-1 11.
29 Browne TR. Paraldehyde, Chlormethiazole, andLidocaine for treatment of status epilepticus. In:Delgado Escueta AV, Wasterlain CG, Treiman DM,Porter RJ, eds. Status epilepticus: mechanisms of braindamage and treatment. Advances in neurology, vol 34.New York: Raven Press, 1983:509-17.
30 Lockman LA. Paraldehyde. In: Levy RH, Dreifuss FE,Mattson RH, Meldrum BS, Penry JK, eds. AntiepilepticDrugs, 3rd ed. New York: Raven Press, 1989:881-6.
31 Harvey PKP, Higenbottam TW, Loh L. Chlormethiazolein treatment of status epilepticus BMJ 1975;2:603-5.
32 Miller P, Kovar I. Chlormethiazole in the treatment ofneonatal status epilepticus. Postgrad Med Y 1983;59:801-2.
33 Lingam S, Bertwistle H, Elliston H, Wilson J. Problemswith intravenous chlormethiazole (Heminevrin) in sta-tus epilepticus BMJ 1980;i: 155-6.
34 Laxenaire M, Tridon P, Poire P. Effect of chlormethiazolein treatment of delirium tremens and status epilepticus.Acta Psychiatrica Scand 1966;42(Suppl 192):87-102.
35 Crawford TO, Mitchell WG, Snodgrass SR. Lorazepamin childhood status epilepticus and serial seizures: effec-tiveness and tachyphylaxis. Neurology 1987;37:190-5.
36 Sorel L, Mechler L, Harmant J. Comparative trial ofintravenous lorazepam and clonazepam in status epilep-ticus. Clinical Therapeutics 1981;4:326-36.
37 Homan RW, Unwin DH. Benzodiazepines: lorazepam.In: Levy R, Dreifuss FE, Mattson R, Meldrum B, PenryJK, eds. Antiepileptic drugs, 3rd ed. New York: RavenPress, 1989:841-54.
38 Mitchell WG, Crawford TO. Lorazepam is the treatmentof choice for status epilepticus. J Epilepsy 1990;3:7-10.
39 Maytal J, Novak GP, King KC. Lorazepam in the treat-ment of refractory neonatal seizures. J Child Neurol1991;6:319-23.
40 Wallis W, Kutt H, McDowell F. IV diphenylhydantoin intreatment of acute repetitive seizures. Neurology 1968;18:513-25.
41 Leppik IE, Patrick BK, Cranford RE. Treatment of AcuteSeizures and Status Epilepticus with IntravenousPhenytoin. In: Delgado-Escueta AV, Wasterlain CG,Treiman DM, Porter RJ, eds. Status epilepticus: mecha-nisms of brain damage and treatment. Advances in neurolo-gy, vol 34. New York: Raven Press, 1983:447-52.
42 Cranford RE, Leppik IE, Patrick B, Anderson CB,Kostick B. Intravenous phenytoin: clinical and pharma-cokinetic aspects. Neurology 1978;28:874-80.
43 Shaner DM, McCurdy SA, Herring MO, Gabor AJ.Treatment of status epilepticus: a prospective compari-son of diazepam and phenytoin versus phenobarbitaland optional phenytoin. Neurology 1988;38:202-7.
44 Crawford TO, Mitchell WG, Fishman LS, Snodgrass R.Very-high-dose phenobarbital for refractory statusepilepticus in children. Neurology 1988;38:1035-40.
45 Gal P, Toback J, Boer HR, Erkan NV, Wells TJ. Efficacyof phenobarbital monotherapy in treatment of neonatalseizures-relationship to blood levels. Neurology1982;32: 1401-4.
46 Lockman LA, Kriel R, Zaske D, Thompson T, Vimig N.Phenobarbital dosage for control of neonatal seizures.Neurology 1979;29:1445-9.
47 Partinen M, Kovanen J, Nilsson E. Status epilepticustreated with barbiturate anaesthesia with continuousmonitoring of cerebral function. BMJr 1981;282:520-21.
48 Young EB, Blume WT, Bolton CF, Warren KG.Anesthetic barbiturates in refractory status epilepticusJournal Canadien des Sciences Neurologiques 1980;7:291-2.
49 Orlowski JP, Erenberg G, Lueders H, Cruse RP.Hypothermia and barbiturate coma for refractory statusepilepticus. Critical Care Medicine 1984;12:367-72.
50 Lowenstein DH, Aminoff MJ, Simon RJ. Barbiturateanesthesia in the treatment of status epilepticus: clinicalexperience of 14 patients. Neurology 1988;38:395-400.
51 MacKenzie SJ, Kapadia F, Grant IS. Propofol infusion forcontrol of status epilepticus. Anaesthesia 1990;45:1043-5.
52 De Maria G, Guarneri D, Pasolini MP, Antonini L. Statodi male versivo trattato con Propofol. Boll Lega It Epil1991;74:191-192.
53 Alia G, Natale E, Mattaliano A, Daniele 0. On two casesof status epilepticus treated with propofol. Epilepsia1991;32(suppl 1):77.
54 Wood PR, Browne GPR, Pugh S. Propofol infusion forthe treatment of status epilepticus. Lancet 1988;i:480-1.
55 Levy R, Dreifuss FE, Mattson R, Meldrum B, Penry JK,eds. Antiepileptic drugs, 3rd ed. New York: Raven Press,1989.
134 on M
arch 25, 2022 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.2.125 on 1 February 1993. D
ownloaded from