Embed Size (px)
Citation preview

If you experience connection problems 10 minutes prior to or during the session,please phone the HNE Telehealth Help Desk on 02 4985 5400 and select option 1.
4/05/2016
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie 1
Welcome toAllied Health Telehealth Virtual Education
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie
Tongue Tie – What is all the fuss?
Melissa Compton
Senior Speech Pathologist
Westmead Centre for Oral Health
Tongue TieWhat is all the Fuss?
Melissa Compton
Senior Speech Pathologist
Westmead Centre For Oral Health

If you experience connection problems 10 minutes prior to or during the session,please phone the HNE Telehealth Help Desk on 02 4985 5400 and select option 1.
4/05/2016
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie 2
What is a Tongue Tie? The facts
It is hereditary
It is a congenital anomaly
Impaired tongue mobility due to a congenital anomaly
It can cause deficits in breastfeeding, bottle feeding, chewing, cleaning teeth and in articulation (degree of deficits unknown)
Incidence still remains around 5% (Dr David Todd, Centenary Hospital Canberra) “Mother nature does not create catastrophic increases in incidence of congenital anomalies….” Hazelbaker, A
Evidence
NHMRC 2012 Infant Feeding Guidelines state:
There is limited evidence that “tongue tie "occurs in 4-10% of healthy newborn infants (Evidence Grade D). There is limited evidence (Evidence Grade D) to suggest that Infants with “tongue Tie” more commonly experience breastfeeding difficulties
Level D Evidence is very low quality, based on no research evidence.
NHMRC concludes that
While surgical management of tongue tie has been tried….further controlled trials are required
www.nhmrc.gov.au/guidelines-publication/n56
Page 52 Breastfeeding-Common Problems and their Management

If you experience connection problems 10 minutes prior to or during the session,please phone the HNE Telehealth Help Desk on 02 4985 5400 and select option 1.
4/05/2016
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie 3
Classification Systems
Hazelbaker:1993
Description of the tongue, attachments to the tongue and floor of mouth
Ballard:2002
Tip of tongue to alveolar ridge
Mid tongue-alveolar ridge
No mention of posterior TT
Coryllos:2004
Type 1, Type 2, Type 3, Type 4 (Base of tongue), alveolar ridge included
Griffiths/Hogan:2004/2005
100%: attached at tip, 75%:anterior tongue, 50%: mid tongue, 25%: Base of tongue (no mention of alveolar ridge)
Classification Cont….
Murphy 2010
Types 1 & 2 are “Anterior”; Types 3 & 4 are “Posterior”
Type 4 : no visible membrane above the mouth floor, all Submucosal
Type I Type II Type III
Type IV
Mahar, M, MD: WIC Annual ConferenceMarch 24. 105Photo Credit: James Murphy, MD
If you experience connection problems 10 minutes prior to or during the session,please phone the HNE Telehealth Help Desk on 02 4985 5400 and select option 1.
4/05/2016
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie 4
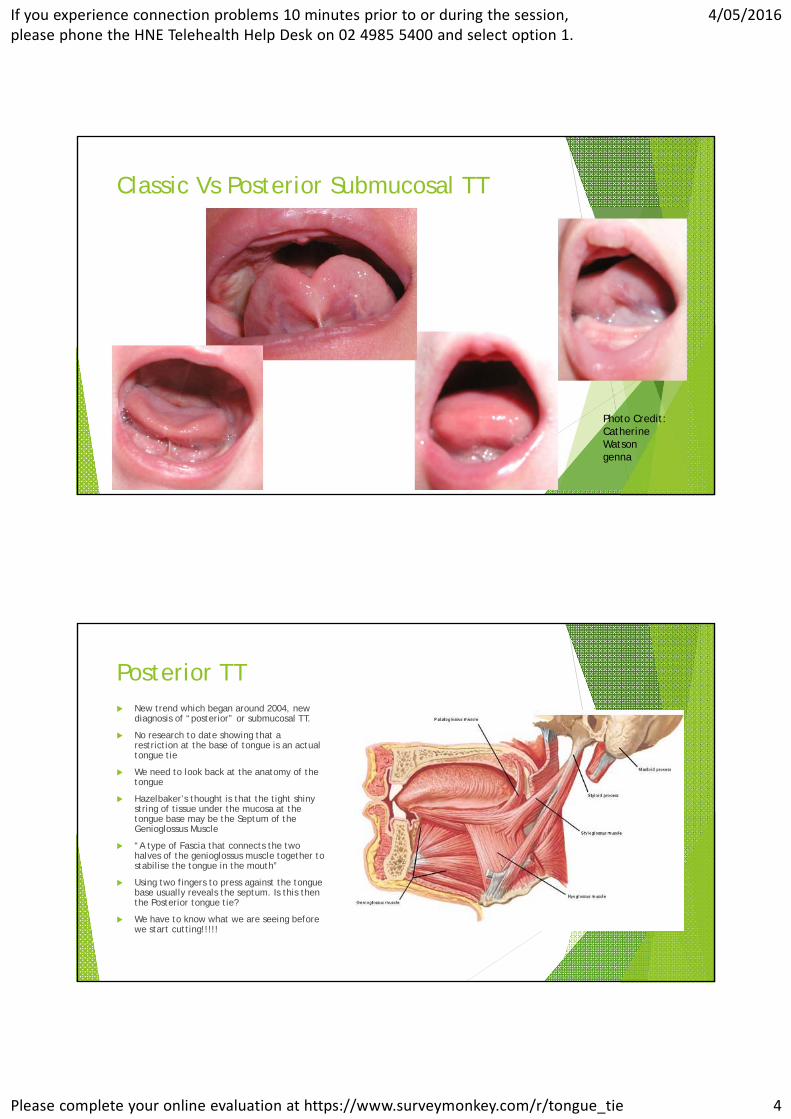
Classic Vs Posterior Submucosal TT
Photo Credit: Catherine Watson genna
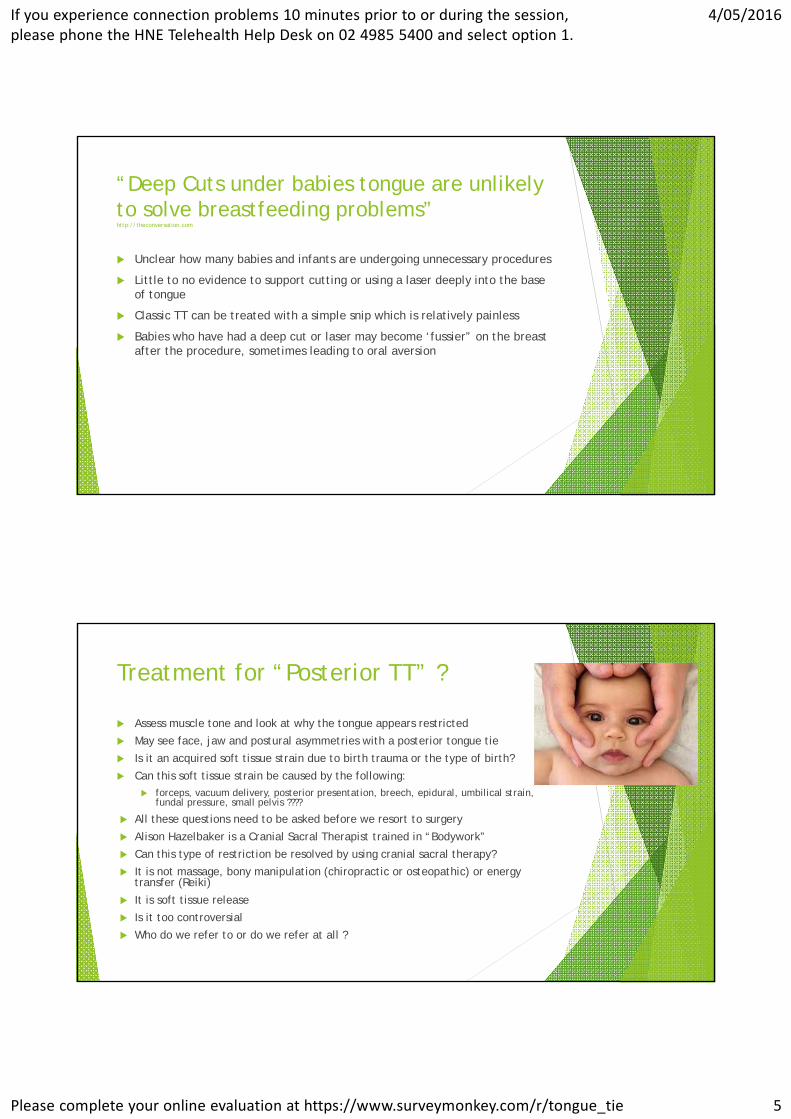
Posterior TT New trend which began around 2004, new
diagnosis of “posterior” or submucosal TT.
No research to date showing that a restriction at the base of tongue is an actual tongue tie
We need to look back at the anatomy of the tongue
Hazelbaker’s thought is that the tight shiny string of tissue under the mucosa at the tongue base may be the Septum of the Genioglossus Muscle
“A type of Fascia that connects the two halves of the genioglossus muscle together to stabilise the tongue in the mouth”
Using two fingers to press against the tongue base usually reveals the septum. Is this then the Posterior tongue tie?
We have to know what we are seeing before we start cutting!!!!!
If you experience connection problems 10 minutes prior to or during the session,please phone the HNE Telehealth Help Desk on 02 4985 5400 and select option 1.
4/05/2016
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie 5
“Deep Cuts under babies tongue are unlikely to solve breastfeeding problems”http://theconversation.com
Unclear how many babies and infants are undergoing unnecessary procedures
Little to no evidence to support cutting or using a laser deeply into the base of tongue
Classic TT can be treated with a simple snip which is relatively painless
Babies who have had a deep cut or laser may become ‘fussier” on the breast after the procedure, sometimes leading to oral aversion
Treatment for “Posterior TT” ?
Assess muscle tone and look at why the tongue appears restricted
May see face, jaw and postural asymmetries with a posterior tongue tie
Is it an acquired soft tissue strain due to birth trauma or the type of birth?
Can this soft tissue strain be caused by the following:
forceps, vacuum delivery, posterior presentation, breech, epidural, umbilical strain, fundal pressure, small pelvis ????
All these questions need to be asked before we resort to surgery
Alison Hazelbaker is a Cranial Sacral Therapist trained in “Bodywork”
Can this type of restriction be resolved by using cranial sacral therapy?
It is not massage, bony manipulation (chiropractic or osteopathic) or energy transfer (Reiki)
It is soft tissue release
Is it too controversial
Who do we refer to or do we refer at all ?
If you experience connection problems 10 minutes prior to or during the session,please phone the HNE Telehealth Help Desk on 02 4985 5400 and select option 1.
4/05/2016
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie 6
Speech Pathology AssessmentBabies and Children
Case history
Birth history
Family history of feeding/speech difficulties
Early feeding experiences
Transition to solids
Developmental milestones
Hearing and any middle ear problems
Allergies, nose problems, Snoring?
Commencement of speech, babbling, single words, intelligibility
Current feeding skills, foods eaten
Other Specialists involved eg ENT, Paediatrician
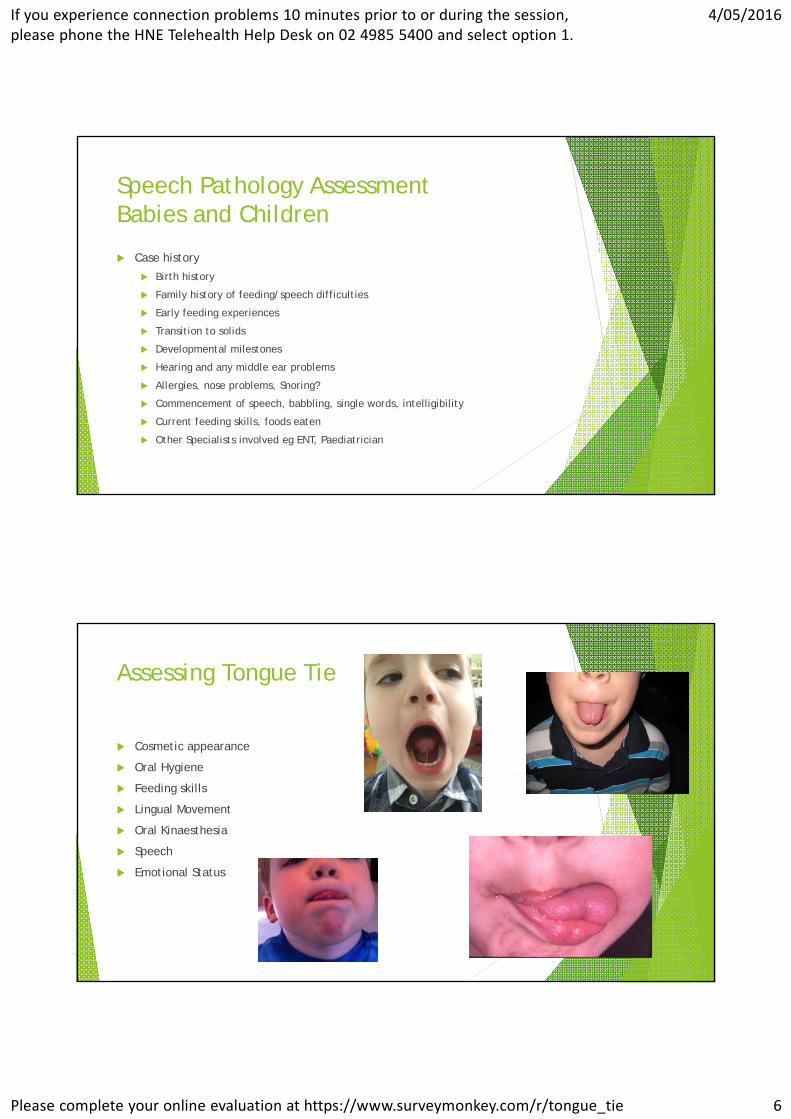
Assessing Tongue Tie
Cosmetic appearance
Oral Hygiene
Feeding skills
Lingual Movement
Oral Kinaesthesia
Speech
Emotional Status

If you experience connection problems 10 minutes prior to or during the session,please phone the HNE Telehealth Help Desk on 02 4985 5400 and select option 1.
4/05/2016
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie 7
Tongue Tie Confusion to Clarity-Carmen Fernando
Hazelbaker Assessment Tool for Babies <6moFunctional Items 0 1 2
Lateralisation None Body of tongue but not tongue tip
Complete
Lift of tongue Tip stays at alveolar ridge or rises to mid-mouth only with jawclosure
Only edges to mid-mouth
Tip to mid-mouth
Extension of tongue Neither above ORanterior or mid-tongue humps
Tip to lower gum only
Tip over lower lip
Spread of anterior tongue
Little or None Moderate or Partial Complete
Cupping Little or no cup Side edges only, moderate cup
Entire edge, firm cup
Peristalsis None or reverse peristalsis
Partial:originating posterior to tip
Complete,anterior to posterior (originates at the tip)
Snapback Frequent or with each suck
Periodic None
If you experience connection problems 10 minutes prior to or during the session,please phone the HNE Telehealth Help Desk on 02 4985 5400 and select option 1.
4/05/2016
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie 8
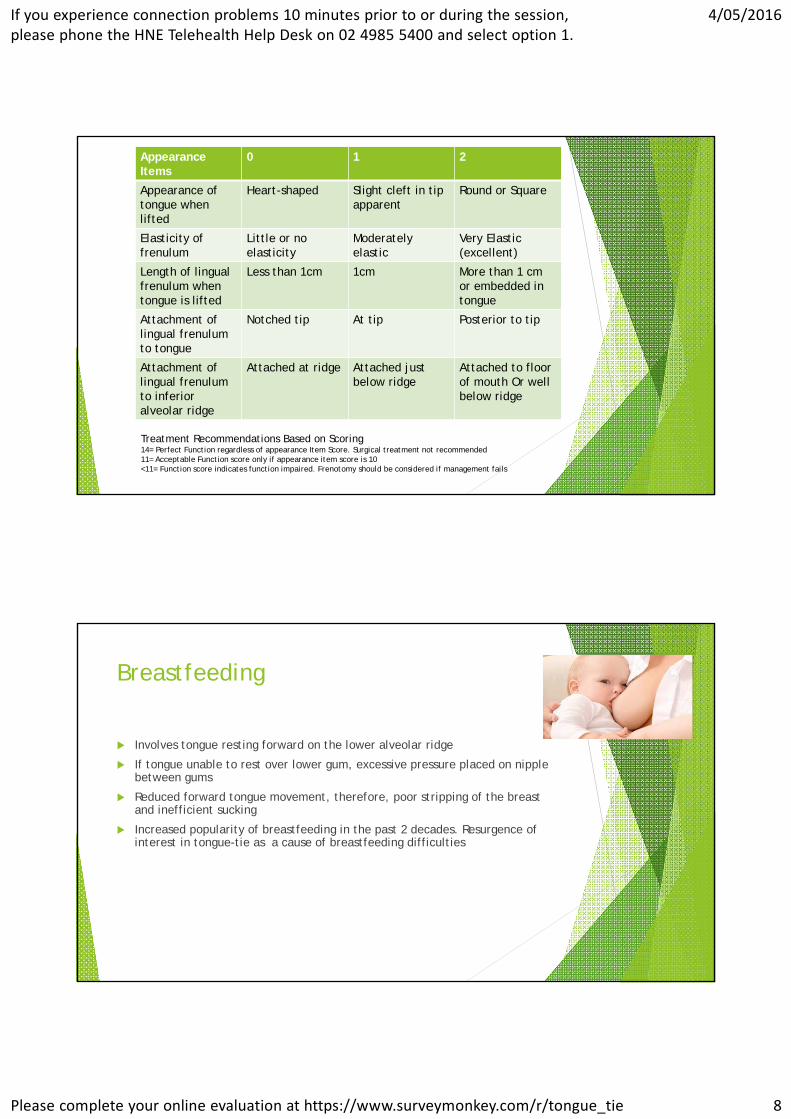
Appearance Items
0 1 2
Appearance of tongue when lifted
Heart-shaped Slight cleft in tip apparent
Round or Square
Elasticity of frenulum
Little or no elasticity
Moderately elastic
Very Elastic (excellent)
Length of lingual frenulum when tongue is lifted
Less than 1cm 1cm More than 1 cm or embedded in tongue
Attachment of lingual frenulum to tongue
Notched tip At tip Posterior to tip
Attachment of lingual frenulum to inferior alveolar ridge
Attached at ridge Attached just below ridge
Attached to floor of mouth Or well below ridge
Treatment Recommendations Based on Scoring14= Perfect Function regardless of appearance Item Score. Surgical treatment not recommended11= Acceptable Function score only if appearance item score is 10<11= Function score indicates function impaired. Frenotomy should be considered if management fails
Breastfeeding
Involves tongue resting forward on the lower alveolar ridge
If tongue unable to rest over lower gum, excessive pressure placed on nipple between gums
Reduced forward tongue movement, therefore, poor stripping of the breast and inefficient sucking
Increased popularity of breastfeeding in the past 2 decades. Resurgence of interest in tongue-tie as a cause of breastfeeding difficulties
If you experience connection problems 10 minutes prior to or during the session,please phone the HNE Telehealth Help Desk on 02 4985 5400 and select option 1.
4/05/2016
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie 9
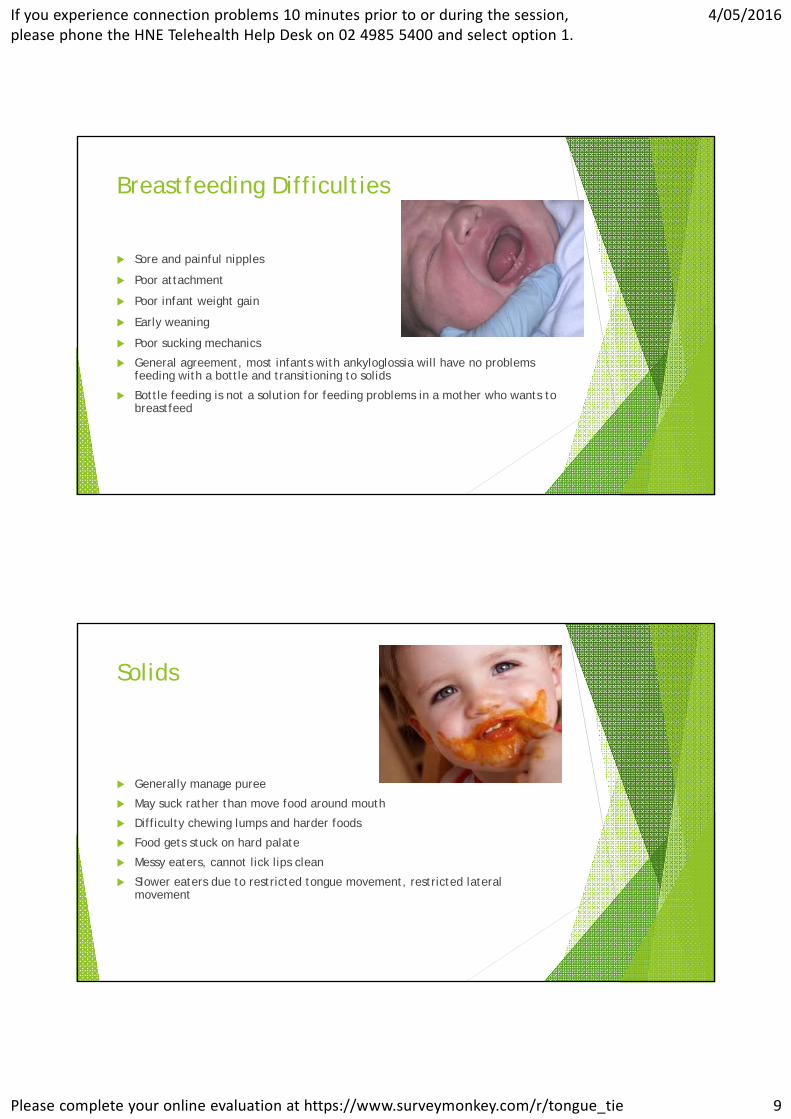
Breastfeeding Difficulties
Sore and painful nipples
Poor attachment
Poor infant weight gain
Early weaning
Poor sucking mechanics
General agreement, most infants with ankyloglossia will have no problems feeding with a bottle and transitioning to solids
Bottle feeding is not a solution for feeding problems in a mother who wants to breastfeed
Solids
Generally manage puree
May suck rather than move food around mouth
Difficulty chewing lumps and harder foods
Food gets stuck on hard palate
Messy eaters, cannot lick lips clean
Slower eaters due to restricted tongue movement, restricted lateral movement

If you experience connection problems 10 minutes prior to or during the session,please phone the HNE Telehealth Help Desk on 02 4985 5400 and select option 1.
4/05/2016
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie 10
Speech /Articulation
Effect of AG on speech is not clearly defined
It is NOT the cause of speech and language delay or learning difficulties
Some children develop normal speech and compensate for limited tongue tip mobility (ie keeping mouth closed)
AG may contribute to some articulation errors or difficulty with the rate and range of articulation, therefore reducing speech intelligibility ( eg. mumbling)
Speech sounds commonly affected are
‘t, d, n, l, s, z, th’
Some children compensate by changing the placement of the tongue (eg. interdental lisp)
Mechanical & Social Effects
Reduced range of movement
Food may be cleared from the buccal cavity with fingers
Difficulty with intra-oral toileting eg. licking lips, sweeping teeth free of food
Difficulty playing wind instruments
Difficulty licking an ice-cream in a cone
Difficulty with French kissing
If you experience connection problems 10 minutes prior to or during the session,please phone the HNE Telehealth Help Desk on 02 4985 5400 and select option 1.
4/05/2016
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie 11

If you experience connection problems 10 minutes prior to or during the session,please phone the HNE Telehealth Help Desk on 02 4985 5400 and select option 1.
4/05/2016
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie 12
Frenotomy Vs Frenectomy
Frenotomy More simple procedure that
removes the membrane or cutting the frenumlum
No anaesthetic used here at Westmead Hospital
Frenectomy Frenectomy is defined as complete
excision
This is a procedure where the entire frenulum is cut down to the tongue muscle or gum
Frenuloplasty“Various methods to release the tongue tie and correct the anatomical situation”
Snipping Vs Laser
Snipping
Can be done up to 4 months of age *ethical reasons
Use a blunt ended scissors and a retractor
Faster
Like a paper cut
Pain immediate but not persistent
Parents can be present
No after care, do not touch the wound under the tongue
Allow baby to breastfeed and sterilise everything that goes in the mouth
Laser Any age
Longer procedure
Parents are not allowed in the room due to guidelines
Delayed onset of pain (burn)
Lasers are expensive
Stretching exercises after lip and tongue-tie release help to reduce the risk of reattachment
Laser can be very dangerous when used by an untrained practitioner.
Different types of lasers
The wrong laser can damage collateral tissue and create excessive scar tissue
Currently no training for anyone who wants to start using lasers on babies.
If you experience connection problems 10 minutes prior to or during the session,please phone the HNE Telehealth Help Desk on 02 4985 5400 and select option 1.
4/05/2016
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie 13
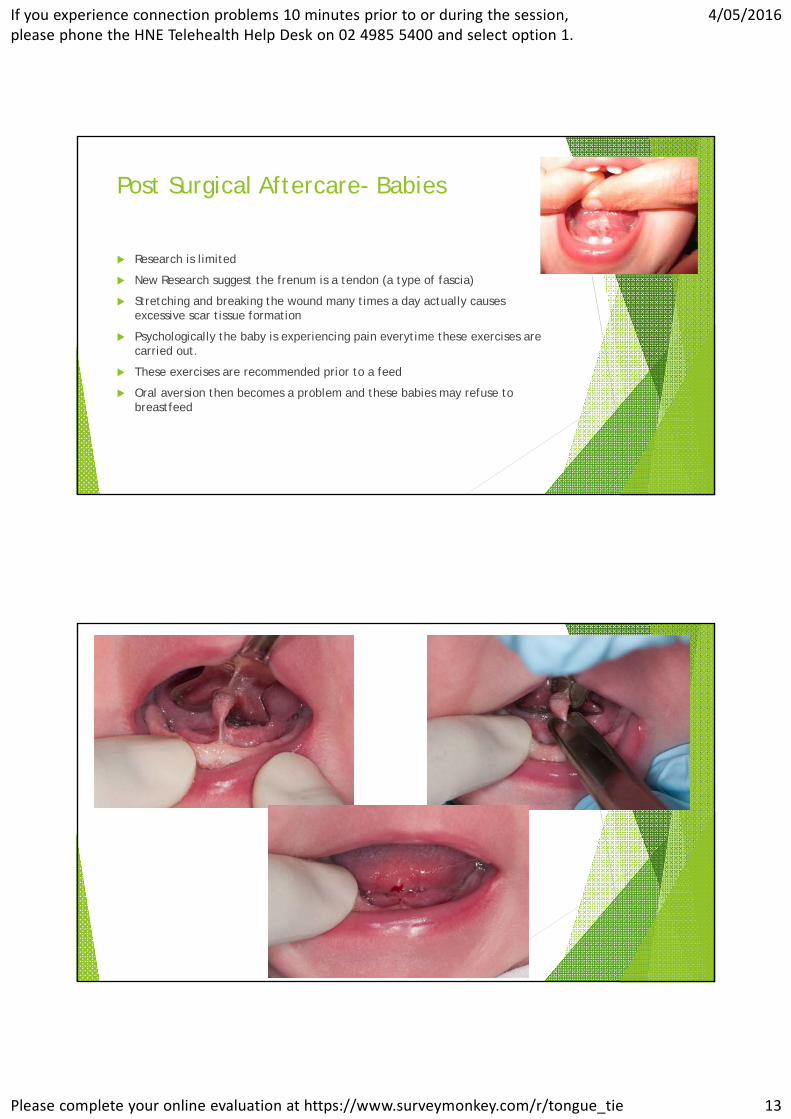
Post Surgical Aftercare- Babies
Research is limited
New Research suggest the frenum is a tendon (a type of fascia)
Stretching and breaking the wound many times a day actually causes excessive scar tissue formation
Psychologically the baby is experiencing pain everytime these exercises are carried out.
These exercises are recommended prior to a feed
Oral aversion then becomes a problem and these babies may refuse to breastfeed
If you experience connection problems 10 minutes prior to or during the session,please phone the HNE Telehealth Help Desk on 02 4985 5400 and select option 1.
4/05/2016
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie 14
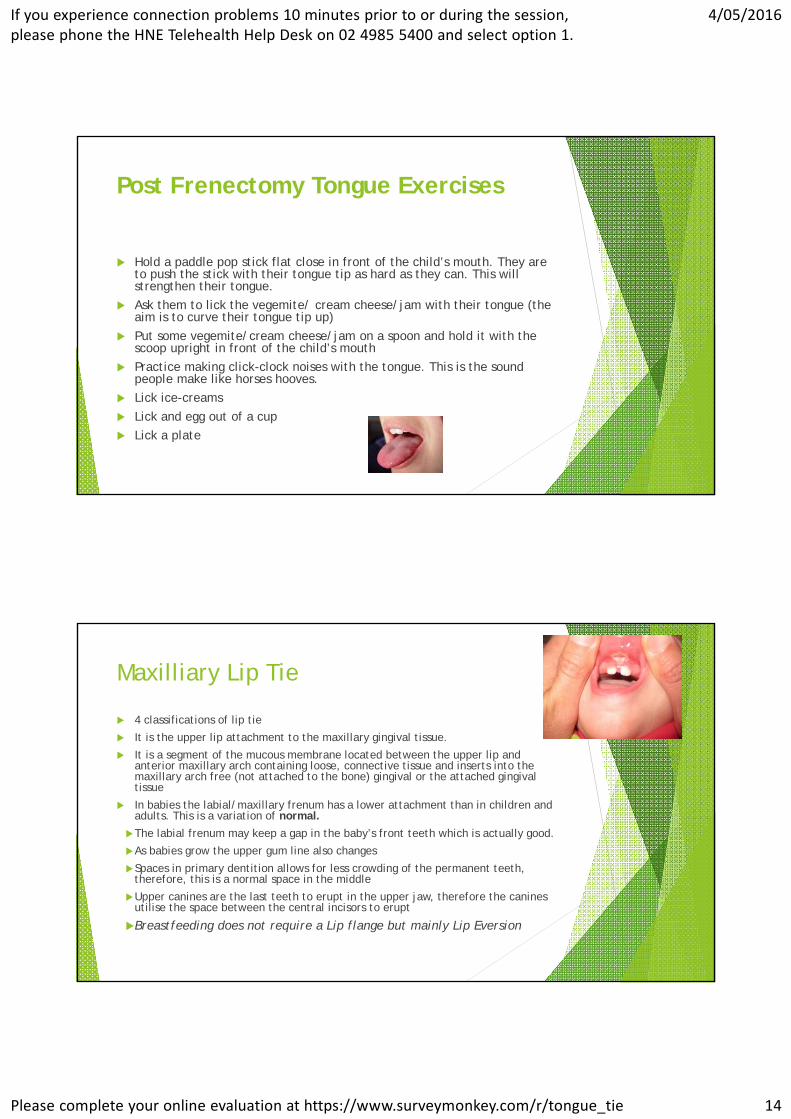
Post Frenectomy Tongue Exercises
Hold a paddle pop stick flat close in front of the child’s mouth. They are to push the stick with their tongue tip as hard as they can. This will strengthen their tongue.
Ask them to lick the vegemite/ cream cheese/jam with their tongue (the aim is to curve their tongue tip up)
Put some vegemite/cream cheese/jam on a spoon and hold it with the scoop upright in front of the child’s mouth
Practice making click-clock noises with the tongue. This is the sound people make like horses hooves.
Lick ice-creams
Lick and egg out of a cup
Lick a plate
Maxilliary Lip Tie
4 classifications of lip tie
It is the upper lip attachment to the maxillary gingival tissue.
It is a segment of the mucous membrane located between the upper lip and anterior maxillary arch containing loose, connective tissue and inserts into the maxillary arch free (not attached to the bone) gingival or the attached gingival tissue
In babies the labial/maxillary frenum has a lower attachment than in children and adults. This is a variation of normal.
The labial frenum may keep a gap in the baby’s front teeth which is actually good.
As babies grow the upper gum line also changes
Spaces in primary dentition allows for less crowding of the permanent teeth, therefore, this is a normal space in the middle
Upper canines are the last teeth to erupt in the upper jaw, therefore the canines utilise the space between the central incisors to erupt
Breastfeeding does not require a Lip flange but mainly Lip Eversion
If you experience connection problems 10 minutes prior to or during the session,please phone the HNE Telehealth Help Desk on 02 4985 5400 and select option 1.
4/05/2016
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie 15
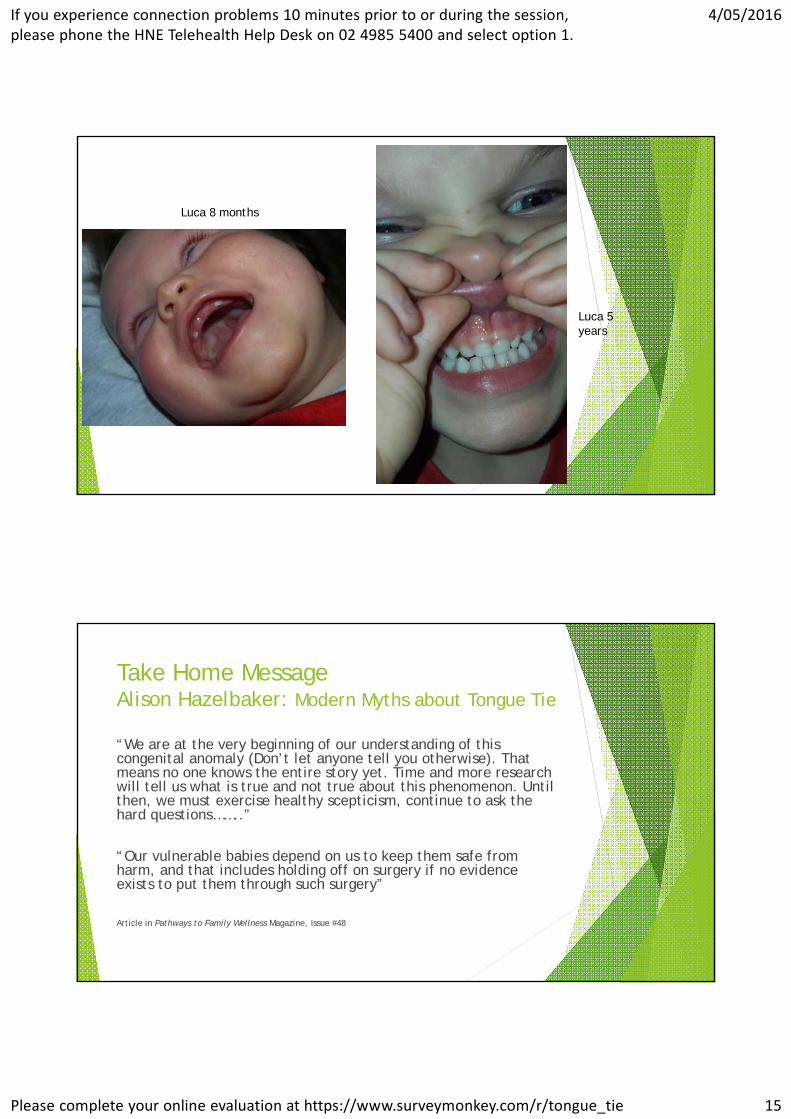
Luca 8 months
Luca 5 years
Take Home Message Alison Hazelbaker: Modern Myths about Tongue Tie
“We are at the very beginning of our understanding of this congenital anomaly (Don’t let anyone tell you otherwise). That means no one knows the entire story yet. Time and more research will tell us what is true and not true about this phenomenon. Until then, we must exercise healthy scepticism, continue to ask the hard questions……..”
“Our vulnerable babies depend on us to keep them safe from harm, and that includes holding off on surgery if no evidence exists to put them through such surgery”
Article in Pathways to Family Wellness Magazine, Issue #48

If you experience connection problems 10 minutes prior to or during the session,please phone the HNE Telehealth Help Desk on 02 4985 5400 and select option 1.
4/05/2016
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie 16
References
Breastfeeding-Common Problems and their Management : Infant Feeding Guidelines www.nhmrc.gov.au/guidelines-publications/n56
Deep Cuts Under babies tongues are unlikely to solve breastfeeding problems http:/theconversation.com/ 30/3/2016
Hazelbaker, A K (2010) Tongue Tie Morphogenesis, Impact, Assessment and Treatment
Fernando, C (1998) Tongue Tie from confusion to Clarity
O’Callahan,C., Macary, S., & Clemente, S (2013). The effects of office- based frenotomy for anterior and posterior ankyloglossia on breastfeeding. Int J Pediatr Otorhinolaryngol, 77 (5), 827-32
Suter, V. G. A., & Bornstein , M. M (2009). Ankyloglossia: Facts and Myths in Diagnosis and Treatment. J Of Periodondology, 80 (8), 1204-1219
Messner, A.H., Lalakea, L.K., Aby, J., Macmahon, J., Blair, E Ankyloglossia: Incidence & Associated Feeding Difficulties. Archives of Otolaryngology- Head & Neck Surgery 2000; 126,:32-39
Messner, A.H & Lalakea, M.L The Effect of Ankyloglossia on Speech in Children.Otolaryngology- Head & Neck Surgery 2002; 127: 539-545
Messner, A.H & Lalakea, M.L. Ankyloglossia: Controversies in Management.
International Journal of Pediatric Otorhinolaryngology 2000; 73: 881-883 Posterior Ankyloglossia A Case Report
References
Kotlow L. The Influence of the Maxillary Frenum on the Development and Pattern of Dental caries on Anterior Teeth in Breastfeeding Infants: Prevention, Diagnosis, and Treatment. J of Human Lactation. 2010 26:304-308
Prevalence and Variations of the median maxillary labial frenum in children, adolescents, and adults in a diverse population. Townsend, J A. Brannon, R B. Cheramie, T. Hagan,J March/April 2013
Kotlow L. Diagnosing and Understanding the maxillary Lip-tie (Superior Labial, the Maxillary Labial Frenum) as it Relates to Breastfeeding. J of Human Lactation. Published online 2 July 2013
Infant Reflux and Aerophagia Associated with the Maxillary Lip Tie and Ankyloglossia (Tongue-tie) Kotlow, L 2011
Ballard, J.L., Auer, C.E., Khoury, J.C (2003) Ankyloglossia: Assessment, Incidence, and Effectof Frenuloplasty on the Breastfeeding Dyad. Paediatrics 2003; 110: pp e63
Griffiths, D.M. Do Tongue-Ties Affect Breastfeeding? Journal of Human Lactation 2004; 20: 409-414
Hogan, M., Westcott, C., Griffiths, M A Randomised Control Trial of Division of Tongue-Tie in Infants with Feeding Problems Journal of Paediatrics and Child Health; 2005: in press
Lalakea, M.L & Messner, A.H Ankyloglossia: Does it matter? The Pediatric Clinics of North America 2003; 50: 381-397
Edmunds, J., Hazelbaker, A., Murphy, J. G., & Philipp, B.L. (2012) 28:14 Roundtable Discussion: Tongue Tie

If you experience connection problems 10 minutes prior to or during the session,please phone the HNE Telehealth Help Desk on 02 4985 5400 and select option 1.
4/05/2016
Please complete your online evaluation at https://www.surveymonkey.com/r/tongue_tie 17
Thank YouMelissa Compton
Senior Speech Pathologist
Westmead Hospital





























