Embed Size (px)
Citation preview
TomoTherapy®
System Treats
all
Breasts
Accuray
Satellite Symposium
6th May 2017
Roberto Orecchia
Chair of Radiation Therapy, University of Milan & Scientific Director at the European Institute of Oncology - IEO, Milan &
at the National Center of Oncological Hadrontherapy - CNAO, Pavia, Italy
Disclosure:
- An honorarium is provided by Accuray for this presentation- Accuray and European Institute of Oncology have a research
agreement in place
Disclaimer:
- The views expressed in this presentation are those of thepresenter and do not necessarily reflect the views or policies ofAccuray Incorporated or its subsidiaries. No official endorsementby Accuray Incorporated or any of its subsidiaries of any vendor,products or services contained in this presentation is intended orshould be inferred
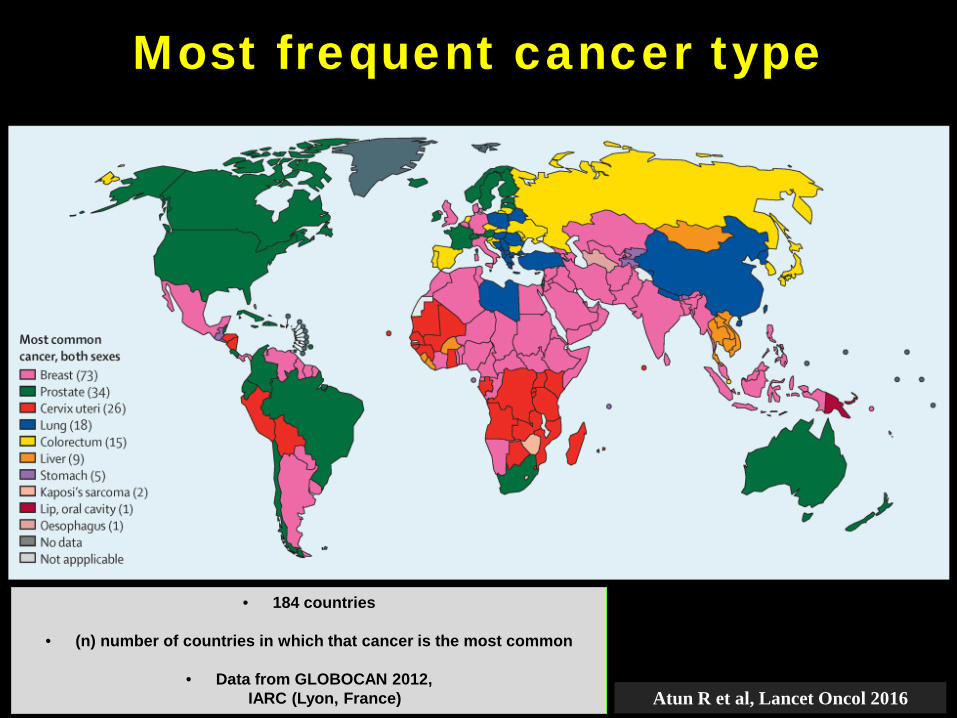
Most frequent cancer type
Atun R et al, Lancet Oncol 2016
• 184 countries
• (n) number of countries in which that cancer is the most common
• Data from GLOBOCAN 2012, IARC (Lyon, France)
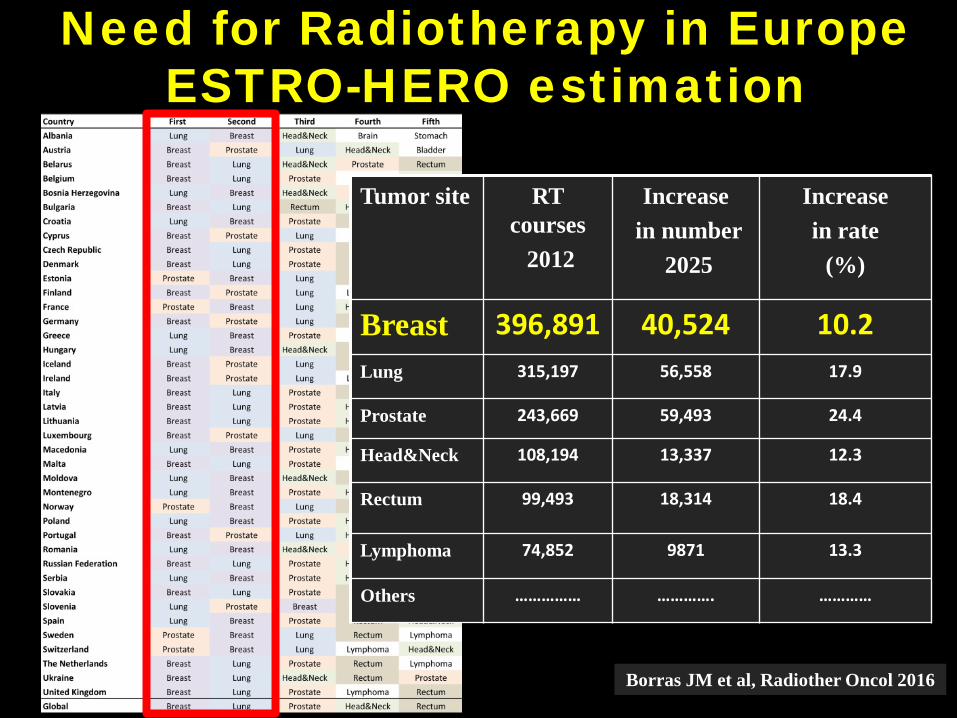
Need for Radiotherapy in Europe ESTRO-HERO estimation
Borras JM et al, Radiother Oncol 2016
Tumor site RT courses
2012
Increasein number
2025
Increasein rate
(%)
Breast 396,891 40,524 10.2Lung 315,197 56,558 17.9
Prostate 243,669 59,493 24.4
Head&Neck 108,194 13,337 12.3
Rectum 99,493 18,314 18.4
Lymphoma 74,852 9871 13.3
Others …………… …………. …………
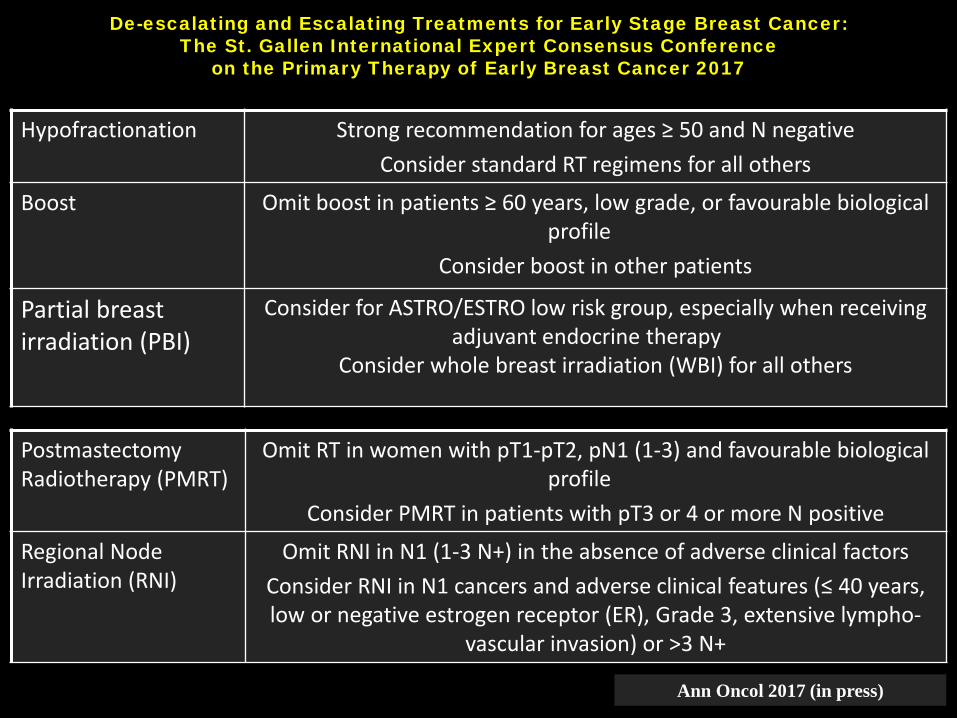
De-escalating and Escalating Treatments for Early Stage Breast Cancer: The St. Gallen International Expert Consensus Conference
on the Primary Therapy of Early Breast Cancer 2017
Hypofractionation Strong recommendation for ages ≥ 50 and N negativeConsider standard RT regimens for all others
Boost Omit boost in patients ≥ 60 years, low grade, or favourable biological profile
Consider boost in other patients
Partial breast irradiation (PBI)
Consider for ASTRO/ESTRO low risk group, especially when receiving adjuvant endocrine therapy
Consider whole breast irradiation (WBI) for all others
PostmastectomyRadiotherapy (PMRT)
Omit RT in women with pT1-pT2, pN1 (1-3) and favourable biological profile
Consider PMRT in patients with pT3 or 4 or more N positive
Regional NodeIrradiation (RNI)
Omit RNI in N1 (1-3 N+) in the absence of adverse clinical factors Consider RNI in N1 cancers and adverse clinical features (≤ 40 years, low or negative estrogen receptor (ER), Grade 3, extensive lympho-
vascular invasion) or >3 N+
Ann Oncol 2017 (in press)
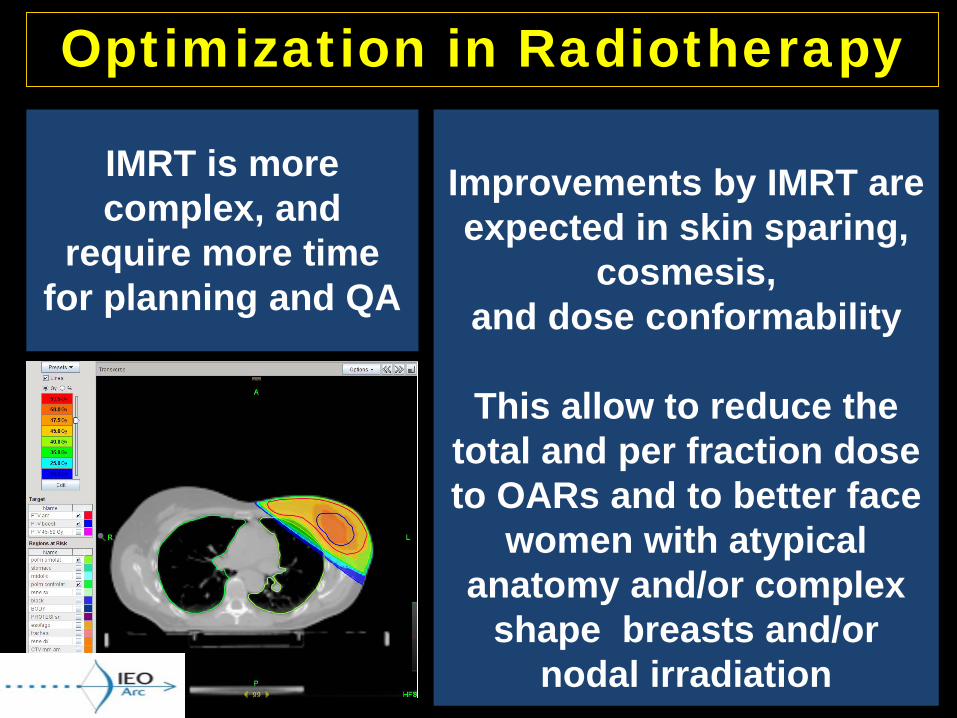
Optimization in Radiotherapy
IMRT is more complex, and
require more time for planning and QA
Improvements by IMRT are expected in skin sparing,
cosmesis, and dose conformability
This allow to reduce the total and per fraction dose to OARs and to better face
women with atypical anatomy and/or complex
shape breasts and/or nodal irradiation
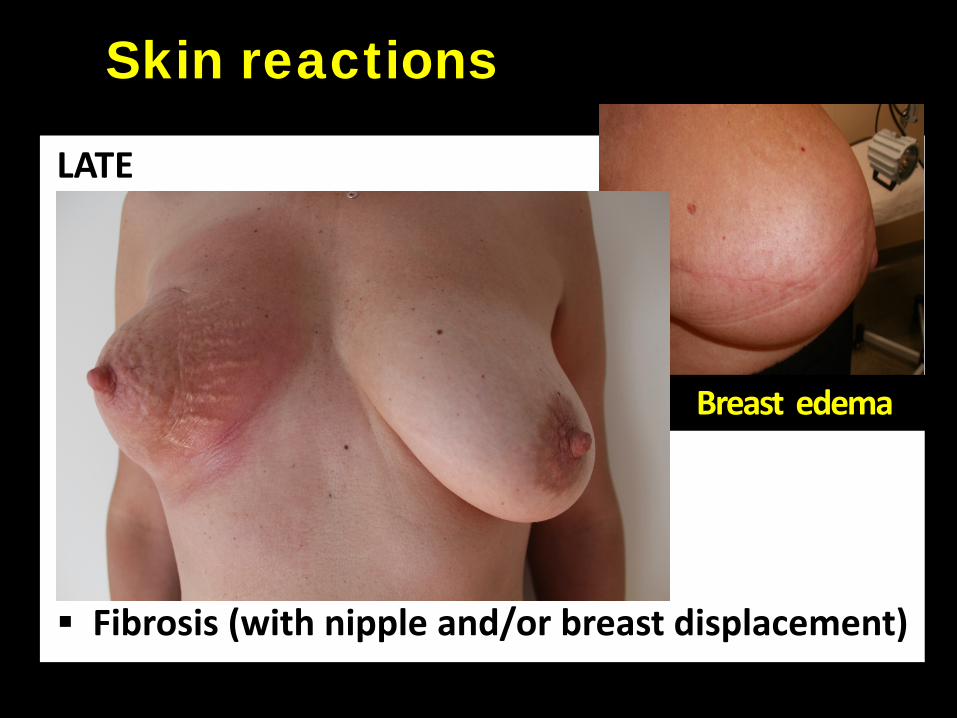
LATE
Edema Peeling Dystrophy or atrophy Hypo or hyper pigmentation Teleangectasia Skin thickening Fibrosis (with nipple and/or breast displacement)
Skin reactions
Breast edema
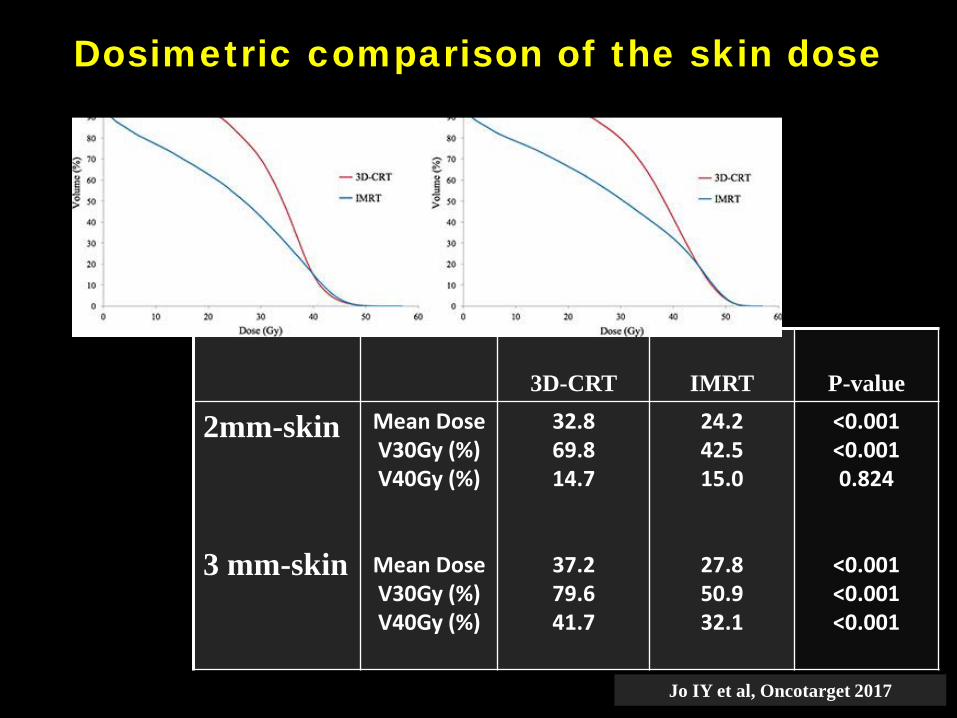
3D-CRT IMRT P-value
2mm-skin
3 mm-skin
Mean Dose V30Gy (%)V40Gy (%)
Mean DoseV30Gy (%)V40Gy (%)
32.869.814.7
37.279.641.7
24.242.515.0
27.850.932.1
<0.001<0.0010.824
<0.001<0.001<0.001
Dosimetric comparison of the skin dose
Jo IY et al, Oncotarget 2017
Breast IMRT using a static field-in-field method resulted in fewer changes in breast appearance at 5 years
Late toxicity
2D vs IMRT
Same results in:
1. Canadian Phase III study, with small breast size and FP FIF IMRT significantly associated with a decreased risk of moist
desquamation (Pignol JP et al, J Clin Oncol 2008)
2. Cambridge Phase III study, with benefits from FP FIF IMRT for all breast sizes, and reduced skin teleangectasia and improved overall
cosmesis (Barnett GC et al, Radiother Oncol 2009)
Randomised trial of standard 2D radiotherapy (RT) versus intensity modulated radiotherapy (IMRT) in patients prescribed breast radiotherapy.Donovan E, Bleakley N, Denholm E, Evans P, Gothard L, Hanson J, PeckittC, Reise S, Ross G, Sharp G, Symonds-Tayler R, Tait D, YarnoldJ, Breast Technology GroupRadiother Oncol. 2007 Mar;82(3):254-64.
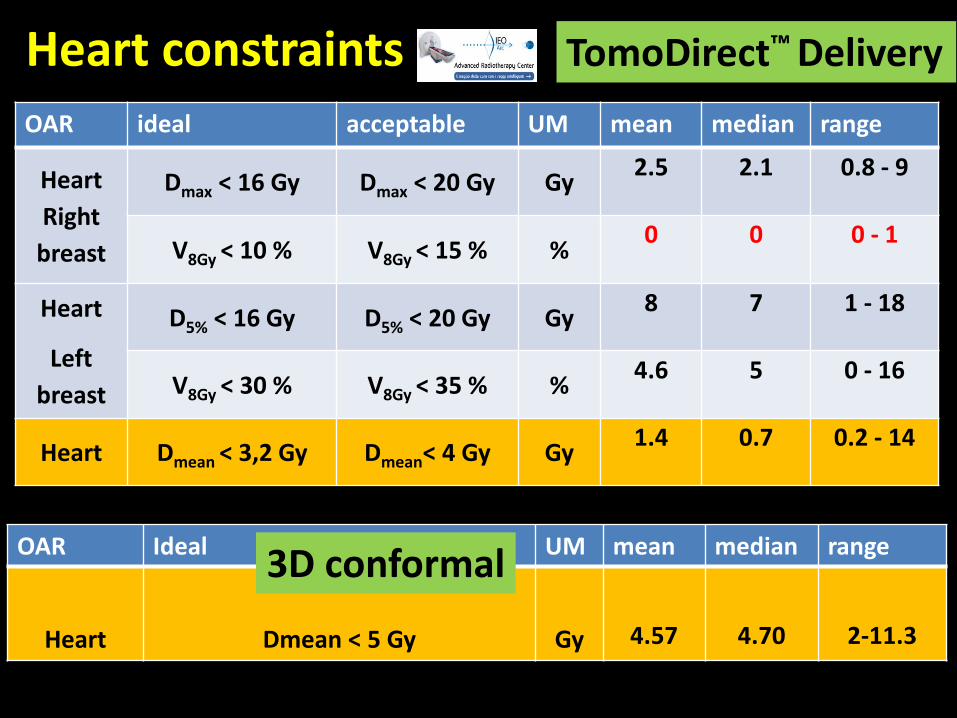
Heart constraintsOAR ideal acceptable UM mean median range
HeartRight
breast
Dmax < 16 Gy Dmax < 20 Gy Gy 2.5 2.1 0.8 - 9
V8Gy < 10 % V8Gy < 15 % % 0 0 0 - 1
Heart
Left breast
D5% < 16 Gy D5% < 20 Gy Gy 8 7 1 - 18
V8Gy < 30 % V8Gy < 35 % % 4.6 5 0 - 16
Heart Dmean < 3,2 Gy Dmean< 4 Gy Gy 1.4 0.7 0.2 - 14
OAR Ideal UM mean median range
Heart Dmean < 5 Gy Gy 4.57 4.70 2-11.3
3D conformal
TomoDirect™ Delivery
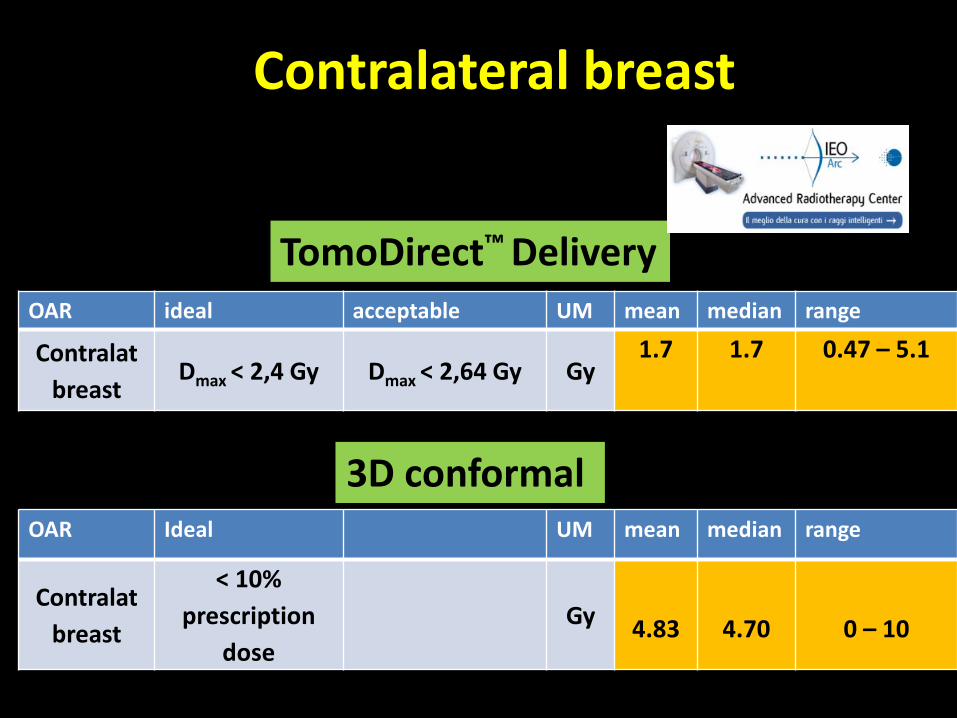
Contralateral breast
OAR ideal acceptable UM mean median range
Contralatbreast
Dmax < 2,4 Gy Dmax < 2,64 Gy Gy1.7 1.7 0.47 – 5.1
OAR Ideal UM mean median range
Contralatbreast
< 10% prescription
doseGy 4.83 4.70 0 – 10
3D conformal
TomoDirect™ Delivery
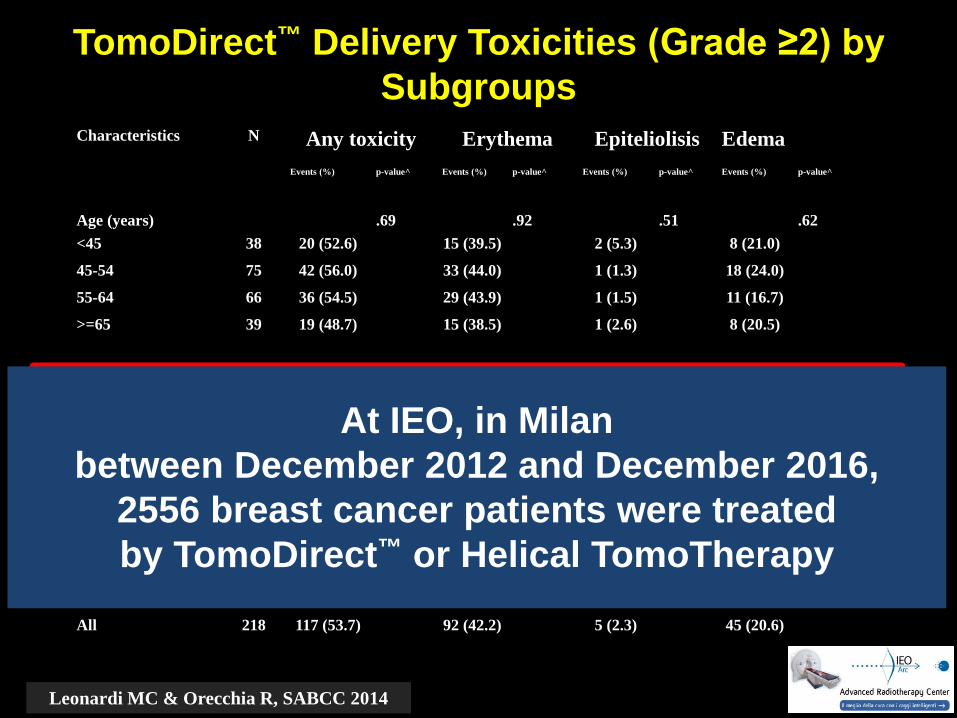
Characteristics N Any toxicity Erythema Epiteliolisis EdemaEvents (%) p-value^ Events (%) p-value^ Events (%) p-value^ Events (%) p-value^
Age (years) .69 .92 .51 .62<45 38 20 (52.6) 15 (39.5) 2 (5.3) 8 (21.0)
45-54 75 42 (56.0) 33 (44.0) 1 (1.3) 18 (24.0)
55-64 66 36 (54.5) 29 (43.9) 1 (1.5) 11 (16.7)
>=65 39 19 (48.7) 15 (38.5) 1 (2.6) 8 (20.5)
Breast volume (cc) .0004 .03 .04 .048<500 110 46 (41.8) 39 (35.4) 1 (0.9) 17 (15.4)
500-1000 85 54 (63.5) 40 (47.1) 2 (2.3) 21 (24.7)
>1000 23 17 (73.9) 13 (56.5) 2 (8.7) 7 (30.4)
Chemotherapy .66 .59 .29 .31No 172 91 (52.9) 71 (41.3) 3 (1.7) 38 (22.1)
Yes 46 26 (56.5) 21 (45.6) 2 (4.3) 7 (15.2)
All 218 117 (53.7) 92 (42.2) 5 (2.3) 45 (20.6)
TomoDirect™ Delivery Toxicities (Grade ≥2) by Subgroups
Leonardi MC & Orecchia R, SABCC 2014
At IEO, in Milanbetween December 2012 and December 2016,
2556 breast cancer patients were treated by TomoDirect™ or Helical TomoTherapy
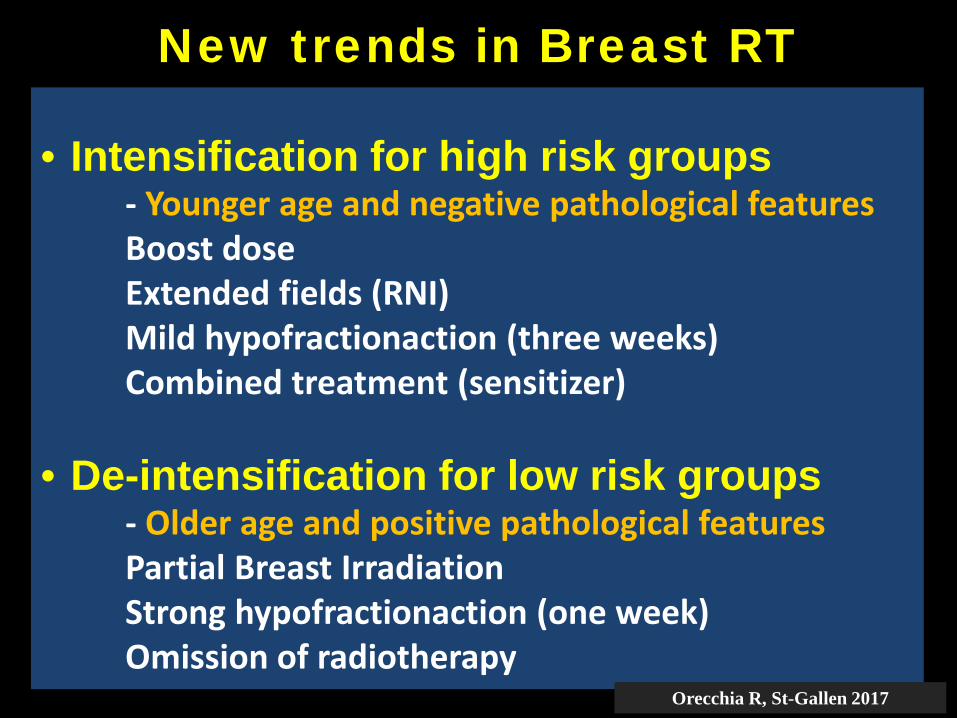
• Intensification for high risk groups- Younger age and negative pathological featuresBoost doseExtended fields (RNI)Mild hypofractionaction (three weeks)Combined treatment (sensitizer)
• De-intensification for low risk groups- Older age and positive pathological featuresPartial Breast IrradiationStrong hypofractionaction (one week)Omission of radiotherapy
New trends in Breast RT
Orecchia R, St-Gallen 2017
Acute side effects are generally common inoccurence, and self-limiting
Skin reactions dominate the early toxicity profile
The most common late toxicities are on theappearance of the breast, such as persistent breastedema, hyperpigmentation, and fibrosis
Lymphedema, radiation pneumonitis and cardiacmorbidity are very uncommon, but can havesignificant health consequences
How we can reduce toxicities
in most patients?
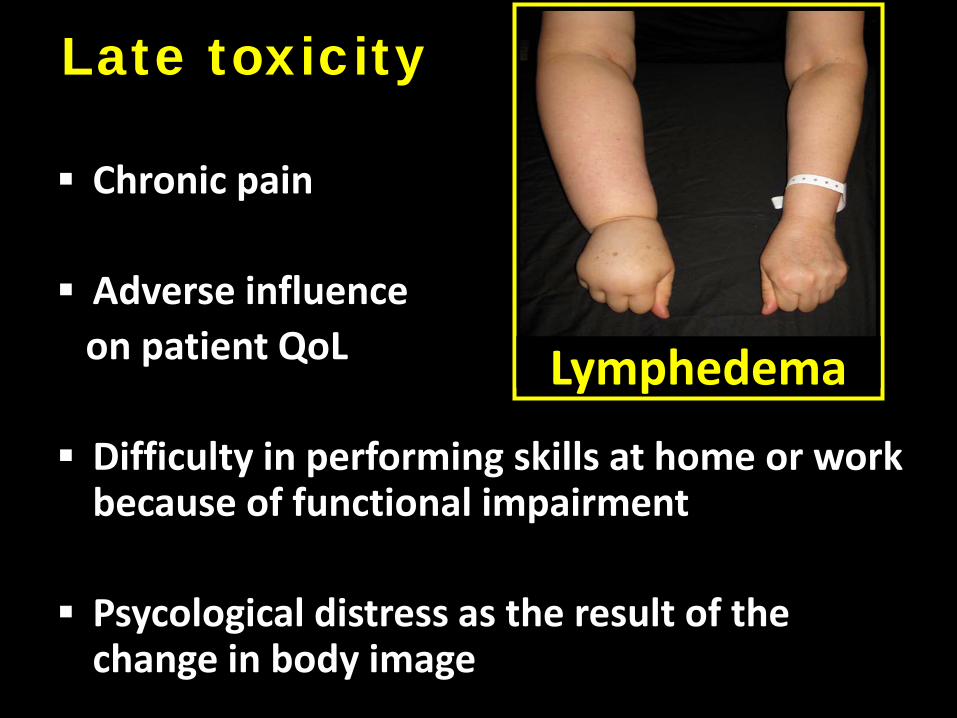
Chronic pain
Adverse influenceon patient QoL
Difficulty in performing skills at home or work because of functional impairment
Psycological distress as the result of the change in body image
Lymphedema
Late toxicity
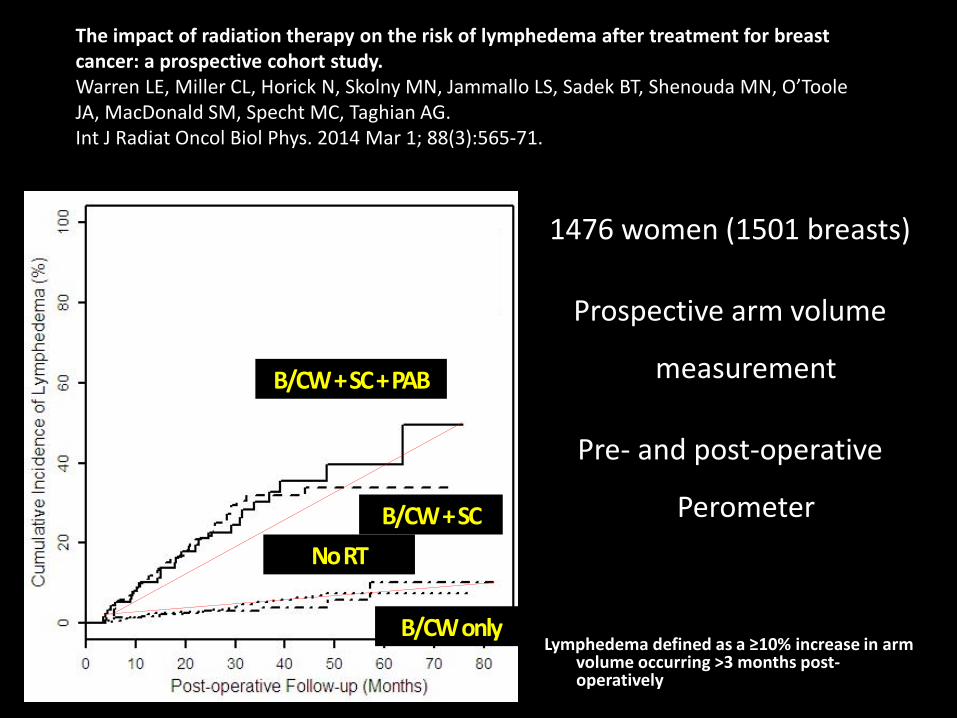
1476 women (1501 breasts)
Prospective arm volume
measurement
Pre- and post-operative
Perometer
Lymphedema defined as a ≥10% increase in arm volume occurring >3 months post-operatively
No RT
B/CW only
B/CW + SC + PAB
B/CW + SC
The impact of radiation therapy on the risk of lymphedema after treatment for breast cancer: a prospective cohort study.Warren LE, Miller CL, Horick N, Skolny MN, Jammallo LS, Sadek BT, Shenouda MN, O’Toole JA, MacDonald SM, Specht MC, Taghian AG.Int J Radiat Oncol Biol Phys. 2014 Mar 1; 88(3):565-71.
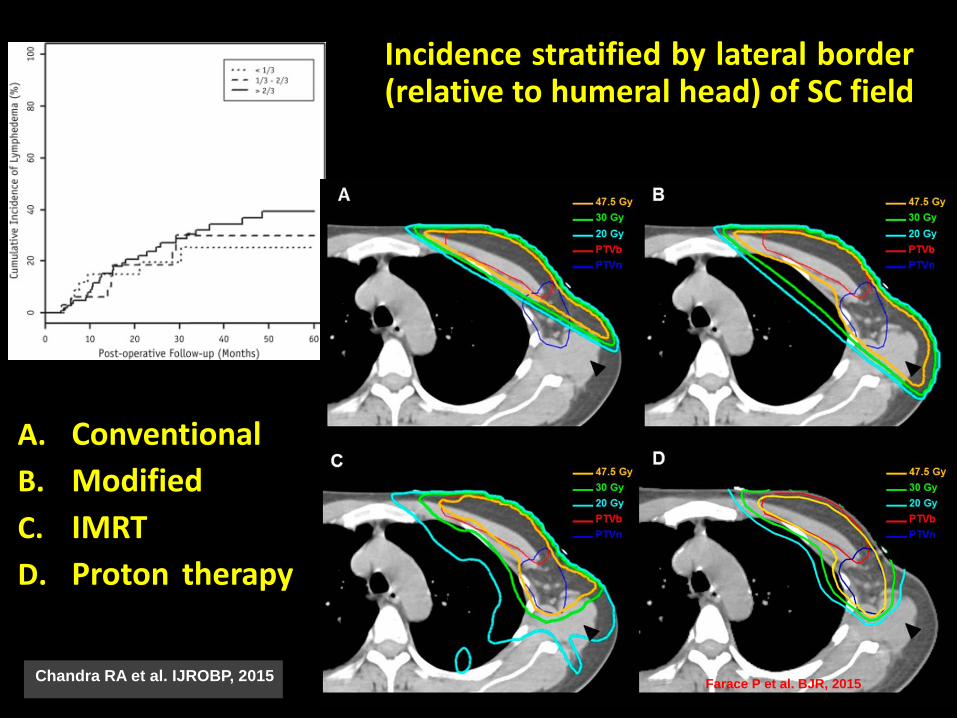
Chandra RA et al. IJROBP, 2015
Incidence stratified by lateral border(relative to humeral head) of SC field
Farace P et al. BJR, 2015
A. ConventionalB. ModifiedC. IMRTD. Proton therapy
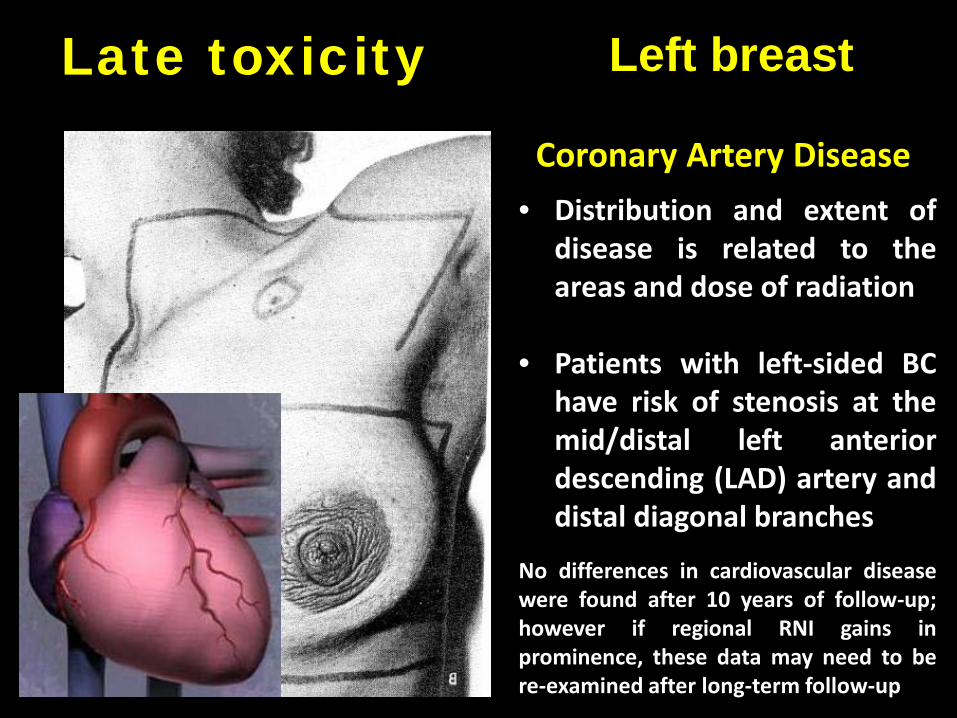
Left breast
Coronary Artery Disease• Distribution and extent of
disease is related to theareas and dose of radiation
• Patients with left-sided BChave risk of stenosis at themid/distal left anteriordescending (LAD) artery anddistal diagonal branches
No differences in cardiovascular diseasewere found after 10 years of follow-up;however if regional RNI gains inprominence, these data may need to bere-examined after long-term follow-up
Late toxicity
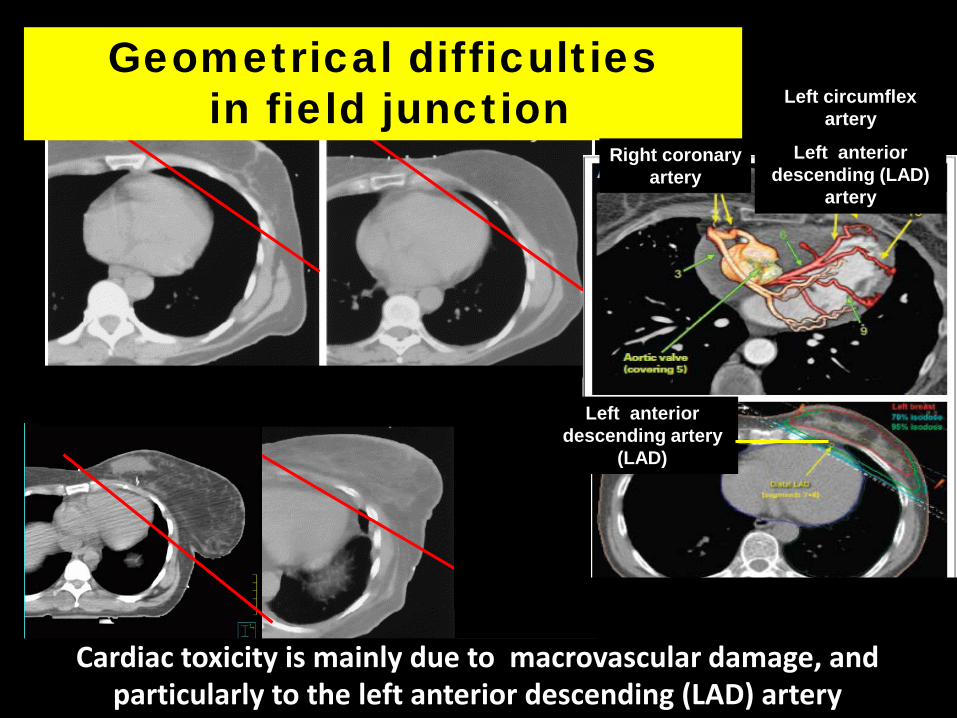
Geometrical difficultiesin field junction
Right coronary artery
Left circumflex artery
Left anterior descending (LAD)
artery
Left anterior descending artery
(LAD)
Cardiac toxicity is mainly due to macrovascular damage, and particularly to the left anterior descending (LAD) artery
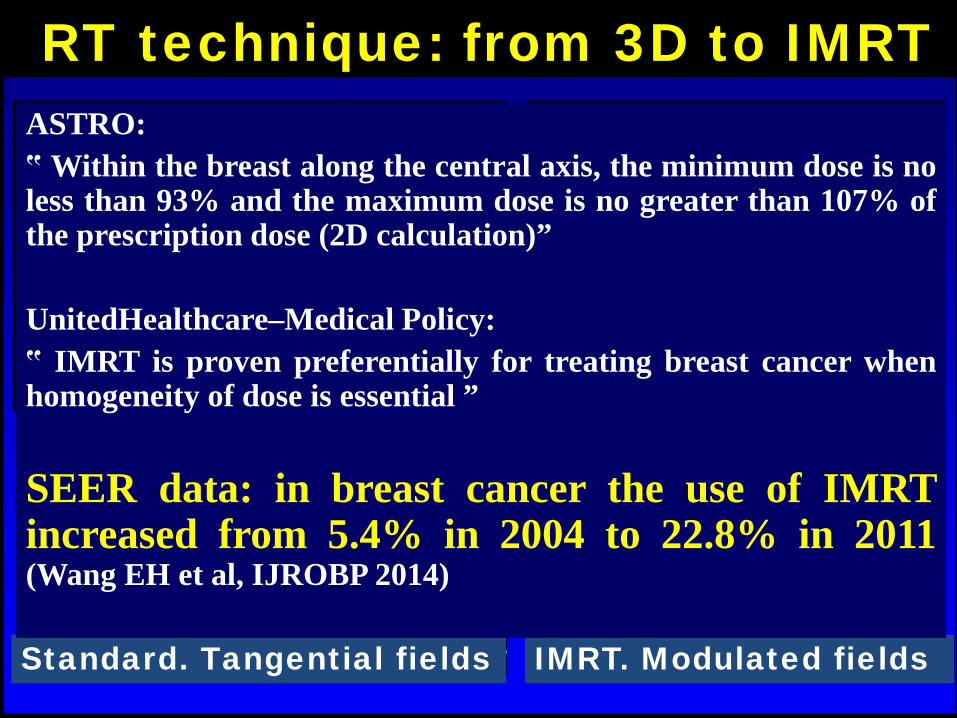
RT technique: from 3D to IMRT
Standard. Tangential fields IMRT. Modulated fields
ASTRO:‟ Within the breast along the central axis, the minimum dose is noless than 93% and the maximum dose is no greater than 107% ofthe prescription dose (2D calculation)”
UnitedHealthcare–Medical Policy:‟ IMRT is proven preferentially for treating breast cancer whenhomogeneity of dose is essential ”
SEER data: in breast cancer the use of IMRTincreased from 5.4% in 2004 to 22.8% in 2011(Wang EH et al, IJROBP 2014)
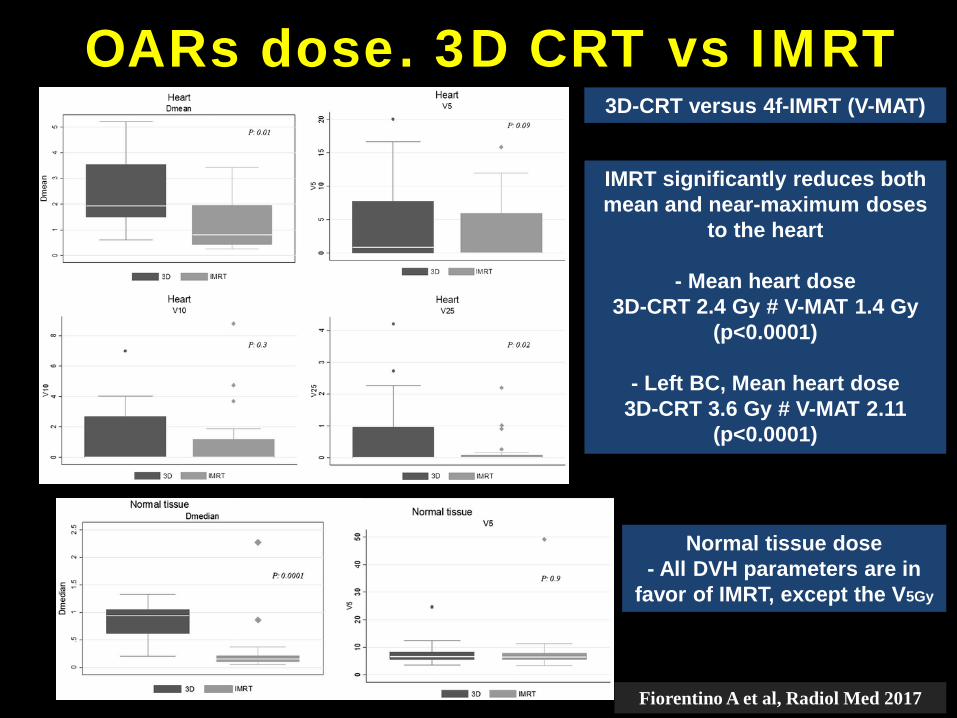
OARs dose. 3D CRT vs IMRT
IMRT significantly reduces both mean and near-maximum doses
to the heart
- Mean heart dose3D-CRT 2.4 Gy # V-MAT 1.4 Gy
(p<0.0001)
- Left BC, Mean heart dose3D-CRT 3.6 Gy # V-MAT 2.11
(p<0.0001)
3D-CRT versus 4f-IMRT (V-MAT)
Normal tissue dose- All DVH parameters are in
favor of IMRT, except the V5Gy
Fiorentino A et al, Radiol Med 2017
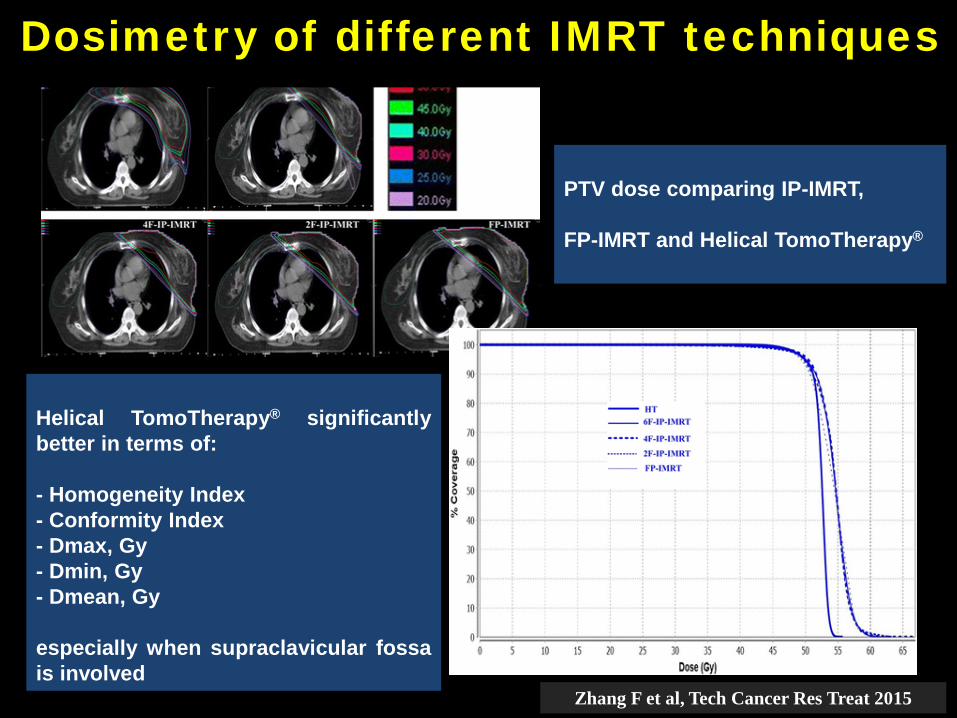
Dosimetry of different IMRT techniques
PTV dose comparing IP-IMRT,
FP-IMRT and Helical TomoTherapy®
Helical TomoTherapy® significantlybetter in terms of:
- Homogeneity Index- Conformity Index- Dmax, Gy- Dmin, Gy- Dmean, Gy
especially when supraclavicular fossais involved
Zhang F et al, Tech Cancer Res Treat 2015
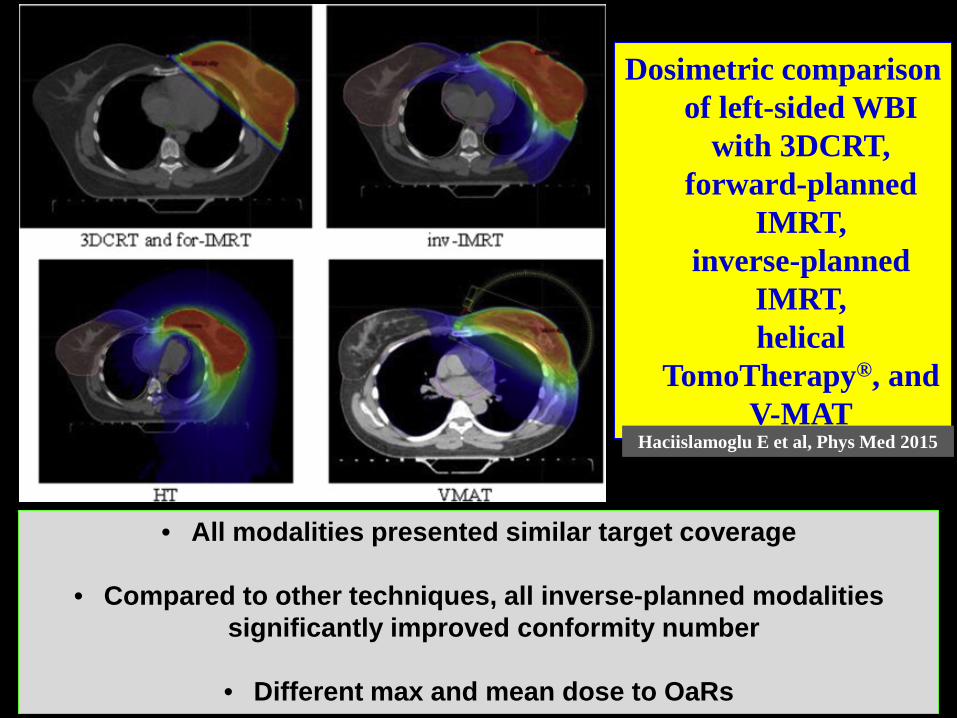
Dosimetric comparison of left-sided WBI
with 3DCRT, forward-planned
IMRT, inverse-planned
IMRT, helical
TomoTherapy®, and V-MAT
Haciislamoglu E et al, Phys Med 2015
• All modalities presented similar target coverage
• Compared to other techniques, all inverse-planned modalitiessignificantly improved conformity number
• Different max and mean dose to OaRs
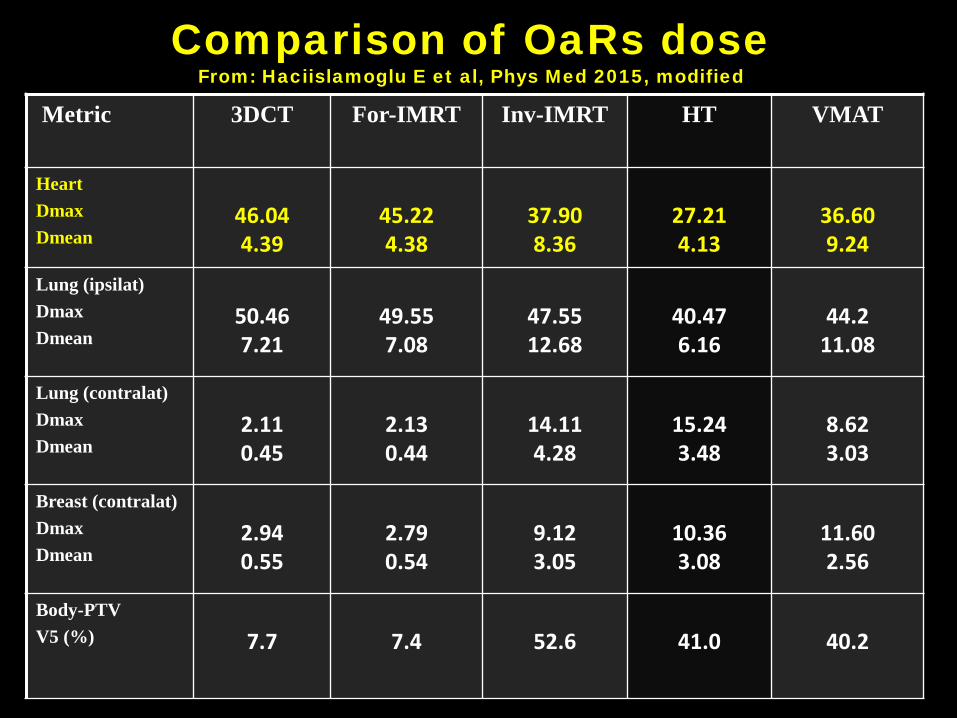
Metric 3DCT For-IMRT Inv-IMRT HT VMAT
HeartDmaxDmean
46.044.39
45.224.38
37.908.36
27.214.13
36.609.24
Lung (ipsilat)DmaxDmean
50.467.21
49.557.08
47.5512.68
40.476.16
44.211.08
Lung (contralat)DmaxDmean
2.110.45
2.130.44
14.114.28
15.243.48
8.623.03
Breast (contralat)DmaxDmean
2.940.55
2.790.54
9.123.05
10.363.08
11.602.56
Body-PTVV5 (%) 7.7 7.4 52.6 41.0 40.2
Comparison of OaRs dose From: Haciislamoglu E et al, Phys Med 2015, modified
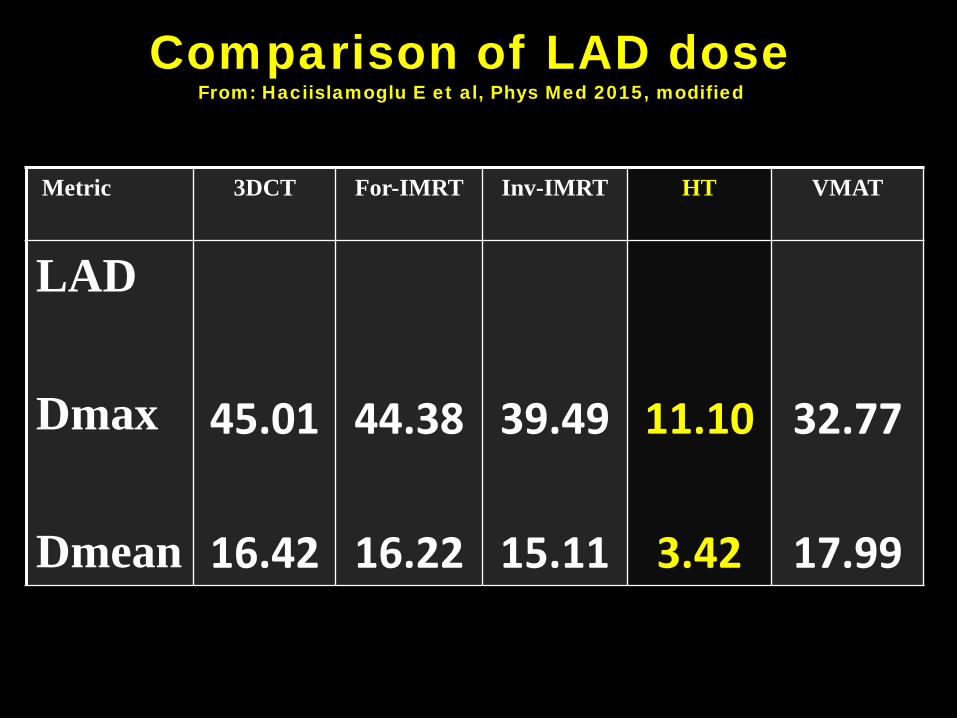
Metric 3DCT For-IMRT Inv-IMRT HT VMAT
LAD
Dmax
Dmean
45.01
16.42
44.38
16.22
39.49
15.11
11.10
3.42
32.77
17.99
Comparison of LAD dose From: Haciislamoglu E et al, Phys Med 2015, modified
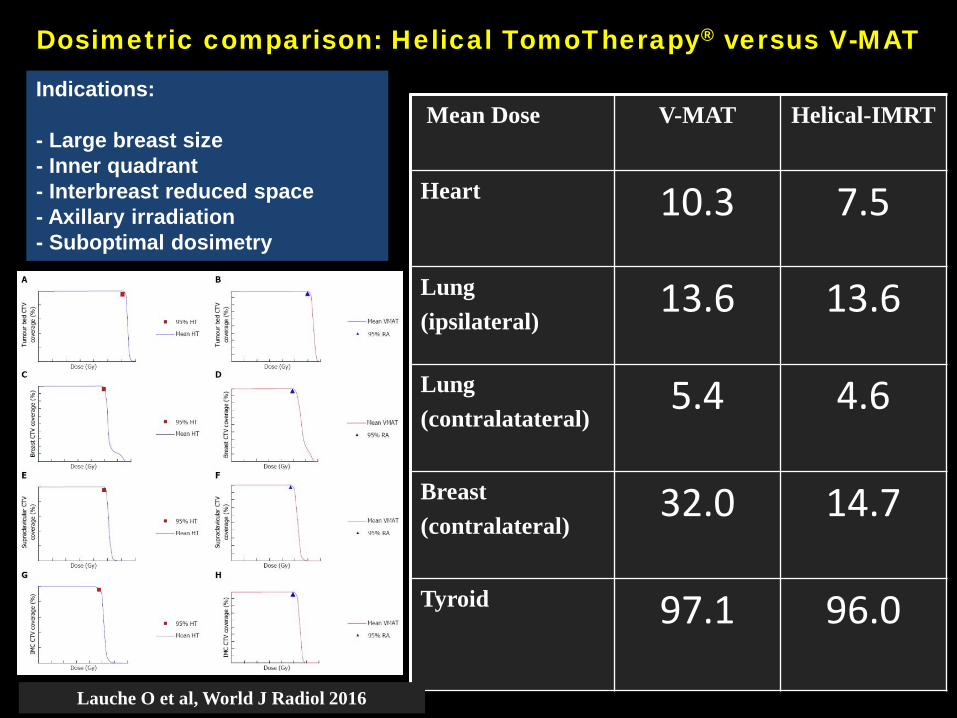
Mean Dose V-MAT Helical-IMRT
Heart 10.3 7.5
Lung(ipsilateral)
13.6 13.6
Lung(contralatateral)
5.4 4.6
Breast(contralateral)
32.0 14.7
Tyroid 97.1 96.0
Dosimetric comparison: Helical TomoTherapy® versus V-MAT
Lauche O et al, World J Radiol 2016
Indications:
- Large breast size- Inner quadrant- Interbreast reduced space- Axillary irradiation- Suboptimal dosimetry
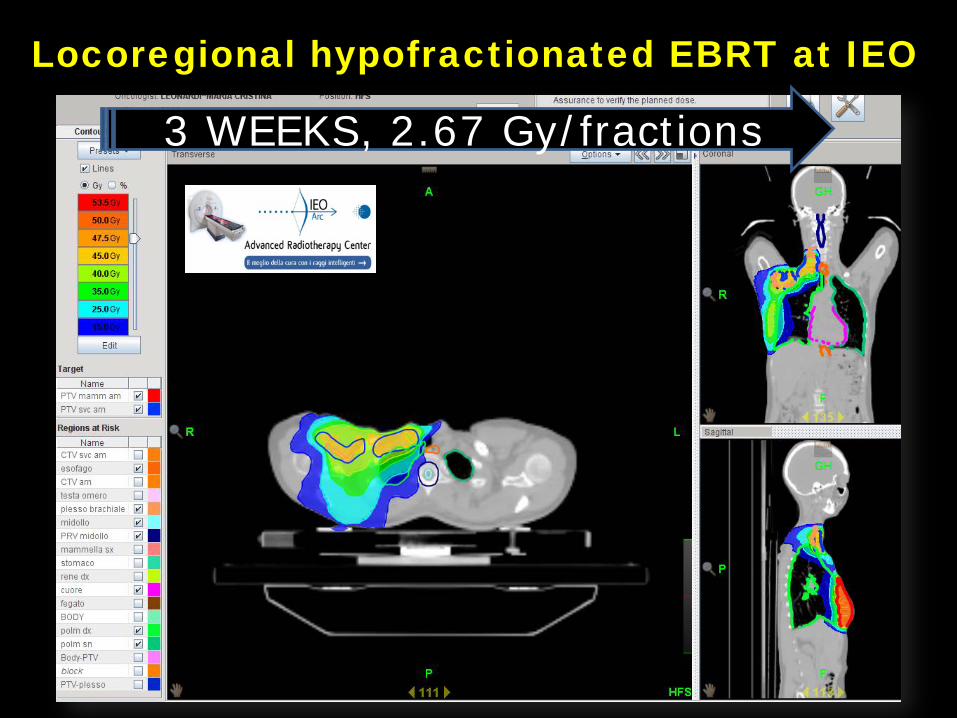
Locoregional hypofractionated EBRT at IEO
3 WEEKS, 2.67 Gy/fractions
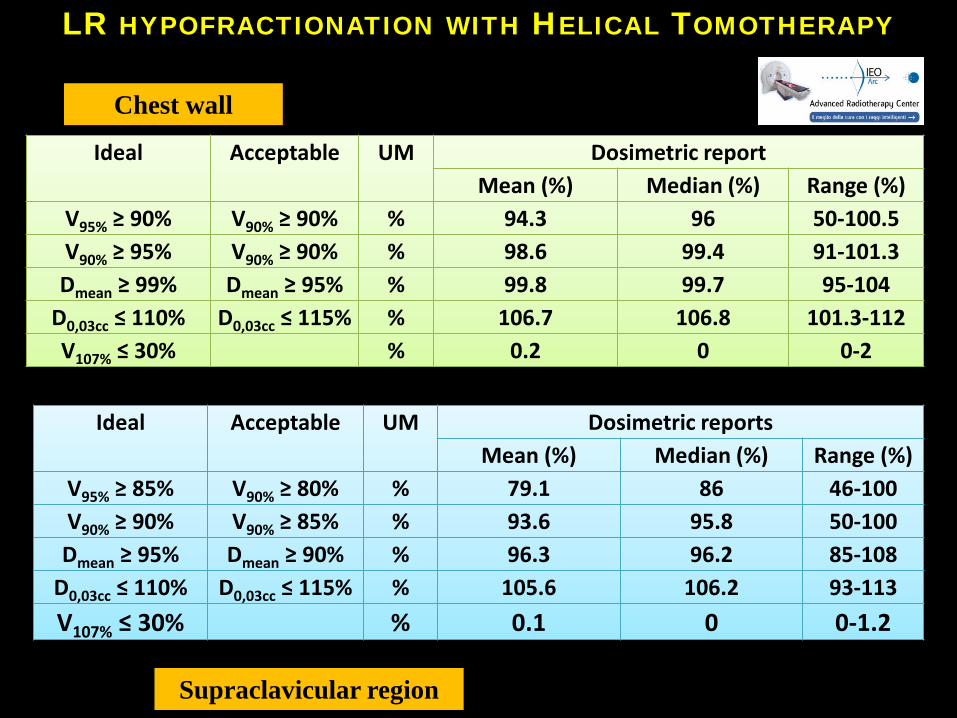
Ideal Acceptable UM Dosimetric reportMean (%) Median (%) Range (%)
V95% ≥ 90% V90% ≥ 90% % 94.3 96 50-100.5V90% ≥ 95% V90% ≥ 90% % 98.6 99.4 91-101.3Dmean ≥ 99% Dmean ≥ 95% % 99.8 99.7 95-104
D0,03cc ≤ 110% D0,03cc ≤ 115% % 106.7 106.8 101.3-112V107% ≤ 30% % 0.2 0 0-2
Ideal Acceptable UM Dosimetric reportsMean (%) Median (%) Range (%)
V95% ≥ 85% V90% ≥ 80% % 79.1 86 46-100V90% ≥ 90% V90% ≥ 85% % 93.6 95.8 50-100Dmean ≥ 95% Dmean ≥ 90% % 96.3 96.2 85-108
D0,03cc ≤ 110% D0,03cc ≤ 115% % 105.6 106.2 93-113V107% ≤ 30% % 0.1 0 0-1.2
Chest wall
Supraclavicular region
LR HYPOFRACTIONATION WITH HELICAL TOMOTHERAPY
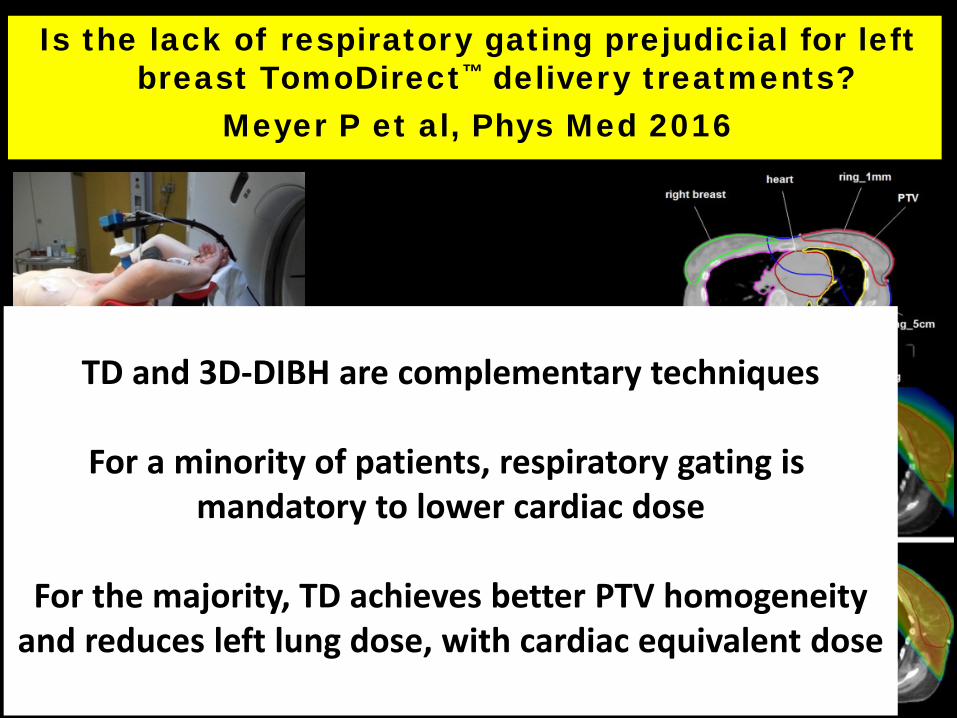
Is the lack of respiratory gating prejudicial for left breast TomoDirect™ delivery treatments?
Meyer P et al, Phys Med 2016
3D-FB TD-FB
IMRT-DIBH 3D-DIBH
TD and 3D-DIBH are complementary techniques
For a minority of patients, respiratory gating ismandatory to lower cardiac dose
For the majority, TD achieves better PTV homogeneityand reduces left lung dose, with cardiac equivalent dose
Intra-fraction respiratory motion and baselin drift during breast Helical TomoTherapy
Ricotti R et al, Radiother Oncol 2017
Polaris SPECTRA optical tracking
Passive marker
configurationThe breathing amplitude of the chest was less than 2 mm,on average, along all anatomical directions
The baseline drift of the body led to more significantset-up uncertainties than the respiratory motion
The main intra-fraction baseline drift were in posteriorand inferior directions and occured within the first
eight minutes of monitoring
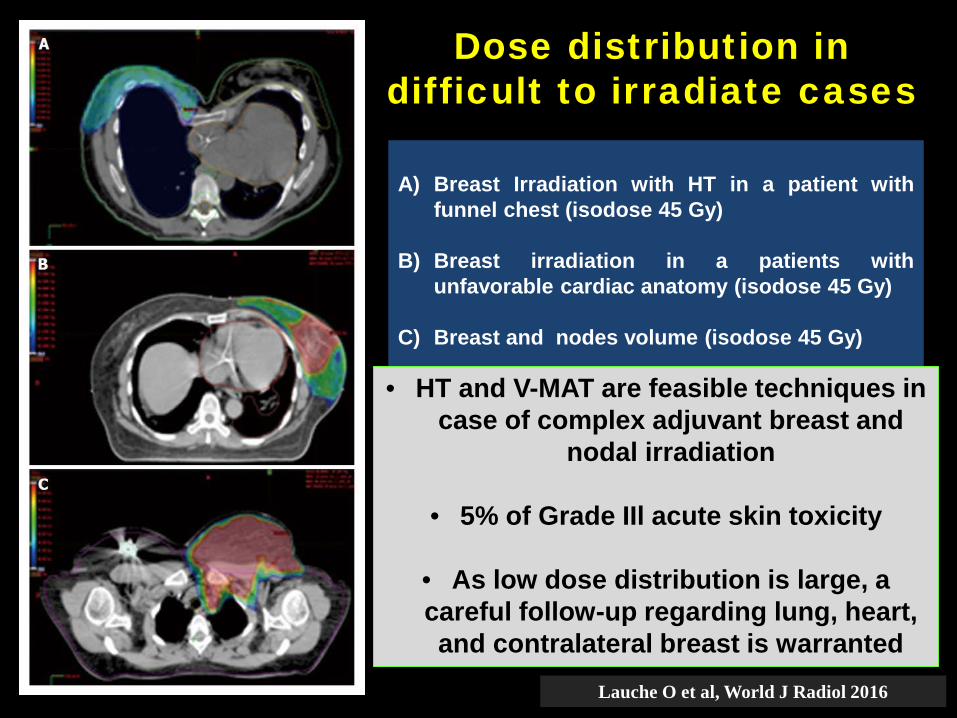
Dose distribution in difficult to irradiate cases
A) Breast Irradiation with HT in a patient withfunnel chest (isodose 45 Gy)
B) Breast irradiation in a patients withunfavorable cardiac anatomy (isodose 45 Gy)
C) Breast and nodes volume (isodose 45 Gy)
Lauche O et al, World J Radiol 2016
• HT and V-MAT are feasible techniques in case of complex adjuvant breast and
nodal irradiation
• 5% of Grade IIl acute skin toxicity
• As low dose distribution is large, a careful follow-up regarding lung, heart, and contralateral breast is warranted
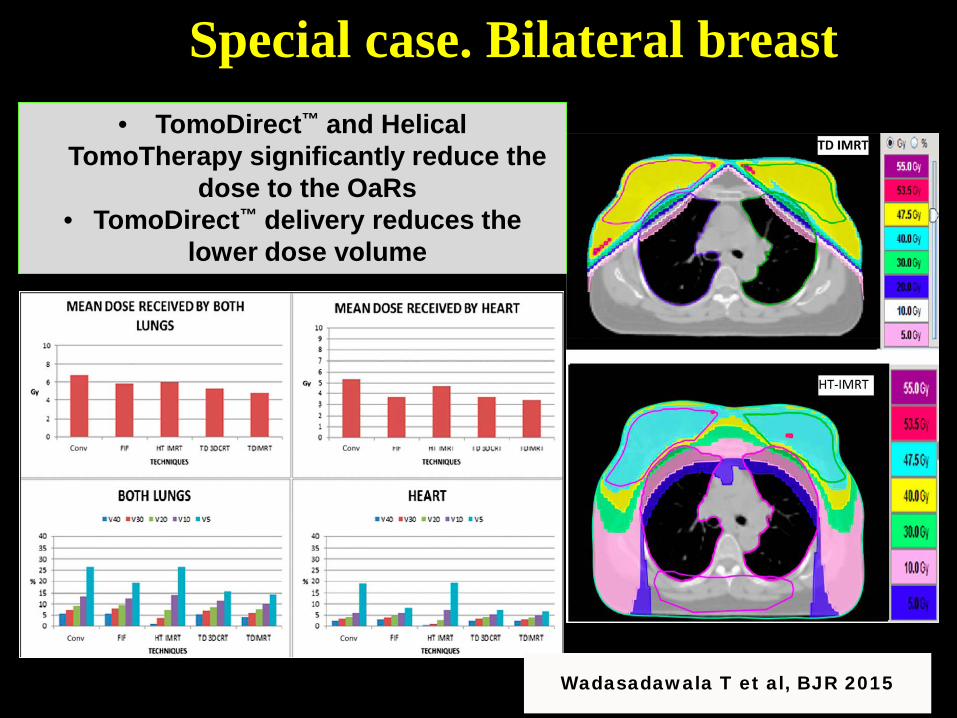
Special case. Bilateral breast
Wadasadawala T et al, BJR 2015
• TomoDirect™ and Helical TomoTherapy significantly reduce the
dose to the OaRs• TomoDirect™ delivery reduces the
lower dose volume
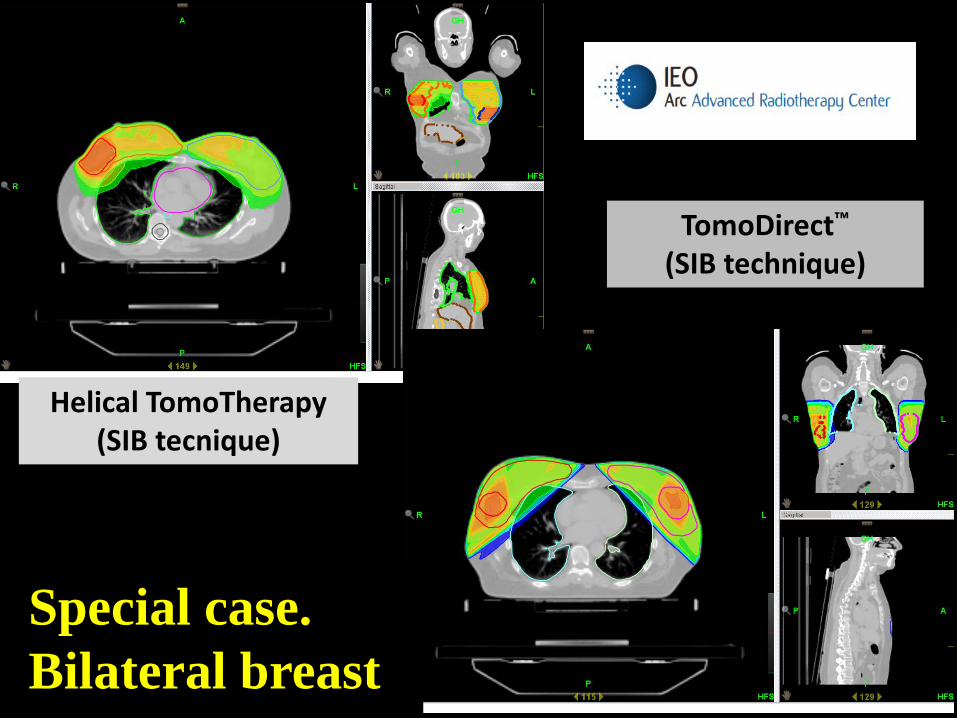
TomoDirect™
(SIB technique)
Helical TomoTherapy (SIB tecnique)
Special case. Bilateral breast
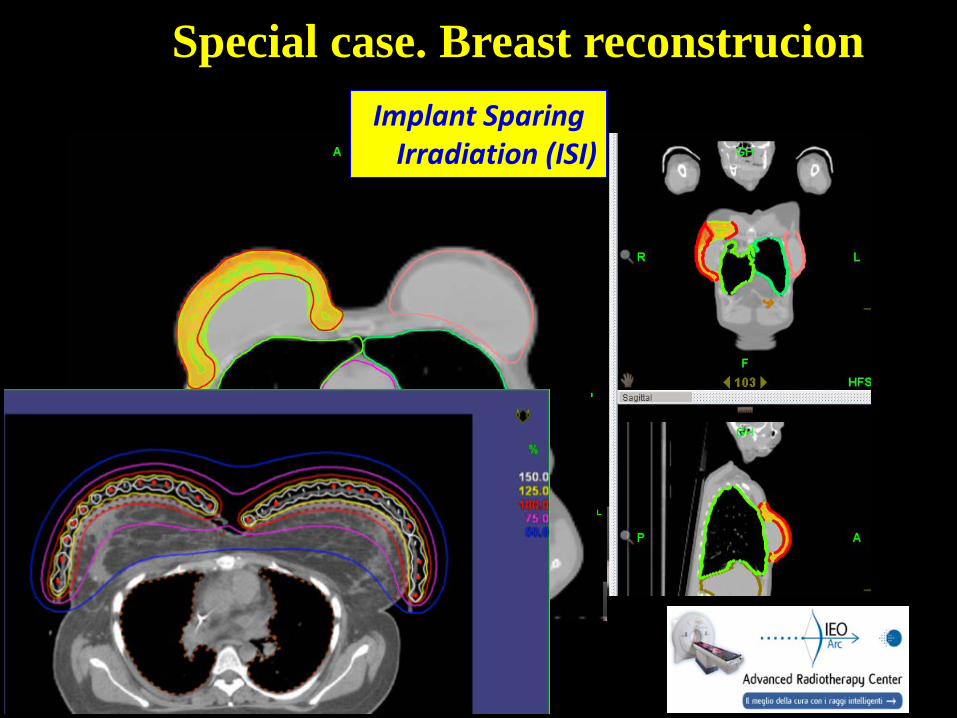
Implant Sparing Irradiation (ISI)
CTV “excluding implant”
Special case. Breast reconstrucion
Hypofractionated postmastectomy radiotherapy with Helical TomoTherapy in patients with
immediated breast reconstructionOrecchia R et al, in press
121 consecutive patients (stage II-III)with implant-based immediate reconstruction
86 of 121 (71.1%) with very high total score, as a resultsof optimal coverage of CW and RN, and optimal
sparing of all OARs
Excellent results for acute skin toxicity: the maximum Grade was 2 in 34.7% of the cases
Time to local or regional recurrence. Personalised Radiotherapy
The right treatment
to the right persons
at the right time
• Number of patients with breast cancer isincreasing and more cases are expected forradiation therapy in 2020-2025
• IMRT has shown to be able to increase thehomogeneity of the dose distribution in thetarget and to reduce the dose to the OARs
• Tailored radiation treatments are needed in theera of personalised medicine, with a greatattention to QoL aspects (reduced toxicities)
Take Home Message (I)
• Among the IMRT modalities, Helical andDirect TomoTherapy, show a very good level ofversatility and flexibility in breast treatment
• These characteristics allow to face the newchallenges of breast RT in hypofractionaction,locoregional treatment and special cases
• IMRT, including Helical TomoTherapy, is anattractive technique in the setting of complexadjuvant breast and node irradiation, but notthe only…..
Take Home Message (II)