Embed Size (px)
Citation preview

Tokyo Subway Sarin Attack by Aum Shinrikyo Lessons Learned
from medical perspective
Mitsuyoshi Urashima MD, PhD, MPH
Jikei University School of Medicine

Introduction
• The use of chemical, biological and radiological weapons by terrorist group remains a potent risk to the world.
• At March 20th, 1995 in Japan, Aum Shinrikyo (Japanese apocalyptic cult), dispersed sarin, a chemical weapon, in the 4 Tokyo subway system, where 13 stations locating in the central government, were affected simultaneously, killing 13 people and prompting 6,000 others to seek hospital treatment.
• In this presentation, I will describe about the importance of information sharing among medical, public health and law enforcement in early phase of crisis, which we failed to do, from medical perspective.

• 7:00-8:10, On Monday March 20, in 1995• At the peak of the morning rush hour• The chemical agent used by Aum Shinrikyo (Japanese
apocalyptic cult), liquid sarin (35%: relatively lower conc.) contained in plastic bags (900mL) which each team then wrapped in newspaper.
• Carrying their packets of sarin and umbrellas with sharpened tips, the perpetrators boarded their appointed trains.
• By leaving the punctured packets on the floor, the sarin was allowed to leak out into the train car and stations.
• This sarin affected passengers, subway workers, and those who came into contact with them.

As the train approached Shin-Ochanomizu Station, he punctured one of his two bags of sarin, leaving the other untouched and exited the train at Shin-Ochanomizu.
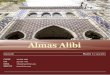
Center of TokyoGovernmental function
The train proceeded down the line with the punctured bag of sarin leaking until 4 stops later at Kasumigaseki Station.
There, the bags were removed and eventually disposed of by station attendants,
of whom two died.
Chiyoda-line

2 bags of sarin
release here1st bag was removed.
2nd bag was removed.
Marunouchi-line

Sarin release
Hibiya line 1


• At the day, first patient was transferred by an ambulance into our hospital around 8:30 that is just rash hour time in Japan. The patient has been complaining “Dyspnea” and “Visually darkness”. Soon after that, number of patients visiting our hospital increased.

• Almost clinical departments are busy for meetings or preparedness of operations. Doctors on night duty usually transfer patients’ information Ordinal outpatient clinics start from 9:00AM. That’s why; it was very hard for nurses in emergency room to catch clinical doctors to see the patient at emergency room. At the time, we had not “Department of Emergency Medicine” yet at the time. One surgeon and one physician on duty at the day coped with these increasing patients. During initial phase, patients who complained narrow vision were referred to ophthalmology and patients who complained dyspnea were treated with oxygen inhalation and drip infusion on beds at ER.

• In a short time, number of patients at ER overflowed and further patients were laid down on the waiting sheets at other outpatient clinics and open beds at clinical wards. At this time, many doctors came to treat these patients on their own judgment.
• The surgeon who was on duty and saw first patient became the leader and tried to uniform treatment strategy. As contracted pupil was the common sign among the patients, “atropine” was considered as first choice of therapy. However, before decision making, he asked opinions of Professors in department of forensic medicine and public health. It was around 9:30 AM: One hour after accepting the first patient.

• Two professors concluded that causative agent could be organophosphate and PAM would be the first choice. The doctor asked hospital pharmacy to find that there were only two ampoules of PAM in the hospital. Immediately, the surgeon asked chief pharmacist to collect ampoules of PAM as many as possible around greater Tokyo area. Two ampoules of PAM were used for one with unconsciousness and another with hypotension. Soon, enough amount of PAM had arrived and protocol was written in a paper of A4 and copied to handout to places where the patients were laid.
Professor TakatsuForensic Medicine
Causative agent could be organophosphate and PAM would be the first choice

• The number of patients inflamed. The president of hospital next took over the leader for this chaos and some doctors were dispatched for triage: patients with contracted pupil alone were got together into an auditorium.
• At 10:15, doctors in Shinshyu university hospital who experienced Matsumoto Sarin Attack a half year before sent the FAX to the hospitals in Tokyo including ours informing suspicion of Sarin.
9:10AM Metropolitan Fire Department informed hospitals that “Acetonitrile (methyl cyanide)” without any proof.
10:15, Prof. Yanagisawa in Shinshyu university hospital and chief of neurology, who experienced Matsumoto Sarin Attack a half year before sent the FAX to the hospitals in Tokyo including ours informing suspicion of Sarin.

• After 11AM, “Sarin” as a causative agent was informed by law investigators.
• Responding to this information, clothes of these patients were taken off for decontamination. Patients in Pediatric and Obstetrics were transferred to other wards.
• Other hospitals having patients exposed to Sarin tried to gather PAM after getting the information released around 11AM. However, as we had collected PAM around greater Tokyo area as many as possible, they needed to transport distant area in Japan. Thus, they could use PAM for the first patient as early as 2PM.
• We shutout media reporters to protect patients’ privacy. Thus, our activity during Tokyo Sarin Attack was not well known to Japanese public. However, we saw more than 2,000 patients for three days without any death.
After 11AM, “Sarin” as a causative agent was informed by law investigators.

One passenger kicked the sarin packets out of the train and onto Kodenmachō Station's subway platform. Four people in the station died as a result.
Passengers stumbled out and collapsed on the station's platform and the train was taken out of service.
Hibiya line 2

• Video

By Shinkan-sen
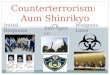
Tokyo Metro
8:10 A conductor informed “Explosion” Sent emergent cars to the scene 8:35 Stopped Hibiya Line9:27 All metro stopped Total 13 stations
Metropolitan Fire Department
HAZMAT
9:10 Acetonitrile
Many causalities Coordinated rescue
riot police
Dispatch doctors to the scene
Inspection of the attacked subway cars
material
National Research Institute of Police Science
11:00 Press conference
Causative agent is sarin!
TV
10:15 FAX fromMatsumoto
Self defense forces
Decontamination
Not shared
Control center
Could not dispatch
other patients
PAM
West side of Japan
by Air


summary
Medical Public Health
Police
Fire
Media
Government
We, medical facilities, should have connections with raw enforcement from ordinal time, through drill or table top exercise.