-
7/29/2019 Tocolysis A clinically based review
1/29
Tocolysis A clinically based review.
Katie M Groom BSc MB BS *
(Clinical Research Fellow)
Phillip R Bennett PhD MD FRCOG
(Professor of Obstetrics and Gynaecology)
Imperial College Parturition Research Group
Imperial College of Science, Technology and Medicine
Institute of Reproductive and Developmental Biology
Hammersmith Campus
Du Cane Road
London. W12 0HN
*Author for correspondence
Telephone No: 020 7594 2137
1
-
7/29/2019 Tocolysis A clinically based review
2/29
Fax No: 020 7594 2189
E-mail: [email protected]
2
-
7/29/2019 Tocolysis A clinically based review
3/29
Premature birth, the major cause of neonatal morbidity and
mortality, complicates up to
10% of all pregnancies. Mortality rates from 32 weeks gestation
are similar to those at
term 1 and therefore it is the very early premature deliveries
at greatest risk of neonatal
death and serious morbidity, which are most likely to benefit
from treatment. This
accounts for 1-2% of the obstetric population. 2
Current treatment of preterm labour is reactive, with tocolytics
only being used once
contractions have started. However, it is now well recognised
that labour both at term and
preterm resembles an inflammatory reaction with upregulation of
inflammatory cytokines
and prostaglandins in the fetal membranes, myometrium and
cervix. 3, 4, 5 This is believed to
occur over a period of several weeks with the onset of
contractions occurring towards the
end of this complex process. 6 Multiple feed forward mechanisms
within this process mean
that once started clinical labour is difficult to stop.
Therefore it may be expected that
tocolytic drugs, targeted solely at stopping contractions, will
be unsuccessful at preventing
preterm delivery. Indeed meta-analyses of studies of tocolytics,
although showing a
prolongation of pregnancy to some degree, do not show a
significant impact on preterm
delivery rates or neonatal outcome. 7 In addition these drugs
are associated with significant
fetal and / or maternal side effects which should always be
considered before prescribing
tocolytic therapy.
There have been recent developments in the prediction of women
at risk of preterm
delivery 8, 9, 10 and increasing interest in preventative
treatment such as cervical cerclage,
cyclo-oxygenase inhibitors, progestogens and antibiotics. These
approaches may be more
successful at reducing overall preterm delivery rates and
improving neonatal outcome but
this remains to be seen. For the purpose of this review we have
concentrated on the acute
3
-
7/29/2019 Tocolysis A clinically based review
4/29
management of preterm labour and will consider the mechanisms of
action of tocolytic
drugs, the rationale for their use and their possible benefits
and side effects.
4
-
7/29/2019 Tocolysis A clinically based review
5/29
Mechanism of action
Myometrial cell contractility is modulated by the intracellular
concentration of calcium.
Increased intracellular calcium, from a variety of different
mechanisms (see table 1) binds
with calmodulin and leads to activation of calcium dependent
myosin light chain kinase
(CDMLK), this in turn triggers an ATP-dependent phosphorylation
of myosin. This allows
interaction with actin filaments and crossbridges form which
result in contraction of the
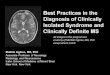
myometrial cell. (see figure 1)
Subgroups of tocolytic drugs act at a variety of different
levels of this pathway to cause
inhibition of contractions. This may be via mechanisms specific
to labour (oxytocin
receptor antagonists, cyclo-oxygenase inhibitors and possibly
nitric oxide donors) or by a
non-specific action on cell contractility (-mimetcs, magnesium
sulphate and calcium
channel blockers). (see figure 1)
5
-
7/29/2019 Tocolysis A clinically based review
6/29
Rationale for tocolytic use
Extreme prematurity is associated with high neonatal mortality
and serious morbidity and
therefore the rationale for the use of any intervention must be
that it will lead to
improvements in neonatal survival and wellbeing without causing
undue risk to either
mother or fetus. It is widely believed that improvement will be
achieved by prolonging
pregnancy until the fetus is more mature and / or to allow time
for additional therapies to
be administered which will improve neonatal outcome.
Finnstrm et al studied a population of almost 250 000 births and
demonstrated a gain in
infant survival from 8% at 23 weeks gestation to 74% at 26 weeks
gestation (see figure
2). 11 This equates to a survival gain of 3% per day at these
low gestational ages.
Therefore if tocolytic drugs are successful at delaying delivery
for up to seven days 7 then
we would expect to see considerable improvements in survival
rates and the risk of serious
morbidity. Further population studies have shown similar large
changes in mortality rates
for each additional week of gestation and for each 100g increase
in birthweight at lower
gestational ages. However, at higher gestational ages (>32
weeks) comparable changes in
gestation and birthweight only have a relatively small impact on
mortality. 1
Respiratory distress syndrome (RDS) is the most common serious
complication of
prematurity and is associated with immediate and long term
mortality and morbidity. The
use of antenatal corticosteroids to improve fetal lung maturity
is now well documented
and recommended for both its health and cost benefits. 12, 13 A
Cochrane review analysed
18 trials covering over 3700 births and demonstrated that
antenatal corticosteroids lead to
a significant reduction in mortality (OR 0.6 95% CI 0.48-0.75)
and RDS (OR 0.53 95%
CI 0.44-0.63). There is a trend towards a reduction in RDS at
24-48 hours and this
becomes significant at 48 hours and up to seven days after
administration. This
6
-
7/29/2019 Tocolysis A clinically based review
7/29
improvement in fetal lung maturity is associated with a
substantial reduction in the risk of
intraventricular haemorrhage (IVH) but has no effect on the risk
of necrotising
enterocolitis (NEC) or chronic lung disease (CLD). 14 No adverse
consequences of a
single course of corticosteroids were identified by this
meta-analysis.
Advances in neonatal care have lead to significant improvements
in neonatal survival
despite no change in preterm delivery rates. The introduction of
neonatal intensive care
units (NICU) in the 1960s is likely to have been one of the most
influential factors
affecting survival rates. Neonatal outcome is also dependent on
the infant being delivered
within a maternity unit with NICU services rather than being
transferred after delivery.
Several studies have demonstrated better outcomes for inborn
infants compared to
outborn infants, 15, 16 although most studies do not adjust for
perinatal risk factors,
birthweight and gestational age. A recent study of 3769
singleton infants born at 32
weeks gestation admitted to 17 Canadian NICUs controlled for
perinatal risks and
admission illness severity. They demonstrated that outborn
infants were at higher risk of
death (OR 1.7 95% CI 1.2-2.5), grade III IV IVH (OR 2.2 95% CI
1.5-3.2), patent
ductus arteriosus (PDA) (OR 1.6 95% CI 1.2-2.1), RDS (OR 4.8 95%
CI 3.6-6.3) and
nosocomial infection (OR 2.5 95% CI 1.9-3.3). Although outborn
infants were more likely
to be of younger gestational age, neonatal outcome was
significantly worse even with
subanalysis of each gestational age group (26 weeks, 27-28 weeks
and 29-30 weeks but
not at 31-32 weeks gestational age). 17 Therefore any therapy
which allows in utero
transfer of mother and baby might be expected to lead to
improved mortality and
morbidity at very early gestational ages. As we will discuss
below however, there is
currently no evidence that this is in fact the case.
7
-
7/29/2019 Tocolysis A clinically based review
8/29
Tocolytics and Outcome
There are many randomised controlled trials assessing the
effectiveness of tocolytic drugs
compared with placebo or no tocolytic drug. The majority are too
small to be clinically
significant on their own. The largest meta-analysis of these
trials, by Gyetvai et al, 7
retrieved 76 trials of which 18 met the inclusion criteria: all
randomised controlled trials
comparing the effect of tocolytic with placebo or no tocolytic
in preterm labour;
perinatal, neonatal or maternal outcome reported, loss to follow
up of >20% of total
recruits; data reported on per-patient treated basis. This
meta-analysis included trials of-
mimetics, magnesium sulphate, indomethacin, atosiban and ethanol
and demonstrated that,
with the exception of magnesium sulphate, these tocolytics did
prolong pregnancy for up
to seven days compared with placebo or no tocolytic.
Evidence discussed previously would suggest that prolonging
pregnancy by one week
should improve morbidity and mortality because delivery is
later, birthweight is increased
and time is available for antenatal corticosteroids and in utero
transfer. However, this
meta-analysis7
showed that none of these drugs affected perinatal death rates,
incidences
of RDS, IVH, NEC, PDA, seizures, hypoglycaemia or neonatal
sepsis (see table 2).
Indomethacin was the only drug, in one study, 18 to reduce
preterm delivery rates (
-
7/29/2019 Tocolysis A clinically based review
9/29
is not used appropriately for the administration of
corticosteroids or for in-utero transfer
to hospitals with NICU facilities. For example in one recent
study, which demonstrated a
delay in delivery of seven days compared to placebo, less than
50% of patients received
antenatal corticosteroids. 19 Many of the tocolytic trials
predate the routine use of
corticosteroids and therefore the lack of effect on outcome is
not related to lack of effect
of corticosteroids. A trial of tocolysis, corticosteroids and
in-utero transfer versus nothing
would be required to fully assess this but is not ethically
justifiable and unlikely to be
undertaken!
Some trials included too many women at later gestational ages
when the time gained by
the drug does not have a significant impact on neonatal survival
or morbidity. In the
Canadian Preterm Labor Investigators Group trial (n=708) 80% of
women recruited were
28 weeks. 20 It may also be possible that tocolytic drugs are
only effective at prolonging
pregnancy at these more advanced gestational ages and that very
early preterm labour
does not respond well to tocolytic treatment. The majority of
studies do not report
subanalysis of data to assess if prolongation of pregnancy is
gestation specific. Romero et
al, in their study of atosiban vs placebo, report that only at
gestational ages 28 weeks did
more women receiving atosiban stay undelivered at 24 hours, 48
hours and 7 days
compared with placebo. This prolongation of pregnancy was not
demonstrated in those
-
7/29/2019 Tocolysis A clinically based review
10/29
it should be considered that tocolytics themselves may be
harmful and therefore any
significant benefit gained by time in utero may be
counteracted.
In addition to improved neonatal outcome a further consideration
for using tocolysis may
be a monetary one. Prolongation of pregnancy by tocolysis may
not have shown a
reduction in NICU admissions but it may lead to a reduction in
number of days in NICU.
Cost of NICU services has not been directly assessed within
tocolytic trials, however, St
John et al have studied the cost of neonatal care according to
gestational age at birth and
survival. Accounting for number of survivors / non-survivors and
cost per survivor / non-
survivor, the mean cost of neonatal care at 24, 25 or 26 weeks
is 75 000 US dollars,
compared with 57 000 US dollars at 28 weeks, 38 000 US dollars
at 30 weeks, 21 000 US
dollars at 32 weeks and 8 000 US dollars at 34 weeks. 23 This
suggests that a prolongation
of pregnancy for one week may lead to considerable savings.
However, it should be
remembered that tocolytics do not reduce the number of
admissions to NICU or the
incidence of serious morbidity and therefore this apparent
saving may not exist.
10
-
7/29/2019 Tocolysis A clinically based review
11/29
-mimetics
-mimetics stimulate -2 adrenergic receptors in smooth muscle
and, via cAMP, reduce
sensitivity to and absolute levels of intracellular calcium
causing myometrial relaxation. -
mimetics have been the most commonly used tocolytic drugs within
the UK over recent
years. Meta-analysis of seven randomised trials of -mimetics has
shown them to be
significantly better at delaying delivery within 24 hours, 48
hours and seven days (but
bizarrely not 72 hours) than placebo or no drug. However, this
did not lead to any
improvement in preterm delivery rates before 30 weeks, 32 weeks
or 37 weeks or in
neonatal outcome in terms of perinatal death, incidence of RDS,
IVH, NEC or birthweight
-
7/29/2019 Tocolysis A clinically based review
12/29
increasing interest in the use of CCB for the treatment of
preterm labour as well as in
hypertension in pregnancy. Tsatsaris et al performed a
meta-analysis of nine randomised
controlled trials of 679 patients receiving -mimetics or
nifedipine and demonstrated that
nifedipine was better than -mimetics in delaying delivery for at
least 48 hours (OR 1.52
95% CI 1.03-2.24) or to gestations over 34 weeks (OR 1.87 95% CI
1.11-3.5). Although
there was no difference in neonatal mortality (OR 1.51 95% CI
0.63-3.65) nifedipine was
well tolerated compared to -mimetics with fewer discontinuations
due to side effects (OR
0.12 95% 0.05-0.29). There was a reduced incidence of RDS (OR
0.57 95% 0.37-0.97)
and admission to NICU (OR 0.65 95% CI 0.43-0.97). 25 Nifedipine
is therefore currently
the only tocolytic to be associated with a benefit for the
neonate.
Oxytocin receptor antagonists
Atosiban, a competitive oxytocin / vasopressin receptor
antagonist, has recently been
licensed for use as a tocolytic in Europe. The rationale for its
use is that oxytocin plays a
fundamental role in labour. Therefore inhibition of its
receptor, which leads to a reduction
in extracellular calcium influx as well as its release from
intracellular stores, should inhibit
myometrial contractility. However, there has been some doubt
over the role of oxytocin in
the initiation and maintenance of labour28.
Romero et al randomly assigned just over 500 women in preterm
labour to atosiban or
placebo with rescue therapy of standard tocolysis after one hour
if contractions continued.
19 There was no significant difference in the primary outcome,
which was time from start
of treatment to delivery or therapeutic failure, between
atosiban and placebo. There was
an increase in the number of patients remaining undelivered and
not requiring alternative
12
-
7/29/2019 Tocolysis A clinically based review
13/29
tocolytic therapy at 24 hours (73% vs 58%), 48 hours (67% vs
56%) and seven days
(62% vs 49%) for those receiving atosiban compared to placebo.
Infant mortality and
morbidity was similar between the two groups at 28 weeks but
were increased in the
atosiban group at
-
7/29/2019 Tocolysis A clinically based review
14/29
effect on contractility in several ways. In preparation for
labour they enhance the
development of gap junctions between myometrial cells to allow
coordinate uterine
activity and cause upregulation of oxytocin receptors.
Prostaglandins also have a direct
effect on calcium influx stimulating myometrial
contractility.
Indomethacin, a non-specific COX inhibitor, has been the most
commonly used NSAI
drug. It is more effective than placebo at delaying delivery for
48 hours and seven days
and unlike all other tocolytic drugs has been shown to cause a
reduction in deliveries
before 37 weeks gestation and the number of low birthweight
deliveries (
-
7/29/2019 Tocolysis A clinically based review
15/29
Magnesium Sulphate
Magnesium sulphate acts as a calcium antagonist at the
neuromuscular junction. It has
been used widely as an anticonvulsant agent in preeclamptic
women for many years and is
the most commonly used tocolytic drug in the USA. However,
meta-analysis has shown it
to be no better than placebo in delaying delivery 7 and the most
recent Cochrane Review
concludes there is insufficient evidence to support its use in
the treatment of preterm
labour. 39
Nitric Oxide (NO) Donors
NO donors act by increasing levels of cGMP in uterine smooth
muscle cells which leads to
uterine relaxation. There have been few studies of transdermal
nitroglycerin, but these
have suggested a reduction in deliveries within 48 hours
compared to placebo 40 and
similar efficacy to -mimetics with possibly fewer maternal side
effects. 41 However, there
is now increasing evidence that NO donors may be associated with
cervical ripening,
making them unsuitable as tocolytic agents. 42, 43
15
-
7/29/2019 Tocolysis A clinically based review
16/29
16
-
7/29/2019 Tocolysis A clinically based review
17/29
Conclusion
The rationale for treatment of preterm labour should be that it
improves neonatal outcome
without undue risk to the mother or fetus. Sadly current
management does not achieve
this. In simple terms all acute tocolytics appear to be little
better than placebo or no drug
and all are associated with almost no clinical benefit. This is
illustrated by inconsistencies
in the results of randomised controlled trials. For example,
nifedipine is more effective
than -mimetics, 25 which is better than placebo, 7 but similar
to magnesium sulphate, 27
which is no better than placebo. 7 Multiple comparisons between
studies of drug vs
drug, drug vs no drug and drug vs placebo make interpretation of
data hazardous
and unreliable.
It is reasonable and clinically justifiable not to use tocolytic
drugs. However, if tocolysis is
considered it should only be in selected situations where
benefit is more likely to be
achieved, for example for antenatal corticosteroid
administration and in-utero transfer.
The use of any tocolytic drug should be carefully considered in
terms of both potential
benefit and possible harm and fully discussed with the mother
before treatment is
instigated.
The choice of drug remains contentious. There is now sufficient
evidence to show that
both atosiban and nifedipine are preferable to -mimetics in
terms of side effect profile. It
maybe ethically difficult to justify high costs for a drug
treatment which has been shown to
make no improvement in outcome and is likely to be administered
to many patients who
would respond equally well to placebo. Therefore in our opinion,
nifedipine, which is
inexpensive and the only tocolytic shown to improve neonatal
morbidity, should be the
drug of choice if a tocolytic is to be used.
17
-
7/29/2019 Tocolysis A clinically based review
18/29
18
-
7/29/2019 Tocolysis A clinically based review
19/29
References
1. Lemons JA, Bauer CR, Oh W, Korones SB, Papile LA, Stoll BJ et
al. Very low
birthweight outcomes of the National Institute of Child Health
and Human
Development Neonatal Research Network, January 1995 through
December 1996.
Pediatrics 2001;107:(1)E1.
2. Draper ES, Manktelow B, Field DJ, James D. Prediction of
survival for preterm births
by weight and gestational age: retrospective population based
study. BMJ
1999;319:1093-1097.
3. Turnbull A. The Fetus and Birth. 1977. London: Elsevier
4. Skinner KA, Challis JR. Changes in the synthesis and
metabolism of prostaglandins by
human fetal membranes and decidua at labor. Am J Obstet Gynecol
1985;151:519-
523.
5. Kelly RW, Leask R, Calder AA. Choriodecidual production of
interleukin-8 and
mechanism of parturition. Lancet 1992;776-777.
6. Bennett P, Allport V, Loudon J, Elliott C. Prostaglandins,
the fetal membranes and the
cervix. The Endocrinology of parturition: basic science and
clinical application.
Frontiers of hormone research 2001;27:147-64.
7. Gyetvai K, Hannah ME, Hodnett ED, Ohlsson A. Tocolytics for
preterm labor: A
systematic review. Obstet Gynecol 1999;94:869-877.
8. Iams JD, Johnson FF, Sonek J, Sachs L, Gebauer C, Samuels P.
Cervical competence
as a continuum: A study of ultrasonographic length and obstetric
performance. Am J
Obstet Gynecol 1995;172:1097-1106.
19
-
7/29/2019 Tocolysis A clinically based review
20/29
9. Heath VCF, Southall TR, Souka AP, Elisseou A, Nicolaides KH.
Cervical length at 23
weeks of gestation: prediction of spontaneous preterm delivery.
Ultrasound Obstet
Gynecol 1998;1;312-317.
10. Goldenberg RL, Mercer BM, Meis PJ, Copper RL, Das A,
McNellis D. The preterm
prediction study: Fetal fibronectin testing and spontaneous
preterm birth Obstet
Gynecol 1996;87:643-648.
11. Finnstrm O, Otterblad Olausson P, Sedin G, Serenius F,
Svenningsen N, Thiringer K
et al. The Swedish national prospective study on extremely low
birthweight (ELBW)
infants. Incidence, mortality, morbidity and survival in
relation to level of care. Acta
Paediatr 1997;86:503-11.
12. Penney GC. Antenatal corticosteroids to prevent respiratory
distress syndrome.
RCOG Green Top guideline.
www.rcog.org.uk/guidelines/corticosteroids.
13. Report of the Consensus Development Conference on the Effect
for Fetal Maturation
on Perinatal outcomes. Bethesda, Maryland: National Institute of
Child Health and
Human Development. Report No.: NIH Publication no. 95-3784.
14. Crowley P. Prophylactic corticosteroids for preterm birth
(Cochrane Review). In: The
Cochrane Library, Issue 2, 2001. Oxford: Update Software.
15. Doyle LW. Changing outcome for infants of birthweight
500-999g born outside level
3 centers in Victoria. Aust NZ J Obstet Gynaecol
1997;37:253-257.
16. Towers CV, Bonebrake R, Padilla G, Rumney P. The effect of
transport on the rate of
severe intraventricular haemorrhage in very low birthweight
infants. Obstet Gynecol
2000;95:291-295.
20
-
7/29/2019 Tocolysis A clinically based review
21/29
17. Chien YL, Whyte R, Aziz K, Thiessen P, Matthew D, Lee SK.
Improved outcome of
preterm infants when delivered in tertiary care centers. Obstet
Gynecol 2001;98:247-
252.
18. Zuckerman H, Shalev E, Gilad G, Katzuni E. Further study of
the inhibition of
premature labor with indomethacin. Part II double blind study. J
Perinat Med
1984;12:25-29.
19. Romero R, Sibai BM, Sanchez-Ramos L, Valenzula GJ, Veille
JC, Tabor B. An
oxytocin receptor antagonist (atosiban) in the treatment of
preterm labor: A
randomized, double blind, placebo-controlled trial with
tocolytic rescue. Am J Obstet
Gynecol 2000;182:1173-1183.
20. The Canadian Preterm Labor Investigators Group. Treatment of
preterm labor with
the beta-adrenergic agonist ritodrine. New Engl J Med
1992;327:308-312.
21. Watts DH, Krohn MA, Hillier SL, Eschenbach DA. The
association of occult fluid
infection with gestational age and neonatal outcome among women
in preterm labour.
Obstet Gynecol 1992;79:351-357.
22. Salafia CM, Vogel CA, Vintzileos AM, Bantham KF, Pezzullo J,
Silbeman L.
Placental pathologic findings in preterm birth. Am J Obstet
Gynecol 1991;165:934-
938.
23. St John EB, Nelson KG, Cliver SP, Bishnoi RR, Goldenberg RL.
Cost of neonatal
care according to gestational age at birth and survival status.
Am J Obstet Gynecol
2000;182:170-175.
24. Higby K, Xenakis EMJ, Pauerstein CJ. Do tocolytics stop
preterm labor? A critical
and comprehensive review of efficacy and safety. Am J Obstet
Gynecol
1993;168:1247-1259.
21
-
7/29/2019 Tocolysis A clinically based review
22/29
25. Tsatsaris V, Papatsonis D, Goffinet F, Dekker G, Carbonne B.
Tocolysis with
nifedipine or beta-adrenergic agonists: A meta-analysis. Am J
Obstet Gynecol
2001;97:840-847.
26. The World Atosiban versus Beta-agonists Study Group.
Effectiveness and safety of
the oxytocin antagonist atosiban versus beta-adrenergic agonists
in the treatment of
preterm labour. BJOG 2001;108:133-142.
27. Larmon JE, Ross BS, May WL, Dickerson GA, Fischer RG,
Morrison JC. Oral
nicardipine versus intravenous magnesium sulphate for the
treatment of preterm labor.
Am J Obstet Gynecol 1999;181:1432-1437.
28. Thornton S, Vatish M, Slater D. Oxytocin antagonists:
clinical and scientific
considerations. Exp Physiol 2001;86.2:297-302.
29. British National Formulary 42. September 2001. Published by
British Medical
Association and the Royal Pharmaceutical Society of Great
Britain.
30. Vermillion ST, Scardo JA, Lashus AG, Wiles HB. The effect of
indomethacin
tocolysis on fetal ductus arteriosus constriction with advancing
gestational age. Am J
Obstet Gynecol 1997;177:256-61.
31. Kirshon B, Moise KJ, Mari G, Willis R. Long-term
indomethacin therapy decrease
fetal urine output and results in oligohydramnios. Am J
Perinatology 1991;8:86-88.
32. Norton ME, Merrill J, Cooper BAB, Kuller JA, Clyman RI.
Neonatal complications
after the administration of indomethacin for preterm labor. New
Engl J Med
1993;329:1602-1607.
33. Macones GA, Robinson CA. Is there justification for using
indomethacin in preterm
labor? An analysis of neonatal risks and benefits. Am J Obstet
Gynecol 1997;177:819-
824.
22
-
7/29/2019 Tocolysis A clinically based review
23/29
34. Macones GA, Marder SJ, Clothier B, Stamilio DM. The
controversy surrounding
indomethacin for tocolysis. Am J Obstet Gynecol
2001;184:264-272.
35. Slater DM, Berger LC, Newton R, Moore GE, Bennett PR.
Expression of cyclo-
oxygenase types 1 and 2 in human fetal membranes at term. Am J
Obstet Gynecol
1995;172:77-82.
36. Sawdy R, Slater D, Fisk N, Edmonds DK, Bennett P. Use of a
cyclo-oxygenase type-2
selective non-steroidal anti-inflammatory agent to prevent
preterm delivery. Lancet
1997;350:265-266.
37. Peruzzi L, Gianoglio B, Porcellini MG, Coppo R. Neonatal end
stage renal failure
associated with maternal ingestion of cyclo-oxygenase type-2
selective inhibitor
nimesulide as tocolytic. Lancet 1999;354:1615.
38. Groom K, Sawdy R, Elliott C, Shennan A, Bennett P.
Experience of the use of
Nimesulide, a COX-2 selective NSAI, in the prevention of preterm
delivery in high
risk cases. J Soc Gynecol Investig 2000;7:60-61A.
39. Crowther CA, Moore V. Magnesium for preventing preterm birth
after threatened
preterm labour (Cochrane Review). In: The Cochrane Library,
Issue 4, 2001: Update
Software.
40. Smith GN, Walker MC, Mc Grath MJ. Randomised, double blind,
placebo-controlled
pilot study assessing nitroglycerin as a tocolytic. Br J Obstet
Gynaecol 1999;106:736-
739.
41. Lees CC, Lojacono A, Thompson C, Danti L, Black RS, Tanzi P,
White IR, Campbell
S. Glyceryl trinitrate and ritodrine in tocolysis: An
international multicenter
randomized study. Obstet Gynecol 1999;94:403-408.
23
-
7/29/2019 Tocolysis A clinically based review
24/29
42. Thomson AJ, Burnett Lunan C, Cameron AD, Cameron IT, Greer
IA, Norman JE.
Nitric oxide donors induce cervical ripening of the human
uterine cervix: a randomised
controlled trial. Br J Obstet Gynaecol 1997;194:1054-1057.
43. Thomson AJ, Burnett Lunan C, Ledingham M, Howat RCL, Cameron
IT, Greer IA,
Norman JE. Randomised trial of nitric oxide donor versus
prostaglandin for cervical
ripening before first-trimester termination of pregnancy. Lancet
1998;352:1093-1096.
24
-
7/29/2019 Tocolysis A clinically based review
25/29
Tables and Figures Titles.
Table 1. Mechanisms of intracellular calcium control.
Table 2. Effect of tocolytics compared to placebo or no
tocolytic drug on
prolongation of pregnancy and neonatal outcome.
Figure 1. Control of Myometrial cell contractility and sites of
tocolytic drug activity.
Key:
OTR Oxytocin receptor OTRA - Oxytocin receptor antagonist
PGR Prostanoid receptor COXI Cyclo-oxygenase inhibitorSR
sarcoplasmic reticulum MgS Magnesium sulphate
V Voltage dependent Ca channel CCB Calcium channel blocker
R Receptor dependent Ca channel - -mimetcs-R - -adrenergic
receptor NO nitric oxide donors
Figure 2. Infant survival rates from 23 to 26 weeks
gestation.
25
-
7/29/2019 Tocolysis A clinically based review
26/29
Table 1. Mechanisms of intracellular calcium control.
Mechanism Effect onintracellular (Ca 2+)
Voltage dependent
calcium channels
Ca 2+ Membrane depolarisation caused byinherent membrane
instability and
increased number of gap junctions leads to
rapid influx of calcium
Receptor dependent
calcium channels
Ca 2+ Coupled to membrane bound G-proteinswhich are activated by
endocrine and
paracrine receptors such as oxytocin and
prostanoid receptor
Release from
sarcoplasmic
reticulum
Ca 2+ Oxytocin receptor linked to G-proteinsactivates
phosholipase C which increases
inositol triphosphate (IP3) levels and bind
to SR causing release of Ca 2+
-adrenoreceptors Ca 2+ Coupled to G-proteins cause increasedcAMP
levels which activates protein
kinase A, this inhibits phosphorylation of
CDMLK and increases SR uptake of Ca 2+
26
-
7/29/2019 Tocolysis A clinically based review
27/29
Table 2. Effect of tocolytics compared to placebo or no
tocolytic drug on prolongation
of pregnancy and neonatal outcome.
-mimetics Magnesiumsulphate
Indomethacin Atosiban
Del within 48hrs
OR (95% CI)
0.56 *
(0.42-0.74)
0.52
(0.26-1.05)
0.12 *
(0.05-0.32)
0.67*
(0.47-0.95)
Del within 7 days
OR (95% CI)
0.65*
(0.50-0.83)
1.54
(0.85-2.82)
0.07*
(0.02-0.27)
0.59*
(0.41-0.84)
Perinatal death
OR (95% CI)
1.08
(0.72-1.62)
1.83
(0.70-4.77)
1.48
(0.24-9.20
RDS
OR (95% CI)
0.76
(0.57-1.01)
1.19
(0.61-2.31)
0.61
(0.16-2.30)
7.66
(0.78-75.15)
IVH
OR (95% CI)
0.70
(0.43-1.15)
0.82
(0.25-2.63)
BW
-
7/29/2019 Tocolysis A clinically based review
28/29
Figure 1.
28
-
7/29/2019 Tocolysis A clinically based review
29/29
Figure 2. Infant survival rates from 23 to 26 weeks
gestation.
Finnstrm 1997.








![Clinically-indicated replacement versus routine ...eprints.qut.edu.au/26122/1/26122.pdf · [Intervention Review] Clinically-indicated replacement versus routine replacement of peripheral](https://img.pdfslide.us/doc/110x75/5ad0ea807f8b9ac1478e807a/clinically-indicated-replacement-versus-routine-intervention-review-clinically-indicated.jpg)