Embed Size (px)
Citation preview
4/2/2013
1
To Do or Not To Do? Crafting Drug Protocols for High‐Risk Therapies
Bryce A. Jackman, RPh, BCNSP, Director of Pharmacy, CareProHome Infusion
Steve M. Kennedy, PharmD, National Director, Infusion Pharmacy Services, Walgreens Infusion and Respiratory Services
Nita Meaux, RN, CRNI®, Heart Failure Program Director, Director of Risk Management, Walgreens Infusion and Respiratory Services
CE Credit in Four Easy Steps!1. Scan your badge as you enter each session.
2. Carry your Evaluation Packet to every session so you can add session evaluation forms to it.
3. Track your hours on the “Statement of Session Attendance Form” as you go.
4. At your last session, total the hours and sign both pages of your Statement of Session Attendance Form.
Keep the PINK copy for your records.
Put the YELLOW and WHITE copies in your Evaluation Packet.
o Make sure a completed Session Evaluation Form is in your Evaluation Packet for each session you attended.
o Miss one? Extras are in a file near Registration.
Complete the General Attendance Evaluation Form located in your Evaluation Packet.
Fill out the information on the outside of your Evaluation Packet envelope, seal it, and drop it in the box near Registration.
Applying for Pharmacy CPE? If you have not yet registered for an NABP e‐Profile ID, please visit www.MyCPEmonitor.net to do so before submitting your packet.
o You must enter your NABP e‐Profile ID in order to receive CE credit this year!
4/2/2013 2
Speaker Disclosures
The speakers declare no conflicts of interest or financial disclosures.
Clinical trials and off‐label/investigational uses will be discussed during this presentation in a fair and unbiased manner.
4/2/2013 3

4/2/2013
2
High Risk Therapies
• Chemotherapy
• Pain management
• Aminoglycosides
• Inotropes
• Drugs with a narrow therapeutic margin
• Drugs with black box warnings
• Drugs with increased potential for adverse reactions
4/2/2013 4
High Risk Situations
• Unusual combinations of drugs
• Multiple therapies/pumps
• Off label uses
• Epidural, intrathecal, intraventricularadministrations
• Aseptic compounding from non‐sterile ingredients
• Administration of vesicants
4/2/2013 5
High Risk Patient Populations• Pediatrics
• Geriatrics
• Pregnant or lactating patients
• Patients with multiple comorbidities
• Patients who are immune compromised
• Patients lacking appropriate caregiver support or home environment
• Language barriers
4/2/2013 6

4/2/2013
3
Assessing High Risk Referrals
• Multidisciplinary team• Research
– Package insert– Clinical trials– White papers– Case studies– Protocol developed by referral source
• Consider– Has patient been receiving therapy?– What is referral source’s experience with other patients?– What is the treatment goal ?
4/2/2013 7
Assessing High Risk Referrals
• What are the specific risks/challenges?• Is therapy appropriate for infusion center or home?• What steps can be implemented to mitigate risk?• Is a special consent needed?• Can a plan be developed that would be defensible under the challenge of “what would a reasonable and prudent clinician do in the same or similar circumstances”
• Final decision to accept or refuse referral must be a clinical rather than a financial decision
4/2/2013 8
Recommendations
• Consider high risk consent for certain therapies or patient types
• Thoroughly document all communications with physician, patient, and caregiver
• Obtain specific physician orders to cover unusual/high risk situations
4/2/2013 9
4/2/2013
4
Audience Participation Questions
4/2/2013 10
• Audience responds via one of three methods:
• Text – text message rates apply (free up to 20 cents)
• Tweet – carrier rate plan applies
• Web site URL – carrier rate plan applies
• Privacy
• Survey service cannot get your phone number
• You will not receive follow‐up messages or spam
Audience Practice Question
4/2/2013 11
4/2/2013 12
22333
165400
1. Standard texting rates only (worst case US $0.20)2. We have no access to your phone number3. Capitalization doesn’t matter, but spaces and spelling do
Vote via Texting
4/2/2013
5
Vote via PollEv.com
4/2/2013 13
165293
Capitalization doesn’t matter, but spaces and spelling do
Vote via Twitter
4/2/2013 14
@poll 165281
1. Capitalization doesn’t matter, but spaces and spelling do2. Since @poll is the first word, your followers will not receive this tweet
4/2/2013 15
4/2/2013
6
Audience Participation Question #1
Case Study: Continuous Lidocaine Infusion
• 42 year old male on heart transplant list
• Hospitalized for 4 months
• Physician , patient & family eager to allow patient time at home
4/2/2013 17
Lidocaine Case Study
• Considerations
– Why is therapy required?
– How long has patient been on therapy?
– Why can’t he be weaned?
– Does he have an implantable cardioverterdefibrillator (ICD)?
4/2/2013 18
4/2/2013
7
Lidocaine Case Study
• Plan– Discussed risks vs. benefits with physician
– Obtained agreement with our care plan and requirements
• Dose cannot be changed at home
• Physician to write order stating “infusion at home without cardiac monitor”
• Physician to document detailed discussion with patient/spouse re: risks vs. benefits and deviance from standard of care (cardiac monitoring)
4/2/2013 19
Lidocaine Case Study
• Our RN and pharmacist to each document separate conversations with patient & spouse re: risks vs. benefits, standard of care issues, care plan
• Document family agreement that patient would not be left alone at home
• Confirm availability of trained EMS
• Obtain high risk consent
• Initiate teaching in hospital
4/2/2013 20
Lidocaine Case Study
• Outcomes
– Patient discharged home on continuous IV lidocaine
– Remained home for 9 months
– Re‐hospitalized twice for dose titration
– Received transplant after 9 months
– Expired during immediate post‐op period
4/2/2013 21
4/2/2013
8
Audience Participation Question #2
Audience Participation Question #3
4/2/2013 23
Policy and Procedures
• Create a High Risk Referral Policy and Procedure for your organization. Include:
– The review process
– Type of situation requiring approval committee
– Actions to be taken
– Use of Clinical Consents
4/2/2013 24
4/2/2013
9
Purpose of a Drug Protocol
• To provide a clear, concise, and practical reference document for all clinicians
• To ensure a consistent patient care process is followed – Must allow for some patient specific variation
• To aid in employee education
• To aid in providing comfort to physicians, payer, or other healthcare provider that the process is safe
4/2/2013 25
Situations When a Drug Protocol May Be Needed
• New drug to the market
• New treatment request that is not clearly spelled out in the product insert
• When ever information needs to be available to multiple people for an extended period of time
• For on‐call or PRN staff
4/2/2013 26
Situation When a Multidisciplinary Patient Specific Care Plan is Sufficient
• High Risk situation that is unique to the patient
– Palliative Care
– Pediatrics
– Oncology
– Rare Drug
4/2/2013 27
4/2/2013
10
Care Plan Components
4/2/2013 28
• In addition to the components of your routine Care Plan, a high risk plan should address all concerns in detail
• Plan for the worst‐case scenarios
• Address each concern with an intervention
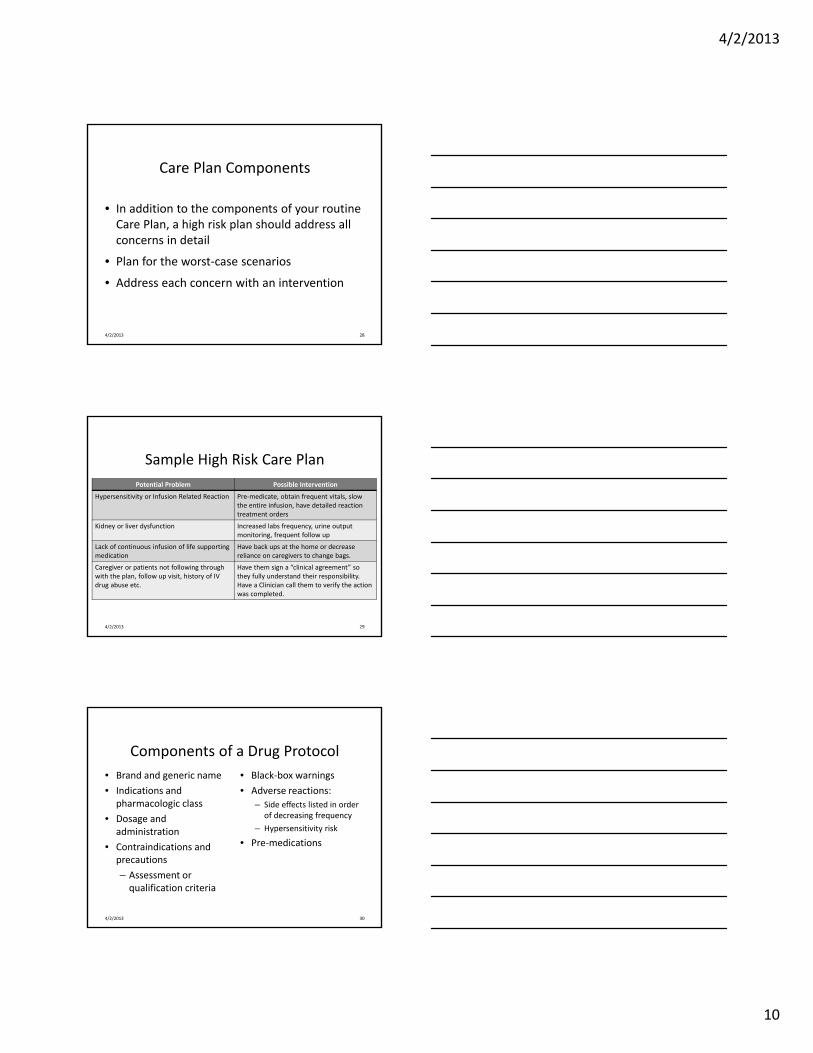
Sample High Risk Care Plan
Potential Problem Possible Intervention
Hypersensitivity or Infusion Related Reaction Pre‐medicate, obtain frequent vitals, slow the entire infusion, have detailed reaction treatment orders
Kidney or liver dysfunction Increased labs frequency, urine output monitoring, frequent follow up
Lack of continuous infusion of life supporting medication
Have back ups at the home or decrease reliance on caregivers to change bags.
Caregiver or patients not following through with the plan, follow up visit, history of IV drug abuse etc.
Have them sign a “clinical agreement” so they fully understand their responsibility.Have a Clinician call them to verify the action was completed.
4/2/2013 29
Components of a Drug Protocol
4/2/2013 30
• Brand and generic name
• Indications and pharmacologic class
• Dosage and administration
• Contraindications and precautions
– Assessment or qualification criteria
• Black‐box warnings
• Adverse reactions:
– Side effects listed in order of decreasing frequency
– Hypersensitivity risk
• Pre‐medications
4/2/2013
11
Components of a Drug Protocol
4/2/2013 31
• Monitoring parameters
• Patient education
• Nursing considerations
• Site of care
considerations —Home vs. ATS
• How supplied
• Resources for more information
• Manufacturer Medical Affairs phone number
• References
Samples
Formats:
• Word documents
• Flow charts
4/2/2013 32
Audience Participation Question #4
4/2/2013 33
4/2/2013
12
4/2/2013 34
Audience Participation Question #5
Benlysta (belimumab)
4/2/2013Source: Benllysta Package Insert 2011
35
• Indication: Treatment of adult patients with systemic lupus
• Dosage: Infuse 10 mg/kg over 1 hour every 2 weeks x 3, then every 4 weeks
• Class: Monoclonal Antibody, approved 2011
Benlysta (belimumab)• Warnings:
– Serious hypersensitivity reactions including anaphylaxis (with fatalities; onset may be delayed)
– Hypersensitivity reactions occurring on the same day of infusion were reported in 13% (191/1458) of patients receiving BENLYSTA and 11% (76/675) of patients receiving placebo.
– Anaphylaxis was observed in 0.6% (9/1458) of patients receiving BENLYSTA and 0.4% (3/675) of patients receiving placebo.
• Administration Instructions: – Should be administered by healthcare provider prepared to manage anaphylaxis
– Consider administering pre‐medications
4/2/2013Source: Benlysta Package Insert 2011
36
4/2/2013
13
Benlysta Initial Assessment
• New drug and patient population
• Reaction rates high but types are manageable
• Reaction rates are fairly similar to the placebo
• No requirements of administration in a healthcare facility
• We administer other monoclonal antibodies in the home.
4/2/2013 37
Our Organization’s Benlysta Plan • Developed a Drug Protocol with restrictions
– Administer on case‐by‐case basis as pilot with Clinical Team review of every patient
– Education of each Nurse on reactions and treatment plan
• Review cases at 6 and 12 months • Experience:
– 54 patients have been treated in the 12 month span – 18 different offices and 618 dispenses– Roughly 50% in home and 50% in ATS– Two hypersensitivity reactions were noted
• Skin rash/hives and scratchy feeling in throat• All symptoms were relieved in the home or ATS
4/2/2013
Merrill, J T at. El. Long‐Term Safety Profile of Belimumab Plus Standard Therapy in Patients With Systemic Lupus Erythematosus. Arthritis and Rheumatism Vol.64,No.10 October 2012, pp 3364‐3373 38
Benlysta Plan, Continued
4/2/2013 39
• Literature Data: – Long‐term safety profile of Belimumab study published October 2012
– Followed patients for 4 years of treatment: • Only 2 severe infusion reactions, one vertigo and the other had dyspnea, N/V, swelling of mouth, chest tightness and difficulty breathing
• All resolved on day of occurrence
– Conclusion: Belimumab was safe and generally well‐tolerated over 4 years of treatment in combination with standard therapy for SLE
• In the Fall of 2012 we modified our protocol to allow unrestricted home or ATS infusions

4/2/2013
14
Can We Give CyclodextrinIn the Home?
4/2/2013 40
• Received call from a parent inquiring about the possibility of investigational cyclodextrin infusions for her 6 year old twins who were diagnosed with Niemann‐Pick Disease Type C1 (NPC)
• After three years of being in a hospital setting, would like to move to home IV infusions
• Current infusions are once weekly for 8 hours
Cyclodextrin in the home cont’d
4/2/2013 41
• Cyclodextrin is only available as an endotoxin‐controlled powder
• We were told:– “People have followed the exact instruction from this protocol and made the solutions in Japan, Brazil, and Spain. There have not been any issues to date.”
• The therapy has been well‐tolerated to date
• More information can be found on the patient’s website
Actions Taken
• Researched Neimann Pick
• Researched Cyclodextrin
• Reviewed hospital protocol
• Reviewed the patient’s website
• Conducted a complete literature search
4/2/2013 42
4/2/2013
15
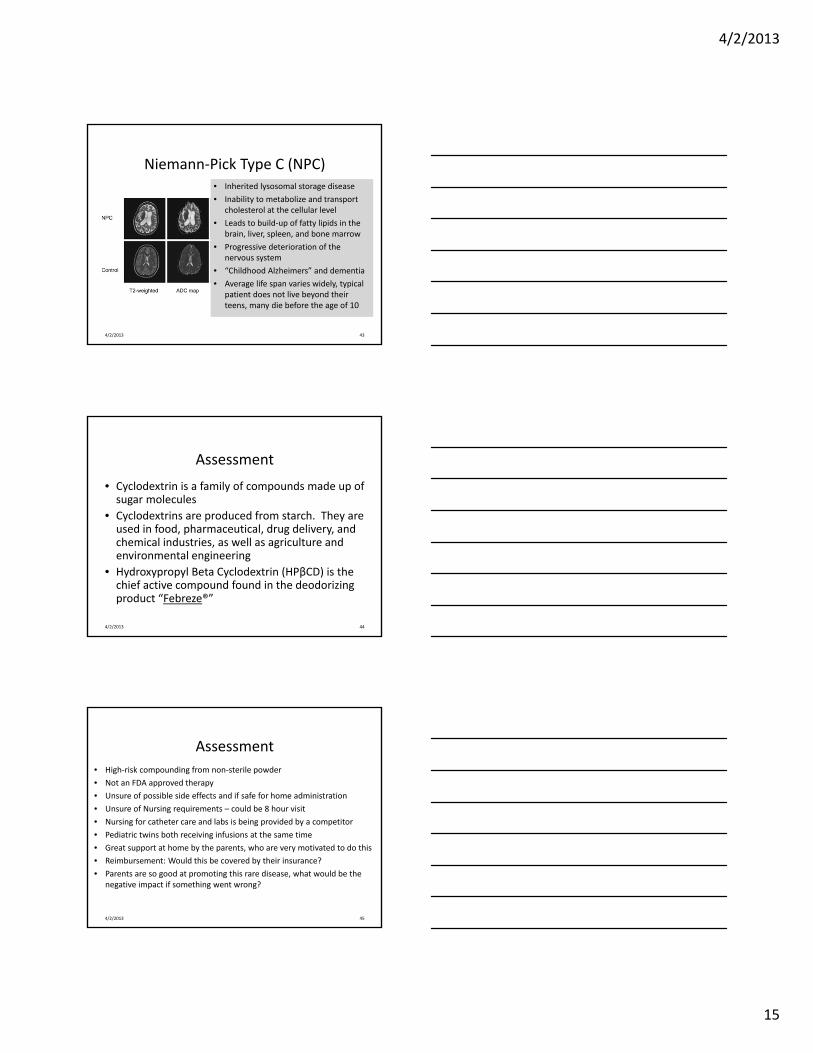
Niemann‐Pick Type C (NPC)
4/2/2013 43
• Inherited lysosomal storage disease
• Inability to metabolize and transport cholesterol at the cellular level
• Leads to build‐up of fatty lipids in the brain, liver, spleen, and bone marrow
• Progressive deterioration of the nervous system
• “Childhood Alzheimers” and dementia
• Average life span varies widely, typical patient does not live beyond their teens, many die before the age of 10
Assessment
4/2/2013 44
• Cyclodextrin is a family of compounds made up of sugar molecules
• Cyclodextrins are produced from starch. They are used in food, pharmaceutical, drug delivery, and chemical industries, as well as agriculture and environmental engineering
• Hydroxypropyl Beta Cyclodextrin (HPβCD) is the chief active compound found in the deodorizing product “Febreze®”
Assessment
• High‐risk compounding from non‐sterile powder
• Not an FDA approved therapy
• Unsure of possible side effects and if safe for home administration
• Unsure of Nursing requirements – could be 8 hour visit
• Nursing for catheter care and labs is being provided by a competitor
• Pediatric twins both receiving infusions at the same time
• Great support at home by the parents, who are very motivated to do this
• Reimbursement: Would this be covered by their insurance?
• Parents are so good at promoting this rare disease, what would be the negative impact if something went wrong?
4/2/2013 45
4/2/2013
16
Actions: Step 1• Internal conference call with 4 pharmacists and 2 nurses to review
findings• Findings:
– An IND for compassionate use with the FDA is present including consents, etc.
• This allowed us to reference our Investigational drug policy
– The drug is structurally related to natural products – no infusion reactions or side effects were noted
• Plenty of information available on the product
– Patients have implanted ports for the infusions– Hospital protocol was very detailed– Physician and hospital willing to do anything we need to make us
comfortable– Family will pay for all services
4/2/2013 46
Actions: Step‐2
• Case conference with the physician, hospital nurse, hospital pharmacist, competition’s nurse, and our clinicians
• Care Plan included:– Providing the drug, pump, and supplies to be infused in the MD office, with the nurse who will administer in the home present for the infusion
– Based on pilot success, the next weekly infusion will be done in the home
– MD protocols were revised to allow home administration
4/2/2013 47
Outcome• Patients have received 51 infusions with no problems
• Parents are extremely relieved to avoid a weekly 8 hour hospital or clinic visit with two small children
• Parents continuously praise our clinicians• Parents promote us on their website and to the rare disease foundations they are involved in
• The mother gave myself and our Executive Vice President a huge hug when we met for the first time at a rare disease foundation meeting
4/2/2013 48
4/2/2013
17
4/2/2013 49
http://addiandcassi.com/
Patient information shared on request of the parents.
ACHC requirements
• DRX5‐2B: Written Policies & Procedures describe the process for the development of the Plan of Care to meet the client/patient needs.
• DRX4‐7A: All Personnel receive training and/or education and competently perform the required client/ patient care/ service activities prior to being assigned to work independently.
4/2/2013 50
ACHC Requirements
• DRX4‐15A: The organization’s personnel have access to a reference library and/or internet access appropriate to the level of services provided.
4/2/2013 51

4/2/2013
18
Patient Case: Withdrawal of Life‐Sustaining Therapy
• 13 yo male w/ hx of rhabdomyosarcoma stage IV, Group IV rhabdomyosarcoma of abdomen.
• Initial diagnosis 11/2003
• Chemotherapy and radiation completed 8/2004
• Reoccurrence and repeat surgery 6/2005
• Chemotherapy completed 2/14/06
4/2/2013 52
• Total anthracycline dose 300 mg/m2 (doxorubicin) between two treatment cycles
• Off therapy evaluation in 3/2006 showed decreased shortening fraction 15% and ejection fraction 41% (8/05 SF=34% & EF=57%)
• Referral to Pediatric Cardiology for treatment and follow‐up.
4/2/2013 53
Patient Case: Withdrawal of Life‐Sustaining Therapy
• Osteosarcoma diagnosis 2/23/2011 (secondary malignancy) from pelvic radiation therapy
• Treatment initiated with cisplatin, ifosfamide and methotrexate
• Therapy was stopped 5/6/2011 because of worsening cardiac function, renal function
• Pt. having symptoms of fluid over load, creatinineof 2
• Pt. in PICU until discharge 5/24/11
4/2/2013 54
Patient Case: Withdrawal of Life‐Sustaining Therapy
4/2/2013
19
• Hospice referral 5/24/2011
• Milrinone 0.75 mcg/kg/min based on 52.8kg
• Dobutamine 5 mcg/kg/min based on 52.8kg
• Epinephrine 0.025mcg/kg/min based on 52.8kg
• Goal: titrate therapies down over several days so he can “die at home with my cats”
• Expired 5/26/11
4/2/2013 55
Patient Case: Withdrawal of Life‐Sustaining Therapy
Plan of Care
• Meeting with Hospice RN to review milrinone, dobutamine and epinephrine monitoring parameters
• HR, BP, weight, abdominal girth, respiratory rate, irregular heart beat
4/2/2013 56
Plan of Care
• Cardiac Nurse makes joint visit at hospital to start patient on 3 infusion pumps for milrinone, dobutamine and epinephrine infusions
• 2 back up pumps provided (milrinone and dobutamine both at same rate)
• Request call to pharmacist from Hospice RN once patient is at home
• Follow up next day by pharmacist to make sure no problems or issues with infusion pumps
4/2/2013 57
4/2/2013
20
Patient Case Course: Withdrawal of Life‐Sustaining Therapy
• 5/24/11– Patient admitted to service with joint visit – RN/Hospice RN conference with pharmacist at time of arrival home
• 5/25/11– Coordination of care call made, plan to remove epinephrine infusion this day
• 5/26/11 – Patient expired
4/2/2013 58
Patient Case: Complex End‐of‐Life Care
• 19 yo female with h/o metastatic osteosarcoma with lesions in lung, right occipital region of brain and left scapula
• Diagnosed with osteosarcoma in 2004– Several resections including above‐the‐knee amputation
– Chemotherapy, including doxorubicin
• Metastatic lesions identified 9/2012
4/2/2013 59
Patient Case: Complex End‐of‐Life Care
• Patient admit to hospital with altered mental status (AMS) on 3/11/13
• Diagnosis: disease progression secondary to increased size of metastatic lesions
• Pt./family chose to proceed with comfort measures, palliative/hospice care
4/2/2013 60
4/2/2013
21
Patient Case: Complex End‐of‐Life Care
• Discharge to home on 3/13/13 with implanted port for IV access
• Morphine 15mg‐25mg/hr basal rate with 3mg every 20 minute bolus as needed for breakthrough
• Lorazepam 1mg IV push q1hr as needed
• Dexamethasone 4mg IV push q 12 hr
• Levetiracetam 500mg IV q 12 hr over 20 min.
• Glycopyrrolate 0.3mg IV q 4hr prn↑ respiratory secretions
4/2/2013 61
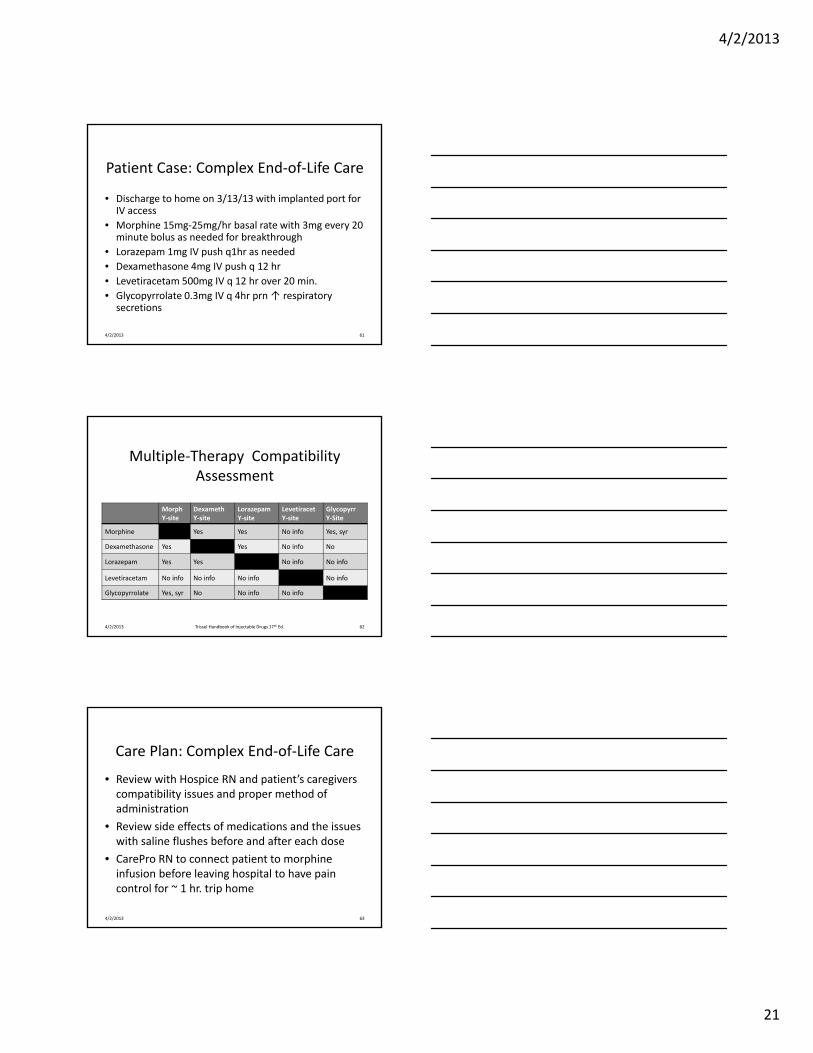
Multiple‐Therapy Compatibility Assessment
Morph Y‐site
DexamethY‐site
LorazepamY‐site
LevetiracetY‐site
GlycopyrrY‐Site
Morphine Yes Yes No info Yes, syr
Dexamethasone Yes Yes No info No
Lorazepam Yes Yes No info No info
Levetiracetam No info No info No info No info
Glycopyrrolate Yes, syr No No info No info
4/2/2013 Trissel Handbook of Injectable Drugs 17th Ed. 62
Care Plan: Complex End‐of‐Life Care
• Review with Hospice RN and patient’s caregivers compatibility issues and proper method of administration
• Review side effects of medications and the issues with saline flushes before and after each dose
• CarePro RN to connect patient to morphine infusion before leaving hospital to have pain control for ~ 1 hr. trip home
4/2/2013 63
4/2/2013
22
Patient Course: Complex End‐of‐Life Care
• Several rate increases for morphine to max of 19mg/hr through weekend
• Seizures controlled through use of levetiracetam and lorazepam
• Patient passed away comfortably on 3/19/13
4/2/2013 64
Audience Participation Question #6
4/2/2013 65
Audience Participation Question #2
4/2/2013
23
Summary• Each company should have a High Risk Policy to guide clinical decisions in unique or high risk situations
• An interdisciplinary team is needed to ensure consideration of all aspects of patient safety
• The team should determine if the situation requires a drug protocol or if a detailed care plan will suffice
• The plan for safety should be well understood by clinicians, referral source and patient
4/2/2013 67





























