Embed Size (px)
Citation preview

To Cover or Not To Cover? - Medication Coverage Guidelines with a dash of PEPPER
Dr. Sherita D. Castille, Pharm DClinical Pharmacist Partner

2
Objectives
Review defining key Medicare terms
Gain a better understanding medication coverage requirements
See how comprehensive relativeness and medication coverage
rationale aides ease of addendum documentation
See how this collectively effects PEPPER reports

3
Please Note
• Sherita Castille has no financial conflicts to disclose
• The views, information, and guidance in this webinar are those of the presenter
• The information may be incomplete and HPS does not make any guarantees or warranties concerning the information contained in this resource
• If expert assistance is required, please seek the services of CMS

4
Everyday hospice providers must determine which medications should or should not be covered for their patients. With increasing reports of misuse of federal funds and the ever-changing guidelines, it can be difficult to navigate and remain compliant. According to the National Hospice and Palliative Care Organization (NHPCO), hospice is expected to evaluate each medication in relation to the terminal diagnosis & prognosis and cover all medications that manage or palliate the principal hospice diagnosis. We will look at the various pathways to determine medication coverage and how your clinical team can be an effective tool in managing cost.
To Cover or Not To Cover?A review of medication coverage guidelines
5
Medicare Terms & ConceptsCenters for Medicare
&Medicaid Services
6
Key Medicare Concepts
• According to the Medicare Hospice Conditions of Participation (CoPs), the hospice is expected to pay for all medications “related to the palliation and management of the terminal illness and related conditions, as identified in the hospice plan of care.”
• The initial assessment is to determine the patient's immediate care needs. Hospices must complete this abbreviated assessment in 48 hours. The comprehensive assessment must assess in-depth all the patient's areas of need and will ensure that hospices are fully aware of the patient's current status. Hospices will be able to use these assessments to establish an individualized hospice plan of care.
• IDG team develops a plan that meets the patient’s individual needs for pain management and symptom control. As reminder, palliative medications are those which manage symptoms, improve quality of life, or prevent complications, without curative intent.

11
Pain Pain medications should be covered unless the pain is clearly not related to the hospice diagnosis or end of life. Covered pain medications would include analgesics such as APAP, NSAIDs, and opioids in addition to adjuvant analgesics (e.g., steroids or muscle relaxants).
Nausea and VomitingMedications treating nausea/vomiting (N/V) should be covered, whether the N/V is related to the terminal condition or end of life, or whether it is a side effect of other palliative medications, such as opioids.
AnxietyMedications used to treat anxiety should be covered unless the patient has a long-standing history of anxiety disorder that preceded the terminal illness and that is clearly unrelated to the hospice diagnosis or end of life.
ConstipationConstipation is not only common symptom of terminal illness but is also a side effect of many different classes of palliativemedications. Therefore, medications used to treat any type of bowel issue should be covered, regardless of hospice diagnosis
Mandatory Symptom CoverageOIG and CMS Guidelines

12
Key CMS TermsTerminal Hospice Diagnosis
Primary Code (ICD- 10) indicating patient’s diagnosis at admission that names the health problem of the patient
Advanced Beneficiary Notice (ABN)A notice that a doctor or supplier should give a Medicare beneficiary when furnishing an item or service for which Medicare is expected to deny payment.
Related Conditions Any conditions that are related to or caused by either the diagnosis/prognosis or the medications used to manage either
Terminal Prognosis The prognosis of an individual is where the life expectancy is 6 months or less if the
illness runs its normal course
Centers for Medicare and
Medicare Services

13
Hospice FormularyUtilizing Clinical Tools
14
Seeing the Big Picture
• Pain and palliative symptom management issues• General drug information guidance: availability, costs, cost-
effective alternatives, adverse effects, etc.
CMS
HPS
• Providing consistent regulatory guidance for cost containment
• Increase coverage transparency and quality of hospice providers
HOSPICE
• Providing patient - centered, cost effective care utilizing an interdisciplinarian team approach
• Balancing hospice services versus palliative services
15
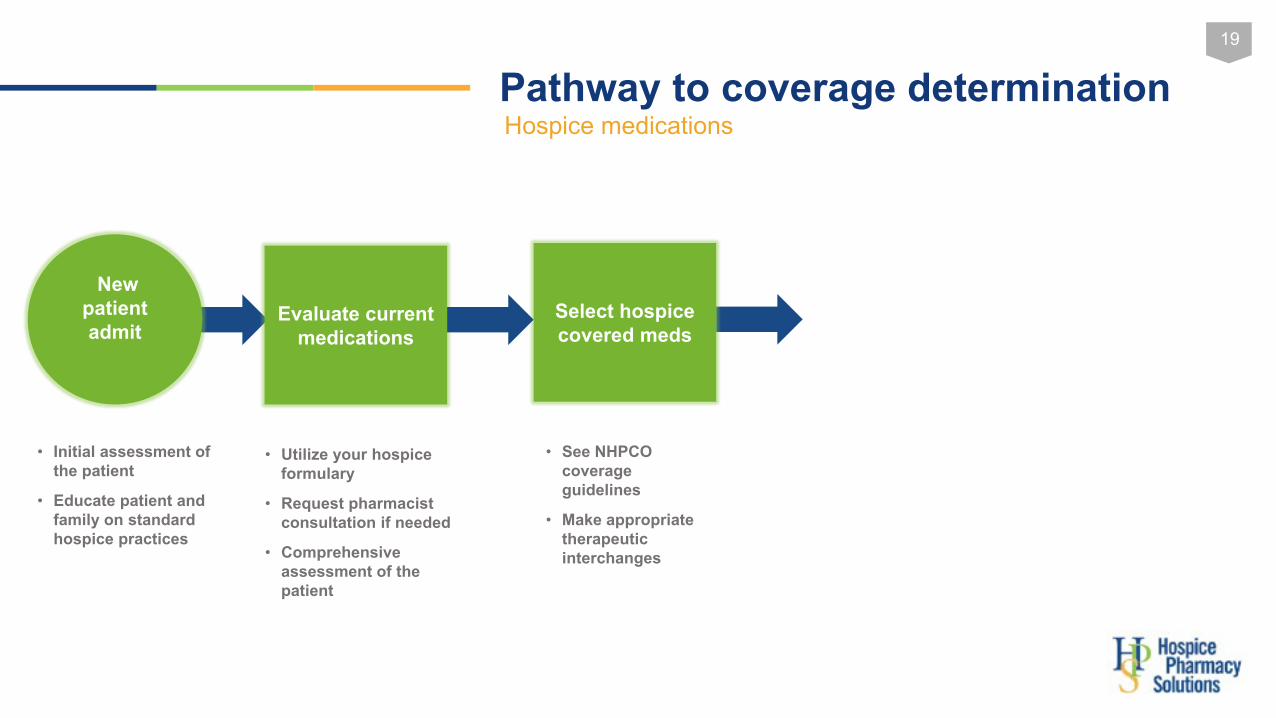
Pathway to coverage determinationHospice medications
New patient admit
• Initial assessment of the patient
• Educate patient and family on standard hospice practices

16
Centers for Medicare&Medicaid Services

17
Pathway to coverage determinationHospice medications
Evaluate current medications
New patient admit
• Initial assessment of the patient
• Educate patient and family on standard hospice practices

18
Coverage Determination How your formulary can be a resource
Commonly covered meds Diagnosis
ACE inhibitors, ARBs, Beta-blockers, Diuretics CHF/Heart Failure
Anti-Parkinson agents and Anticholinergics Parkinson's Disease
Antipsychotics and Anticonvulsants Psychosis/Dementia
Bronchodilators, corticosteroids, expectorants, antitussives and mucolytics
Lung Cancer/Pulmonary
19
Pathway to coverage determinationHospice medications
Evaluate current medications
New patient admit
Select hospice covered meds
• Utilize your hospice formulary
• Request pharmacist consultation if needed
• Comprehensive assessment of the patient
• See NHPCO coverage guidelines
• Make appropriate therapeutic interchanges
• Initial assessment of the patient
• Educate patient and family on standard hospice practices

20
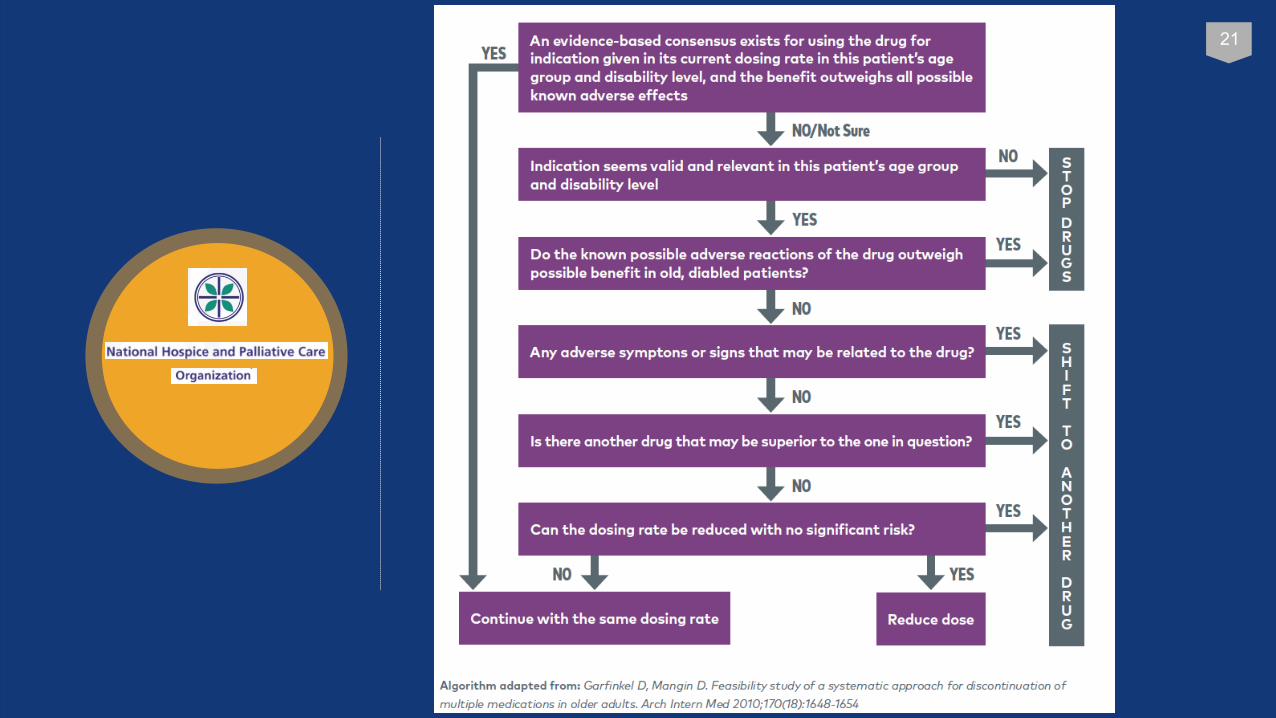
NHPCO - Medication Flow Chart
No
Yes
21

22
Non- Palliative Medications There is a place for deprescribing in hospice
Risk for bleedingMedication no
longer indicatedDrug-drug
interactions Decreased renal /hepatic function
Disease, med & diet changes
Asymptomatic hyperglycemia Not monitoring
frequently to use insulin safely
Drug-drug interactions Inconsistent adherence Dysphagia FAST score
Risk outweighs benefit
Improve QOL Reduce pill burdenOutside goals of
care
Hyperlipidemia Treatment
Cognitive Enhancing
Agents
Diabetes Medications
Anticoagulants
23
Addendum to the EOB

24
Centers for Medicare&Medicaid Services

25
Addendum to the EOB

26
NHPCO - Medication Flow Chart
No
Yes
27
Addendum Updates
CMS 2022 proposed rule will allow Hospice to furnish the addendum within 5 days from the date of a beneficiary or representative requests , if the request is within 5 days from the date of a Hospice election
For example, if the patient elects Hospice on June 1st and request the addendum on June 3rd , the Hospice would have until June 8th to furnish the addendum.
If the addendum is requested as care is proceeding, the addendum must be provided within three days. This was changed from the 2021 hospice proposed rule of 72 hours.
Centers for Medicare&Medicaid Services

28
2022 Proposed Rule Updates - Refusal to Sign
“If a patient or representative refuses to sign the addendum, the Hospice must document clearly in the medical record (and on the addendum itself ) the reason the addendum is not signed in order to mitigate a claim denial for this condition for payment. In such a case, although the beneficiary has refused to sign the addendum, the ‘date furnished’ must still be within the required timeframe (that is, within three or five days of the beneficiary or representative requests, depending on when such a request was made), and noted in the chart an on the addendum itself .”
CMS is “proposing to clarify in regulation that if a non-Hospice provider requests the addendum, rather than the beneficiary or representative, the non-Hospice provider is not required to sign the addendum.”
Centers for Medicare&Medicaid Services

30
Pathway to coverage determinationHospice medications
Evaluate current medications
New patient admit
Select hospice covered meds
• Utilize your hospice formulary
• Request pharmacist consultation if needed
• Comprehensive assessment of the patient
Request ABN on qualifying meds
• See NHPCO coverage guidelines
• Make appropriate therapeutic interchanges
• Initial and comprehensive assessment of the patient
• Educate patient and family on standard hospice practices

31
Pathway to coverage determinationHospice medications
Evaluate current medications
Medication profile
finalized
New patient admit
Select hospice covered meds
• Required when payment approved outside of hospice standards
• Know when ABN are not required
Request ABN* on qualifying
meds
• See NHPCO coverage guidelines
• Make appropriate therapeutic interchanges
• Initial and comprehensive assessment of the patient
• Educate patient and family on standard hospice practices
• Utilize your hospice formulary
• Request pharmacist consultation if needed
• Comprehensive assessment of the patient

32
PEPPER Overview

33
Don’t Forget to add PEPPERProgram for Evaluating Payment Patterns Electronic Report
Why is CMS providing PEPPERs?
• A data report to help hospice identity “target areas” where there is risk for improper Medicare Payment
• The report shows how a hospice’s data compares to national, jurisdiction and state statistics.
• PEPPER does not identify the presence of improper payments, but it can be used as a guide for auditing and monitoring efforts.
What is PEPPER?
• To protect the Medicare trust fund from fraud, waste and abuse
• Supports CMS’ program integrity• It is an educational tool intended
to help providers access their risk for improper Medicare payments

34
Don’t Forget to add PEPPERProgram for Evaluating Payment Patterns Electronic Report
Haven’t accessed your PEPPER yet? Review the Secure PEPPER Access Guide (PDF) and then visit the PEPPER Resources Portal to access your PEPPER.

35
Don’t Forget to add PEPPERProgram for Evaluating Payment Patterns Electronic Report
36
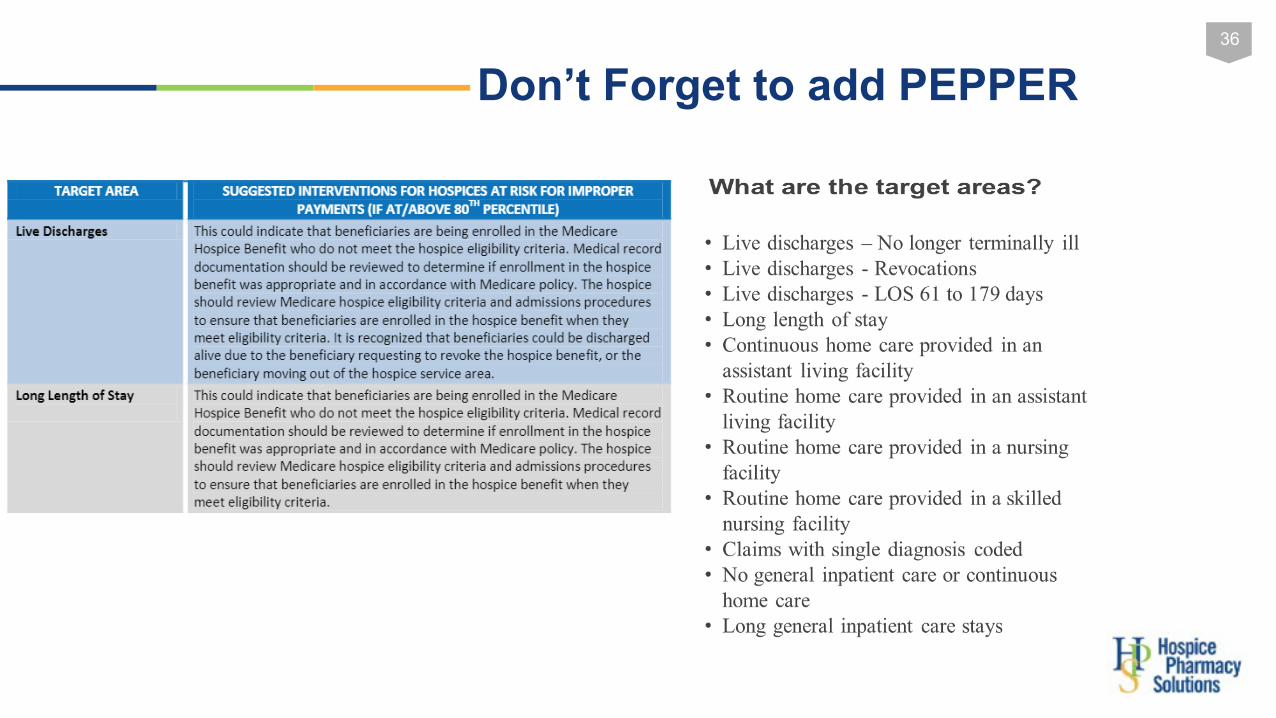
Don’t Forget to add PEPPER
37
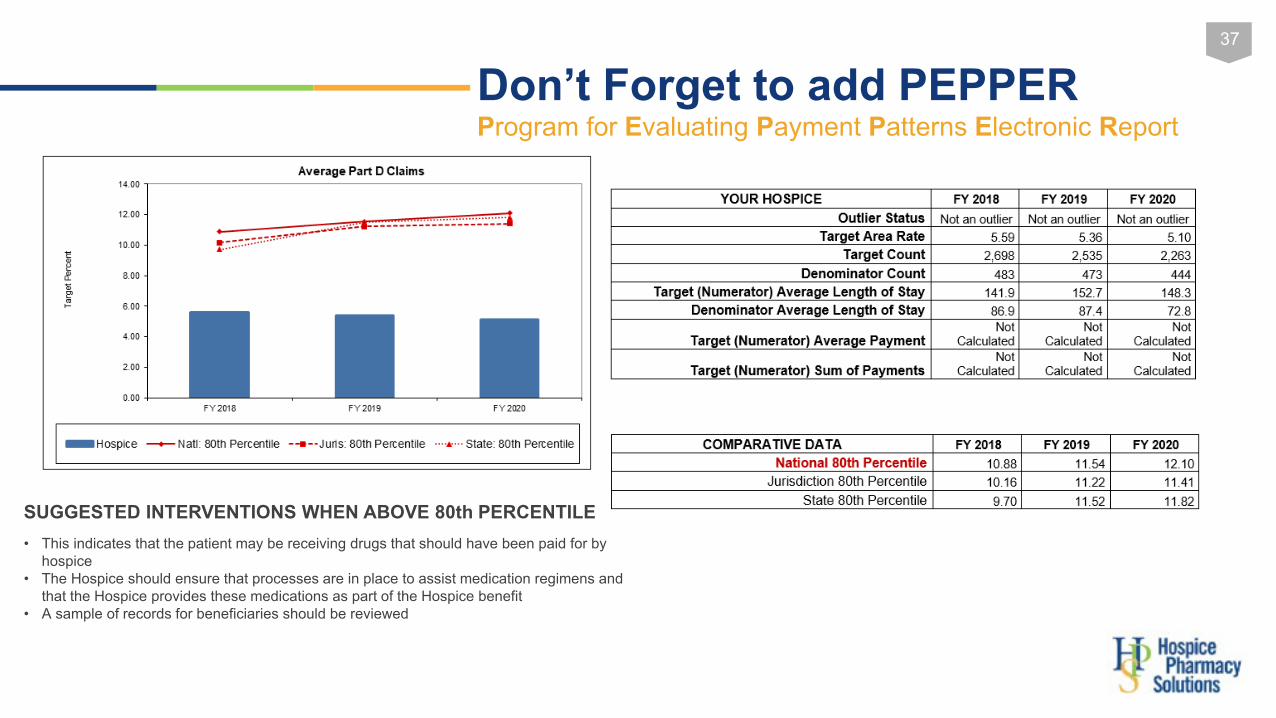
Don’t Forget to add PEPPERProgram for Evaluating Payment Patterns Electronic Report
SUGGESTED INTERVENTIONS WHEN ABOVE 80th PERCENTILE• This indicates that the patient may be receiving drugs that should have been paid for by
hospice• The Hospice should ensure that processes are in place to assist medication regimens and
that the Hospice provides these medications as part of the Hospice benefit • A sample of records for beneficiaries should be reviewed

38
Don’t Forget to add PEPPERProgram for Evaluating Payment Patterns Electronic Report
Strategies to Consider • Do not panic!
o Outlier status does not necessarily mean that compliance issues exist.
• If you are an “outlier, ” determine why that may be. o Do the statistics reflect your operation? Patient population? Referral
sources? Health care environment? o Verify by sampling claims and reviewing documentation in medical
record. Determine if coded and billed appropriately based upon documentation in the medical record?
• Ensure you are following best practices, even if you are not an outlier.

40
Thank you!Questions?
41
References
https://www.federalregister.gov/documents/2008/06/05/08-1305/medicare-and-medicaid-programs hospice-conditions-of-participation
https://www.cms.gov/apps/glossary/default.asp?Letter=C&Language=English
https://www.oig.hhs.gov/oei/reports/oei-02-06-00221.pdf
https://www.cms.gov/Regulations-and-Guidance/Legislation/CFCsAndCoPs/Hospice.html
https://www.nhpco.org/
https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Medicare-Provider-Charge-Data/PAC_Hospice
https://feepmdlmhplaojabeoecaobfmibooaid/https://www.nhpco.org/wp-content/uploads/NHPCO-Facts-Figures-2020-edition.pdf
1. Holmes HM, Min L, Yee M, et al. Rationalizing prescribing for older patients with multimorbidity: considering time to benefit. Drugs Aging 2013;30(9):655-666. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3755031/ Accessed August 20, 2020.
42
References2. Pisters R, Lane DA, Nieuwlaat R, et al. A novel use r-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest. 2010;138(5):1093-100.





























