Embed Size (px)
Citation preview
TM
TM
Centers for Disease Control and Prevention
National Center on Birth Defectsand Developmental Disabilities
Division of Human Development and Disability
Centers for Disease Control and Prevention
National Center on Birth Defectsand Developmental Disabilities
Division of Human Development and Disability
Military Audiology AssociationFebruary 13, 2006
Military Audiology AssociationFebruary 13, 2006
John Eichwald, Team LeadJohn Eichwald, Team Lead
TM
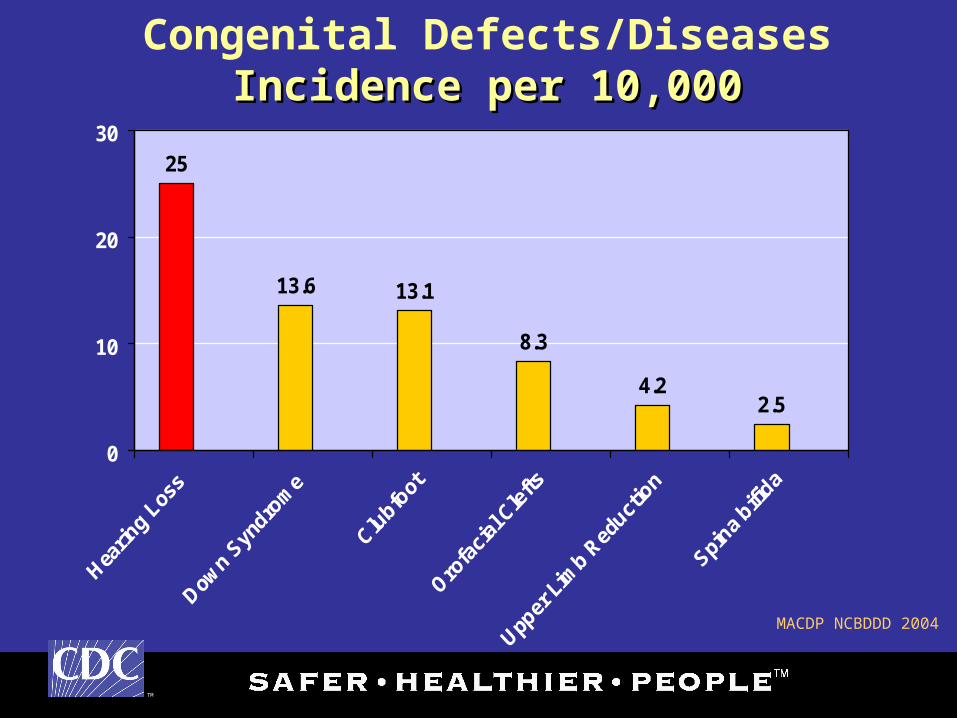
Congenital Defects/DiseasesIncidence per 10,000Incidence per 10,000
25
13.6 13.1
8.3
4.22.5
0
10
20
30
MACDP NCBDDD 2004
TM
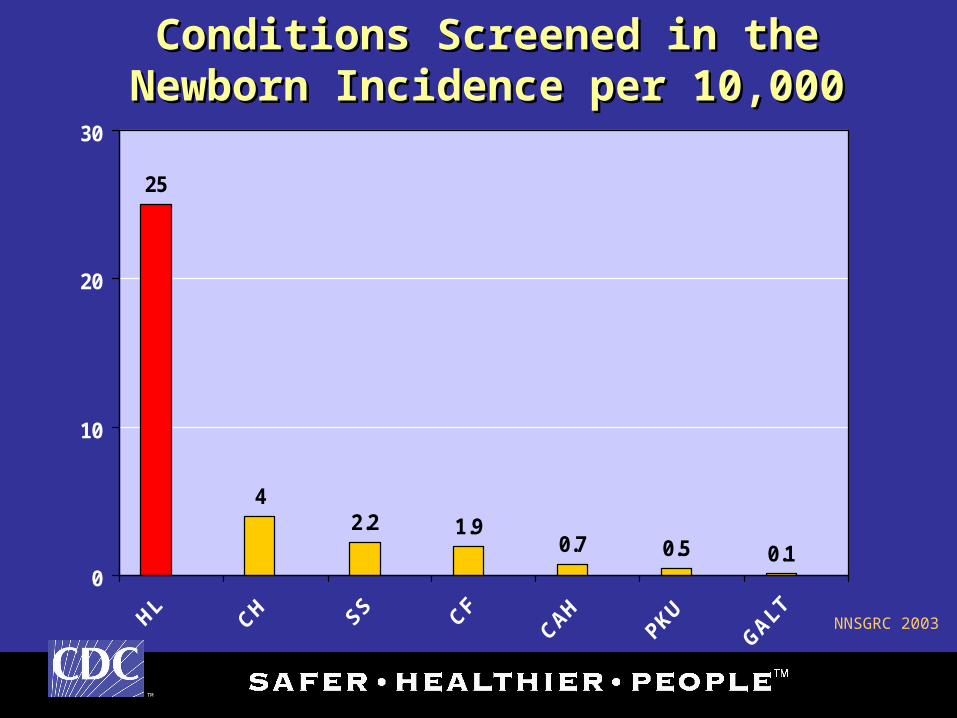
Conditions Screened in the Newborn Conditions Screened in the Newborn Incidence per 10,000Incidence per 10,000
25
42.2 1.9
0.7 0.5 0.10
10
20
30
NNSGRC 2003
TM
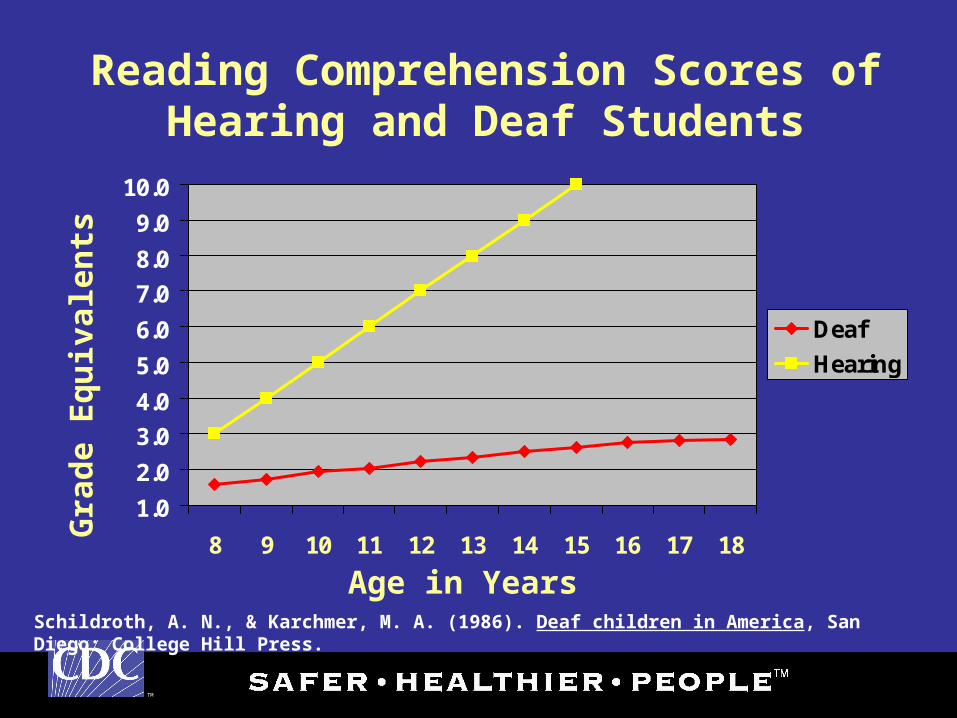
Reading Comprehension Scores of Hearing and Deaf Students
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
9.0
10.0
8 9 10 11 12 13 14 15 16 17 18
Deaf
Hearing
Age in YearsSchildroth, A. N., & Karchmer, M. A. (1986). Deaf children in America, San Diego: College Hill Press.
Gra
de
Eq
uiv
alen
ts
TM
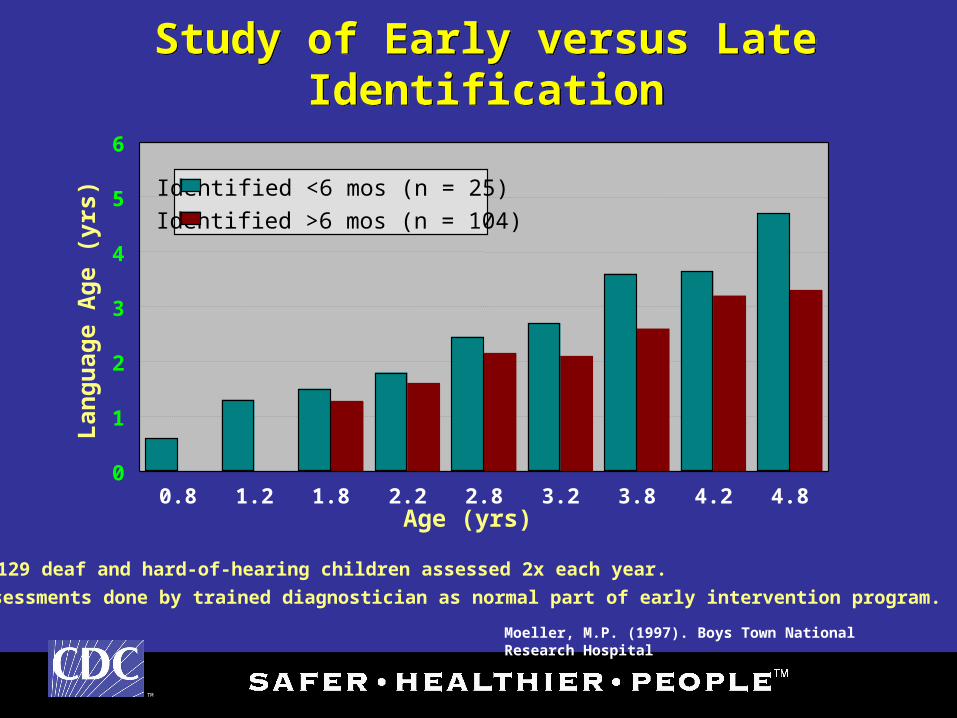
Study of Early versus Late IdentificationStudy of Early versus Late Identification
0.8 1.2 1.8 2.2 2.8 3.2 3.8 4.2 4.80
1
2
3
4
5
6
Identified <6 mos (n = 25)
Identified >6 mos (n = 104)
Age (yrs)
Lan
gu
age
Ag
e (y
rs)
Moeller, M.P. (1997). Boys Town National Research Hospital
129 deaf and hard-of-hearing children assessed 2x each year.
Assessments done by trained diagnostician as normal part of early intervention program.

TM
Universal Newborn Hearing Screening Endorsement
Universal Newborn Hearing Screening Endorsement
• American Academy of Audiology (AAA)• American Academy of Pediatrics (AAP)• American Speech-Language-Hearing Association
(ASHA)• Centers for Disease Control and Prevention (CDC)• Joint Committee on Infant Hearing (JCIH)• Maternal and Child Health Bureau (MCHB)• National Association of the Deaf (NAD)• National Institutes of Health (NIH)
TM
CDC EHDI Vision and MissionCDC EHDI Vision and MissionCDC EHDI Vision and MissionCDC EHDI Vision and Mission
• The vision of the Early Hearing Detection The vision of the Early Hearing Detection and Intervention (EHDI) program is to and Intervention (EHDI) program is to promote communication from birth for all promote communication from birth for all children.children.
• The mission of EHDI is for every state and The mission of EHDI is for every state and territory to have a complete EHDI tracking territory to have a complete EHDI tracking and surveillance system that ensures and surveillance system that ensures children with hearing loss achieve children with hearing loss achieve communication and social skills communication and social skills commensurate with their cognitive abilities. commensurate with their cognitive abilities.
TM
Children’s Health Act of 2000Public Law 106–310
Children’s Health Act of 2000Public Law 106–310
DIVISION A—CHILDREN’S HEALTH
TITLE VII—EARLY DETECTION, DIAGNOSIS, AND TREATMENT REGARDING HEARING LOSS IN INFANTS
The purposes of this title are to clarify the authority within the Public Health Service Act to authorize statewide newborn and infant hearing screening, evaluation and intervention programs and systems, technical assistance, a national applied research program, and interagency and private sector collaboration for policy development, in order to assist the States in making progress toward the following goals:

TM
Children’s Health Act of 2000Public Law 106–310
Children’s Health Act of 2000Public Law 106–310
(1) All babies born in hospitals in the United States and its territories should have a hearing screening before leaving the birthing facility.
(2) All babies who are not born in hospitals in the United States and its territories should have a hearing screening within the first 3 months of life.
(3) Appropriate audiologic and medical evaluations should be conducted by 3 months for all newborns and infants suspected of having hearing loss to allow appropriate referral and provisions for audiologic rehabilitation, medical and early intervention before the age of 6 months.
TM
Children’s Health Act of 2000Public Law 106–310
Children’s Health Act of 2000Public Law 106–310
(4) All newborn and infant hearing screening programs and systems should include a component for audiologic rehabilitation, medical and early intervention options that ensures linkage to any new and existing state-wide systems of intervention and rehabilitative services for newborns and infants with hearing loss.
(5) Public policy in regard to newborn and infant hearing screening and intervention should be based on applied research and the recognition that newborns, infants, toddlers, and children who are deaf or hard-of-hearing have unique language, learning, and communication needs, and should be the result of consultation with pertinent public and private sectors.
TM
Children’s Health Act of 2000Children’s Health Act of 2000
DIVISION A — CHILDREN’S HEALTHDIVISION A — CHILDREN’S HEALTH
TITLE VII — EARLY DETECTION, DIAGNOSIS, AND TITLE VII — EARLY DETECTION, DIAGNOSIS, AND TREATMENT REGARDING HEARING LOSS IN TREATMENT REGARDING HEARING LOSS IN INFANTSINFANTS
Health Resources and Services Administration (HRSA) shall:
make awards of grants or cooperative agreements to develop statewide newborn and infant hearing screening, evaluation and intervention programs and systems
TM
Children’s Health Act of 2000Children’s Health Act of 2000
The Centers for Disease Control and Prevention shall:• develop standardized procedures for data management• provide technical assistance on data collection and
management • promote the sharing of data regarding early hearing loss
with state-based birth defects and developmental disabilities monitoring programs
TM
Children’s Health Act of 2000Children’s Health Act of 2000
The Centers for Disease Control and Prevention (CDC) shall:
develop standardized procedures for data management and program effectiveness and costs, such as to:
• ensure quality monitoring of newborn and infant hearing loss screening, evaluation, and intervention programs and systems;
• provide technical assistance on data collection and management;
• to study the costs and effectiveness of newborn and infant hearing screening, evaluation and intervention programs and systems conducted by State-based programs in order to answer issues of importance to State and national policymakers;
TM
Children’s Health Act of 2000Children’s Health Act of 2000
National Institutes of Health (NIH) shall:
continue a program of research and development on the efficacy of new screening techniques and technology, including clinical studies of screening methods, studies on efficacy of intervention, and related research.
TM
WA 81%
MT 97%
OR 95%
NV99%
CA 56%
UT 98%
AZNM 92%
CO 97%
ID 83%
WY 98%
ND 95%
SD 90%
MN 93%
IA NE 97%
KS 97%
TX 97%
FL86%
MS95%
LA94%
GA 96%
SC 98%
NC 96%
VA96%
ME 94%
NY 92%
WI 93%
OK 96%
MO 99%
AR 92%TN 97%
KY 99%
IL100%
IN 99%
MI*
OH40%
WV98% MD 91%
DE 83%NJ 98%
VT 93%
RI 99%
CT 97%
NH 91%
MA 99%
AK 81%
HI 99%
PA 98%
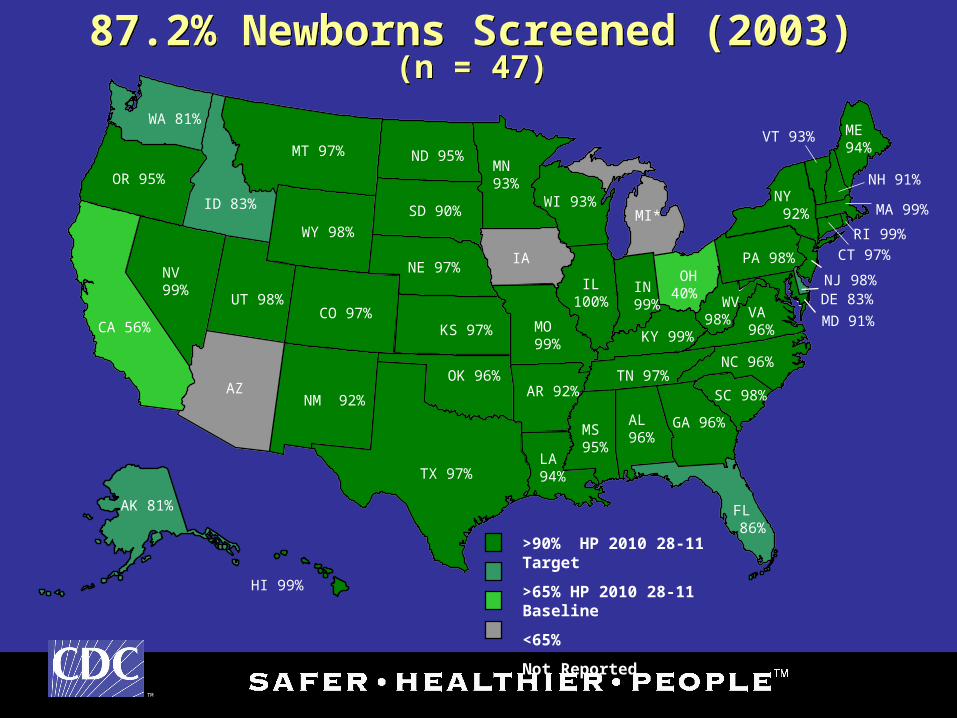
87.2% Newborns Screened (2003)(n = 47)
87.2% Newborns Screened (2003)(n = 47)
>90% HP 2010 28-11 Target
>65% HP 2010 28-11 Baseline
<65%
Not Reported
AL96%
TM
WA
MT*
OR 35%
NV
CA80%
UT 66%
AZNM
CO89%
ID 100%
WY 94%
ND43%
SD69%
MN53%
IA NE 82%
KS 77%
TX
FL
MS84%
LA65%
AL GA14%
SC 65%
NC*
VA70%
ME
NY25%
WI
OK 32%
MO 20%
AR 47%TN 61%
KY 14%
IL77%
IN
MI*
OH17%
WV66% MD 27%
DE 100%NJ 53%
VT86%
RI 95%
CT 73%
NH 9%
MA 85%
AK
HI 74%
PA60%
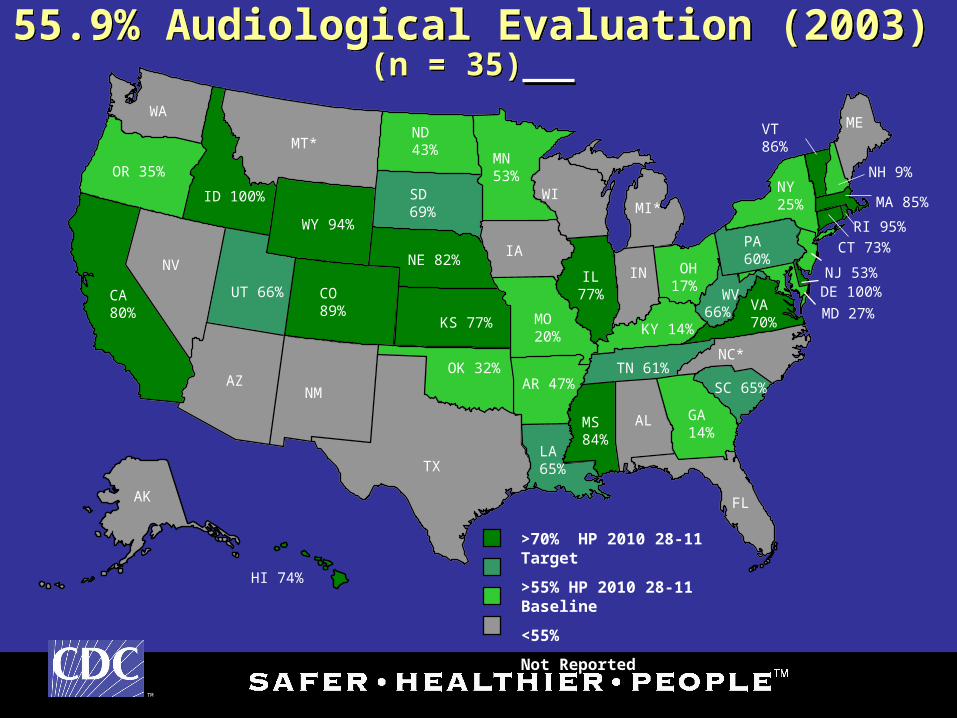
55.9% Audiological Evaluation (2003)(n = 35)
55.9% Audiological Evaluation (2003)(n = 35)
>70% HP 2010 28-11 Target
>55% HP 2010 28-11 Baseline
<55%
Not Reported
TM
WA
MT*
OR 39%
NV
CA87%
UT 41%
AZ NM50%
CO 45%
ID 100%
WY 100%
ND
SD100%
MN100%
IA NE 67%
KS 84%
TX
FL
MS85%
LA53%
AL GA
SC*
NC
VA63%
ME
NY61%
WI
OK 91%
MO 52%
AR 64%TN 100%
KY 100%
IL29%
IN67%
MI*
OH28%
WV75% MD
DE 100%NJ 75%
VT0%
RI 100%
CT 100%
NH 64%
MA 71%
AK 0%
HI 83%
PA64%
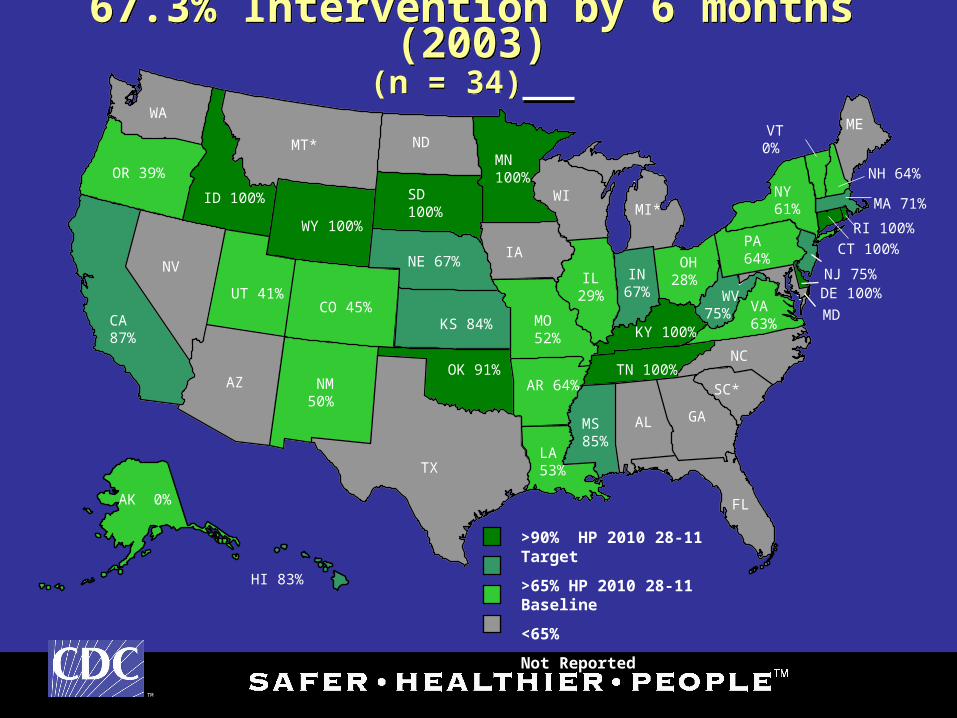
67.3% Intervention by 6 months (2003)(n = 34)
67.3% Intervention by 6 months (2003)(n = 34)
>90% HP 2010 28-11 Target
>65% HP 2010 28-11 Baseline
<65%
Not Reported
TM
Births: Combined US Military ForcesBirths: Combined US Military Forces
• Approximately 95,000 military families each year - more individual births than all but the 12 largest states
• Approximately 40% of these births occur at military facilities
• Military births take place in all 50 states and more than 20 foreign countries (8.5%)
• More than 2,000 military births per year occur in each of 11 states:– CA, CO, FL, GA, HI, KY, MD, NC, TX, VA, and WA
Non-US sites:– Germany and Japan (both > 2,000)– 3,700 in other sites
TM
Hawaii
Puerto Rico
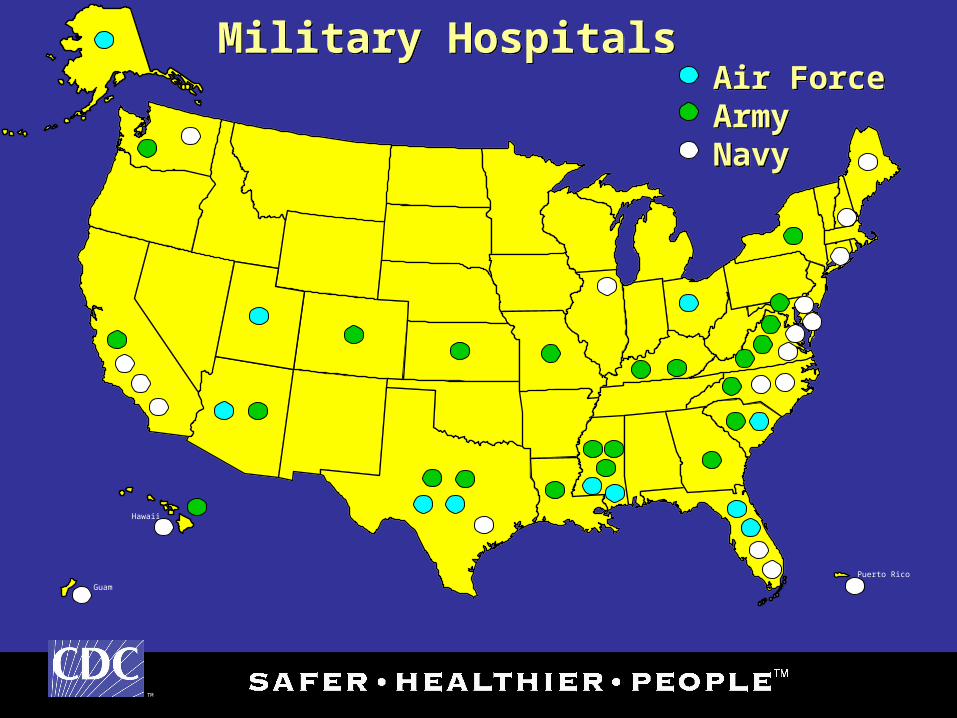
Military Hospitals Military Hospitals
Guam
Air ForceArmyNavy
Air ForceArmyNavy
TM
Recent CDC EHDI ActivitiesRecent CDC EHDI Activities
• DoD Birth and Infant Health Registry (BIHR)DoD Birth and Infant Health Registry (BIHR)
05 Jan 06
• telephone call with LCDR Margaret Ryan, M.D.
(Navy) Director, DoD Center for Deployment Health
Research and Christina Spooner, M.S., coordinator
for the BIHR
– Surveillance for birth defects in partnership with
CDC’s National Birth Defects Prevention Network
TM
DoD Birth and Infant Health RegistryDoD Birth and Infant Health Registry
• Preliminary BIHR results suggest a steady increase in
the use of V72.1 (examination of ears and hearing)
since 1998 with a large increase in the year 2000
– Increase in services or reporting?
• Approximately 1/3 of reported military births had this
code associated with their obtained services in 2003
• BIHR will continue to explore codes in their data set
TM
11 Jan 06 Teleconference11 Jan 06 Teleconference
ArmyArmy (Walter Reed): Donna MacNeil, M.A., FAAA
Air ForceAir Force: CPT Alicia Burke, M.A.
NavyNavy: CDR Leslie Sims, M.S., FAAA
CDR Margaret Ryan, M.D.
CDR Michelle Gasper, M.D.
CPT Martin McCaffrey, M.D.
LT Anne Jarrett, M.A. CCC-A
Christina Spooner, M.S.
BUMEDBUMED (D.C.) CDR Khin Aungthein, RNC, MSN
CDCCDC: John Eichwald, M.A., FAAA
Craig Mason, Ph.D.

TM
Teleconference Issues IdentifiedTeleconference Issues Identified• Most military programs are felt to be reporting data to their
respective state EHDI program• There is no uniform reporting of EHDI data or centralized
database for military families• Audiologists are generally responsible for follow-up
newborns who fail the initial screen• Primary Care Manager (PCM) responsible for follow-up
when no audiologist is assigned to a facility• Good early intervention support system available through
Educational and Developmental Intervention Services (EDIS) both domestically and overseas
• EHDI services spread out in particular for non US sites
TM
CDC / NCBDDD / EHDI Briefing CDC / NCBDDD / EHDI Briefing
06 Feb 06• RADM José Cordero, MD, MPH, FAAP
– Director, CDC National Center on Birth Defects and Developmental Disabilities
– Assistant Surgeon General• Peter Rzeszotarski, MA
– Acting Associate Director for Policy, Planning, and Evaluation
TM
Future ActivitiesFuture Activities• Continue communication among CDC-EHDI
and all military branches• Development of a new audiology survey for all
branches (Dr. McCaffrey and Dr. Ryan expressed interest in collaborating on the survey)
• Teleconference with the EDIS Program Manager
• Possible EHDI Special Topics Teleconference concerning EHDI and the Military
• Offer of resources, materials and training
TM
American Academy of Pediatrics PediaLinkAmerican Academy of Pediatrics PediaLink
• Web-based educational program for pediatric health care professionals
• Modules:
– different types of hearing loss
– screening methods for hearing loss
– medical and genetic risk factors
– the importance of early recognition and ongoing surveillance
– the role of the medical home in hearing screening
TM
American Academy of Pediatrics PediaLinkAmerican Academy of Pediatrics PediaLink
• CDC-EHDI Free Scholarships for Continuing Medical Education
(5 AMA PRA Category 1 credits)• Contact:
– John Eichwald: ‘[email protected]@cdc.gov’ – Jill Ackermann: ‘[email protected]@aap.org– or: [email protected] [email protected]’
TM
Questions?Questions?
The findings and conclusions in this presentation have not been formally disseminated by the Centers for Disease Control and Prevention and should not be construed to represent any agency determination or policy.