Embed Size (px)
Citation preview

Cancer Therapy: Preclinical
Tivantinib (ARQ197) Displays Cytotoxic Activity That IsIndependent of Its Ability to Bind MET
Cristina Basilico1,5, Selma Pennacchietti1,5, Elisa Vigna2,5, Cristina Chiriaco2, Sabrina Arena3,Alberto Bardelli3,5, Donatella Valdembri4,5, Guido Serini4,5, and Paolo Michieli1,5
AbstractPurpose: MET, the high-affinity receptor for hepatocyte growth factor, is frequently deregulated in
human cancer. Tivantinib (ARQ197; Arqule), a staurosporine derivative that binds to the dephosphorylated
MET kinase in vitro, is being tested clinically as a highly selectiveMET inhibitor. However, themechanismof
action of tivantinib is still unclear.
ExperimentalDesign:The activity of tivantinibwas analyzed inmultiple cellularmodels, including: cells
displaying c-MET gene amplification, strictly ‘addicted’ toMET signaling; cells with normal c-MET gene copy
number, not dependent on MET for growth; cells not expressing MET; somatic knockout cells in which the
ATP-binding cleft of MET, where tivantinib binds, was deleted by homologous recombination; and a cell
system ‘poisoned’ byMET kinase hyperactivation, where cells die unless cultured in the presence of a specific
MET inhibitor.
Results: Tivantinib displayed cytotoxic activity independently of c-MET gene copy number and
regardless of the presence or absence of MET. In both wild-type and isogenic knockout cells, tivantinib
perturbed microtubule dynamics, induced G2/M arrest, and promoted apoptosis. Tivantinib did not
rescue survival of cells ‘poisoned’ by MET kinase hyperactivation, but further incremented cell death. In
all cell models analyzed, tivantinib did not inhibit HGF-dependent or -independent MET tyrosine
autophosphorylation.
Conclusions:We conclude that tivantinib displays cytotoxic activity via molecular mechanisms that are
independent from its ability to bindMET. This notion has a relevant impact on the interpretation of clinical
results, on the design of future clinical trials, and on the selection of patients receiving tivantinib treatment.
Clin Cancer Res; 19(9); 2381–92. �2013 AACR.
IntroductionMET, the high-affinity receptor for hepatocyte growth
factor (HGF), is one of the most frequently activated tyro-sine kinases in human cancer and a key target for therapy(1–4). Tivantinib, also known as ARQ197, is a staurospor-ine derivative identified in a cell-based screen for proapop-totic agents. In this screen, heterocyclic compounds wereprobed for their ability to promote cell death in a panel of
human tumor cell lines. Tivantinib, a pyrroloquinolinyl-pyrrolidine-2,5-dione, was selected for its superior cytotoxicactivity toward a large number of cell types (5). Subsequentefforts aimed at characterizing its mechanism of action ledto proposing that tivantinib is a non-ATP–competitiveinhibitor of the MET kinase. Although in vitro kinase assaysconducted using a purified MET protein do suggest thattivantinib may interfere with MET enzymatic activity underparticular conditions, it is not clear whether these condi-tions can be met in real tumor cells. Furthermore, thehypothesis that MET inhibition would explain such a wide-spread cytotoxicity is not consistent with the biology ofHGF/MET.
A first study conducted by Arqule suggested that tivanti-nib reduces the VMAX of the kinase reaction without affect-ing the KM of the enzyme for ATP in a filtermat-based assay(6). The same work also showed that tivantinib displayscytotoxic activity against a wide panel of human tumor celllines with an EC50 ranging from 300 to 600 nmol/L.Intriguingly, all but one cell line (MKN-45) belonging tothis panel bear normal c-MET gene copy number. This issomehow puzzling because only cells displaying c-METgene amplification have been shown to be ‘addicted’ to
Authors' Affiliations: 1Laboratory of Experimental Therapy, 2Laboratory ofGene Transfer and Therapy, 3Laboratory of Molecular Genetics, and4Laboratory of Cell Adhesion Dynamics, Institute for Cancer Research andTreatment (IRCC); and 5Department of Oncological Sciences, University ofTorino Medical School, Candiolo, Turin, Italy
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
C. Basilico and S. Pennacchietti contributed equally to this work.
Corresponding Author: Paolo Michieli, Laboratory of Experimental Ther-apy, Institute forCancerResearch andTreatment, SP142, km3.95, I-10060Candiolo, Torino, Italy. Phone: 39-011-9933219; Fax: 39-011-9933225;E-mail: [email protected].
doi: 10.1158/1078-0432.CCR-12-3459
�2013 American Association for Cancer Research.
ClinicalCancer
Research
www.aacrjournals.org 2381
on April 17, 2021. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 26, 2013; DOI: 10.1158/1078-0432.CCR-12-3459

MET signaling in in vitro proliferation assays (7–12) in theconditions used with tivantinib (6).
A second study showed that tivantinib binds to METonly when the kinase is found in the inactive conforma-tion and disclosed the crystal structure of the depho-sphorylated MET kinase in complex with the drug (13).In this model, the tricyclic aromatic ring of tivantinib isbound deep inside a hydrophobic niche between theribose ring sugar and the a-phosphate group of ATP,thus, completely occupying the ATP-binding cleft of METwithout directly competing with ATP. The same work alsoshowed that tivantinib is capable of interfering with METkinase activity only if the latter is found in a totallydephosphorylated state and if the drug is preincubatedwith the enzyme before addition of ATP (13). In theseconditions, tivantinib delays the start of the reaction, butafter an initial lag phase, autophosphorylation eventuallytakes place with a rate that is indistinguishable from thatobserved in the absence of the drug. Conversely, if ATP isadded before tivantinib, the drug has no effect on METkinase activity. These data suggest that tivantinib mayhave limited efficacy on tumor cells expressing a consti-tutively autophosphorylated MET protein. However, incontradiction with this notion, the first study (5) clearlyshows that tivantinib effectively inhibits proliferation ofMKN-45 human gastric carcinoma cells, which displayconstitutive MET activation as a result of c-MET geneamplification (9, 14).
A third study analyzed the ability of tivantinib toinhibit metastasis in a mouse model of breast cancer. Inthis model, both tivantinib and a short hairpin RNA(shRNA) directed against the MET transcript reducedmetastatic dissemination of MDA-MB-231 cells to thebones. However, MET shRNA did not affect MDA-MB-231 cell proliferation and survival in vitro, whereas tivan-
tinib displayed potent cytotoxic activity in the sameconditions (15). This discrepancy suggests that at leastpart of the pharmacologic effects of tivantinib is notmediated by MET inhibition in this system.
The clinical development of tivantinib is highlyadvanced. Its safety and efficacy is under investigation ina variety of clinical trials in solid tumors (16). Although thepreclinical data do not support a clear role of MET inmediating its pharmacologic activity, tivantinib is beingtested in the clinic as a highly selective MET tyrosine kinaseinhibitor. In a phase II trial (NCT00777309), the progres-sion-free survival of non–small cell lung carcinoma(NSCLC) patients receiving tivantinib plus erlotinib (Tar-ceva; Genentech)was comparedwith that of patients receiv-ing placebo plus erlotinib (17). While the primary endpoint was not met, the tivantinib–erlotinib associationshowed a statistically significant benefit in a subset ofpatients carrying ras mutations, a condition known topromote resistance to MET inhibitors (9, 18). On the otherhand, it also showed a significant delay in the developmentof new metastases among patients with nonsquamoushistology, a sub-population displaying higher levels ofMETexpression. On the basis of these results, a phase III studywas designed (NCT01244191, MARQUEE) that tested thesame drug scheme in nonsquamous NSCLC patients.Unfortunately, this study was interrupted for futility (19).Several other phase II trials and two phase III trials(NCT01377376, ATTENTION; NCT01755767, METIV) arecurrently active, and the correlation between MET expres-sion in tumors and the therapeutic response to tivantinib isbeing investigated.
In order to cast light onto themechanismof action of thispromising drug, we decided to analyze the ability of tivan-tinib to inhibit MET using several cellular models. Thesemodels include: (i) human tumor cell lines displaying c-MET gene amplification, strictly ‘addicted’ to MET; (ii)human tumor cell lines bearing normal c-MET gene copynumber, insensitive to MET inhibition in proliferationassays; (iii) a genetically engineered human cell line inwhich the exon encoding the ATP-binding cleft of the METkinase—where tivantinib binds—was knocked out byhomologous recombination; (iv) two human tumor celllines not expressing MET at all; and (v) an engineered cellsystem ‘poisoned’ by MET kinase hyperactivation, wherecells survive and grow only in the presence of a specificMETinhibitor.
Materials and MethodsCell culture
HepG2 hepatocarcinoma cells, MKN-45, Hs746T, andSNU-5 gastric carcinoma cells, H1993, NCI-H441, A549lung carcinoma cells, TOV-112D and A2780 ovarian carci-noma cells, U87-MG glioblastoma cells, and HCT-116colon carcinoma cells were obtained from the EuropeanCollection of Cell Cultures (Salisbury, Wiltshire, UnitedKingdom) and cultured as suggested by the supplier.EBC-1 lungcarcinoma cellswereobtained fromthe JapaneseCollection of ResearchBioresources (Osaka, Japan). GTL-16
Translational RelevanceMET is one of the most frequently activated tyrosine
kinases in human cancer. Although a variety of METinhibitors have been developed, only a few have pro-gressed to the clinic. The recent failure of a phase III trialwith tivantinib, the most clinically advanced molecule,could raise concerns about the validity of MET as atherapeutic target. However, the data presented hereprovide evidence that tivantinib is not a MET inhibitorbut an antimitotic agent that kills tumor cells indepen-dently of MET. Therefore, the negative results obtainedwith tivantinib should not be generalized to other METinhibitors. Moreover, selection of patients undergoingtivantinib treatment should not be based onMET status,and future clinical trials should be designed acknowl-edging that MET is not the pharmacologic target oftivantinib. Finally, patients who could benefit of METinhibition should not be subtracted from treatmentwithan authentic anti-MET drug.
Basilico et al.
Clin Cancer Res; 19(9) May 1, 2013 Clinical Cancer Research2382
on April 17, 2021. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 26, 2013; DOI: 10.1158/1078-0432.CCR-12-3459

gastric carcinoma cells were derived from MKN-45 cells asdescribed previously (14). EBC-1 and GTL-16 cells weremaintained in RPMI medium (Sigma Life Sciences) supple-mented with 10% FBS and 2mmol/L glutamine (Sigma LifeSciences). Isogenic wild-type (WT) andMET exon 16 knock-out (KO)DLD-1 colon carcinoma cells have been describedpreviously (20).
Drugs and chemicalsTivantinib (ARQ197), JNJ-38877605, and DN30 Fab
were supplied by Arqule, Janssen Pharmaceutical Co. ofJohnson& Johnson, andMetheresis (Lugano, Switzerland),respectively. PHA-665752 (Pfizer) was purchased fromTocris Bioscience. Paclitaxel (Taxol; Bristol-Myers-Squibb)was obtained from our hospital pharmacy. Imatinib (Glee-vec; Novartis), SU-5416 (Semaxinib; Pfizer), and Iressa(Gefitinib; AstraZeneca) were obtained from Selleck Che-micals. Staurosporine and puromycin were purchased fromSigma-Aldrich.
In vitro proliferation and apoptosis assaysFor proliferation assays, cells were seeded in 96-well
plates (1,000 cells/well) with the appropriate culture medi-um in the presence of FBS. The day after, cells were treatedwith increasing concentrations of tivantinib or a controlMET inhibitor (JNJ-38877605, PHA-665752, DN30 Fab).After 3 days of treatment, cell numberwas determined usingCell Titer Glo (Promega) with a Victor X4 multilabel platereader (Perkin Elmer). For apoptosis assays, cells wereseeded in 96-well plates as described above. The followingday, cells were exposed to increasing concentrations (0–1,200 nmol/L) of tivantinib or JNJ-38877605, and apopto-sis was determined after 48 hours by the free nucleosomemethod using a Cell Death Detection ELISAPLUS kit (RocheDiagnostics). Data were analyzed and fit using Prism soft-ware (GraphPad).
Cell-cycle analysisWT and MET exon 16 KO DLD-1 cells were incubated
with 600 nmol/L tivantinib or JNJ-38877605. After 48hours, cells were detached with trypsin, washed with PBS,fixed in ice-cold 70% ethanol, and stored at �20�C. Theday after, cells were washed with PBS, re-suspended in 0.2mL of staining solution (50 mg/mL propidium iodide, 100mg/mL RNase A in PBS), and incubated for 3 hours at 4�C.Samples were analyzed by flow cytometry using aCyANADP apparatus (Dako, Glostrup, Denmark). Cell-cycle distribution was determined using Flowjo software(Tree Star).
Gene copy number analysisGenomicDNAwas isolated usingDNeasy Blood&Tissue
Kit (Qiagen) according to the manufacturer’s instructions.DNA concentration was determined using a Nanodrop1000 spectrophotometer (Thermo Fisher Scientific). Quan-titative PCR (qPCR) on genomic DNAwas carried out usingthe Go Taq qPCR Master Mix (Promega) and a 7900 HTAbiprism Real-Time System (Applied Biosystems) with the
appropriate primers as described previously (21). The ribo-somal protein S6 kinase (RPS6KC1) gene, located on chro-mosome 1, was used for gene dosage normalization.
Confocal microscopyWT andMET exon 16 KODLD-1 cells were seeded in 24-
well plates (12,500 cells/well) on glass coverslips coatedwith human plasma fibronectin (3 mg/mL; R&D Systems).One day after plating, cells were incubated for 36 hourswith the appropriate concentrations of tivantinib, JNJ-38877605, or paclitaxel and then fixed in 4% formaldehydefor 20 minutes at room temperature, permeabilized with0.1% Triton X-100 in PBS for 2minutes on ice, and blockedwith 1%bovine serumalbumin (BSA) inPBS for 30minutesat room temperature. Fixed cells were stained with rabbitanti-a tubulin polyclonal antibody (Abcam) and revealedby Alexa Fluor 555-conjugated secondary antibody (Molec-ular Probes, Life Technologies). Confocal analysis wascarried out on a Leica TCS SP2 AOBS microscope (LeicaMicrosystems) by maintaining the same laser intensity,gain, and offset settings for all samples including controls.Each image was acquired at a 200-Hz line scanning rate,each line being integrated 8 times. Maximum projectionimages were created from Z stacks of 30 to 40 sections (stepinterval¼ 0.1–0.2 mm) spanning the whole cell using LeicaConfocal Software (LCS). Mean fluorescence intensity(MFI) was determined by analyzing 20 different cells persample and expressed as 8-bit greyscale values.
Lentiviral vector engineeringThe amino acid sequence of Tpr-MET and of HGF corre-
sponds to GenBank #U19348 and #M73239, respectively.The cDNAs encoding the above proteins were subclonedinto the lentiviral vector backbone pRRL.sin.cPPT.CMV.Wpre (22) downstream to the cytomegalovirus (CMV)promoter. Lentiviral vectors particles were packaged bytransient transfection of 293T cells as described previously(23). Vector particle concentration was determined by HIV-1 p24 core profile ELISA (Perkin Elmer).
HepG2 cell growth rescue assaysExponentially growing HepG2 cells were seeded in 96-
well plates at a density of 2,000 cells per well. One day later,cells were transducedwith purified lentiviral vector particlesencoding HGF, Tpr-MET, or with empty vector as control(100 ng/mL HIV-1 p24). One day after transduction andevery 2 days thereafter, the medium was replaced with afresh medium containing increasing concentrations of thevarious drugs as indicated (0–1,000 nmol/L). Cell numberwas determined after 10days usingCell TiterGlo (Promega)as described above. Data were analyzed and fit using Prismsoftware (GraphPad).
MET expression and activationFor analysis of MET autophosphorylation, GTL-16 and
EBC-1 cells were incubated for 24 hours with increasingconcentrations of tivantinib (0–3,000 nmol/L) or JNJ-38877605 (0–1,000 nmol/L) and then lysed as previously
Tivantinib Displays MET-Independent Cytotoxic Activity
www.aacrjournals.org Clin Cancer Res; 19(9) May 1, 2013 2383
on April 17, 2021. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 26, 2013; DOI: 10.1158/1078-0432.CCR-12-3459

described (24). Cell lysates were resolved by electrophoresisand analyzed by Western blotting using antibodies specificfor the two most relevant phosphorylated forms of MET(Tyr1234–Tyr1235 and Tyr1349; Cell Signaling Technology).Total MET was determined by Western blotting using the3D4 anti-human Met antibody (Life Technologies). A549,HCT-116, U87-MG, and NCI-H441 cells were incubatedfor 24 hours in 0.5% FBS in the presence of increasingconcentrations (0–1,000 nmol/L) of tivantinib or JNJ-38877605 and then stimulatedwith 50ng/mL recombinanthuman HGF (R&D Systems) for 10 minutes. Cell lysateswere resolved by electrophoresis and analyzed by Westernblotting using anti-phospho-MET or anti-total MET anti-bodies as described above.WT andMET exon 16 KODLD-1cells were incubated for 24 hours in 0.5% FBS in thepresence of 1,000 nmol/L tivantinib or JNJ-38877605 andthen stimulated with 50 ng/mL recombinant human HGF(R&D Systems) for 10 minutes. Cell lysates were immuno-precipitated as described previously (24) using the DQ-13anti-MET antibody (25) and resolved by electrophoresis.The levels of phosphorylated and totalMETwas determinedby Western blotting using the appropriate antibodies asdescribed above.
ResultsTivantinib inhibits the growth of tumor cells notexpressing MET or not dependent on MET forproliferation
Previous studies suggest that only cells carrying c-METgene amplification are ‘addicted’ toMET signaling in in vitroproliferation assays (7–12). Cell lines with normal c-METgene copy number, regardless of their MET expressionlevels, are insensitive toMET blockade in anchorage-depen-dent conditions and in the absence of HGF (reviewed inref. 26). To assess the specificity of tivantinib, its ability toinhibit cell proliferation was analyzed on a panel of tumorcells that included six cell lines with high c-MET gene copynumber (GTL-16, MKN-45, Hs746T, SNU-5, EBC-1, andH1993) and six cell lines with normal c-MET gene copynumber (NCI-H441, A549, HCT-116, U87-MG, A2780,and TOV-112D; Supplementary Fig. S1A). In addition, thelatter group contained two cell lines that donot expressMETprotein or mRNA (A2780 and TOV-112D; SupplementaryFig. S1B; refs. 27, 28). Using this cell panel, the antiproli-ferative activity of tivantinib was compared with that ofother anti-MET drugs including twoATP-competitive small-molecule inhibitors (JNJ-38877605, Johnson & Johnson;refs. 18, 21, 29; PHA-665752, Pfizer; ref. 30) and a mono-clonal antibody Fab fragment causing MET ‘shedding’(DN30 Fab, Metheresis; refs. 31, 32). This analysis revealedthat the response profile of tivantinib clearly segregates itfrom that of other MET-specific agents (Fig. 1). Indeed, JNJ-38877605, PHA-665752, and DN30 Fab selectively inhib-ited proliferation of cells displaying c-MET gene amplifica-tion in a dose-dependent fashion without affecting thegrowth of cells with normal c-MET gene copy number. Incontrast, tivantinib indiscriminately inhibited proliferationof all cells independently of c-MET gene amplification and
MET protein expression with an EC50 ranging from 60 to600 nmol/L. These results are surprising for multiple rea-sons. On one hand, due to its peculiar binding moderequiring MET dephosphorylation (13), tivantinib shouldnot work in cells with high c-MET gene copy number (GTL-16, MKN-45, Hs746T, SNU-5, EBC-1, and H1993) becausethese display constitutive MET kinase activation. On theother, if tivantinib were a selective MET inhibitor, it shouldnot inhibit the growth of cells bearing normal c-MET genecopy number (NCI-H441, A549, HCT-116, and U87-MG),as these are not dependent on MET signaling in prolifera-tion assays (7–12). Finally and most importantly, if thebiological activity of tivantinib was because of its ability toinhibit MET, this drug should have no effect on cells that donot express the MET protein (A2780 and TOV-112D).
Tivantinib does not inhibit MET autophosphorylationin tumor cells
Prompted by these data, we analyzed whether tivantinibinhibitedMETactivity in the same cellswhere it proved tobeactive biologically. GTL-16 gastric and EBC-1 lung carcino-ma cells, which display HGF-independent, constitutiveMET activation due to MET protein overexpression (9),were incubated for 24 hours with increasing concentrationsof tivantinib (0–3,000 nmol/L) or JNJ-38877605 (0–1,000nmol/L), and MET tyrosine autophosphorylation wasdetermined by Western blot analysis using antibodies spe-cific for the two most relevant phosphorylated forms ofMET (Tyr1234–Tyr1235 and Tyr1349). While JNJ-38877605potently inhibited MET autophosphorylation at 100nmol/L, tivantinib had no significant effect on phospho-MET signal at any concentration (Fig. 2A). As discussed,the failure of tivantinib to inhibit MET kinase activity inthese cells could be because of its peculiar binding moderequiring MET dephosphorylation (13). However, tivanti-nib effectively inhibited GTL-16 and EBC-1 cell prolifera-tion with an EC50 of approximately 300 nmol/L (Fig. 1),thus questioning that the biological activity of this drugis due to MET kinase inhibition in these cells. The ability oftivantinib to inhibit MET autophosphorylation was alsoanalyzed in cells bearing normal c-MET gene copy number(Supplementary Fig. S1). A549 lung carcinoma and HCT-116 colon carcinoma cells were preincubated with increas-ing concentrations (0–1,000 nmol/L) of tivantinib or JNJ-38877605 and then stimulatedwith 50ng/mL recombinanthuman HGF. MET activation was determined using anti-phospho-MET antibodies as above. Remarkably, MET wasfound in a completely dephosphorylated state in these cellsbefore HGF stimulation, thus representing an ideal targetfor tivantinib. In spite of this, tivantinib failed to inhibitHGF-induced MET tyrosine autophosphorylation at eitherTyr1234–Tyr1235 or Tyr1349 at any concentration tested (Fig.2B and 2C). In contrast, JNJ-38877605 effectively reducedphospho-MET levels in both cell lines. A similar analysiswas conducted using U87-MG glioblastoma cells and NCI-H441 lung carcinoma cells that also display normal c-METgene copy number (Supplementary Fig. S1). In thesecell models as well, tivantinib did not affect MET
Basilico et al.
Clin Cancer Res; 19(9) May 1, 2013 Clinical Cancer Research2384
on April 17, 2021. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 26, 2013; DOI: 10.1158/1078-0432.CCR-12-3459

autophosphorylation at either the major phosphorylationsite or the docking site (Supplementary Fig. S2). As tivanti-nib inhibited proliferation of A549, HCT-116, U87-MG,and NCI-H441 cells with an EC50 ranging from 60 (HCT-116) to 600 nmol/L (NCI-H441; Fig. 1), we conclude thatthe antiproliferative activity of tivantinib is not due to METkinase inhibition in these cells as well.
Deletion of the ATP-binding cleft of MET does notimpair the cytotoxic activity of tivantinibTo further assess whether the pharmacologic activity of
tivantinib requires MET, we employed an isogenic pair ofhuman DLD-1 colon carcinoma cells. This pair consistsin WT DLD-1 cells—that are diploid and display normalc-MET gene copy number—and an engineered variant inwhich exon 16 of the c-MET gene, encoding the ATP-binding cleft of the MET kinase, was knocked out on bothalleles by homologous recombination (20). The resultingengineered cells (referred to as ‘MET exon 16 KO DLD-1cells’ in this study) express a deleted MET protein that not
only is completely kinase-inactive (20), but also lacks theentire tivantinib-binding domain according to crystal struc-ture data (ref. 13; Fig. 3A). The biochemical and biologicalresponse to tivantinibwas tested in parallel on bothWT andMET exon 16 KO DLD-1 cells, using JNJ-38877605 as apositive control for MET inhibition. In receptor activationexperiments, tivantinib failed to inhibit HGF-induced METautophosphorylation, while JNJ-38877605 completelyabrogated it (Supplementary Fig. S3). In cell proliferationassays, tivantinib potently inhibited the growth of bothWTand MET exon 16 KO DLD-1 cells with exactly the sameefficiency, thus confirming that the antiproliferative activityof tivantinib is not mediated by MET kinase inhibition. Incontrast, and consistent with the notion that cells bearingnormal c-MET gene copy number are not dependent onMET signaling for proliferation, JNJ-38877605 did notaffect the growth of either cell type (Fig. 3B). Flow cyto-metric analysis of DNA content revealed that tivantinibcaused cell-cycle arrest in G2/M independently of the METstatus (Fig. 3C). At the same time, tivantinib also reduced
Figure 1. Tivantinib inhibits thegrowth of tumor cells not expressingMET or not dependent on MET forproliferation. Ample experimentalevidence suggests that only cellsdisplaying high c-MET gene copynumber (GCN) are 'addicted' to METsignaling in proliferation assays(7–12, 26). We selected a panel ofhuman tumor cells that included 6cell lines with high c-MET GCN(GTL-16, MKN-45, Hs746T, SNU-5,H1993, EBC-1; blue lines) and 6 celllines with normal c-MET GCN (NCI-H441, A549, HCT-116, U87-MG,A2780, TOV-112D; red lines). Thelatter group included 2 cell lines thatdo not express MET protein ormRNA (A2780 and TOV-112D, reddotted lines; refs. 27, 28). Using thispanel, the ability of tivantinib toinhibit cell proliferation wascompared with that of other anti-MET drugs including 2 ATP-competitive small-moleculeinhibitors (JNJ-38877605 and PHA-665752) and a monoclonal antibodyFab fragment causing MET'shedding' (DN30 Fab). Cell numberis expressed as % relative to theuntreated control (CTRL). Values arethe mean � SD of 2 sets ofexperiments conducted inquadruplicate. See SupplementaryFig. S1A and S1B for moreinformation on GCN and METexpression, respectively.
100 101 102 103
0
50
100
150
100 101 102 103
0
50
100
150
100 101 102 103
0
50
100
150JNJ-38877605
Drug conc. (log nmol/L)
Ce
ll n
um
be
r (%
of
ctr
l)
PHA-665752
Drug conc. (log nmol/L)
Ce
ll n
um
be
r (%
of
ctr
l)
DN30 Fab
Drug conc. (log nmol/L)
Ce
ll n
um
be
r (%
of
ctr
l)
Tivantinib
Drug conc. (log nmol/L)
Ce
ll n
um
be
r (%
of
ctr
l)
SNU-5
MKN-45GTL-16
Hs746T
H1993 EBC-1
NCI-H441
U87-MG
A549
HCT-116
A2780 TOV-112D
High c-MET GCN (≥ 15) Normal c-MET GCN (≤ 3)
100 101 102 103
0
50
100
150
Tivantinib Displays MET-Independent Cytotoxic Activity
www.aacrjournals.org Clin Cancer Res; 19(9) May 1, 2013 2385
on April 17, 2021. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 26, 2013; DOI: 10.1158/1078-0432.CCR-12-3459

the fraction of cells in G1 and dramatically increased thesub-G1 population. This suggests that tivantinib promotesmitotic arrest, prevents cells from re-entering G1, and drivesthem to apoptosis. Analysis of free nucleosomes in thecytoplasm—a hallmark of apoptosis—confirmed thattivantinib induces programmed cell death regardless of thepresence or absence of a functional MET kinase (Fig. 3D).
Tivantinib promotes microtubule stabilizationindependently of MET
The results discussed here suggest that tivantinib is amitotic inhibitor and a proapoptotic agent that displays
its cytotoxic activity independently of MET. Because mostantimitotic agents impair cytoskeleton dynamics, we test-ed whether tivantinib could affect microtubule stability.WT and MET exon 16 KO DLD-1 cells were incubatedwith increasing concentrations (177–900 nmol/L) oftivantinib or JNJ-38877605 for 36 hours, and the amountof a-tubulin–containing microtubules was determined byconfocal immunofluorescence analysis using antibodiesdirected against total a-tubulin. For each sample, 20different cells were scanned, and fluorescence signal wasexpressed as MFI in 8-bit greyscale values (0–255). Thisanalysis revealed that tivantinib increases the amount of
A
B
− HGF + HGF − HGF + HGF
JNJ-38877605
150 kDa
150 kDa
150 kDa
Drug conc.
(nmol/L)
0 10
100
1000
10
100
1,0
00
0 0 10
100
1,0
00
10
100
1,0
00
0
Tivantinib
C
Drug conc.
(nmol/L)
0 10
100
1000
10
100
1,0
00
0 0 10
100
1,0
00
− HGF + HGF − HGF + HGF
JNJ-38877605
150 kDap-MET (Tyr1234-Tyr1235)
150 kDap-MET (Tyr1349)
150 kDaTotal MET
10
100
1,0
00
0
Tivantinib
A549
HCT-116
p-MET (Tyr1234-Tyr1235)
p-MET (Tyr1349)
Total MET
Drug conc.
(nmol/L)
p-MET (Tyr1234-Tyr1235)
p-MET (Tyr1349)
Total MET
30
300
3,0
00
0 30
300
3,0
00
0
GTL-16 EBC-1
Tivantinib
10
100
1,0
00
0 10
100
1,0
00
0
GTL-16 EBC-1
JNJ-38877605
150 kDa
150 kDa
150 kDa
Figure 2. Tivantinib does not inhibitMET autophosphorylation in tumorcells. A, GTL-16 human gastriccarcinoma cells and EBC-1 humanlung carcinoma cells, whichdisplay c-MET gene amplificationand constitutive MET kinaseautophosphorylation, wereincubated for 24 hours withincreasing concentrations oftivantinib (0–3,000 nmol/L) or JNJ-38877605 (0–1,000 nmol/L), andMET activation was determined byWestern blotting using anti-phospho-MET (p-MET) antibodiesdirected against the majorphosphorylation site (Tyr1234–Tyr1235) or the docking site(Tyr1349). Total MET wasdetermined using anti-METantibodies. B, A549 human lungcarcinoma cells, which bearnormal c-MET gene copy numberand express physiologic METlevels, were preincubated for24 hours with increasingconcentrations (0–1,000 nmol/L) oftivantinib or JNJ-38877605 andthen stimulated with 50 ng/mLrecombinant HGF. MET activationwas determined by Westernblotting using anti-phospho-METantibodies as described. TotalMET was determined using anti-MET antibodies. C, HCT-116human colon carcinoma cells,which bear normal c-MET genecopy number and expressphysiologic MET levels, weretreated, stimulated, and analyzedas described in B. The 170 and145 kDa bands correspond to theunprocessed and mature form ofMET, respectively.
Basilico et al.
Clin Cancer Res; 19(9) May 1, 2013 Clinical Cancer Research2386
on April 17, 2021. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 26, 2013; DOI: 10.1158/1078-0432.CCR-12-3459

a-tubulin–containing microtubules in a dose-dependentfashion (Fig. 4A). Remarkably, the microtubule-stabiliz-ing activity of tivantinib in MET exon 16 KO cells wasindistinguishable from that observed in WT DLD-1 cells.Because the former cells express a deleted form of METthat is kinase inactive (Supplementary Fig. S3; ref. 20) andlacks the tivantinib-binding site (13), these results suggestthat tivantinib impairs microtubule dynamics via amolecular mechanism that does not involve MET kinaseinhibition or MET binding. Consistent with this idea,MET inhibition by JNJ-38877605 did not have any effecton microtubule stability at any concentration in eithercell line (Fig. 4A). Representative confocal microscopyimages of cells treated with tivantinib or JNJ-38877605are shown in Fig. 4B.
An engineered cell system ‘poisoned’ by MET kinasehyperactivation allows identification of MET-specificinhibitors
Previous studies have shown that human HepG2hepatocarcinoma cells undergo growth arrest and apop-tosis—instead of growing—following activation of theMETsignaling pathway (33). Exploiting this paradoxical phe-nomenon,we set up an engineered cell system ‘poisoned’ byMET kinase hyperactivation in which cells die unless theyare cultured with a specific MET inhibitor. The principle ofthis system is illustrated in Fig. 5. HepG2 cells are trans-duced with an engineered lentiviral vector (LV) expressingHGF or Tpr-MET (34), a constitutively active form of METfound in transformed cells (Fig. 5A). Following transduc-tion, cells are cultured with no drug or with increasing
A
101 102 103 1040
30
60
90
120
Drug conc. (log nmol/L)
Ce
ll n
um
be
r (%
of
ctr
l)
B
DC
101 102 103 1040
30
60
90
120
Drug conc. (log nmol/L)
Fre
e n
uc
leo
so
me
s/c
ell (
AU
)
SEMA
PSI
KDABC
IPT 1-4
Tivantinib
ATP
Exon 16 KO MET
Tivantinib
ATP
Wild-type MET
KD
TCTC
SEMA
PSI
IPT 1-4
0
20
40
60
80
100
SG
2–M
Sub
-G1
G0–
G1
Ce
ll-c
yc
le d
istr
ibu
tio
n (
%)
WT DLD-1
CTRL TVB JNJ
31.35
16.64
51.56
00.45
30.09
28.67
14.52
26.72
00.52
51.97
30.69
16.82
JNJ WT
JNJ KO
TVB WT
TVB KO
00.66
13.32
26.89
59.13
21.85
13.74
32.65
31.76
00.59
13.69
59.67
26.05
KO DLD-1
CTRL TVB JNJ
JNJ WT
JNJ KO
TVB WT
TVB KO
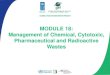
Figure 3. Deletion of the ATP-binding cleft of MET does not impair the cytotoxic activity of tivantinib. A, exon 16 of the c-MET gene encodes the ATP-bindingcleft ofMET (ABC; in red) that containsboth the catalytic ATPsite and thehydrophobic pouchwhere tivantinib binds (13). InMETexon16knockout (KO) humanDLD-1 colon carcinoma cells, exon 16 has been deleted by homologous recombination (22). Therefore, the resulting deleted MET protein lacks both kinaseactivity and the ability to bind tivantinib. SEMA, 7-bladed b-propeller Semaphorine homology domain; PSI, plexin–semaphorine–integrin homology domain;IPT 1-4, immunoglobulin–plexin–transcription factor homology domains 1–4; KD, kinase domain; CT, C-terminal tail. B, the ability of tivantinib (TVB; red lines)or JNJ-38877605 (JNJ; blue lines) to inhibit cell proliferation was tested in parallel in both wild-type (WT; solid lines) orMET exon 16 KO (dotted lines) DLD-1cells. Cell number is expressed as percentage relative to untreated control (CTRL). Values are the mean � SD of 2 sets of experiments conducted inquadruplicate. C, flow cytometric analysis showing cell-cycle distribution ofWT andMET exon 16 KODLD-1 cells treated with no drug, 600 nmol/L tivantinib,or 600 nmol/L JNJ-38877605. Values corresponding to each cell-cycle phase are shown within columns. D, WT or MET exon 16 KO DLD-1 cells wereincubated with increasing concentrations (0–1,200 nmol/L) of tivantinib or JNJ-38877605 for 48 hours and then processed for apoptosis analysis.Programmedcell deathwasmeasuredby the freenucleosomemethod. Valuesare themean�SDof 2 sets of experiments conducted inquadruplicate andarenormalized for cell number. AU, arbitrary units.
Tivantinib Displays MET-Independent Cytotoxic Activity
www.aacrjournals.org Clin Cancer Res; 19(9) May 1, 2013 2387
on April 17, 2021. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 26, 2013; DOI: 10.1158/1078-0432.CCR-12-3459

concentrations of a putative MET inhibitor. Without anytreatment, HGF- or Tpr-MET–expressing cells stop growingand die. If the drug analyzed possesses MET inhibitoryactivity, the survival and growth of HepG2 cells is rescuedin a dose-dependent fashion. In contrast, if the drug is not aMET inhibitor, cells die regardless of its concentration. Atthe same time, cells are also transducedwith an empty LV ascontrol and are subjected to the same pharmacologic treat-ment (Fig. 5B). Without any drug or in the presence of atargeted agent, whether directed against MET or against adifferent tyrosine kinase, control cells proliferate normally.However, if the drug tested has cytotoxic activity, controlcells die. By comparing the drug-response profile observedin cells expressing HGF or Tpr-MET with that observed incontrol cells, it is possible to determine whether a drug is aMET inhibitor, a targeted agent directed against a differentmolecule, or a cytotoxic compound.
Tivantinib is a cytotoxic drug and not a MET-targetedagent
Using the HepG2 system, we compared the pharmaco-logic profile of tivantinibwith that of other drugs, includingtargeted agents and generic cytotoxic compounds (Supple-mentary Table S1). Targeted agents included JNJ-38877605,PHA-665752, gefitinib (an inhibitor of EGF receptor), ima-tinib (an inhibitor of platelet-derived growth factor recep-
tor, Bcr-ABL, and KIT) and semaxinib (an inhibitor of VEGFreceptor, KIT, and RET). Generic cytotoxic compoundsincluded staurosporine (a protein kinase inhibitor), puro-mycin (a protein synthesis inhibitor), and paclitaxel(a microtubule inhibitor). This analysis revealed that onlyJNJ-38877605 and PHA-665752 could rescue survival andgrowth of cells expressing HGF or Tpr-MET (Fig. 6, bluelines). Gefitinib, imatinib, and semaxinib failed to achievethis rescue, and did not affect control cells either (greenlines). In contrast, cytotoxic compounds not only failed torescue survival and growth of cells ‘poisoned’ by METactivation, but also caused death of control cells (red lines).In this setting, tivantinib clearly behaved as a cytotoxic drugand not as a MET inhibitor (black lines). These data areconsistent with our biochemical analysis indicating thattivantinib does not inhibit MET autophosphorylation intumor cells. In addition, they are consistent with the originof tivantinib that was discovered as a cytotoxic agent in acell-based screen (5, 6). Our engineered system confirmsthat tivantinib displays cytotoxic activity in tumor cells, butdoes not support the hypothesis that this activity is medi-ated by MET kinase inhibition.
DiscussionTivantinib was identified in a cell-based screen for proa-
poptotic agents (5) as a compound that displayed potent
B
A
0
20
40
60
80
100
120
140
160
600400267178 9000
MF
I
Drug conc. (nmol/L)
TVB KO DLD-1
JNJ KO DLD-1
TVB WT DLD-1
JNJ WT DLD-1
WT
DL
D-1
PaclitaxelJNJ-38877605TivantinibControl
ME
T K
O D
LD
-1
Figure 4. Tivantinib promotesmicrotubule stabilizationindependently of MET. A, WT andMET exon 16 KO DLD-1 humancolon carcinoma cells wereincubated with increasingconcentrations (178–900 nmol/L)of tivantinib (TVB) or JNJ-38877605 (JNJ) for 36 hours,and the amount of a-tubulin–containing microtubules wasdetermined by confocalimmunofluorescence analysisusing antibodies directed againsttotal a-tubulin. Fluorescencesignal was quantified usingdedicated software and isexpressed as mean fluorescenceintensity (MFI) in 8-bit greyscalevalues (0–255). Values are themean� SD of 20 different cells perexperimental point. B, cells weretreated with 600 nmol/L tivantinib,600 nmol/L JNJ-38877605, or 300nmol/L paclitaxel as a control andthen analyzed by confocalimmunofluorescence usingantibodies directed againsta-tubulin (green). Nuclei werestained with DAPI (blue).Magnification, �630.
Basilico et al.
Clin Cancer Res; 19(9) May 1, 2013 Clinical Cancer Research2388
on April 17, 2021. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 26, 2013; DOI: 10.1158/1078-0432.CCR-12-3459

cytotoxic activity in a wide variety of tumor cell types (6).The biology of HGF and its receptor MET has been object ofintense study in the last three decades. Accurate review ofthese studies suggests that MET inhibition cannot explainsuch a widespread cytotoxicity. Inhibition of MET signalingis causally associated to apoptosis—in the conditions usedin the screen—only in a very restricted group of tumor cellswith a precise genotype (reviewed in ref. 26). Therefore,even considering its unconventional mechanism of bind-ing, the pharmacologic activity of tivantinib can hardly beexplained by its ability to interact withMET. The preclinicaldata also do not show that tivantinib really inhibits METkinase activity, but rather suggest that tivantinib delaysMETkinase activation only if the drug is preincubated withdephosphorylated MET in the absence of ATP (13). Thepossibility of encountering or reproducing these conditionsin tumor cells is uncertain. In any case, the results presentedhere show that tivantinib does not inhibit HGF-dependentor -independent MET autophosphorylation in any of thetumor cell lines examined, despite the drug concentrationstested were significantly higher than those sufficient forinducing apoptosis in the same cells.Although these data suggest that tivantinib does not
inhibit MET kinase activity in tumor cells, the possibilitythat this drug may modulate some other MET-relatedfunction remains open. However, tivantinib elicited asound cytotoxic effect also in cells expressing a deleted
MET protein lacking the tivantinib-binding site and,strikingly, in cells not expressing MET at all. These obser-vations do not support a crucial role of MET in mediatingthe pharmacologic activity of tivantinib. The virtuallyuniversal cytotoxic activity of this drug is more likely tobe explained by interference with a more basic cellularfunction. The observation that tivantinib promotes dose-dependent stabilization of microtubules provides a usefulhint for future studies. Microtubules are the target ofseveral antimitotic drugs including taxanes and the moreclassical colchicine-derived agents. Impairment of micro-tubule dynamics is causally linked to mitotic blockadeand is consistent with the ability of tivantinib to arrest cellcycle in G2/M.
Although these findings do not diminish the thera-peutic potential of tivantinib in any way, they do haveprofound implications in clinical oncology. The firstconsideration concerns interpretation of clinical results.So far, tivantinib has been tested clinically assuming thatit was a highly selective MET inhibitor. This assumptionled to testing the tivantinib–erlotinib association inNSCLC, where MET activity is known to mediate resis-tance to EGF receptor inhibitors (35). A first phase II trial(NCT00777309) did not show any benefit in progres-sion-free survival (17), while the MARQUEE Phase IIItrial involving almost 1,000 patients was prematurelydiscontinued due to futility (19). The data presented here
HGF LV or
Tpr-MET LV
MET
Inhibitor
No
drug
Other
TKI
Cytotoxic
agent
HepG2 cellsA
Empty
LV
MET
inhibitor
No
drug
Other
TKI
Cytotoxic
agent
HepG2 cellsB
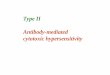
Figure 5. An engineered cell system 'poisoned' by MET kinase hyperactivation allows identification of MET-specific inhibitors. A, HepG2 humanhepatocarcinoma cells, that undergo growth arrest and apoptosis upon activation of the MET signaling pathway (33), are transduced with an engineeredlentiviral vector (LV) expressing HGF or Tpr-MET, a constitutively activated form of the MET kinase (red). LV-mediated expression of HGF or Tpr-METleads to growth arrest and cell death, unless cells are cultured with a MET inhibitor. Any other drug that is not a selective inhibitor of MET fails to rescue cellsurvival and growth. B, at the same time, HepG2 cells are also transduced with an empty LV as control (green) and are subjected to the same pharmacologictreatment. In this case, targeted agents—whether specific for MET or directed against other tyrosine kinases—do not affect cell proliferation or survival.However, if the drug tested has cytotoxic activity, empty LV-transduced cells die.
Tivantinib Displays MET-Independent Cytotoxic Activity
www.aacrjournals.org Clin Cancer Res; 19(9) May 1, 2013 2389
on April 17, 2021. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 26, 2013; DOI: 10.1158/1078-0432.CCR-12-3459

offer a new interpretation key for these results: thesetrials did not fail because MET is not a good target inlung cancer as it may be inferred, but because tivantinibis not a MET inhibitor. This notion is also crucial for thedesign of future clinical trials, as it raises some concernon the rationale for recruiting patients based on theirMET status.
A similar case of ‘mistaken identity’ recently involvediniparib (Sanofi-Aventis), a nicotinamide analogue testedclinically as a highly selective, noncompetitive poly-(ADP-ribose) polymerase (PARP) inhibitor. In a phaseII trial in triple-negative breast cancer, the iniparib-che-motherapy combination was associated with a significantimprovement in overall survival (36). However, theseresults could not be reproduced in a phase III trial,raising questions about the future of PARP inhibitionas a therapeutic strategy. Remarkably, in striking analogywith tivantinib, subsequent studies showed that iniparibis not a PARP inhibitor but a cytotoxic agent thatkills tumor cells by an unrelated molecular mechanism(37, 38). In the iniparib as in the tivantinib case, morerigorous preclinical analysis would have addressed thesedrugs toward a more appropriate clinical testing, pre-
venting failure, and misinterpretation of clinical trials(39).
It is not uncommon that antitumor agents are admin-istered to patients before knowing their mechanism ofaction. This is fine as long as their safety and efficacy isdetermined in unbiased clinical trials. However, theassumption that tivantinib is a selective MET inhibitorand not a cytotoxic agent may be misleading in thedevelopment of predictive biomarkers. In fact, whiletargeted agents are effective only in specific subsets oftumors displaying the appropriate genetic features, cyto-toxic agents aim at universal mechanisms of cell survivaland proliferation and, therefore, exert their activity largelyindependent of tumor genetics. On the other hand,acquired resistance to a cytotoxic agent is more likely todepend on induction of multidrug resistance and antia-poptotic mechanisms rather than on activation of alterna-tive oncogenic pathways like in the case of targeted agents.These aspects should be taken into account when searchingfor markers of response or resistance to tivantinib.
The findings presented in this study offer new perspec-tives of clinical development for this promising, well-tol-erated cytotoxic drug. Continuing to consider tivantinib as a
100 101 102 103-25
0
25
50
75
100
125Tpr-MET LV
Drug conc. (log nmol/L)
Ce
ll n
um
be
r (%
of
ctr
l)
100 101 102 103-25
0
25
50
75
100
125
Drug conc. (log nmol/L)
Ce
ll n
um
be
r (%
of
ctr
l)
Empty LV
100 101 102 103-25
0
25
50
75
100
125
Drug conc. (log nmol/L)
Ce
ll n
um
be
r (%
of
ctr
l)
HGF LV
JNJ-38877605
PHA-665752MET inhibitors
Semaxinib
Gefitinib
ImatinibOther TKIs
Staurosporine
Puromycin
Paclitaxel
Cytotoxics
Tivantinib
Figure 6. Tivantinib is a cytotoxicdrug and not a MET-targetedagent. The HepG2 systemwas used to compare thepharmacologic profile of tivantinib(black lines)with that of other drugsincluding MET kinase inhibitors(blue lines), drugs targeting othertyrosine kinases (green lines), andgeneric cytotoxic compounds (redlines). HepG2 cells weretransduced with a lentiviral vector(LV) expressing HGF, Tpr-MET,or no factor (empty LV). Followingtransduction, cells were culturedin the presence of increasingconcentrations (0–1,000 nmol/L)of the indicated drugs, and cellnumber was determined by astandard chemoluminescence-based ATP assay 10 days later.Cell number is expressed aspercentage relative to control,untransduced cells (CTRL). Valuesare the mean � SD of 3 sets ofexperiments conducted inquadruplicate. TKIs, tyrosinekinase inhibitors.
Basilico et al.
Clin Cancer Res; 19(9) May 1, 2013 Clinical Cancer Research2390
on April 17, 2021. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 26, 2013; DOI: 10.1158/1078-0432.CCR-12-3459

selective MET inhibitor may lead, on 1 hand, to the risk ofnot meeting the clinical end points that authentic METinhibitors are expected to achieve and, on the other, to thepotential subtraction of patients who could benefit fromMET inhibition from the proper treatment.
Disclosure of Potential Conflicts of InterestP. Michieli is a consultant/advisory board member of Metheresis SA and
arGEN-X BVBA. No conflicts of interest were disclosed by the other authors.
Authors' ContributionsConception and design: P. MichieliDevelopment of methodology: C. Basilico, S. Pennacchietti, E. Vigna, A.Bardelli, P. MichieliAcquisitionofdata (provided animals, acquired andmanagedpatients,provided facilities, etc.):C. Basilico, S. Pennacchietti, E. Vigna, C. Chiriaco,D. Valdembri, G. SeriniAnalysis and interpretation of data (e.g., statistical analysis, biosta-tistics, computational analysis): C. Basilico, S. Pennacchietti, E. Vigna, C.Chiriaco, A. Bardelli, D. Valdembri, G. Serini, P. MichieliWriting, review, and/or revision of the manuscript: C. Basilico, S.Pennacchietti, A. Bardelli, D. Valdembri, G. Serini, P. Michieli
Administrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): S. ArenaStudy supervision: A. Bardelli, G. Serini, P. Michieli
AcknowledgmentsThe authors thank Edward Garmey for providing ARQ197, Tim Perera for
supplying JNJ-38877605, Erica Lantelme for flow cytometric analysis, LivioTrusolino, Silvia Marsoni, and Paolo Comoglio for helpful discussion,Federica Di Nicolantonio for critical reading of the article, and Lara Fontanifor lentiviral vector particle preparation.
Grant SupportThis work was supported in part by the Italian Association for Cancer
Research (AIRC 2010 Special Program in Molecular Clinical Oncology 5%Project n. 9970 and AIRC 2012 IG grant n. 12798) and the FondazionePiemontese per la Ricerca sul Cancro-ONLUS (Intramural Grant 5% 2008).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received November 7, 2012; revised March 9, 2013; accepted March 11,2013; published OnlineFirst March 26, 2013.
References1. Nakamura T, Sakai K, Nakamura T, Matsumoto K. Hepatocyte growth
factor twenty years on: much more than a growth factor. J Gastro-enterol Hepatol 2011;26 Suppl 1:188–202.
2. Boccaccio C, Comoglio PM. Invasive growth: a MET-driven geneticprogramme for cancer and stem cells. Nat RevCancer 2006;6:637–45.
3. Birchmeier C, Birchmeier W, Gherardi E, Vande Woude GF. MET,metastasis, motility and more. Nat Rev Mol Cell Biol 2003;4:915–25.
4. Trusolino L, Comoglio PM. Scatter-factor and semaphorin receptors:cell signalling for invasive growth. Nat Rev Cancer 2002;2:289–300.
5. Li CJ, Ashwell AM, Hill J, Moussa MM, Munshi N. Compositions andmethods for treatment of cancer. US Patent 7,713,969 B2; publishedMay 11, 2010. Available online on the Patent Lenswebsite: http://www.patentlens.net/patentlens/patents.html?patnums=US_7713969
6. MunshiN,JeayS,LiY,ChenCR,FranceDS,AshwellMA,etal. ARQ197,a novel and selective inhibitor of the human c-MET receptor tyrosinekinase with antitumor activity. Mol Cancer Ther 2010;9:1544–53.
7. Smolen GA, Sordella R, Muir B, Mohapatra G, Barmettler A, ArchibaldH, et al. Amplification of MET may identify a subset of cancers withextreme sensitivity to the selective tyrosine kinase inhibitor PHA-665752. Proc Natl Acad Sci U S A 2006;103:2316–21.
8. McDermott U,SharmaSV,Dowell L,GreningerP,MontagutC, LambJ,et al. Identification of genotype-correlated sensitivity to selectivekinase inhibitors by using high-throughput tumor cell line profiling.Proc Natl Acad Sci U S A 2007;104:19936–41.
9. Bertotti A, Burbridge MF, Gastaldi S, Galimi F, Torti D, Medico E, et al.Only a subset of MET-activated pathways are required to sustainoncogene addiction. Sci Signal 2009;2:ra80.
10. Lutterbach B, Zeng Q, Davis LJ, Hatch H, Hang G, Kohl NE, et al. Lungcancer cell lines harboring MET gene amplification are dependent onMET for growth and survival. Cancer Res 2007;67:2081–8.
11. Barretina J, Caponigro G, StranskyN, Venkatesan K,Margolin AA, KimS, et al. The Cancer Cell Line Encyclopedia enables predictive model-ling of anticancer drug sensitivity. Nature 2012;483:603–7.
12. Garnett MJ, Edelman EJ, Heidorn SJ, Greenman CD, Dastur A, LauKW, et al. Systematic identification of genomic markers of drugsensitivity in cancer cells. Nature 2012;483:570–5.
13. Eathiraj S, Palma R, Volckova E, Hirschi M, France DS, Ashwell MA,et al. Discovery of a novel mode of protein kinase inhibition charac-terized by the mechanism of inhibition of human mesenchymal-epi-thelial transition factor (c-MET) protein autophosphorylation by ARQ197. J Biol Chem 2011;286:20666–76.
14. Giordano S, Ponzetto C, Di Renzo MF, Cooper CS, Comoglio PM.Tyrosine kinase receptor indistinguishable from the c-MET protein.Nature 1989;339:155–6.
15. Previdi S, AbbadessaG,Dal�oF, FranceDS,BrogginiM.Breast cancer-derived bonemetastasis canbe effectively reduced through specific c-MET inhibitor tivantinib (ARQ 197) and shRNA c-MET knockdown.MolCancer Ther 2012;11:214–23.
16. Sharma N, Adjei AA. In the clinic: ongoing clinical trials evaluating c-MET-inhibiting drugs. Ther Adv Med Oncol 2011;3 Suppl 2:S37–50.
17. Sequist LV, vonPawel J,GarmeyEG,AkerleyWL,BruggerW,Ferrari D,et al. Randomized phase II study of erlotinib plus tivantinib versuserlotinib plus placebo in previously treated non-small-cell lung cancer.J Clin Oncol 2011;29:3307–15.
18. Cepero V, Sierra JR, Corso S, Ghiso E, Casorzo L, Perera T, et al.METand KRAS gene amplification mediates acquired resistance to METtyrosine kinase inhibitors. Cancer Res 2010;70:7580–90.
19. Arqule/Daiichi-Sankyo world-wide news release: Arqule and DaiichiSankyo announce discontinuation of phase 3 MARQUEE clinical trialin non-small cell lung cancer. Published on Daiichi-Sankyo web siteon October 2, 2012. http://investors.arqule.com/releasedetail.cfm?ReleaseID=710618
20. Arena S, Pisacane A, Mazzone M, Comoglio PM, Bardelli A. Genetictargeting of the kinase activity of theMET receptor in cancer cells. ProcNatl Acad Sci U S A 2007;104:11412–7.
21. Galimi F, Torti D, Sassi F, Isella C, Cor�a D, Gastaldi S, et al.Genetic and expression analysis of MET, MACC1, and HGF inmetastatic colorectal cancer: response to MET inhibition in patientxenografts and pathologic correlations. Clin Cancer Res 2011;17:3146–56.
22. Follenzi A, Ailles LE, Bakovic S, Geuna M, Naldini L. Gene transfer bylentiviral vectors is limited by nuclear translocation and rescued byHIV-1 pol sequences. Nat Genet 2000;25:217–22.
23. Follenzi A, Naldini L. Generation of HIV-1 derived lentiviral vectors.Methods Enzymol 2002;346:454–65.
24. Longati P, Bardelli A, Ponzetto C, Naldini L, Comoglio PM. Tyro-sines 1234-1235 are critical for activation of the tyrosine kinaseencoded by the MET proto-oncogene (HGF receptor). Oncogene1994;9:49–57.
25. Ruco LP, Ranalli T, Marzullo A, Bianco P, Prat M, Comoglio PM, et al.Expression of MET protein in thyroid tumours. J Pathol. 1996;180:266–70.
26. Comoglio PM, Giordano S, Trusolino L. Drug development of METinhibitors: targeting oncogene addiction and expedience. Nat RevDrug Discov 2008;7:504–716.
27. Michieli P,MazzoneM, BasilicoC, Cavassa S, Sottile A, Naldini L, et al.Targeting the tumor and its microenvironment by a dual-functiondecoy MET receptor. Cancer Cell 2004;6:61–73.
Tivantinib Displays MET-Independent Cytotoxic Activity
www.aacrjournals.org Clin Cancer Res; 19(9) May 1, 2013 2391
on April 17, 2021. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 26, 2013; DOI: 10.1158/1078-0432.CCR-12-3459

28. Maggiora P, Lorenzato A, Fracchioli S, Costa B, Castagnaro M, ArisioR, et al. The RON and MET oncogenes are co-expressed in humanovarian carcinomas and cooperate in activating invasiveness. ExpCellRes 2003;288:382–9.
29. De Bacco F, Luraghi P, Medico E, Reato G, Girolami F, Perera T,et al. Induction of MET by ionizing radiation and its role in radio-resistance and invasive growth of cancer. J Natl Cancer Inst2011;103:645–61.
30. Christensen JG, SchreckR, Burrows J, Kuruganti P, Chan E, LeP, et al.A selective small molecule inhibitor of c-MET kinase inhibits c-MET-dependent phenotypes in vitro and exhibits cytoreductive antitumoractivity in vivo. Cancer Res 2003;63:7345–55.
31. Pacchiana G, Chiriaco C, Stella MC, Petronzelli F, De Santis R,GalluzzoM, et al. Monovalency unleashes the full therapeutic potentialof the DN-30 anti-MET antibody. J Biol Chem 2010;285:36149–57.
32. Petrelli A, Circosta P,Granziero L,MazzoneM, PisacaneA, Fenoglio S,et al. Ab-induced ectodomain shedding mediates hepatocyte growthfactor receptor down-regulation and hampers biological activity. ProcNatl Acad Sci U S A 2006;103:5090–5.
33. Tajima H, Matsumoto K, Nakamura T. Hepatocyte growth factor haspotent anti-proliferative activity in various tumor cell lines. FEBS Lett1991;291:229–32.
34. Peschard P, Park M. From Tpr-MET toMET, tumorigenesis and tubes.Oncogene 2007;26:1276–85.
35. Hammerman PS, J€anne PA, Johnson BE. Resistance to epidermalgrowth factor receptor tyrosine kinase inhibitors in non–small cell lungcancer. Clin Cancer Res 2009;15:7502–9.
36. O'Shaughnessy J, Osborne C, Pippen JE, Yoffe M, Patt D, Rocha C,et al. Iniparib plus chemotherapy in metastatic triple-negative breastcancer. N Engl J Med 2011;364:205–14.
37. Liu X, Shi Y, Maag DX, Palma JP, Patterson MJ, Ellis PA, et al. Iniparibnonselectively modifies cysteine-containing proteins in tumor cellsand is not abona fidePARP inhibitor. ClinCancerRes2012;18:510–23.
38. Patel AG,DeLorenzoSB, FlattenKS,PoirierGG,KaufmannSH.Failureof iniparib to inhibit poly(ADP-Ribose) polymerase in vitro. Clin CancerRes 2012;18:1655–62.
39. Ledford H. Drug candidates derailed in case of mistaken identity.Nature 2012;483:519.
Basilico et al.
Clin Cancer Res; 19(9) May 1, 2013 Clinical Cancer Research2392
on April 17, 2021. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 26, 2013; DOI: 10.1158/1078-0432.CCR-12-3459

2013;19:2381-2392. Published OnlineFirst March 26, 2013.Clin Cancer Res Cristina Basilico, Selma Pennacchietti, Elisa Vigna, et al. Independent of Its Ability to Bind METTivantinib (ARQ197) Displays Cytotoxic Activity That Is
Updated version
10.1158/1078-0432.CCR-12-3459doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2013/04/05/1078-0432.CCR-12-3459.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/19/9/2381.full#ref-list-1
This article cites 37 articles, 17 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/19/9/2381.full#related-urls
This article has been cited by 18 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/19/9/2381To request permission to re-use all or part of this article, use this link
on April 17, 2021. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 26, 2013; DOI: 10.1158/1078-0432.CCR-12-3459