Embed Size (px)
Citation preview

Title:Esophageal motor disorders are frequentduring pre and post lung transplantation.Can they influence lung rejection?
Authors:Constanza Ciriza de los Ríos, FernandoCanga Rodríguez-Valcárcel, Alicia de PabloGafas, Isabel Castel de Lucas, David LoraPablos, Gregorio Castellano Tortajada
DOI: 10.17235/reed.2018.5263/2017Link: PubMed (Epub ahead of print)
Please cite this article as:Ciriza de los Ríos Constanza, CangaRodríguez-Valcárcel Fernando, de PabloGafas Alicia, Castel de Lucas Isabel, LoraPablos David, Castellano Tortajada Gregorio.Esophageal motor disorders are frequentduring pre and post lung transplantation.Can they influence lung rejection? . Rev EspEnferm Dig 2018. doi:10.17235/reed.2018.5263/2017.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to ourcustomers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form.Please note that during the production process errors may be discovered which could affect thecontent, and all legal disclaimers that apply to the journal pertain.

OR 5263
Esophageal motor disorders are frequent during pre and post lung transplantation.
Can they influence lung rejection?
Constanza Ciriza-de-los-Ríos1, Fernando Canga-Rodríguez-Valcárcel1, Alicia de-Pablos-
Gafas1, Isabel Castel-de-Lucas1, David Lora-Pablos2 and Gregorio Castellano-Tortajada1
1Department of Gastroenterology. Hospital Universitario 12 de Octubre. Madrid, Spain.2Clinical Research Unit. IMAS12-CIBERESP. Hospital Universitario 12 de Octubre.
Madrid, Spain
Received: 21/09/2017
Accepted: 02/01/2018
Correspondence: Constanza Ciriza-de-los-Ríos. Department of Gastroenterology.
Hospital Universitario 12 de Octubre. Av. de Córdoba s/n. 28041 Madrid, Spain
e-mail: [email protected]
ABSTRACT
Background: lung transplantation (LTx) is a viable option for most patients with end-
stage lung diseases. Esophageal motor disorders (EMD) are frequent in candidates for
LTx, but there is very little data about changes in esophageal motility post-LTx.
Aim: the aim of our study was to assess esophageal motor disorders by high resolution
manometry (HRM) both pre-LTx and six months post-LTx in patients with and without
organ rejection.
Study: HRM (Manoscan®) was performed in 57 patients both pre-LTx and six months
post-LTx. HRM plots were analyzed according to the Chicago classification 3.0.
Results: EMD were found in 33.3% and in 49.1% of patients pre-LTx and post-LTx,
respectively, and abnormal peristalsis was more frequently found post-LTx (p = 0.018).
Hypercontractile esophagus was frequently found post-LTx (1.8% and 19.3% pre-LTx
and post-LTx, respectively). Esophagogastric junction (EGJ) morphology changed
significantly pre-LTx and post-LTx; type I (normal) was more frequent post-LTx (63-2%

and 82.5% respectively, p = 0.007). EMD were more frequent post-LTx in both the non-
rejection and rejection group, although particularly in the rejection group (43.2% and
69.2% respectively, p = 0.09). EMD such as distal spasm, hypercontractile esophagus
and EGJ outflow obstruction were also observed more frequently post-LTx in the
rejection group.
Conclusion: significant changes in esophageal motility were observed pre-LTx and
particularly post-LTx; hypercontractile esophagus was a frequent EMD found post-LTx.
EMD were more frequent in the group of patients that experienced organ rejection
compared to the non-rejection group. EMD leading to an impaired esophageal
clearance should be considered as an additional factor that contributes to LTx failure.
Key words: Esophageal motility disorders. High resolution manometry. Lung
transplantation. Hypercontractile esophagus. Lung rejection.
INTRODUCTION
Lung transplantation (LTx) is a viable option for most patients with end-stage lung
diseases (1). Transplant failure is frequently caused by the development of
bronchiolitis obliterans syndrome (BOS), a devastating complication that accounts for
30% of all deaths within a three-year period post transplantation (1). Risk factors
associated with the development of BOS include cytomegalovirus infection and
positive antibodies to class I HLA. Gastroesophageal reflux disease (GERD) is associated
with other pulmonary diseases such as asthma, cystic and pulmonary fibrosis and
obstructive sleep apnea syndrome (2). Therefore, pH, bile acid and trypsin levels in
GERD have been studied as biomarkers for chronic allograft dysfunction (3). GERD is
also associated with esophageal motor disorders (EMD), although it is not clear if GERD
is the cause or the consequence of the esophageal motility impairment (4). Although
GERD has been extensively studied as a factor associated with LTx rejection, there are
some gaps with regard to the potential contribution to the abnormal motility of the
esophagus. Esophageal dysmotility can impair esophageal clearance and could favor
retrograde movement of the esophageal content to the pharyngeal area. Therefore,
the refluxate material is not necessarily the acid that comes from the stomach. In this

respect, experimental studies performed in rat lung transplant models (WKY-to-F344)
showed that both acid (pH 2.5) and neutralized acid pH (pH 7.4) caused lesions
consistent with obliterative bronchiolitis (5). Findings show that impaired esophageal
peristalsis and hypotensive lower esophageal sphincter (LES) are more prevalent in LTx
candidates with GERD (6) and hypercontractile motor disorders have been reported
post-LTx (7). Patients who have undergone a bilateral lung transplantation or a re-
transplantation have a more pronounced delay in gastric emptying, impaired
esophageal motility and delayed esophageal acid clearance as compared to patients
who had undergone a unilateral lung transplantation (8).
Esophageal high-resolution manometry (HRM) represents an unquestionable advance
in esophageal manometry and allows a better characterization of EMD and
esophagogastric junction (EGJ) morphology (9). The Chicago classifications include the
new data that HRM provides for the study of EMD (10).
The aim of the study was to assess esophageal motor disorders by high resolution
manometry (HRM) both pre-LTx and six months post-LTx, in patients with and without
organ rejection.
MATERIAL AND METHODS
Patients
This was a single-center retrospective analysis of a prospectively-collected database of
57 consecutive patients over 18 years of age referred to our esophageal motility
laboratory both pre-LTx and six months post-LTx, between October 2009 and
November 2016. Inclusion criteria were: a) signed informed consent; 2) a minimum
age of 18 years; and 3) indication for LTx. The exclusion criteria was: a) patients who
refused to sign the informed consent.
Gastrointestinal (GI) symptoms were evaluated both pre and six months post-LTx using
the modified DeMeester Questionnaire that evaluated heartburn, regurgitation and
dysphagia. These were scored between 0-3 (0: none; 1: mild; 2: moderate; 3: very
severe) (11).
Acute rejection was defined as a clinical, radiological or functional episode that was
compatible with a histological demonstration according to the international

classification of the Lung Rejection Study Group, or without histological demonstration
but with a response to the specific treatment for rejection (12). Chronic rejection was
defined according to the international guidelines. This was defined as a drop in forced
expiratory volume in one second (FEV1) < 80% of the maximum volume achieved after
transplant. This was on the condition that other etiologies such as infections, airway
stenosis or native lung complications in single-lung transplant recipients were excluded
(12). Chronic rejection can present at any time after the transplant.
The study was performed following the protocol proposed by the Lung Transplant
Program approved by the Hospital Universitario 12 de Octubre.
HRM protocol
HRM was performed both pre-LTx and six months post-LTx in all patients according to
the protocol established at our hospital. HRM was performed using a solid-state
manometric assembly with 36 circumferential sensors with an outer diameter of 4.2
mm spaced at 1-cm intervals (Given Scientific Instruments Inc., Los Angeles, CA, USA).
The transducers were calibrated at 0 and 300 mmHg by applying an external pressure
prior to recording. The previously described standard protocol was used (13). All
subjects were studied following an overnight fast and after discontinuing medication
within 48 hours (except for immunosuppressant therapy post-LTx) that could affect the
examination results. However, all patients received a double dose of proton pump
inhibitors (PPI) post-LTx as per protocol and when the HRM was performed six months
post-LTx. After calibrating the equipment, the recording probe was introduced nasally
with the patient in the supine position (14). Subsequently, the recording was started
with a 30 second basal period (landmark) with no deglutitions in order to obtain the
sphincter pressures, followed by ten deglutitions of 5 ml every 20 seconds. If the first
landmark were not satisfactory, a second landmark was performed at the end of the
study. Furthermore, if the patient swallowed twice or the interval between swallows
was under 20 seconds, these deglutitions were not considered as valid for the analysis.
The final analysis required ten valid deglutitions (15).
24h pH-monitoring protocol

Twenty-four hours ambulatory pH-monitoring without PPI was carried out pre-LTx. The
sensor was placed 5 cm above the upper limit of the lower esophageal sphincter (LES)
determined by HRM. The study catheter was attached to an ambulatory recorder
(Matla Systems Inc, Madrid, Spain). Post-LTx, pH-monitoring was performed with a
double dose of PPI as per protocol (Lung Transplantation Unit). The proximal sensor
was placed 5 cm above the upper limit of the LES and the distal sensor on the stomach.
Patients were encouraged to carry out their normal diet and daily activities.
Data analysis
Manometric data were analyzed using the Mano ViewTM analysis software version 2.1
(Given Scientific Instruments Inc. Los Angeles, CA, USA) and reanalyzed with the new
version 3.3. Two experienced researchers performed HRM and reviewed manually all
the deglutitions of each patient. Finally, a manometric diagnosis was reached using the
analysis algorithm recommended by the Chicago Classification. Esophageal motor
function (10) was evaluated according to the Chicago Classification v. 3.0 (10).
Subsequently, the EMD were classified into the following subtypes: normal, achalasia,
hypercontractile esophagus, distal esophageal spasm, absent and ineffective peristalsis
(16).
The following manometric measurements were analyzed: basal pressure of the LES
(normal values: 10-35 mmHg; minimum pressure obtained with the sleeve device)
(17), integrated relaxation pressure (IRP) (four seconds IRP normal values [IRP4s]: < 15
mmHg) (10), pressurization presence or absence (9), distal contractile integral (DCI)
(normal values: 450-8,000 mmHgm.s.cm) (10), and distal latency (DL) (normal values: >
4.5 s) (10).
The normal values (thresholds) applied were based on the Chicago Classification,
except for the cut-offs for LES resting pressure, as this was not considered in this
classification. LES was considered as normal (basal pressure was between 10 and 35
mmHg and IRP-4s < 15 mmHg), hypotensive (basal LES pressure was < 10 mmHg and
IRP < 15 mmHg) and hypertensive (basal pressure ≥ 35 and IRP < 15 mmHg).
HRM diagnosis was divided into the following groups: normal, ineffective peristalsis (≥
50% weak and failed contractions; DCI < 450 mmHg.cm.s and DCI < 100 mmHg.cm.s

respectively), absent peristalsis (100% failed contraction and IRP < 15 mmHg), EGJ
outflow obstruction (EGJOO) (IRP-4s ≥ 15 mmHg), achalasia (100% of failed
contractions and IRP ≥ 15 mmHg), distal esophageal spasm (≥ 20% of premature
contractions; distal latency < 4.5 s) and hypercontractile esophagus (≥ 20% of
hypercontractile contractions; DCI ≥ 8000 mmHg.cm.s) (10).
EGJ morphology was classified depending on the distance between the LES and crural
diaphragm (CD) as follows: type I (normal), for distances < 1 cm; type II, for distances
between 1-2 cm; and type III (hiatal hernia), for distances over 2 cm (10,18).
Patients were classified as having GERD when the total time at pH < 4 was over 4.5%
according to the DeMeester reference values when the procedure was performed
without PPI (19) and 1.6% when performed with PPI (20). The association with reflux
symptoms was not used in the final diagnosis for GERD as most patients were
asymptomatic. pH data were not compared pre-LTx and post-LTx.
Statistical analysis
HRM quantitative data were described using the mean and confidence intervals (CI) for
parametric variables and the median and interquartile range (IQR) for non-parametric
variables. Qualitative data were expressed as absolute frequencies. Acute and chronic
rejection patients were grouped for analysis purposes. Data were stratified for patients
as rejection and non-rejection and the distribution was compared with the Mann-
Whitney U test (non-normal distribution) or Chi-squared test (categorical variables) or
Fisher’s exact test, as appropriate. The statistical significance of paired differences
between pre-LTx and post-LTx HRM data was calculated using the Wilcoxon signed
rank test (non-normal distribution) or McNemar’s test (categorical variables). The data
analysis was generated using the IBM SPSS statistics 22 software.
RESULTS
Fifty-seven patients were included and analyzed both pre-LTx and post-LTx. Forty-four
(77.2%) did not experience a rejection, nine (15.8%) had acute rejection and four (7%),
chronic rejection. Most patients had obstructive type end-stage lung disease both in
the non-rejection and rejection groups (53.2% and 46.2%). GI symptoms were very

infrequent and the symptom score was similar in both the pre-LTx and post-LTx
groups. Overall, 17.5% and 15.8% of patients had symptoms pre-LTx and post-LTx,
respectively; heartburn and regurgitation were the most frequent. None of the
patients had dysphagia either pre-LTx or six months post-LTx. However, two patients
presented with dysphagia during follow up after the initial six month period. Patient
characteristics are shown in table 1.
Analyses (pre-LTx vs post-LTx)
HRM parameters and diagnosis are shown in table 2. EMD were found in 33.3% and
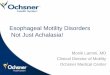
49.1% of patients pre-LTx and post-LTx respectively (p = 0.018); hypercontractile
esophagus was the most relevant EMD post-LTx (p = 0.018). Accordingly, DCI was
significantly higher post-LTx (p < 0.001) (Fig. 1). Of the eleven patients with
hypercontractile esophagus post-LTx, three (27.3%) had abnormal pH monitoring, two
(18.2%) had EGJOO and one (9%) had abnormal pH monitoring with EGJOO. There was
no evidence of other possible causes in the remaining five (45.5%) cases.
An EGJ morphology change was observed pre-LTx and post-LTx; type I (normal) was
more predominant post-LTx (63.2% and 82.5% respectively, p = 0.007). Accordingly,
EGJ length was shorter post-LTx due to a decrease in the intrathoracic length.
Hypotensive LES was more frequent pre-LTx than post-LTx (33.3% and 17.5%
respectively, p = 0.017) (Table 2). There were no differences in the frequency of EMD
according to the type of LTx (bilateral or unilateral); 19 (51.4%) patients had bilateral
LTx and ten (50%) patients with unilateral had normal peristalsis (NS).
Analysis rejection vs non-rejection group
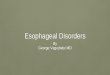
EMD were more frequent post-LTx in both the non-rejection and rejection groups, but
particularly in the rejection group (43.2% and 69.2%, respectively; p = 0.09).
Hypercontractile esophagus was observed in 23% of the cases post-LTx in the rejection
group (Table 3). Accordingly, DCI tended to be higher in the rejection group (Fig. 2).
EGJ was more frequently classed as type I (normal) in the non-rejection compared to
the rejection group (86.4% vs 69.2% respectively, NS) (Table 3).

The HRM results were as follows in the nine patients with acute rejection, three cases
had no abnormalities, three had hypercontractile esophagus (one of them had also
EGJOO), one had EGJOO and two, distal spasm. The three patients with
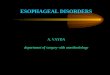
hypercontractile esophagus still had the same disorder one year post-LTx. Two of these
patients presented with dysphagia during follow up after six months and were treated
with endoscopic botulinum toxin injection (Fig. 3). In addition, four patients had
chronic rejection, two had weak peristalsis and one had EGJOO.
DISCUSSION
Patients with end stage lung disease pre-LTx have a high prevalence of EMD and
hypotensive LES with a reported frequency of around 76.6% using HRM (1). We found
a similar frequency in our series of 66.6% (including EMD and hypotensive LES).
According to the Chicago Classification 3.0, the frequency of EMD pre-LTx in our series
was 33.3%, and these alterations increased post-LTx up to 49.1%. The most frequent
disorders found were ineffective peristalsis, hypercontractile esophagus and EGJOO.
Previous studies performed with water perfused manometry have reported dysmotility
post-LTx in up to 44% of the patients. Although the results are not strictly comparable
between conventional and HRM, the authors found similar findings, including
ineffective motility and nutcracker esophagus (21). In addition, we found significant
changes in EGJ morphology pre-LTx and post-LTx; more type I (normal) EGJ was
observed post-LTx, particularly in the non-rejection group. These changes could be
related to the surgical changes and the improvement of pulmonary function. However,
these findings were not present in the rejection group (Table 3).
There is some evidence that demonstrates a link between GERD and LTx rejection
(8,22,23) that can occur early post-LTx (21), but the potential implication of esophageal
dysmotility in LTx rejection has not yet been clarified. The importance of EGJOO for
chronic rejection has been recently reported (24). In our series, EGJOO was observed
pre-LTx in five patients, two related with abnormal acid reflux. The disorder persisted
post-LTx in the same five patients and only one had abnormal pH-monitoring. When
the data was analyzed considering the rejection vs non-rejection group, EGJOO was
more frequent in the rejection group. On the other hand, hypercontractile esophagus

was diagnosed more frequently than expected in the post-LTx group, which was 19.3%
(18.2% in the non-rejection and 23% in the rejection group).
The physiopathology of hypercontractile esophagus remains unclear and different
hypotheses have been suggested, including mechanical EGJOO, occurrence secondary
to reflux disease, primary esophageal muscle hypercontractility (25) and eosinophilic
infiltration into the muscularis propria (26). In this regard, EMD was observed in one
patient four weeks post-LTx, who nevertheless recovered without any specific
treatment besides PPI (7).
In our series, all the patients received double doses of PPI as per protocol post-LTx and
HRM was performed after six months. Therefore, the disorder was not corrected with
PPI use. Furthermore, the small group of patients with complications post-LTx and
EMD were followed up over six months and the disorder persisted in all cases.
Therefore, we do not consider this as a transient problem. It was not possible to clarify
the etiology of the disorder in 45.5% of the patients. In this respect, and according to
previous reports (25), the disorder could have been initiated by neuromuscular stress
induced by surgical trauma and perhaps, complicated by partial vagotomy during LTx
leading to esophageal dysmotility. Some medications such as azithromycin can
influence esophageal motility (27), but none of the patients were under the effects of
this medication during the procedure as this treatment was stopped at least 48 hours
previously.
The mechanism could be related to abnormal acid reflux or EGJOO in the remaining
54.5% of patients. An abnormal pH monitoring result was found in 27.3% of cases.
EGJOO was a possible mechanism in 18.2% of cases with hypercontractile esophagus,
and abnormal GERD was also found in one of these cases. Therefore, some of the
complications post-LTx could be related to GERD and others could be a consequence of
retained material in the esophagus due to an impaired esophageal clearance. A very
recent finding supports our theory, namely, that poor esophageal clearance is due to
an abnormal post-reflux swallow-induced peristaltic wave index associated with
obstructive chronic lung allograft dysfunction (24). PPI treatment is necessary in these
types of patients due to the high prevalence of GERD, although it would not be useful
to prevent the aspiration of esophageal content. Even though antireflux surgery has

been demonstrated to be safe post-LTx and leads to a stabilization of lung function in
patients with reflux, there is no definitive data supporting the hypothesis that it
improves the survival rate (28). On the other hand, antireflux surgery has not
prevented acute rejection episodes (28). Although some other factors can influence
rejection, it is important to appreciate that esophageal dysmotility which can impair
bolus transit, may also contribute to LTx failure.
The main limitation of our study is the small number of patients in the rejection group,
although we still observed significant changes pre-LTx and post-LTx and between the
rejection vs non-rejection group. Another limitation is the fact that HRiM and 24h
pH/impedance was not performed in all of the patients.
In conclusion, significant changes in esophageal motility can be observed pre-LTx and
particularly post-LTx; hypercontractile esophagus is a frequent EMD. EMD were more
frequent in the rejection group compared to the non-rejection group. Esophageal
motility alterations leading to impaired esophageal clearance should be considered as
another factor that might contribute to LTx failure.
REFERENCES
1. Basseri B, Conklin JL, Pimentel M, et al. Esophageal motor dysfunction and
gastroesophageal reflux are prevalent in lung transplant candidates. Ann Thorac Surg
2010;90(5):1630-6. DOI: 10.1016/j.athoracsur.2010.06.104
2. Fisichella PM, Jalilvand A. The role of impaired esophageal and gastric motility
in end-stage lung diseases and after lung transplantation. J Surg Res 2014;186(1):201-
6. DOI: 10.1016/j.jss.2013.09.023
3. Berastegui C, Roman J, Monforte V, et al. Biomarkers of pulmonary rejection.
Transplant Proc 2013;45(9):3163-9. DOI: 10.1016/j.transproceed.2013.06.013
4. Ciriza de los Ríos C, García Menéndez L, Díez Hernández A, et al. Motility
abnormalities in esophageal body in GERD: are they truly related to reflux? J Clin
Gastroenterol 2005;39(3):220-3. DOI: 10.1097/01.mcg.0000152780.76524.a9
5. Tang T, Chang JC, Xie A, et al. Aspiration of gastric fluid in pulmonary allografts:
effect of pH. J Surg Res 2013;181(1):e31-8. DOI: 10.1016/j.jss.2012.06.036

6. Sweet MP, Herbella FA, Leard L, et al. The prevalence of distal and proximal
gastroesophageal reflux in patients awaiting lung transplantation. Ann Surg
2006;244(4):491-7. DOI: 10.1097/01.sla.0000237757.49687.03
7. Khan MQ, Nizami IY, Khan BJ, et al. Lung transplantation triggered “jackhammer
esophagus”: a case report and review of literature. J Neurogastroenterol Motil
2013;19(3):390-4. DOI: 10.5056/jnm.2013.19.3.390
8. Fisichella PM, Davis CS, Shankaran V, et al. The prevalence and extent of
gastroesophageal reflux disease correlates to the type of lung transplantation. Surg
Laparosc Endosc Percutan Tech 2012;22(1):46-51. DOI:
10.1097/SLE.0b013e31824017d4
9. Ciriza de los Rios C, Canga Rodríguez-Valcárcel F, Castel de Lucas I, et al. How
useful is esophageal high resolution manometry in diagnosing gastroesophageal
junction disruption: causes affecting this disruption and its relationship with
manometric alterations and gastroesophageal reflux. Rev Esp Enferm Dig
2014;106(1):22-9. DOI: 10.4321/S1130-01082014000100004
10. Kahrilas PJ, Bredenoord A, Fox M, et al; International High Resolution
Manometry Working Group. The Chicago Classification of esophageal motility
disorders, v3.0. Neurogastroenterol Motil 2015;27(2):160-74.
11. DeMeester TR , Lafontaine E, Joelsson BE, et al. Relationship of a hiatal hernia
to the function of the body of the esophagus and the gastroesophageal junction. J
Thorac Cardiovasc Surg 1981;82:547-58.
12. Stewart S, Fishbein MC, Snell GI, et al. Revision of the 1996 working formulation
for the standardization of nomenclature in the diagnosis of lung rejection. J Heart Lung
Transplant 2007;26(12):1229-42. DOI: 10.1016/j.healun.2007.10.017
13. Bredenoord AJ, Hebbard G. Technical aspects of clinical high-resolution
manometry studies. Neurogastroenterol Motil 2012;24(Suppl 1):5-10. DOI:
10.1111/j.1365-2982.2011.01830.x
14. Ciriza-de-Los-Ríos C, Canga-Rodríguez-Valcárcel F, Lora-Pablos D, et al. How the
body position can influence high-resolution manometry results in the study of
esophageal dysphagia and gastroesophageal reflux disease. J Neurogastroenterol Motil
2015;21(3):370-9. DOI: 10.5056/jnm14110

15. Roman S, Kahrilas PJ, Boris L, et al. High-resolution manometry studies are
frequently imperfect but usually still interpretable. Clin Gastroenterol Hepatol
2011;9(12):1050-5. DOI: 10.1016/j.cgh.2011.08.007
16. Ruiz de León San Juan A, Ciriza de Los Ríos C, Pérez de la Serna Bueno J, et al.
Practical aspects of high resolution esophageal manometry. Rev Esp Enferm Dig
2017;109(2):91-105.
17. Fox MR, Bredenoord A. Oesophageal high-resolution manometry: moving from
research into clinical practice. Gut 2008;57:405-23. DOI: 10.1136/gut.2007.127993
18. Pandolfino JE, Ghosh SK, Zhang Q, et al. Quantifying EGJ morphology and
relaxation with high-resolution manometry: a study of 75 asymptomatic volunteers.
Am J Physiol Gastrointest Liver Physiol 2006;290(5):G1033-40. DOI:
10.1152/ajpgi.00444.2005
19. Bodger K, Trudgill N. Guidelines for oesophageal manometry and pH
monitoring. Guidelines in Gastroenterology. London: British Society of
Gastroenterology; 2006. pp. 1-11.
20. Kuo B, Castell DO. Optimal dosing of omeprazole 40 mg daily: effects on gastric
and oesophageal pH and serum gastrin in healthy controls. Am J Gastroenterol
1996:1532-8.
21. Griffin SM, Robertson AG, Bredenoord AJ, et al. Aspiration and allograft injury
secondary to gastroesophageal reflux occur in the immediate post-lung
transplantation period (prospective clinical trial). Ann Surg 2013 ;258(5):705-
11;discussion 11-2. DOI: 10.1097/SLA.0b013e3182a6589b
22. Castor JM, Wood RK, Muir AJ, et al. Gastroesophageal reflux and altered
motility in lung transplant rejection. Neurogastroenterol Motil 2013;22(8):841-50. DOI:
10.1111/j.1365-2982.2010.01522.x
23. Blondeau K, Mertens V, Vanaudenaerde BA, et al. Gastro-oesophageal reflux
and gastric aspiration in lung transplant patients with or without chronic rejection. Eur
Respir J 2008;31(4):707-13. DOI: 10.1183/09031936.00064807
24. Tangaroonsanti A, Lee AS, Crowell MD, et al. Impaired esophageal motility and
clearance post-lung transplant: risk for chronic allograft failure. Clin Transl
Gastroenterol 2017;8(6):e102. DOI: 10.1038/ctg.2017.30

25. Roman S, Kahrilas P. Management of spastic disorders of the esophagus.
Gastroenterol Clin North Am 2013;42(1):27-43. DOI: 10.1016/j.gtc.2012.11.002
26. Sato H, Takeuchi M, Takahashi K, et al. Nutcracker and jackhammer esophagus
treatment: a three-case survey, including two novel cases of eosinophilic infiltration
into the muscularis propria. Endoscopy 2015;47(9):855-7. DOI: 10.1055/s-0034-
1391985
27. Jafari J, Yazaki E, Woodland P, et al. Effect of azithromycin on esophageal
hypomotility (EH) and prediction of response by esophageal stimulations tests during
high resolution manometry. Gastroenterology 2015;148(4):S-75. DOI: 10.1016/S0016-
5085(15)30264-X
28. Gulack BC, Meza JM, Lin SS, et al. Reflux and allograft dysfunction: is there a
connection? Thorac Surg Clin 2015;25(1):97-105. DOI: 10.1016/j.thorsurg.2014.09.006

Table 1. Patient characteristics pre-LTx and post-LTx according to the rejection vs
non-rejection groups
Clinical data Non-rejection (n =
44)
Rejection (n =
13)
p-
value
Age (mean [CI 95%], yr)
Pre-LTx
Post-LTx
52.6 (41.7-63.5)
57.4 (46.4-68.3)
55.1 (50.2-59.8)
57.9 (53.1-62.8)
0.962
0.505
Male (n [%]) 28 (49.1%) 8 (61.5%) 0.890
BMI (mean; kg/m2)
Pre-LTx
Post-LTx
24.6 (22.1-27)
24.7 (21.5-27.8)
26.3 (23.9-28.6)
35.7 (23.5-27.9)
0.024
0.025
Abdominal perimeter (mean; cm)
Pre-LTx
Post-LTx
94.5 (88.7-100.2)
92.3 (82.9-101.5)
95.2 (89.6-
100.7)
94.8 (89.1-
100.6)
0.487
0.189
LTx indication (n [%])
Obstructive
COPD
Emphysema
Cystic fibrosis
Bronchiectasis
Fibro emphysema
Restrictive
Scleroderma
Idiopathic pulmonary fibrosis
Pulmonary hypertension
Others (histiocytosis X, etc.)
23 (52.3%)
5 (21.7%)
9 (39.1%)
5 (21.7%)
1 (4.4%)
3 (13%)
13 (29.5%)
1 (7.7)
12 (92.3%)
4 (9.1%)
4 (9.1%)
6 (46.2%)
6 (100%)
0
0
0
0
4 (30.8%)
4 (100%)
0
3 (23%)
0
0.414
DeMeester score (mean)
Pre-LTx 2.8 (0.9-4.5) Nd

Post-LTx 1.9 (0.1-3.6) Nd
GI and extraesophageal symptoms
pre-LTx
None
Heartburn
Heartburn and regurgitation
Hoarnesses
Chest pain
Cough
34 (77.3%)
4 (9.1)
3 (6.8%)
1 (2.3%)
1 (2.3%)
1(2.3%)
13 (100%)
0.611
GI and extraesophageal symptoms
post-LTx
None
Heartburn
Heartburn and regurgitation
Hoarnesses
Chest pain
Cough
36 (81.8%)
3 (6.8%)
2 (4.5%)
0
2 (4.5%)
1 (2.3%)
12 (92.3%)
0
0
0
0
1 (7.7%)
0.318
pH-monitoring pre-LTx*
Normal
Abnormal
Not performed
31 (70.5)
11 (25%)
2 (4.5%)
5 (38.5%)
8 (61.5%)
0
0.019
pH-monitoring post-LTx*
Normal
Abnormal
Not performed
31 (70.5%)
9 (20.5%)
4 (9%)
10 (76.9%)
3 (23.1%)
0
0.966
LTx type (n [%])
Bilateral
Right lung
Left lung
28 (63.6%)
12 (27.3%)
4 (9.1%)
9 (69.2%)
3 (23.1%)
1 (7.7%)
0.933
BMI: body mass index; LTx: lung transplantation; GI: Gastrointestinal; Nd: no data
(patients did not report symptoms). Statistical method: Mann-Whitney U, Chi-squared

test. *Double channel esophageal pH monitoring pre-LTx was performed without PPI
and double channel esophago-gastric pH monitoring post-LTx, with PPI as per protocol.
pH data pre-LTx and post-LTx were not compared.

Table 2. HRM parameters, EGJ morphology and EMD diagnosis pre-LTx and six
months post-LTx
HRM parameter Pre-LTx
Median (IQR)
Post-LTx
Median (IQR)
p-value
LES pressure (mmHg) 11.4 (6.9-18.9) 15.8 (10.7-26.3) < 0.001
IRP (mmHg) 6.9 (3.3-11.5) 7.4 (4.9-12.8) 0.324
EGJ total length (cm) 3.9 (3.4-4.2) 3.5 (3.3-4.1) 0.044
EGJ abdominal length (cm) 2.1 (1.8-2.5) 2.1 (1.9-2.7) 0.677
EGJ thoracic length (cm) 1.6 (1.3-2.3) 1.4 (1.1-1.7) 0.004
DCI (mmHg.cm.s) 1,503 (782.8-2,647.5) 2,559.8 (1,523.2-4,593) < 0.001
Distal latency (s) 6.3 (6-7.3) 7 (6-7.7) 0.029
Intrabolus pressure (mmHg) 15.4 (13-20.7) 17.8 (13.8-24.4) 0.155
LES basal pressure (n, %)
Normal
Hypotensive
Hypertensive
37 (65%)
19 (33.3%)
1 (1.7%)
42 (73.7%)
10 (17.5%)
5 (8.8%)
0.017
EGJ morphology (n, %)
Type I
Type II
Type III
36 (63.2%)
19 (33.3%)
2 (3.5%)
47 (82.5%)
10 (17.5%)
0
0.007
Diagnosis (n, %)
Normal
EMD
Ineffective peristalsis
Absent peristalsis
Hypercontractile
esophagus*
Distal spasm
EGJOO
Achalasia
38 (66.7%)
19 (33.3%)
6 (10.5%)
4 (7%)
1 (1.8%)
3 (5.3%)
5 (8.8%)
0
29 (50.9%)
28 (49.1%)
9 (15.8%)
0
11 (19.3%)
3 (5.3%)
5 (8.8%)
0
0.018

HRM: high-resolution manometry; LES: lower esophageal sphincter; IRP: integral
relaxation pressure; EGJ: esophagogastric junction; DCI: distal contractile integral;
EGJOO: esophagogastric junction outflow obstruction; IQR: interquartile range.
Statistical methods: Wilcoxon signed rank test and McNemar’s test. *Two patients
with hypercontractile esophagus also had EGJOO post-LTx.

Table 3. HRM results with regard to the rejection vs non-rejection group pre-LTx and
six months post-LTx
HRM results Non-rejection (n = 44) Rejection (n = 13)
Pre-LTx Post-LTx* Pre-LTx Post-LTx*
EGJ morphology (n, %)
Type I
Type II
Type III
27 (61.4%)
16 (36.4%)
1 (2.2%)
38 (86.4%)
6 (13.6%)
0
9 (69.2%)
3 (23.1%)
1 (7.7%)
9 (69.2%)
4 (30.8%)
0
Diagnosis (n, %)
Normal
EMD
29 (65.9%)
15 (34.1%)
25 (56.8%)*
19 (43.2%)
9 (69.2%)
4 (30.8%)
4 (30.8%)*
9 (69.2%)
Type of EMD
Ineffective peristalsis
Absent peristalsis
Hypercontractile esophagus
Distal spasm
EGJOO
Achalasia
6 (13.6%)
3 (6.8%)
0 (0%)
2 (4.5%)
4 (9.1%)
0
7 (15.9%)
0
8 (18.2%)
1 (2.3%)
3 (6.8%)
0
0
1 (7.7%)
1 (7.7%)
1 (7.7%)
1 (7.7%)
0
2 (15.4%)
0
3 (23%)
2 (15.4%)
2 (15.4%)
0
HRM: high-resolution manometry; EMD: esophageal motor disorder; EGJOO:
esophagogastric junction outflow obstruction. *Comparison of post-LTx between the
non-rejection and rejection group (normal vs EMD, p = 0.09). Statistical methods: Chi-
squared test or Fisher’s exact test, as appropriate.

Fig. 1. DCI pre-LTx and six months post-LTx.

Fig. 2. DCI pre-LTx and post-LTx in the rejection vs non-rejection groups.



Fig. 3. High resolution manometry (HRM) plot pre-LTx and six months post-LTx. High
resolution impedance manometry (HRiM) was performed three months later to follow
up the esophageal motor disorder (EMD) previously treated with botulinum toxin (at
the level of the esophagogastric junction [EGJ] and in the esophageal body) when the
patient presented dysphagia and also acute rejection. A. HRM plot pre-LTx. B. HRM
plot six months post-LTx with a diagnosis of hypercontractile esophagus and impaired
EGJ relaxation. C. HRiM performed three months later, after treatment with botulinum
toxin. Persistence of EMD and bolus retention can be observed.