Embed Size (px)
Citation preview

©2016 MFMER | slide-1
`Tis the Season Influenza and Pneumococcal Vaccine Updates
Alex Quinn, PharmDPGY2 Ambulatory Care ResidentPharmacy Grand RoundsSeptember 20, 2016

©2016 MFMER | slide-2
Objectives• Identify current influenza and pneumococcal
immunization recommendations
• Explain rationale behind the current recommendations
• Select an appropriate influenza and pneumococcal immunization schedule for patients

©2016 MFMER | slide-3
Influenza Vaccine

©2016 MFMER | slide-4

©2016 MFMER | slide-5
Who should receive the influenza vaccine?
• All persons > 6 months of age without contraindications
Grohskopf LA, et al. MMWR Recomm Rep 2016;65(5):1-56

©2016 MFMER | slide-6
Types of Influenza Vaccines• Inactivated Influenza Vaccines (IIVs)
• Available as trivalent (IIV3) & quadrivalent (IIV4)
• Recombinant Influenza Vaccine (RIV)• 1 RIV product Flublok
• Live Attenuated Influenza Vaccine (LAIV)• 1 LAIV4 product FluMist Quadrivalent
Grohskopf LA, et al. MMWR Recomm Rep 2016;65(5):1-56

©2016 MFMER | slide-7
Influenza Update #1 for 2016-17 Season• Vaccine Composition:
• Trivalent vaccines:• A/California/7/2009 • A/Hong Kong/4801/2014 • B/Brisbane/60/2008
• Quadrivalent vaccines:• All of the above strains plus…• B/Phuket/3073/2013
Grohskopf LA, et al. MMWR Recomm Rep 2016;65(5):1-56

©2016 MFMER | slide-8
Influenza Update #2 for 2016-17 Season
• LAIV4 should NOT be used• ACIP interim recommendation
Grohskopf LA, et al. MMWR Recomm Rep 2016;65(5):1-56LAIV4: quadrivalent live attenuated influenza vaccineACIP: Advisory Committee on Immunization Practices

©2016 MFMER | slide-9
Intranasal Efficacy ConcernsStudy U.S. Influenza
Vaccine EffectivenessNetwork
Department of Defense Laboratory-based Influenza Surveillance
ICICLE Observational Study
Population • 2286 patients • 2 – 17 years • Acute respiratory
illness including cough < 7 days
• Military dependents• 2 – 17 years• Influenza-like illness
• 1012 patients• 2 – 17 years• Febrile acute
respiratory illness with onset < 5 days
Timeframe 11/2/15 – 4/15/16 Not specified 11/30/15 – 4/15/16
Design Test-negative design Test-negative design Test-negative design
Efficacy Results
LAIV4: 3% IIV3/4: 63%
LAIV4: 53%IIV3/4: 66%
LAIV4: 46%IIV: 65%
CDC Web site. Available at: www.cdc.gov/media/releases/2016/s0622-laiv-flu.htmlFlannery B. et al. US Flu VE Network. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2016-06/influenza-05-flannery.pdf. Ambrose C. Influenza Clinical Investigation for Children (ICICLE) Study. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2016-06/influenza-06-ambrose.pdf.
LAIV4: quadrivalent live attenuated influenza vaccineIIV3/4: trivalent/quadrivalent inactivated influenza vaccineIIV: inactivated influenza vaccine

©2016 MFMER | slide-10
LAIV vs. IIV Efficacy from US Flu VE Network
-10%
0%
10%
20%
30%
40%
50%
60%
70%
80%
2010 -2011
2011 -2012
2012 -2013
2013 -2014
2014 -2015
2015 -2016
LAIV3LAIV4IIV3IIV3/4
Flannery B. Influenza Division, CDC. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2016-06/influenza-07-flannery.pdf.
LAIV3: trivalent live attenuated influenza vaccineLAIV4: quadrivalent live attenuated influenza vaccineIIV3: trivalent inactivated influenza vaccineIIV3/4: trivalent/quadrivalent inactivated influenza vaccine

©2016 MFMER | slide-11
Conflicting Evidence in Canada • Does vaccinating children & adolescents with LAIV provide
better community protection than IIV?• Design
• Cluster randomized blinded trial • Conducted between October 2012 and May 2015
• Primary endpoint• Reverse transcriptase polymerase chain reaction-confirmed influenza A
or B virus
• Population• 52 Hutterite colonies in Alberta & Saskatchewan, Canada• 1186 Canadians aged 36 months to 15 years received vaccine
Loeb M. et al. Ann Intern Med. Epub 2016 Aug 16: 1-13.LAIV: live attenuated influenza vaccineIIV: inactivated influenza vaccine

©2016 MFMER | slide-12
Conflicting Evidence in Canada
• Intervention• Randomly assigned, blinded
• Trivalent LAIV or trivalent IIV
• Results• Rate of influenza A or B virus infection:
• LAIV: 5.3%• IIV: 5.2%• Hazard ratio: 1.03 (95% CI 0.85 to 1.24)
• Limitations• Canada using LAIV3• U.S. using LAIV4
Loeb M. et al. Ann Intern Med. Epub 2016 Aug 16: 1-13.LAIV: live attenuated influenza vaccineLAIV3: trivalent live attenuated influenza vaccineLAIV4: quadrivalent live attenuated influenza vaccineIIV: inactivated influenza vaccine

©2016 MFMER | slide-13
Hypothesis for LAIV4 decreased effectiveness
• Suboptimal vaccine component performance
• Potential interference among live viruses
• More highly vaccinated population
Flannery B. Influenza Division, CDC. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2016-06/influenza-07-flannery.pdf.

©2016 MFMER | slide-14
Influenza Update #3 for 2016-17 Season• History of severe allergic reaction to egg
Symptom Influenza Vaccine Product
Administration Recommendations
Only hivesAny licensed & recommended
influenza vaccine
Supervision NOTrequired
Any symptom other than hives
Any licensed & recommended
influenza vaccine
Vaccinate under the supervision of a
health care provider
Grohskopf LA, et al. MMWR Recomm Rep 2016;65(5):1-56

©2016 MFMER | slide-15
Influenza Update #3 for 2016-17 Season
• No longer need to monitor egg-allergic recipients for 30 minutes postvaccination
• Consider monitoring all patients at least 15 minutes postvaccination
Grohskopf LA, et al. MMWR Recomm Rep 2016;65(5):1-56

©2016 MFMER | slide-16
Assessment Question #1• What is a potential reason(s) for the decreased
efficacy with LAIV4?
a) Interference amongst vaccine strainsb) Recipient is not inhaling full dosec) Population is more highly vaccinatedd) A & Ce) A, B, & C
LAIV4: quadrivalent live attenuated influenza vaccine

©2016 MFMER | slide-17
Influenza Vaccine Highlights• Continue recommending influenza vaccine for
• Patients > 6 months of age
• Intranasal flu vaccine is not recommended
• Egg-allergic patients:• Administer under supervision of health care provider
• If history of severe allergic reaction (other than hives)• 30 minute post-vaccination observation no longer required

©2016 MFMER | slide-18
Pneumococcal Vaccine

©2016 MFMER | slide-19
Types of Pneumococcal Vaccines
Product PCV13 (Prevnar 13) PPSV23 (Pneumovax 23)Composition 13-valent pneumococcal
conjugate vaccine
Protein Carrier = Diphtheria CRM197
23-valent pneumococcal polysaccharide vaccine
Dose 0.5 mL 0.5 mL
Route IM IM or SC
Preservatives No Yes
Pharmacologic Category
Inactivated vaccine Inactivated vaccine
PCV13 & PPSV23 are NOT interchangeable Clinical Pharmacology Web site. Accessed August 20, 2016.Plosker, GL et al. Drugs (2015)75:1535-1546.Facts & Comparisons Web site. Accessed August 20, 2016.UpToDate Web site. Accessed August 20, 2016.
PCV13: pneumococcal conjugate vaccine (13 valent)PPSV23: pneumococcal polysaccharide vaccine (23 valent)IM: intramuscularSC: subcutaneous

©2016 MFMER | slide-20
Why do we need to give 2 vaccines?• Polysaccharide antigens are poorly immunogenic in children
< 2 years old
• PCV13 has shown to elicit similar or higher antibody titers compared to PPSV23
• Giving PPSV23 followed by PCV13 has shown lower antibody response than giving PCV13 first
• Potential for broader protection by utilizing both vaccines
MMWR. 2012; 61(40):816-819.Tomczyk S. et al. MMWR. 2014; 63(37):822-825.
PCV13: pneumococcal conjugate vaccine (13 valent)PPSV23: pneumococcal polysaccharide vaccine (23 valent)

©2016 MFMER | slide-21
Review of CAPiTA Trial• Determine efficacy of pneumococcal conjugate vaccine in
adults > 65 years
• Design• Parallel-group, randomized, placebo-controlled, double-blind trial
• Primary Endpoint• Efficacy of PCV13 in prevention of a 1st episode of confirmed vaccine-
type CAP
• Population• > 65 years of age• Enrolled between 9/15/2008 and 1/30/2010
• Intervention• Randomly assigned 1:1 to receive PCV13 or placebo
Bonten MJM, et al. N Engl J Med. 2015;372:1114-25.CAPiTA: Community-Acquired Pneumonia Immunization Trial in AdultsPCV13: pneumococcal conjugate vaccine (13 valent)CAP: community acquired pneumonia

©2016 MFMER | slide-22
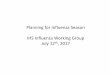
Review of CAPiTA Trial
49
90
0
10
20
30
40
50
60
70
80
90
100
Number of Confirmed CAP with
vaccine-type strain
PCV13Placebo
P < 0.001
Bonten MJM, et al. N Engl J Med. 2015;372:1114-25.CAPiTA: Community-Acquired Pneumonia Immunization Trial in AdultsPCV13: pneumococcal conjugate vaccine (13 valent)CAP: community acquired pneumonia

©2016 MFMER | slide-23
Does my patient need a pneumococcal vaccine?• How old are they?
• 19 – 64 years of age• > 65 years of age
• Medical history?• Immunocompetent with specific chronic diseases• Immunocompromised• Functional or anatomic asplenia• Cerebrospinal fluid (CSF) leak • Cochlear implant
• Vaccine naïve?

©2016 MFMER | slide-24
General Guidelines
• Adults recommended to receive:• 1 dose of PCV13• 1, 2, or 3 doses of PPSV23
• Ideally PCV13 should be given 1st (when both are indicated)
• Separate PCV13 & PPSV23 by at least 1 year• Exception: separate by at least 8 weeks
• Adults with immunocompromising conditions• Anatomical or functional asplenia• Cerebrospinal fluid leak• Cochlear implant
• Separate PPSV23 doses by at least 5 years
CDC Web site. Adult Immunization Schedule. Available at: https://www.cdc.gov/vaccines/schedules/downloads/adult/adult-combined-schedule.pdf
PCV13: pneumococcal conjugate vaccine (13 valent)PPSV23: pneumococcal polysaccharide vaccine (23 valent)

©2016 MFMER | slide-25
Pneumococcal Vaccination 19 – 64 Years OldImmune Status Immunocompetent
Risk Factors • Alcoholism• Cardiac: except hypertension• Diabetes• Liver• Pulmonary• Smoking
• Cerebrospinal fluid leak• Cochlear implant
Vaccine Naïve Yes
NoPPSV23 already
givenYes
NoPPSV23 already
given
Vaccine TypePPSV23
No doses needed until
age 65PCV13
PCV131 year after
PPSV23
Interval 8 weeks
Vaccine Type PPSV23
MMWR. 2010;59(34);1102-1106CDC Web site. Adult Immunization Schedule. Available at:www.cdc.gov/vaccines/schedules/hcp/imz/adult-compliant.html. MMWR. 2012;61(40);816-819CDC Web site. Recommended Adult Immunization Schedule. Available at: https://www.cdc.gov/vaccines/schedules/downloads/adult/adult-combined-schedule.pdfImmunization Action Coalition Web site. Available at:www.immunize.org/catg.d/p2011.pdfMinnesota Department of Health Web site. Available at: http://www.health.state.mn.us/divs/idepc/diseases/pneumococcal/hcp/pocket.pdf
PCV13: pneumococcal conjugate vaccine (13 valent)PPSV23: pneumococcal polysaccharide vaccine (23 valent)

©2016 MFMER | slide-26
Pneumococcal Vaccination 19 – 64 Years OldImmune Status Immunocompromised or Functional/Anatomic Asplenia
Vaccine Naïve Yes No1 PPSV23 already given
No2 PPSV23 already given
Vaccine Type PCV13 PCV131 year after PPSV23
PCV131 year after PPSV23
Interval 8 weeks
8 weeks after PCV13and
5 years after PPSV23
Vaccine Type PPSV23 PPSV23
Interval 5 years
Vaccine Type PPSV23
MMWR. 2012;61(40);816-819CDC Web site. Recommended Adult Immunization Schedule. Available at:www.cdc.gov/vaccines/schedules/downloads/adult/adult-combined-schedule.pdfCDC Vaccine Schedules AppMinnesota Department of Health Web site. Available at: http://www.health.state.mn.us/divs/idepc/diseases/pneumococcal/hcp/pocket.pdf
PCV13: pneumococcal conjugate vaccine (13 valent)PPSV23: pneumococcal polysaccharide vaccine (23 valent)

©2016 MFMER | slide-27
Vaccine Naïve Yes
NoPreviously received PPSV23 at age > 65
NoPreviously received PPSV23 at age < 65
NoPreviously received PCV13 & possibly
PPSV23 at age < 65
Interval NA1 year after
PPSV231 year after
PPSV23
8 weeks after PCV13 and 5 years after
PPSV23
Vaccine Type PCV13 PCV13 PCV13 PPSV23
Interval > 1 year
1 year after PCV13and
5 years after PPSV23
Vaccine Type PPSV23 PPSV23
Pneumococcal Vaccination > 65 Years Old
Tomczyk S et al. MMWR. 2014:63(37);822-825Kobayashi M et al. MMWR. 2015:64(34);944-947MMWR. 2012;61(40);816-819MMWR. 2010;59(34);1102-1106CDC Vaccine Schedules AppMN Department of Health Web site. Available at: http://www.health.state.mn.us/divs/idepc/diseases/pneumococcal/hcp/pocket.pdf
PCV13: pneumococcal conjugate vaccine (13 valent)PPSV23: pneumococcal polysaccharide vaccine (23 valent)

©2016 MFMER | slide-28
Case for Assessment Questions # 2 & 3• 71 year old male with PMH significant for
GERD, hypertension, migraines, and history of smoking 1 pack per day x20 years (quit 8 years ago). Immunization history: PPSV23 01/2005, influenza vaccine 9/2013, 9/2014, 10/2015, Tdap 7/2011.
PMH: past medical historyGERD: gastroesophageal reflux diseasePPSV23: pneumococcal polysaccharide vaccine (23 valent)Tdap: tetanus toxoid-reduced diphtheria toxoid-acellular pertussis

©2016 MFMER | slide-29
Assessment Question #2• Does patient qualify for a pneumococcal vaccine?
a) Yes
b) No

©2016 MFMER | slide-30
Assessment Question #3• What pneumococcal vaccine regimen would
you recommend?a) PCV13 nowb) PPSV23 now, followed by PCV13 in 9/2017c) PPSV23 now, followed by PCV13 in
9/2017, then PPSV23 in 9/2022d) PCV13 now, followed by PPSV23 in
9/2017
PCV13: pneumococcal conjugate vaccine (13 valent)PPSV23: pneumococcal polysaccharide vaccine (23 valent)

©2016 MFMER | slide-31
Pneumococcal Vaccine Highlights• Vaccination sequence & timing dependent upon:
• Age• Medical history• Pneumococcal vaccine history
• Adults recommended to receive:• 1 dose of PCV13• Up to 3 doses of PPSV23
• Interval either 8 weeks, 1 year, or 5 years
PCV13: pneumococcal conjugate vaccine (13 valent)PPSV23: pneumococcal polysaccharide vaccine (23 valent)

©2016 MFMER | slide-32
Questions & Discussion

©2016 MFMER | slide-33
`Tis the Season Influenza and Pneumococcal Vaccine Updates
Alex Quinn, [email protected]