Embed Size (px)
DESCRIPTION
qs
Citation preview

The Thyroid Epidemiology, Audit, and Research Study:Thyroid Dysfunction in the General Population
R. W. V. FLYNN, T. M. MACDONALD, A. D. MORRIS, R. T. JUNG, AND G. P. LEESE
Medicines Monitoring Unit (R.W.V.F., T.M.M), Diabetes Centre (A.D.M., R.T.J.), and Wards 1 and 2 (G.P.L.), NinewellsHospital and Medical School, Dundee, DD1 9SY, United Kingdom
The objective of this study was to define the level of treatedthyroid dysfunction in a complete and representative popu-lation base in an area of sufficient dietary iodine intake. Weused record-linkage technology to retrospectively identifysubjects treated for hyperthyroidism or hypothyroidism inthe general population of Tayside, Scotland from 1 January1993 to 30 April 1997. Thyroid status was ascertained byrecord linkage of patient-level datasets containing details oftreatments for hyperthyroidism and hypothyroidism.
We identified 620 incident cases of hyperthyroidism, anincidence rate of 0.77/1000�yr [95% confidence interval (CI),0.70–0.84] in females and 0.14/1000�yr (95% CI, 0.12–0.18) in
males. There were 3,486 incident cases of diagnosed primaryhypothyroidism, an incidence rate of 4.98/1000�yr (95% CI,4.81–5.17) in females and 0.88/1000�yr (95% CI, 0.80–0.96) inmales. For both hyperthyroidism and hypothyroidism, the in-cidence increased with age, and females were affected two toeight times more than males across the age range. The mid-year point prevalence of all-cause hypothyroidism rose from2.2% in 1993 to 3.0% in 1996.
The level of thyroid dysfunction in Tayside, Scotland ishigher than previously reported, and it increased from 1993 to1996. (J Clin Endocrinol Metab 89: 3879–3884, 2004)
THYROID DYSFUNCTION IS a common disorder pre-viously thought to affect 1–2% of the United Kingdom
adult population (1). T4 is also the sixth most commonlydispensed drug in Scotland (2); and with the inclusion ofmonitoring thyroid dysfunction as a part of the new generalpractitioners contract in the United Kingdom, its importancefor public health is confirmed. Despite this, the epidemiologyof thyroid disease and thyroid dysfunction remains unclear,especially when compared with other endocrine disorders.Previous studies have tended to use selected populationsthat are unrepresentative of the general population (3, 4). Inparticular, there is a paucity of studies investigating hypo-thyroid disease as a result of it being routinely managed incommunity care, thus making area-wide follow-up difficult.Robust data are available from only one region of sufficientiodine intake (Whickham, UK), but the relatively small num-bers of subjects studied resulted in unclear findings for malesin particular (1, 5). In addition, the incidence of thyroiddysfunction has increased with time and varies betweenlocalities [a feature associated with the level of dietary iodine(6, 7)]. There is a requirement for multiple studies fromdifferent locations.
The present study used record-linkage technology to iden-tify incident and prevalent cases of treated thyroid dysfunc-tion in the population of Tayside, Scotland between 1993 and1997. The aim of the study was to define the amount oftreated thyroid disease in a complete and representativepopulation base.
Subjects and Methods
We used databases available at the Medicines Monitoring Unit(MEMO) based at the University of Dundee. MEMO uses record-linkagetechnology to conduct epidemiological and pharmacoepidemiologicalstudies and has been described in detail elsewhere (8, 9). In brief, weused record linkage of a number of routinely collated population-baseddatasets. The data linkage was facilitated by the presence of a unique10-digit patient identifier, the community health number (CHN). Everyperson in Scotland registered with a general practitioner is assigned aCHN; and in Tayside, this is used as a patient identifier for all contactswith healthcare activity.
Study population
A fixed population comprising all subjects continuously registeredwith a general practitioner during the study period from 1 January 1993to 30 April 1997 was used. This population included those who diedduring the intervening period and those who were born after 1 January1993.
Definition of hyperthyroid and hypothyroid cases
Six principle databases were used to identify patients with thyroiddysfunction in the population.
CHN master patient index. This index provided data on registered Taysidegeneral practitioner, dates registered with general practitioner, date ofbirth and date of death. It was used to define the study population fromwhich cases were identified.
MEMO dispensed prescription database. This database contained validatedsubject specific data on all prescriptions dispensed from all communitypharmacies in Tayside, including drug name, formulation, dosage, fre-quency, and duration (8). Details of any thyroid replacement or anti-thyroid medication received from January 1993 to April 1997 wereextracted (Table 1).
Scottish morbidity record 1 (SMR1). These data are routinely validated andcollated by the Information and Statistics Division of the National HealthService in Scotland and were available for Tayside from 1 January 1980to 30 April 1997. Diagnostic and procedural codes relating to all hospitalinpatient episodes of care using the International Classification of Dis-eases ninth and 10th revisions and the Office of the Population and
Abbreviations: CHN, Community health number; CI, confidence in-terval; MEMO, Medicines Monitoring Unit; RAI, radioactive iodine;SMR1, Scottish morbidity record 1.JCEM is published monthly by The Endocrine Society (http://www.endo-society.org), the foremost professional society serving the en-docrine community.
0021-972X/04/$15.00/0 The Journal of Clinical Endocrinology & Metabolism 89(8):3879–3884Printed in U.S.A. Copyright © 2004 by The Endocrine Society
doi: 10.1210/jc.2003-032089
3879
at Indonesia:Endo Jnls Sponsored on May 26, 2009 jcem.endojournals.orgDownloaded from

Census Surveys classification of surgical Operations and Procedureswere available. These data were used to identify thyroid-related surgi-cal, diagnostic, and therapeutic procedures.
Radioactive iodine (RAI) database. This database is a computerized data-base of all RAI treatments administered in Tayside since 1955. Detailsincluded patient, dose, date of administration, and name of prescribingconsultant.
Tayside thyroid register. This register is a community-based databasederived from the Scottish Automated Follow-Up Register (10). Thissystem automatically follows up patients on thyroid replacement ther-apy, including those with primary hypothyroidism and those previouslytreated for hyperthyroidism or other thyroid conditions. Since 1991, ithas captured GP as well as consultant referrals for thyroid dysfunction.This provided data on diagnosis and date of registration.
Biochemistry data. TSH results were used. Electronic data were not com-plete for all areas for the early part of the study, so they were used onlyin conjunction with other data to confirm diagnoses.
Patient identification
Hyperthyroid patients. Patients were selected if they had been treated forhyperthyroidism by surgery, RAI, or medication or they had a historyof hyperthyroidism on the thyroid register. Patients were classified assurgically treated hyperthyroid if there were SMR1 codes for both thediagnosis and procedure fields (Table 1) or if they had a suppressed TSHresults (�0.04 mU/liter) in the 12 months before the date of thyroidsurgery. Patients treated with RAI at a dose with the range 220-1110 MBqwere classified as hyperthyroid. Subjects who received more than oneprescription for antithyroid medication were classified as medicallytreated (Table 1). Patients prescribed RAI by an oncologist at a dose ofover 1500 Bq, those with appropriate SMR1 codes for thyroid cancer, orthose with cancer of the thyroid register were excluded. Prevalent caseswere those who had a history of overactive thyroid, regardless of theircurrent thyroid status. Incident cases were newly treated cases arisingfrom 1 July 1993 to 30 April 1997 (this allowed a 6-month screeningperiod to identify the new cases).
Hypothyroid patients. Hypothyroid patients were those on continuouslong-term thyroid replacement therapy because of an underactive thy-roid (Table 1), and with the requirement that the subject should still bereceiving it in the 6 months before the end of the study or in the 6 monthsbefore death. To establish prevalent cases of hypothyroidism, those withany form of thyroid cancer or those treated with T4 for euthyroid goiterwere excluded. Existing cases were all those treated for hypothyroidismfrom 1 January 1993 to 30 June 1993. Incident cases were all new casesarising from 1 July 1993 to 31 October 1996. In defining primary hypo-thyroidism, those that were hypothyroid secondary to treatment forother thyroid disorders were excluded.
Validation of electronically derived cohorts
A manual validation exercise was performed by an experienced re-search nurse to determine the predictive power of the electronic datalinkage. The primary care case records of all thyroid patients identifiedat four geographically representative general practices in Tayside regionwere inspected. The validation process considered whether the elec-
tronic diagnosis was appropriately assigned and whether incident caseswere correctly designated.
Statistical methods
The prevalence was calculated as the number of existing cases ofdisease divided by the number of live persons from the fixed populationon 30 June each year. Confidence intervals (CIs) were calculated forproportions (11). Incidence was expressed as the person-time incidencerate and calculated as the number of new cases divided by the numberof person-years at risk during follow-up with units of cases per 1000persons per year (/1000 per yr). CI limits were calculated assuming aPoisson distribution (12). For the validation exercise, positive predictivevalues were calculated as the number of correctly identified patientsdivided by the total number of electronically identified patients in thecohort.
Ethical approval
The databases used by MEMO are anonymized and registered underthe Data Protection Act for purposes of research and audit. At all times,confidentiality of individual patients and individual general practicedata was maintained, and all statistical analyses were performed onanonymized datasets. This study was approved by the Tayside Researchand Ethics Committee, and permission for the case record validationaudit was obtained from Tayside Caldicott Guardians (13).
Results
Case records were retrieved and validated in general prac-tice for 450 subjects (363 hypothyroid, 87 hyperthyroid). Theelectronic database performed well, with positive predictivevalues of 0.98 for treated hyperthyroidism and 0.96 fortreated hypothyroidism. Errors occurred where case notesshowed no evidence of thyroid dysfunction. Of the apparenthypothyroid subjects validated, 2.8% (n � 10; 95% CI, 1.5–5.0%) were actually euthyroid goiters being treated by long-term T4. In addition, six cases of prevalent hypothyroidismwere misclassified as incident cases.
Hyperthyroidism
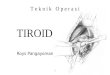
The fixed population for Tayside for the period 1 January1993 to 30 April 1997 was 369,885. During this time, therewere 167,781 TSH tests carried out on 78,714 subjects in thepopulation. Of these, 47,975 (28.6%) tests were outside thereference range of 0.4–4.0 mU/liter. We identified 1,910 ex-isting and 620 incident cases of treated hyperthyroidism (Fig.1). The midyear point prevalence of hyperthyroidism for theyears 1993 to 1996 is shown in Table 2. The increasing year-on-year trend in prevalence was found to be highly signif-icant (�2
trend � 43.6; df � 1; P � 0.0001). Table 3 shows the
TABLE 1. Data codes used in identifying thyroid dysfunction
Thyroid replacement medication found on MEMO prescription database T4 (Eltroxine)Liothyronine (Tertroxine, Triiodothyronine)
Antithyroid medication found on MEMO prescription database Carbimazole (Neomercazole)PropylthiourcilIodine and iodide
ICD codesHyperthyroidism ICD9: 242 and ICD10: E05Thyroid cancer ICD9: 193, 234.8 and ICD10: C73
OPCS codes for surgical procedures on thyroidOPCS3: 070, 071, 072, 075OPCS4: B08, B12
3880 J Clin Endocrinol Metab, August 2004, 89(8):3879–3884 Flynn et al. • Research Study: Thyroid Dysfunction in Scotland
at Indonesia:Endo Jnls Sponsored on May 26, 2009 jcem.endojournals.orgDownloaded from

number of cases and incident rates of hyperthyroidism byage and sex.
Hypothyroidism
The fixed population for the period 1 January 1993 to 31October 1996 was 367,639. Overall we classified 11,745 sub-jects as receiving long-term thyroid replacement treatment(Fig. 2).
The midyear point prevalence of all-cause hypothyroid-ism for the years 1993 to 1996 is shown in Table 4. Theincreasing trend in prevalence was found to be highly sig-nificant (�2
trend � 503.2; df � 1; P � 0.0001). There were 3469cases of incident primary hypothyroidism. Table 5 shows thenumber of cases and incident rates of treated primary hy-pothyroidism by age and gender.
Discussion
This study has used record-linkage technology to identifyincident and prevalent cases of treated thyroid dysfunctionin Tayside from 1993 to 1997. A case-record validation ex-ercise has shown the methodology to have strong positivepredictive value in diagnosing thyroid disease and was re-assuring in finding only a low level of treatment for condi-tions other than thyroid dysfunction, such as T4 use fortreatment of euthyroid goiter. Although the incidence of bothhyperthyroidism and hypothyroidism was found to increasewith age, the trend was more pronounced among the hy-pothyroid subjects, with the highest incidence found in the
80� age category. We have established the incidence of thy-roid dysfunction in males, something that has not been pos-sible in previous studies in iodine-replete areas. Thyroiddysfunction is often quoted as affecting 10- to 20-times asmany females as males; however, we have found this to varyfrom a 2-fold increase in the 80� age group to an 8-foldincrease in younger age groups (a relationship true for bothhyper- and hypothyroidism). Additionally we found a year-on-year increase in the prevalence of both hyper- and hy-pothyroidism from 1993 to 1996.
The cases were drawn from a large fixed population witha long follow-up time. Recent census findings have shownTayside to have an age-sex distribution that is broadly rep-resentative of the Scottish population and to be composed ofapproximately 2% nonwhite ethnic groups (14). The area hasa low subject migration of 2.7%/yr (15). In line with otherstudies, we have considered any prior cases of hyperthy-roidism as being prevalent cases, regardless of the state of theillness at the time (1, 5). Subjects having suffered from thy-roid cancer were excluded from the analysis. One feature ofour study is that we defined incidence and prevalence ratesof diagnosed disease and cannot comment on the amount ofsubclinical disease. The study could not detect undiagnosedor untreated thyroid dysfunction or cases treated outsideTayside.
FIG. 1. Identification of cases of hyperthyroidism in Tayside from 1January 1993 to 30 April 1997
TABLE 2. Prevalent and incident cases of hyperthyroidism from 1993–1996 measured on 30 June each year
Year 1993 1994 1995 1996
Population 350,136 349,884 349,626 349,369Prevalent cases 1,791 1,933 2,040 2,188Point prevalence 0.51% 0.55% 0.58% 0.63%
(95% CI for point prevalence) (0.49–0.54%) (0.53–0.58%) (0.56–0.61%) (0.60–0.65%)Incident cases previous 12 months 188 157 207Incidence rate (per 1000) 0.54 0.45 0.59
(95% CI for incidence rate) (0.46–0.62) (0.38–0.53) (0.51–0.68)
TABLE 3. Incidence of hyperthyroidism in Tayside between 1993and 1997
Incidentcases
Person-years offollow-up
Incidence rate(per 1000 peryear) (95% CI)
Females�9 0 77,913 0.00 (0.00–0.05)10–19 10 72,677 0.14 (0.07–0.25)20–29 60 76,743 0.78 (0.60–1.01)30–39 81 95,146 0.85 (0.68–1.06)40–49 85 94,295 0.90 (0.72–1.14)50–59 73 80,596 0.91 (0.71–1.14)60–69 90 80,242 1.12 (0.90–1.38)70–79 83 64,282 1.29 (1.03–1.60)80� 44 42,050 1.05 (0.76–1.40)
All females 526 683,944 0.77 (0.70–0.84)Males
�9 0 81,799 0.00 (0.00–0.05)10–19 2 79,937 0.03 (0.00–0.09)20–29 5 85,953 0.06 (0.02–0.14)30–39 13 98,250 0.13 (0.07–0.23)40–49 20 96,782 0.21 (0.13–0.32)50–59 14 78,725 0.18 (0.10–0.30)60–69 19 70,443 0.27 (0.16–0.42)70–79 13 45,528 0.29 (0.15–0.49)80� 8 17,975 0.45 (0.19–0.88)
All males 94 655,392 0.14 (0.12–0.18)All cases 620 1,339,336 0.46 (0.43–0.50)
Flynn et al. • Research Study: Thyroid Dysfunction in Scotland J Clin Endocrinol Metab, August 2004, 89(8):3879–3884 3881
at Indonesia:Endo Jnls Sponsored on May 26, 2009 jcem.endojournals.orgDownloaded from

Hyperthyroidism
The Whickham survey, which followed a cohort over 18yr of age, found the incidence of hyperthyroidism in fe-
males to be 0.8/1000�yr, with negligible results amongmales (5). Other studies from the 1970s and early 1980sreported incidences of hyperthyroidism of 0.23– 0.28/1000�yr (16 –19), whereas subsequent studies put the figureat 0.43– 0.52/1000�yr (20, 21). Recently, two areas of Den-mark have reported incidences of hyperthyroidism of0.93/1000�yr and 0.65/1000�yr (7). The Tayside result of0.46/1000�yr was lower than that of Denmark. The Whick-ham survey found an incidence of hyperthyroidism of0.8/1000 in females, a finding similar to Tayside; however,the Whickham population was over 18 yr of age, whereasours was inclusive of all ages. Recalculating the incidencefor Tayside by excluding those under the age of 18 gavea figure of 0.96/1000�yr, higher than Whickham’s. We alsofound a year-on-year increase in the prevalence of hyper-thyroidism from 1993 to 1996. As with previous studies,we used a cumulative measure of hyperthyroidism, in-cluding all patients who have ever been hyperthyroid (1).Using a cumulative measure will cause the year-on-yearprevalence to increase; however, this will not reflect thenumber of cases of active disease.
Hypothyroidism
Few studies have attempted to establish the incidence ofhypothyroidism in the general population. The Whickhamsurvey found an incidence of 3.5/1000�yr in females and0.6/1000�yr in males, whereas the recent Danish findingsshowed incidences of 0.27/1000�yr and 0.40/1000�yr, respec-
FIG. 2. Identification of cases of hypo-thyroidism in Tayside from 1 January1993 to 31 October 1996.
TABLE 4. Prevalent and incident cases of all cause hypothyroidism from 1993 to 1996 measured on 30 June each year
Year 1993 1994 1995 1996
Population 350,136 349,884 349,626 349,369Prevalent cases 7,627 8,466 9,471 10,408Point prevalence 2.18% 2.42% 2.71% 2.98%
(95% CI for point prevalence) (2.13–2.23%) (2.37–2.47%) (2.66–2.77%) (2.92–3.04%)Incident cases previous 12 months 1,113 1,286 1,233Incidence rate (per 1000) 3.18 3.68 3.53
(95% CI for incidence rate) (2.99–3.37) (3.48–3.88) (3.33–3.73)
TABLE 5. Incidence of primary hypothyroidism in Taysidebetween 1993 and 1996
Incidentcases
Person-years offollow-up
Incidence rate(per 1000 peryear) (95% CI)
Females�9 9 67,205 0.13 (0.06–0.25)10–19 22 62,901 0.35 (0.22–0.53)20–29 124 67,614 1.83 (1.53–2.19)30–39 280 82,485 3.39 (3.01–3.82)40–49 498 82,089 6.07 (5.55–6.62)50–59 547 70,311 7.78 (7.14–8.46)60–69 635 70,099 9.06 (8.37–9.79)70–79 496 56,135 8.84 (8.08–9.65)80� 358 36,827 9.72 (8.74–10.87)
All females 2969 595,666 4.98 (4.81–5.17)Males
�9 11 70,673 0.16 (0.08–0.28)10–19 6 69,378 0.09 (0.03–0.19)20–29 18 75,281 0.24 (0.14–0.38)30–39 37 85,553 0.43 (0.30–0.60)40–49 54 83,991 0.64 (0.48–0.84)50–59 82 68,778 1.19 (0.95–1.48)60–69 109 61,373 1.78 (1.46–2.14)70–79 107 39,840 2.69 (2.20–3.25)80� 76 15,683 4.85 (3.82–6.07)
All males 500 570,550 0.88 (0.80–0.96)All cases 3,469 1,166,216 2.97 (2.88–3.08)
3882 J Clin Endocrinol Metab, August 2004, 89(8):3879–3884 Flynn et al. • Research Study: Thyroid Dysfunction in Scotland
at Indonesia:Endo Jnls Sponsored on May 26, 2009 jcem.endojournals.orgDownloaded from

tively. Our result of 2.97/1000�yr in a combined male/femalepopulation is higher than the Whickham follow-up and sub-stantially higher than the Danish findings. Additionally, wehave found a year-on-year increase in the prevalence of hy-pothyroidism from the years 1993 to 1996. The higher thanpreviously recorded incidence and increasing prevalence ofhypothyroidism may reflect a temporal increase in autoim-mune diseases. Thyroid disease in the United Kingdom isgenerally of autoimmune etiology; and levels of other auto-immune disease, such as type-1 diabetes, are increasing (22).It has been suggested that recent years have seen a rise in thelevel of autoimmune disease and of immune mediated dis-orders in general, and this has been put forward as a possiblereason for the perceived increase in thyroid disorders (23). Itis also possible that there has been an increase in the diag-nosis or ascertainment of thyroid disease due to improvedpractice and increased availability of diagnostic tests. An-other possibility is that there is an increasing older femalepopulation due to increasing longevity of life (24). Thus,there is a greater opportunity for the diagnosing ofhypothyroidism.
There are a number of other possible reasons for the dif-ferences found between the results presented here and thosefound elsewhere. The difference may reflect the methodol-ogies employed: some have used population screening andfollow-up of survivors in a cohort over 18 years of age,whereas others have highlighted incident cases from abnor-mal biochemistry results or hospital admissions (7, 20). Thepopulation dynamics of the different locations will also havean impact on the levels of thyroid dysfunction, because in-cidence was higher among females and the elderly. Anotherpossibility is that there is a geographic variation in the riskof thyroid dysfunction between regions (7, 19), which couldreflect a variety of environmental and/or genetic factors. Onesuch factor could be the role of dietary iodine in determiningthyroid function. It has been hypothesized that higher levelsof dietary iodine decrease the incidence of hyperthyroidismat the expense of increased incidence of hypothyroidism (6,7). The overall incidence of hyperthyroidism observed inTayside was lower, and the incidence of hypothyroidism washigher, than that reported from Denmark, with mild or mod-erate iodine deficiency. The British diet is acknowledged asbeing sufficient in iodine, with a mean urinary iodine ex-cretion in the United Kingdom of 141 �g/liter (25). Similarresults have been reported in nonpregnant females fromTayside (26), so our finding of a lower incidence of hyper-thyroidism and higher incidence of hypothyroidism is inaccordance with the theory. These findings further supportthe theory that populations with sufficient dietary iodine willhave a lower incidence of hyperthyroidism and higher in-cidence of hypothyroidism than populations that are iodinedeficient.
In conclusion, this study has established the incidence andprevalence of treated thyroid dysfunction in a population-based study in a population that is representative of Scot-land. The prevalence of hypothyroidism was higher than hasbeen found previously and was found to be increasing from1993 to 1996.
Acknowledgments
We thank those members of the MEMO team who made this studypossible, notably Philip Thompson and Gill Reekie. We also thank thosegeneral practices that allowed us access to their case records: MuirheadMedical Centre, Muirhead; Princes Street Surgery, Dundee; Mauve Prac-tice, Drumhar Health Centre, Perth; and Lour Road Group Practice,Forfar.
Received December 4, 2003. Accepted May 10. 2004.Address all correspondence and requests for reprints to: G. Leese,
Ward 1, Ninewells Hospital and Medical School, Dundee, DD1 9SY,United Kingdom. E-mail: [email protected].
This work was funded by the Chest, Heart and Stroke, Scotland.
References
1. Tunbridge WM, Evered DC, Hall R, Appleton D, Brewis M, Clark F, EvansJG, Young E, Bird T, Smith PA 1977 The spectrum of thyroid disease in acommunity: the Whickham survey. Clin Endocrinol (Oxf) 7:481–493
2. Information, Statistics Division—NHS Scotland 2003 Top ten drugs:http://www.isdscotland.org/isd/info3.jsp?pContentID�2229 (Accessed10 –3-2004)
3. Rallison ML, Dobyns BM, Meikle AW, Bishop M, Lyon JL, Stevens W1991 Natural history of thyroid abnormalities: prevalence, incidence, andregression of thyroid diseases in adolescents and young adults. Am J Med91:363–370
4. Knudsen N, Jorgensen T, Rasmussen S, Christiansen E, Perrild H 1999 Theprevalence of thyroid dysfunction in a population with borderline iodinedeficiency. Clin Endocrinol (Oxf) 51:361–367
5. Vanderpump MP, Tunbridge WM, French JM, Appleton D, Bates D, ClarkF, Grimley EJ, Hasan DM, Rodgers H, Tunbridge F 1995 The incidence ofthyroid disorders in the community: a twenty-year follow-up of the WhickhamSurvey. Clin Endocrinol (Oxf) 43:55–68
6. Laurberg P, Pedersen KM, Hreidarsson A, Sigfusson N, Iversen E, KnudsenPR 1998 Iodine intake and the pattern of thyroid disorders: a comparativeepidemiological study of thyroid abnormalities in the elderly in Iceland andin Jutland, Denmark. J Clin Endocrinol Metab 83:765–769
7. Bulow Pedersen I, Knudsen N, Jørgensen T, Perrild H, Ovesen L, Laurb-erg P 2002 Large differences in incidences of overt hyper- and hypothy-roidism associated with a small difference in iodine intake: a prospectivecomparative register-based population survey. J Clin Endocrinol Metab87:4462– 4469
8. Evans JMM, MacDonald TM 2000 The Tayside Medicines Monitoring Unit(MEMO). In: Strom BL, ed. Pharmacoepidemiology. 3rd ed. Chichester: JohnWiley, Sons; 361–374
9. Morris AD, Boyle DI, MacAlpine R, Emslie-Smith A, Jung RT, Newton RW,MacDonald TM 1997 The diabetes audit and research in Tayside Scotland(DARTS) study: electronic record linkage to create a diabetes register. DARTS/MEMO Collaboration. Br Med J 315:524–528
10. Jung RT, Scott A, Chong P, Browning M, Waugh N 1991 A new Pick basedcomputer thyroid register based on the national SAFUR requirements for localusage. Health Bull (Edinb) 49:244–249
11. Newcombe RG, Altman DG 2000 Proportions and their differences. In: Alt-man DG, Machin D, Bryant TN, Gardner MJ, eds. Statistics with confidence.2nd ed. London: BMJ Books; 45–56
12. Morris JA, Gardner MJ 2000 Epidemiological studies. In: Altman DG, MachinD, Bryant TN, Gardner MJ, eds. Statistics with confidence. 2nd ed. London:BMJ Books; 57–72
13. Evans JM, McNaughton D, Donnan PT, MacDonald TM 2001 Pharmaco-epidemiological research at the Medicines Monitoring Unit, Scotland: dataprotection and confidentiality. Pharmacoepidemiol Drug Saf 10:669–673
14. General Register’s Office for Scotland 2003 Scotland Census 2001. Key sta-tistics for council areas and health board areas Scotland. Edinburgh: GeneralRegister’s Office for Scotland
15. General Register’s Office for Scotland 1993 The 1991 Census—Report forTayside Region. Part 1. Edinburgh: HMSO; 94–95
16. Berglund J, Christensen SB, Hallengren B 1990 Total and age-specific inci-dence of Graves’ thyrotoxicosis, toxic nodular goitre and solitary toxic ade-noma in Malmo 1970–74. J Intern Med 227:137–141
17. Mogensen EF, Green A 1980 The epidemiology of thyrotoxicosis in Denmark.Incidence and geographical variation in the Funen region 1972–1974. Acta MedScand 208:183–186
18. Haraldsson A, Gudmundsson ST, Larusson G, Sigurdsson G 1985 Thyro-toxicosis in Iceland 1980–1982. An epidemiological survey. Acta Med Scand217:253–258
19. Barker DJ, Phillips DI 1984 Current incidence of thyrotoxicosis and pastprevalence of goitre in 12 British towns. Lancet 2:567–570
Flynn et al. • Research Study: Thyroid Dysfunction in Scotland J Clin Endocrinol Metab, August 2004, 89(8):3879–3884 3883
at Indonesia:Endo Jnls Sponsored on May 26, 2009 jcem.endojournals.orgDownloaded from

20. Berglund J, Ericsson UB, Hallengren B 1996 Increased incidence of thyro-toxicosis in Malmo during the years 1988–1990 as compared to the years1970–1974. J Intern Med 239:57–62
21. Galofre JC, Garcıa-Mayor RV, Fluiters E, Fernandez-Calvet L, Rego A,Paramo C, Andrade MA 1994 Incidence of different forms of thyroiddysfunction and its degrees in an iodine sufficient area. Thyroidology6:49 –54
22. Onkamo P, Vaananen S, Karvonen M, Tuomilehto J 1999 Worldwide increasein incidence of type I diabetes—the analysis of the data on published incidencetrends. Diabetologia 42:1395–1403
23. Hunter I, Greene SA, MacDonald TM, Morris AD 2000 Prevalence andaetiology of hypothyroidism in the young. Arch Dis Child 83:207–210
24. ISD Scotland 1998 Scottish Health Statistics 1997. Edinburgh: Information,Statistics Division; 252
25. International Council for Control of Iodine Deficiency Disorders 2002 Westand central Europe assesses its iodine nutrition. IDD Newsletter November,51–55
26. Barnett CA, Visser TJ, Williams F, van Toor H, Duran S, Presas MJ, Morrealede Escobar G, Hume R 2002 Inadequate iodine intake of 40% of pregnantwomen from a region of Scotland. J Endocrinol Invest 25(Suppl):90 (Abstract)
JCEM is published monthly by The Endocrine Society (http://www.endo-society.org), the foremost professional society serving theendocrine community.
3884 J Clin Endocrinol Metab, August 2004, 89(8):3879–3884 Flynn et al. • Research Study: Thyroid Dysfunction in Scotland
at Indonesia:Endo Jnls Sponsored on May 26, 2009 jcem.endojournals.orgDownloaded from

![Atypical Thyroid Function Tests, Thyroid Hormone ... · Atypical Thyroid Function Tests, Thyroid Hormone Resistance [Atipik Tiroid Fonksiyon Testleri: Tiroid Hormon Direnci] Soner](https://img.pdfslide.us/doc/110x75/5c83755009d3f2be2a8b56f6/atypical-thyroid-function-tests-thyroid-hormone-atypical-thyroid-function.jpg)