Embed Size (px)
Citation preview

Timing of RRT in AKI:The STARRT-AKI Trial
Paul M. Palevsky, M.D.
Chief, Renal SectionVA Pittsburgh Healthcare System
Professor of MedicineUniversity of Pittsburgh School of Medicine

Indications for Renal Support in Acute Kidney Injury
Volume overload Metabolic acidosis Hyperkalemia Uremic state
encephalopathy pericarditis
Azotemia without uremic manifestations Oliguria

Timing of Renal Replacement Therapy in AKI
“While there is increasing recognition of the value of earlier dialysis, the published consensus, and the practice in many centers at present, is still to apply dialysis to relatively ill rather than to relatively healthy patients”
-Teschan PE, et al: Ann Intern Med 1960; 53:992-1016

Timing of Renal Replacement Therapy in AKI
“We would urge that dialyses applied to patients who might otherwise survive should not under any circumstances be considered to be superfluous. Rather, the judgment of whether to undertake dialysis should also be made in view of the possible risks of not employing this procedure. We would question both the wisdom and the safety of subjecting patients to several days of avoidable nausea, vomiting, drowsiness and thirst, which not only implies significant discomfort to the patient but may also impose considerable risk of aspiration, pneumonia and other unexpected ‘complications’”
-Teschan PE, et al: Ann Intern Med 1960; 53:992-1016

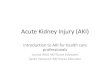
Timing of CVVHin Post-Traumatic AKI
39 %
20 %
0%
10%
20%
30%
40%
50%
60%
Surv
ival
BUN < 60 mg/dL BUN > 60 mg/dL
Gettings LG, et al: Intensive Care Med 1999; 25:805-813
(Mean: 42.6±12.9) (Mean: 94.5±28.3)n=41 n=59

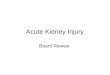
Timing of CVVHin Post-Cardiac Surgery AKI
22% 23.5%
43%
55.5%
0%
10%
20%
30%
40%
50%
60%
Mor
tali
ty
Early Late
Elahi Demirkilic
Elahi MM, et al: Eur J Cardiothorac Surg 2004; 26: 1027-1031Demirkilic U, et al: J Card Surg 2004; 19: 17-20
BUN ≥ 84 mg/dL,Cr >2.8 mg/dL, or
Potassium > 6 mEq/L
UOP < 100 mL for 8 hours
n=28n=36 n=27n=34
Cr >5.0 mg/dL, or Potassium > 5.5 mEq/L

Timing of RRT in AKI: PICARD Study Data
BUN ≤76 mg/dL(n=122)
BUN>76 mg/dL(n=121)
Mean BUN 47.4 mg/dL 114.9 mg/dL p<0.0001
Mean Creatinine 3.4 mg/dL 4.7 mg/dL p<0.0001
Failed Organ Systems 4 (IQR: 3-4) 3 (IQR: 2-4) p=0.008
Sepsis 37% 46% p=0.14
Initial RRT with CRRT 69% 43% p<0.001
Survival day 14 day 28
80%65%
75%59%
p=0.09
Adjusted mortality risk adjusted for covariates adjusted for propensity score adjusted for both covariates and propensity
1.85 (95% CI: 1.16-2.96)2.07 (95% CI: 1.30-3.29)1.97 (95% CI: 1.21-3.20)
Liu K et al. Clin J Am Soc Nephrol 2006; 1: 915-919

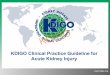
2011 Meta-Analysis of Timing of Initiation of RRT in AKI: Survival
Karvellas et al. Critical Care 2011 15:R72

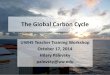
2012 Meta-Analysis of Timing of Initiation of RRT in AKI: Survival
Wang X, et al. Renal Fail 2012; 34: 396-402

Timing of RRT in AKI
Patients with Early AKI
Early RRT Late RRT
Recover without RRT
Diewithout RRT

74.3% 68.8% 75.0%
0%
20%
40%
60%
80%
100%
28-D
ay S
urvi
val
EHV ELV LLV
Treatment Group
Timing and Dose of CVVH in AKI
n=35
SOFA10.1±2.2
n=35
SOFA10.3±2.8
Bouman CS, et al. Critical Care Med 2002; 30:2205-2211
n=36
SOFA10.6±1.9

Earlier versus Usual Start of RRT in Community-Acquired AKI
Jamale TE, et al. Am J Kidney Dis 2013; 62:1116-1121

Earlier versus Usual Start of RRT in Community-Acquired AKI
Jamale TE, et al. Am J Kidney Dis 2013; 62:1116-1121
Baseline Data
Early Start Usual Start
BUN (mg/dL) 71.7±21.7 100.9±32.6
Creatinine (mg/dL) 7.4±5.3 10.4±3.3

Standard vs Accelerated initiation of Renal Replacement Therapy in Acute Kidney Injury (STARRT-AKI)
RCT comparing strategies of accelerated vs delayed initiation of RRT in critically ill patients with AKI
Pilot Phase Completed by Canadian Critical Care Trials Group 100 Patients Evaluated study feasibility
Definitive Phase International collaboration led by Ron Wald and Sean
Bagshaw Target enrollment 2,866 patients Target US enrollment: 920 patients

STARRT-AKI Pilot
Eligibility Criteria Presence of severe AKI (2 of the following)
Twofold increase in serum creatinine from baseline Urine output <6 ml/kg in the preceding 12 h, or Whole-blood NGAL ≥400 ng/ml)
<48 hours since doubling of serum creatinine Absence of urgent indications for RRT initiation (serum K+≤5.5 mmol/l and HCO3
-≥15 mmol/l)
Low likelihood of volume-responsive AKI (defined CVP≥8 mm Hg). Exclusions:
Lack of commitment to ongoing life support; Presence of an intoxication requiring RRT RRT within the previous 2 months; Clinical suspicion of renal obstruction, RPGN or AIN Pre-hospitalization eGFR<30 ml/min per 1.73 m2;
Equipoise among treating team (attending intensivist and nephrologist) Did treating physicians believe that either immediate RRT initiation or RRT deferral
was mandated.
Wald R, et al. Kidney Int e-published 8 July 2015

STARRT-AKI Pilot
Wald R, et al. Kidney Int e-published 8 July 2015

STARRT-AKI Pilot
Wald R, et al. Kidney Int e-published 8 July 2015
Treatment Group 90-day Mortality
Accelerated Initiation of RRT (n=48) 37.5%
Standard Initiation of RRT (n=52) 36.5%
Received RRT (n=33) 39.4%
Did not receive RRT (n=19) 31.6%

STARRT-AKI Definitive Phase:Eligibility Criteria
Inclusion Criteria Age ≥18 years and receiving care in an ICU Early severe AKI
KDIGO stage 2/3 AKI Serum creatinine not >3x baseline for >48 hours
Equipoise regarding timing of RRT for the individual patient based on: Absence of metabolic criteria predicting need for RRT within the
next 24 hours: Serum potassium>5.5 mmol/L Total CO2 <15 mmol/L
Absence of drug intoxication requiring RRT Agreement by treating physicians that RRT does not need to be
initiated immediately but with no objection to the possibility of immediate initiation

STARRT-AKI Definitive Phase:Eligibility Criteria
Exclusion Criteria Lack of commitment to ongoing life support, including RRT AKI resulting from a potentially treatable etiology History of pre-existing kidney disease defined by:
RRT in previous 2 months Kidney transplant within past year; Known advanced CKD
with eGFR<20 mL/min/1.73 m2

STARRT-AKI Definitive Phase:Treatment Groups
Accelerated RRT Initiation Dialysis Catheter to be placed and RRT initiated as soon as possible within 12
hours of eligibility
Delayed RRT Initiation
Persistent severe AKI defined as Screat that remains >50% of value at
randomization AND at least one of the following: K+ ≥ 6.0 mmol/L;
pH < 7.20 or tCO2 ≤ 12 mmol/L; or
Evidence of severe respiratory failure based on PaO2/FiO2 < 200 with volume overload
or Persistent severe AKI for >72 hours from randomization The decision to initiate RRT in the delayed arm will be made by the treating
physicians and not by research personnel

STARRT-AKI Definitive Phase:RRT Management
Other than timing of initiation of RRT, all other aspects of RRT will be based on usual care guided by accepted clinical practice guidelines
RRT will be continued until Death; Withdrawal of life support; or Kidney function recovery as per treating physician’s
judgment

STARRT-AKI Definitive Phase:Endpoints
Primary outcome 90-day all-cause mortality
Secondary outcomes Dialysis-dependence at 90 days Patient self-assessment of HRQoL and functional status
Tertiary outcomes eGFR among patients alive at day 90 Major adverse kidney events (MAKE)
Death RRT dependence eGFR <75% of baseline eGFR at 90 days

STARRT-AKI Definitive Phase:Sample Size
Assumptions: 40% 90-day all cause mortality in delayed RRT
initiation arm 34% 90-day all cause mortality in accelerated RRT
initiation arm (absolute risk reduction of 6%; relative risk reduction of 15%)
3% loss to follow-up α=0.05 1-β=0.90
Sample size: 2,866

STARRT-AKI Trials Group
International Study Chairs Ron Wald (Toronto, ON) Sean Bagshaw (Edmonton, AB)
Data Management & Coordinating Center Applied Health Research Center, St. Michael’s Hospital, Toronto
International Steering Committee Canada – Ron Wald & Sean Bagshaw United Kingdom – Marlies Ostermann Austria – Michael Joannidis Finland – Ville Pettilä Australia – Rinaldo Bellomo & Martin Gallagher New Zealand – Shay McGuiness United States – Paul Palevsky & Kathleen Liu

STARRT-AKI United States Consortium US Steering Committee
Paul M. Palevsky, US Study Chair Kathleen D. Liu, US Study Co-Chair
US Clinical Sites Beth Israel Deaconess Medical Center, Boston, MA - Ali Poyan Mehr & Daniel
Talmor Brigham & Women’s Hospital, Boston, MA – Sushrut Waikar Cleveland Clinic, Cleveland, OH – Sevag Demirjian Massachusetts General Hospital, Boston, MA – John Niles University of Alabama, Birmingham, AL – Ashita Tolwani University of California, San Francisco, CA – Kathleen Liu University of Chicago, Chicago, IL – Jay Koyner University of Miami, Miami, FL – Gabriel Contreras & Roland Schein University of Pittsburgh, Pittsburgh, PA - Raghavan Murugan & Chethan
Puttarajappa University of Texas HSC, Houston, TX – Kevin Finkel Vanderbilt University, Nashville, TN – Edward Siew Washington University, St. Louis, MO – Anitha Vijayan