Embed Size (px)
Citation preview

Transplant Immunology xxx (2014) xxx–xxx
TRIM-00909; No of Pages 6
Contents lists available at ScienceDirect
Transplant Immunology
j ourna l homepage: www.e lsev ie r .com/ locate / t r im
Time elapsed after transplantation influences the relationship betweenthe number of regulatory T cells in lung allograft biopsies and subsequentacute rejection episodes
Dorrit Krustrup a,⁎, Martin Iversen b, Torben Martinussen c, Claus B. Andersen a
a Department of Pathology, Copenhagen University Hospital, Rigshospitalet, Denmarkb The Heart and Lung Transplantation Unit, Copenhagen University Hospital, Rigshospitalet, Denmarkc Department of Biostatistics, University of Copenhagen, Denmark
⁎ Corresponding author at: Department of Pathology, CRigshospitalet, Blegdamsvej 9, 2100 Copenhagen, Denmar
E-mail address: [email protected] (D. Krustr
http://dx.doi.org/10.1016/j.trim.2014.04.0070966-3274/© 2014 Elsevier B.V. All rights reserved.
Please cite this article as: KrustrupD, et al, Timin lung allograft biopsies..., Transpl Immunol
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 5 February 2014Received in revised form 19 April 2014Accepted 23 April 2014Available online xxxxKeywords:Lung transplantationRegulatory T cellAcute rejectionFoxP3
Background: Regulatory T lymphocytes (Tregs) play an important role in acute rejection after lung transplanta-tion. However, the importance of the time elapsed after transplantation on the Treg response requires further in-vestigation.We aim to evaluate the change over time in the frequency of Tregs in lung allograft biopsies and to assess howTregs relate to simultaneous and subsequent acute cellular rejection.Materials and methods: A total of 258 biopsy samples obtained 0.5, 1, 3, 12 and 24 months after transplantationfrom 58 consecutive lung transplant patients were included. The biopsieswere scored for acute rejection accord-ing to the ISHLT criteria (A0–A4) and immunohistochemically stained with antibodies against FoxP3.Results: Therewas a tendency for a decrease in the number of Tregs/mm2with time. However, the previous levelsof Tregs/mm2 did not have any significant effect on future levels of Tregs/mm2. For biopsies taken 0.5 and
1 month after transplantation, a significant correlation between Tregs/mm2 and the degree of acute rejectionwas found, and logistic regression analysis using updated values for Tregs/mm2 showed a significant relationshipbetweenTregs/mm2 at 2 weeks and anA-score≥2 after 1 and 3 months. At later timepoints, this correlation dis-appeared.Discussion and conclusion:Our data indicate that the time elapsed after transplantation is an important parameterinfluencing the Treg response after lung transplantation. This observation is in accordancewith studies indicatinga narrow therapeuticwindow for induction of tolerance by specifically targeting T-cells. The results also indirect-ly indicate that Tregs early after transplantation could have an impact on the long-term outcome.© 2014 Elsevier B.V. All rights reserved.
1. Introduction
Aftermore than two decades of lung transplantation, short term sur-vival has improved significantly, but long term survival is still relativelypoor, mainly due to obliterative bronchiolitis, sometimes referred to aschronic allograft dysfunction [1]. The most significant known risk factorfor this condition is acute cellular rejection [2–6], and a better under-standing of the complex immunologic background for acute rejectionis needed to further improve survival and reduce morbidity for this pa-tient group.
One of the interesting participants in the immunologic response totransplantation is a subpopulation of T lymphocytes with suppressorfunction known as regulatory T lymphocytes (Tregs) [7–9]. These cellsare thought to play an important role in the process of acute rejection
openhagen University Hospital,k. Tel.: +45 35 45 54 57.up).
e elapsed after transplantatio(2014), http://dx.doi.org/10.
after lung transplantation [10], and the long term outcome is consideredto be influenced by the balance between Tregs and T-effector cells [11].However, the plasticity of these cells and the importance of the local mi-croenvironment on their function complicate research into their role inthis process.
Forkhead Box P3 (FoxP3) protein is a marker of Tregs [12–16]. It isalso expressed by activated effector T cells, but only transiently and toa significantly lower degree [17]. Other subsets of FoxP3 negative regu-latory T cells exist, but have been less extensively studied. In the follow-ing text, the term “Tregs” refers to FoxP3 positive T cells including both“natural” Tregs originating from the thymus and “induced” Tregs arisingfrom peripheral T-effector cells.
Previous studies have shown a relation between the number and ac-tivity of Tregs in lung allograft tissue and the rejection status of the pa-tient [10,18], but the results vary [19], perhaps among other thingsbecause these studies have been performed at different time pointsafter transplantation. Because the immunologic response evolves overtime, one hypothesis is that there would be a time point with the
n influences the relationship between the number of regulatory T cells1016/j.trim.2014.04.007

Table 1Recipient demographics for all 58 patients included in the study.
Mean recipient age (years) 42 (14–66)Recipient gender (male:female) 25:33Recipient diagnosisA1AT deficiency 7 (12%)CF 20 (34%)COPD and emphysema 15 (26%)Pulmonary fibrosis 6 (10%)Pulmonary hypertension 2 (3%)Sarcoidosis 8 (14%)
Transplant procedureSingle-lung 26Double-lung 31Heart–Lung 1
A1AT: alfa-1-antitrypsin deficiency, CF: cystic fibrosis, COPD: chronic obstructive pulmonarydisease.
2 D. Krustrup et al. / Transplant Immunology xxx (2014) xxx–xxx
greatest predictive value regarding future rejection episodes. However,the development of the Treg response over time has not been thorough-ly investigated.
Furthermore, previous studies regarding lung transplant patientshave primarily focused on the frequency of Tregs in the bronchoalveolarlavage fluid (BALF) and the blood [20–23]. In an earlier study, weshowed that the level of FoxP3mRNA in BALF corresponded to thenum-ber of FoxP3 positive cells per tissue square millimeter (Tregs/mm2) intransbronchial allograft biopsies taken at the same time [18]; how-ever, to our knowledge, the frequency of Tregs in lung tissue, thepresumed site of major activity, has not been systematically investi-gated. In addition, previous studies have used different methods tomeasure Tregs, such as the percentage of CD4+ or CD3+ cells ortheir percentage out of the total number of cells, but these differentmethods have not been validated to identify which has the greatestpredictive value. Our study focuses on the number of Tregs relativeto lung tissue area based on the idea that the effect of Tregs mightbe so abundant that the intensity of the lymphocytic infiltrate is ofless importance.
2. Objective
The purpose of this study is to evaluate the change over time in thefrequency of Tregs in lung allograft biopsies and to assess how thefrequency of Tregs relates to simultaneous and subsequent acute
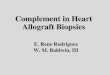
Fig. 1. Examples of immunohistochemical stainingwith antibodies against FoxP3 in lung tissue(A1), C) mild acute cellular rejection (A2), and D) moderate acute cellular rejection (A3). Treglegend, the reader is referred to the web version of this article.)
Please cite this article as: KrustrupD, et al, Time elapsed after transplantatioin lung allograft biopsies..., Transpl Immunol (2014), http://dx.doi.org/10.
cellular rejection. We focused on the number of Tregs/mm2 in lung tis-sue as the measurement of interest.
3. Material and methods
3.1. Material
A total of 258 transbronchial biopsy samples from58patients partic-ipating in the surveillance follow-up program after lung transplantationwere included. These comprised available biopsies obtained 0.5, 1, 3, 12and 24 months after transplantation from all patients that had alung transplantation performed in Copenhagen University Hospital,Rigshospitalet, Denmark, during 2005 or 2006. Of the initial 60 con-secutive patients, 2 died shortly after the surgical procedure andwere excluded from the study.
Demographic data on the study population is summarized in Table 1.An insufficient amount of tissue for immunohistochemical evaluation
was found in 25 of the samples, and for those biopsies only the degree ofacute rejection was noted. For the remaining 233 biopsy samples, thenumber of Tregs/mm2 was calculated as described below.
The number of time points with available biopsy samples varied be-tween 1 and 5 per patient, and the total number of biopsy samples foreach time point varied between 36 and 50. In the study, 43 patientshad at least 4 sufficient biopsies included.
The details of the immunosuppressive treatment and follow-uphave been described previously [1]. Briefly, all patients received initialstandard immunosuppression consisting of induction therapy withantithymocyte globulin (ATG, 1.5 mg/kg for 3 days); cyclosporineand azathioprine with prednisolone as maintenance therapy; and sched-uled biopsies at 2, 4, 6, and 12 weeks and 6, 12, 18 and 24 months aftertransplantation.
The biopsies were scored for acute cellular rejection according to theISHLT criteria (A0-A4) by one pathologist (CBA) [24].
The study was approved by the Ethical Committee of Copenhagen.
3.2. Immunohistochemical staining of biopsies and subsequent digitalimaging
The transcription factor FoxP3 was used as a marker for Tregs,and immunohistochemistry was performed on formalin-fixedparaffin-embedded tissue with monoclonal antibodies against FoxP3(236A/E7, 14-4777, eBioscience, San Diego, CA, USA) according to the
from a patient with: A) no acute cellular rejection (A0), B)minimal acute cellular rejections show a red staining nucleus. (For interpretation of the references to color in this figure
n influences the relationship between the number of regulatory T cells1016/j.trim.2014.04.007

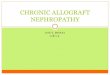
Fig. 2. Fluctuations in the number of Tregs/mm2 over time for the first 3 months (2a) and for the entire 2 year period (2b).
3D. Krustrup et al. / Transplant Immunology xxx (2014) xxx–xxx
recommendations from themanufacturer. Sectionsweremanually evalu-ated by one observer (DK). A positively stained cell was defined as havinga distinctly positive nuclear reaction (Fig. 1).
Table 2The mean number of Tregs/mm2 for samples taken at 0.5 month. The samples are grouped on
Months Mean Tregs/mm2, all samples (95% conf. interval) Mean Tregs/mm2, cM
0.5 14.23(9.81–20.65)
9.51(5.87–15.41)
Please cite this article as: KrustrupD, et al, Time elapsed after transplantatioin lung allograft biopsies..., Transpl Immunol (2014), http://dx.doi.org/10.
All slides were scanned using a Pannoramic Midi slide scanner from3D Histech, and afterwards, the digital images were processed usingVisiopharm Quantitative Digital Pathology software. A computerized
the basis of the cMARS values of the patients.
ARS b 1 (95% conf. interval) Mean Tregs/mm2, cMARS ≥ 1 (95% conf. interval)
24.52(14.32–41.96)
n influences the relationship between the number of regulatory T cells1016/j.trim.2014.04.007

0
2
4
6
8
10
12
14
16
0 10 20 30
Mean Tregs/mm2
Months
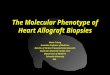
Fig. 3. The mean number of Tregs/mm2 for samples taken at each time point.
Table 4Odds ratio (OR) for acute rejection grade 2 or higherwhen increasing thenumber of Tregs/mm2 by 10 given with 95% confidence limits.
Time after transplantation, months OR 95% confidence limits
0.5 1.24 1.02–1.511 1.69 1.24–2.313 1.27 0.84–1.9112 0.91 0.57–1.43
4 D. Krustrup et al. / Transplant Immunology xxx (2014) xxx–xxx
algorithmwas established to calculate the total tissue area excluding al-veolar spaces for each biopsy sample.
The results were expressed as the number of positive cells per squaremillimeter (Tregs/mm2).
3.3. Statistical analysis
Statistical analyses were performed using SAS Enterprise Guidestatistical software (version 4.3) and R (version 3.0.2).
We applied repeated measures ANOVA to analyze the number ofTregs/mm2 using time as the explanatory variable. Before running theanalysis, Tregs/mm2 was transformed to log10 (Tregs/mm2 + 1). Wealso performed consecutive regression analysis in which we comparedTregs/mm2 to previously measured values of Tregs/mm2.
To investigate the effect of Tregs/mm2 on acute rejection (A-score),we applied logistic regression, dichotomizing the A-score as A ≤ 1 (A0and A1) and A≥ 2 (A2 and A3). To take into account the repeatedmea-surements from the same patients, the analysis was performed usingthe generalized estimating (GEE) approach under theworking indepen-dence assumption [25]. The analysis was performed with updatedvalues of Tregs/mm2, meaning that the estimation was performedwith the relevant values at each of the different time points. We alsoanalyzed the effect of the Tregs/mm2 value measured after 2 weeks onthe following A-score measurements, and similarly with the Tregs/mm2
measured at 1 month and3 months. TheobservedA-scores at 24 monthswere not used as therewas only onepatientwith anA-score larger than1.
Fluctuations in the number of Tregs were calculated as the mean ofthe log10 (Tregs/mm2 + 1) with 95% confidence intervals for eachtime point and are shown as the corresponding value after back-transformation.
The cumulativemean acute rejection score (cMARS) for each patientwas calculated by summing the acute rejection scores at each time pointand dividing by the number of biopsies [26]. This approach was chosento compensate for the different number of observations per individual,but it is important to be aware that there are limitations to the interpre-tation of this parameter as A-score is an ordinal variable. Furthermore,cMARS could be flawed since it will be heavily weighted by a significantnumber of A1 rejection episodes, which are not viewed as clinicallysignificant.
Table 3Biopsy samples for each time point grouped according to acute rejection grade.
Acute rejection grade 0.5 month 1 m
A0 23 19A1 18 20A2 7 16A3 6 3A4 0 0Total number of rejection episodes (A1–A4) 31 39
Please cite this article as: KrustrupD, et al, Time elapsed after transplantatioin lung allograft biopsies..., Transpl Immunol (2014), http://dx.doi.org/10.
Linear regression analysis using robust standard errorwas applied toanalyze cMARS against log10 (Tregs/mm2 + 1) at 0.5 months. Thisanalysis only assumes that the mean is correctly specified, avoiding anassumption of the normality of residuals.
A p-value b 0.05 was considered statistically significant.
4. Results
4.1. The fluctuations in the number of Tregs/mm2 over the time elapsed after transplantationwere not correlated between time points
Fluctuations in the frequency of Tregs over time for each patient are shown in Fig. 2aand b for the first 3 months as well as over the whole 2 year period.
Themean levels of Tregs/mm2 after 0.5 months for thewhole group and for the patientswith a cMARS value b1 and ≥1 are listed in Table 2, and the mean levels of Tregs/mm2 foreach time point are depicted graphically in Fig. 3.
The highest mean number of Tregs/mm2 was observed after 2 weeks. There was atendency for Tregs/mm2 numbers to decrease with time, but this was only significantwhen comparing the initial level at 2 weeks to the level at 12 months, with a decreaseof 37% (p = 0.048).
However, the consecutive regression analysis showed that previous Tregs/mm2
numbers did not have any significant effect on future Tregs/mm2 numbers.
4.2. The time elapsed after transplantation influenced the correlation between acute cellularrejection and the number of Tregs/mm2
Acute rejection was more prevalent in biopsies obtained early after transplantation,with the highest number of rejection episodes diagnosed after 1 month (Table 3). For bi-opsies collected 0.5 and 1 month after transplantation, a significant correlation was foundby logistic regression between the number of Tregs/mm2 and the degree of acute rejectionassessed at the same time point. Increasing numbers of Tregs/mm2 with 10 results in anodds ratio (OR) for A ≥ 2 of 1.24 (1.02–1.51) at 0.5 month and an OR of 1.69 (1.24–2.31) at 1 month. At later time points, there was no significant effect (Table 4).
4.3. The number of Tregs/mm2 early after transplantationwas related to subsequent acute cel-lular rejection
Logistic regression analysis with updated values for Treg/mm2 showed a significantrelationship between the number of Tregs/mm2 at 2 weeks and an A-score ≥ 2 after 1and 3 months. However, for Tregs/mm2 numbers at later time points, this correlation dis-appeared (Table 5).
Linear regression analysis showed a significant relationship between the number ofTregs/mm2 at 0.5 month and the cMARS value (estimated regression coefficient 0.527(95%-confidence interval: 0.358, 0.696), p b 0.001) (Fig. 4).
5. Discussion
Our data show that the number of Tregs in lung tissue fluctuates overtime –particularly during thefirst fewmonths after transplantation – andthat the time elapsed after transplantation is an important parame-ter influencing the relationship between the regulatory T-cell re-sponse and acute cellular rejection. In addition, we found that thenumber of Tregs in lung allograft tissue early after transplantation
onth 3 months 12 months 24 months
28 32 2914 13 1012 6 11 0 00 0 0
27 19 11
n influences the relationship between the number of regulatory T cells1016/j.trim.2014.04.007

Table 5Tregs at each time point (horizontal) compared to subsequent A-score.
0.5 month (Tregs) 1 month (Tregs) 3 months (Tregs)
Time after transplantation (A-score) OR 95% conf. limits OR 95% conf. limits OR 95% conf. limits
0.5 1.24 1.02–1.51 – – – –
1 1.86 1.32–2.60 1.69 1.24–2.31 – –
3 1.34 1.08–1.67 0.90 0.64–1.26 1.27 0.84–1.9112 1.09 0.83–1.44 0.92 0.67–1.26 0.71 0.35–1.44
Results are expressed as the odds ratio (OR) for A ≥ 2 when increasing the number of Tregs/mm2 by 10, given with 95% confidence limits for each time point.
5D. Krustrup et al. / Transplant Immunology xxx (2014) xxx–xxx
has a predictive value towards the number and severity of subse-quent rejection episodes, whereas Treg numbers at later time pointsdo not have a predictive value.
The comparison of our results with previous studies is complicatedby the different approaches used to assess Tregs. Our results indicatethat time is an important factor to consider when designing or evaluat-ing studies in this field, as different results might be obtained from ob-servations made at different time points after transplantation. Theobservation that there is a relationship between Tregs and acute rejec-tion is in accordance with some previous studies examining BALF andblood [20] but is in conflict with other studies [22].
In this study, we used acute cellular rejection as the response vari-able for the statistical analysis. There have been previous indicationsthat Tregs increase in number after acute rejection and decrease in asetting of prolonged rejection quiescence [10], but the exact cause andeffect relationship between rejection and Tregs could not be determinedin this study. Further elucidation of this association would requireseveral biopsy samples taken over short time intervals. Our choice ofA-score as the response variable was based on the assumption that ahistologically identified acute rejection is a response to a preceding im-munological recipient–donor situation, and tissue damage histologicallyscored as a rejection would therefore represent a consequence of theimmunologic response including the regulatory response.
The explanation for the observed results cannot be fully determinedbased on the present data, but the observations are in accordance withstudies indicating a narrow therapeutic window for inducing toleranceby specifically targeting T-cells [27,28].
Fig. 4. Number of Tregs/mm2 2 weeks after transplantation comp
Please cite this article as: KrustrupD, et al, Time elapsed after transplantatioin lung allograft biopsies..., Transpl Immunol (2014), http://dx.doi.org/10.
Few studies are based on tissue samples, and often the frequency ofTregs compared to other T cells is used as a measurement. We foundthat an easily performed immunohistochemical approach to countTregs/mm2 in tissue from surveillance biopsies is a reliable measure-ment method that correlates well with acute rejection status in earlypost-transplantation biopsies.
It could be thought that the observed fluctuations in the number ofTregs/mm2 were a result of general fluctuations in the total number oflymphocytes in the surrounding tissue. However, even though ourdata showed a certain degree of concordance between CD3+T lympho-cytes and FoxP3 positive Tregs, the variance was large. Although thepercentage of Tregs of the total number of T cells showed the sametrends regarding a relationship to acute rejection, the correlation wasmuch weaker. A possible explanation could be that the effect of Tregsis particularly intense in the affected area regardless of the number ofother inflammatory cells.
There are a number of limitations to this retrospective study. Thepopulation size was limited to 58 patients, and some of the Treg valuesand rejection status information was missing due to insufficient tissueor because the patient died or was too fragile for the biopsy procedure.The numbers of missing valueswere larger for the later time points, andthe mean value for Tregs and the acute rejection score for these timepointswere based on fewer observations. Also, the frequency and sever-ity of acute rejection episodes were higher during the earlier timepoints. The immunosuppressive treatment of acute rejection grade 2 orhigher could hypothetically influence the regulatory response in subse-quent biopsies, especially for the time points early after transplantation
ared to the cumulative mean acute rejection score (cMARS).
n influences the relationship between the number of regulatory T cells1016/j.trim.2014.04.007

6 D. Krustrup et al. / Transplant Immunology xxx (2014) xxx–xxx
when the intervals between biopsies are shorter. Finally, it has beenpointed out that the level of FoxP3 proteinwithin the cell might influencethe regulatory effect [11], but in this study we did not differentiate be-tween weak and strong FoxP3 staining because of the potentially highlevel of variability.
In conclusion, because acute rejection is a known risk factor forchronic allograft dysfunction, the data indirectly indicate that Tregsmight affect the development of chronic allograft dysfunction andlong-term outcome. However, further studies examining the Treg re-sponse are required to estimate the time point with the greatest prog-nostic significance relating to long-term outcome.
Disclosure statement
None of the authors has any financial relationshipwith a commercialentity that has an interest in the subject of the presented manuscript orother conflicts of interest to disclose.
References
[1] Burton CM, Carlsen J, Mortensen J, Andersen CB, Milman N, Iversen M. Long-termsurvival after lung transplantation depends on development and severity of bron-chiolitis obliterans syndrome. J Heart Lung Transplant 2007;26(7):681–6.
[2] Burton CM, Iversen M, Carlsen J, Mortensen J, Andersen CB, Steinbruchel D, et al.Acute cellular rejection is a risk factor for bronchiolitis obliterans syndromeindependent of post-transplant baseline FEV1. J Heart Lung Transplant2009;28(9):888–93.
[3] Girgis RE, Tu I, Berry GJ, Reichenspurner H, Valentine VG, Conte JV, et al. Risk factorsfor the development of obliterative bronchiolitis after lung transplantation. J HeartLung Transplant 1996;15(12):1200–8.
[4] Hopkins PM, Aboyoun CL, Chhajed PN, Malouf MA, Plit ML, Rainer SP, et al. Associa-tion ofminimal rejection in lung transplant recipients with obliterative bronchiolitis.Am J Respir Crit Care Med 2004;170(9):1022–6.
[5] Khalifah AP, Hachem RR, Chakinala MM, Yusen RD, Aloush A, Patterson GA, et al.Minimal acute rejection after lung transplantation: a risk for bronchiolitis obliteranssyndrome. Am J Transplant 2005;5(8):2022–30.
[6] Hachem RR, Khalifah AP, Chakinala MM, Yusen RD, Aloush A, Mohanakumar T, et al.The significance of a single episode of minimal acute rejection after lung transplan-tation. Transplantation 2005;80(10):1406–13.
[7] Roncarolo MG, Battaglia M. Regulatory T-cell immunotherapy for tolerance to selfantigens and alloantigens in humans. Nat Rev Immunol 2007;7(8):585–98.
[8] Wood KJ, Sakaguchi S. Regulatory T cells in transplantation tolerance. Nat RevImmunol 2003;3(3):199–210.
[9] Yong Z, Chang L, Mei YX, Yi L. Role and mechanisms of CD4+CD25+ regulatory Tcells in the induction and maintenance of transplantation tolerance. TransplImmunol 2007;17(2):120–9.
Please cite this article as: KrustrupD, et al, Time elapsed after transplantatioin lung allograft biopsies..., Transpl Immunol (2014), http://dx.doi.org/10.
[10] Neujahr DC, Cardona AC, Ulukpo O, Rigby M, Pelaez A, Ramirez A, et al. Dynamics ofhuman regulatory T cells in lung lavages of lung transplant recipients. Transplanta-tion 2009;88(4):521–7.
[11] Li XC, Turka LA. An update on regulatory T cells in transplant tolerance and rejection.Nat Rev Nephrol 2010;6(10):577–83.
[12] Yagi H, Nomura T, Nakamura K, Yamazaki S, Kitawaki T, Hori S, et al. Crucial role ofFOXP3 in the development and function of human CD25+CD4+ regulatory T cells.Int Immunol 2004;16(11):1643–56.
[13] Hori S, Nomura T, Sakaguchi S. Control of regulatory T cell development by the tran-scription factor Foxp3. Science 2003;299(5609):1057–61.
[14] Fontenot JD, Rasmussen JP, Williams LM, Dooley JL, Farr AG, Rudensky AY. Regulato-ry T cell lineage specification by the forkhead transcription factor foxp3. Immunity2005;22(3):329–41.
[15] Fontenot JD, Gavin MA, Rudensky AY. Foxp3 programs the development and func-tion of CD4+CD25+ regulatory T cells. Nat Immunol 2003;4(4):330–6.
[16] Hori S, Sakaguchi S. Foxp3: a critical regulator of the development and function ofregulatory T cells. Microbes Infect 2004;6(8):745–51.
[17] Allan SE, Crome SQ, Crellin NK, Passerini L, Steiner TS, Bacchetta R, et al. Activation-induced FOXP3 in human T effector cells does not suppress proliferation or cytokineproduction. Int Immunol 2007;19(4):345–54.
[18] Krustrup D,Madsen CB, Iversen M, Engelholm L, Ryder LP, Andersen CB. The numberof regulatory T cells in transbronchial lung allograft biopsies is related to FoxP3mRNA levels in bronchoalveolar lavage fluid and to the degree of acute cellularrejection. Transpl Immunol 2013;29(1–4):71–5.
[19] Gregson AL, Hoji A, Saggar R, Ross DJ, Kubak BM, Jamieson BD, et al. Bronchoalveolarimmunologic profile of acute human lung transplant allograft rejection. Transplanta-tion 2008;85(7):1056–9.
[20] San SD, Brunet M, Ballesteros MA, Millan O, Muro M, Castro MJ, et al. Prospectivestudy of biomarkers of immune response in lung transplant recipients. TransplantProc 2012;44(9):2666–8.
[21] Madsen CB, Norgaard A, Iversen M, Ryder LP. Elevated mRNA levels of CTLA-4,FoxP3, and granzyme B in BAL, but not in blood, during acute rejection of lung allo-grafts. Transpl Immunol 2010;24(1):26–32.
[22] Bhorade SM, Chen H, Molinero L, Liao C, Garrity ER, Vigneswaran WT, et al. De-creased percentage of CD4+FoxP3+ cells in bronchoalveolar lavage from lungtransplant recipients correlates with development of bronchiolitis obliterans syn-drome. Transplantation 2010;90(5):540–6.
[23] Satoda N, Shoji T, Wu Y, Fujinaga T, Chen F, Aoyama A, et al. Value of FOXP3 expres-sion in peripheral blood as rejection marker after miniature swine lung transplanta-tion. J Heart Lung Transplant 2008;27(12):1293–301.
[24] Stewart S, Fishbein MC, Snell GI, Berry GJ, Boehler A, Burke MM, et al. Revision of the1996 working formulation for the standardization of nomenclature in the diagnosisof lung rejection. J Heart Lung Transplant 2007;26(12):1229–42.
[25] Liang K-Y, Zeger S. Longitudinal data analysis using generalized linear models.Biometrika 1986;73(1):13–22.
[26] Burton CM, Iversen M, Scheike T, Carlsen J, Andersen CB. Minimal acute cellular re-jection remains prevalent up to 2 years after lung transplantation: a retrospectiveanalysis of 2697 transbronchial biopsies. Transplantation 2008;85(4):547–53.
[27] Parekh K, Trulock E, Patterson GA. Use of cyclosporine in lung transplantation. Trans-plant Proc 2004;36(2 Suppl.):318S–22S.
[28] Bhorade SM, Stern E. Immunosuppression for lung transplantation. Proc Am ThoracSoc 2009;6(1):47–53.
n influences the relationship between the number of regulatory T cells1016/j.trim.2014.04.007