Embed Size (px)
Citation preview
Appendix 1
Tihei Wairarapa - Progress report
1. PURPOSE This report provides an update on progress made to the Tihei Wairarapa business case. This was developed by a partnership of stakeholders with an interest in community-based healthcare in the Wairarapa. The business case set the five year (2010 – 2015) direction for progressing delivery to the Primary Health Care Strategy in the Wairarapa, and the Government’s promise of “Better, Sooner, More Convenient” health care. Key questions addressed in this report are:
Has the programme met the aspirational targets of the business case? Has the programme been delivered in accordance to the Alliance Charter? Has the Tihei programme been successfully implemented? What lessons have been learnt over the last three years? What could help further progress over the next two years?
Information to answer these questions has been gathered through a review of programme documentation, and 14 interviews with primary care, Compass Health and WDHB staff (former and current) involved with Tihei’s implementation1, and the person responsible for Ministry of Health liaison. This report will inform the development of a strategic plan for the next two years of the programme.
2. BACKGROUND Work on the business case was led by an alliance of Wairarapa Community Primary Health Organisation (WCPHO), Compass Health and the Wairarapa District Health Board (WDHB). Original problem definition
The business case aimed to address problems facing the district including: the ageing population and escalating incidence and impact of long term conditions;
poor health outcomes for Māori, Pacific, people living with high deprivation, and people living with long-term mental illness;
sector wide workforce constraints and restraints;
unnecessary levels of primary care services being provided in the secondary care setting;
1 People interviewed for this report are: Chris Kerr (Compass Health), Tony Becker (GP and former ALT chair), Annie Lincoln (GP and former GP liaison), Steve Phillips (GP and former ALT member), David Holt (pharmacist and former and current ALT member), Tracey Adamson (former CEO, WDHB), Allan Shirley (former ALT member and WDHB Chief Medical Officer), Berni Marra (former programme director), Lisa Burch (SIDU, WDHB), Hilary Ryan (GP and former ALT member and mental health project lead), Yvette Grace (Compass Health), John Baird (MoH liaison), Tim Mathews (aged care lead, WDHB), Cathy O’Malley (former CEO, Compass Health).
rigid primary care contracting models, acting as an impediment to the development of the Integrated Family Health Centre network;
limited funding increases forecasted, with reductions of funding and efficiencies expected to be realised from the existing PHO infrastructure; and the
need to improve the sustainability of WDHBs funding and service provision - at the time WDHB was in deficit and looking to save $4m.
The business case sought to reduce these problems through the formalisation of an alliance and the implementation of a set of initiatives or projects. This would occur within existing funding streams and through collaboration between providers and health professionals across the district and region.
Programme overview
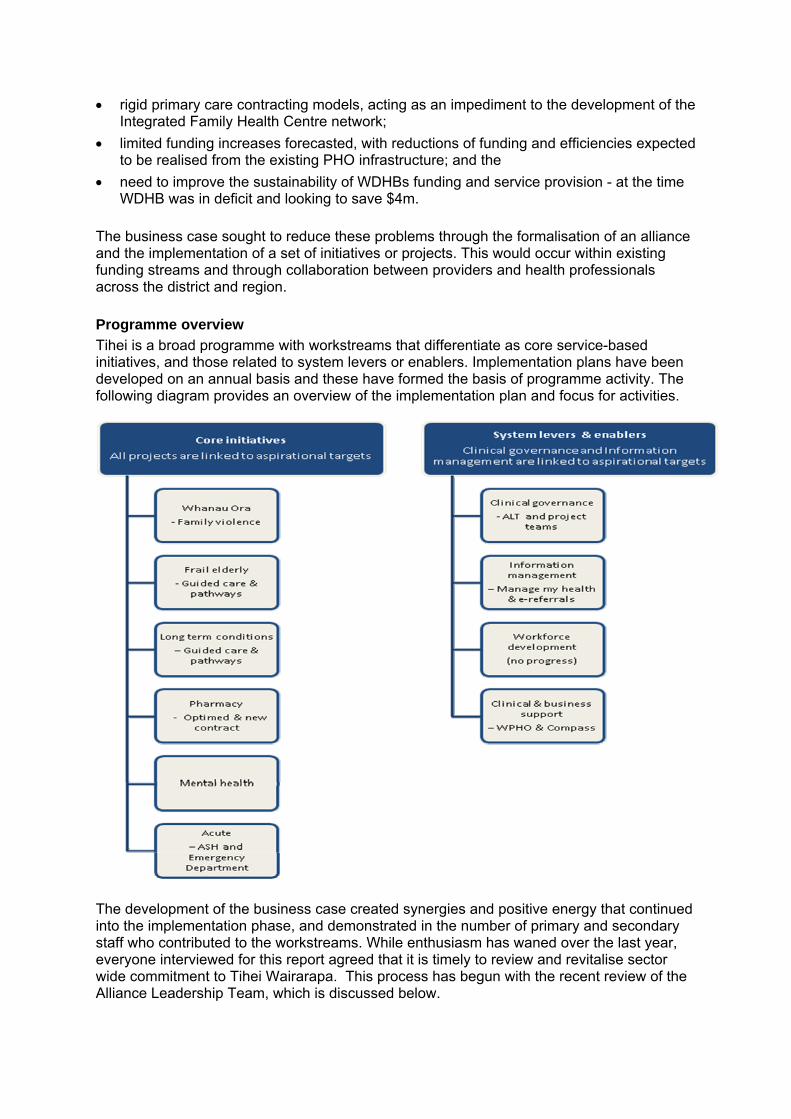
Tihei is a broad programme with workstreams that differentiate as core service-based initiatives, and those related to system levers or enablers. Implementation plans have been developed on an annual basis and these have formed the basis of programme activity. The following diagram provides an overview of the implementation plan and focus for activities.
The development of the business case created synergies and positive energy that continued into the implementation phase, and demonstrated in the number of primary and secondary staff who contributed to the workstreams. While enthusiasm has waned over the last year, everyone interviewed for this report agreed that it is timely to review and revitalise sector wide commitment to Tihei Wairarapa. This process has begun with the recent review of the Alliance Leadership Team, which is discussed below.
3. PROGRESS TOWARDS THE ASPIRATIONAL TARGETS The business case outlined three sets of targets based on the ‘triple aim’ and these are to:
Improve the health of the whole population Improve the patient experience Reduce and control healthcare costs in the Wairarapa
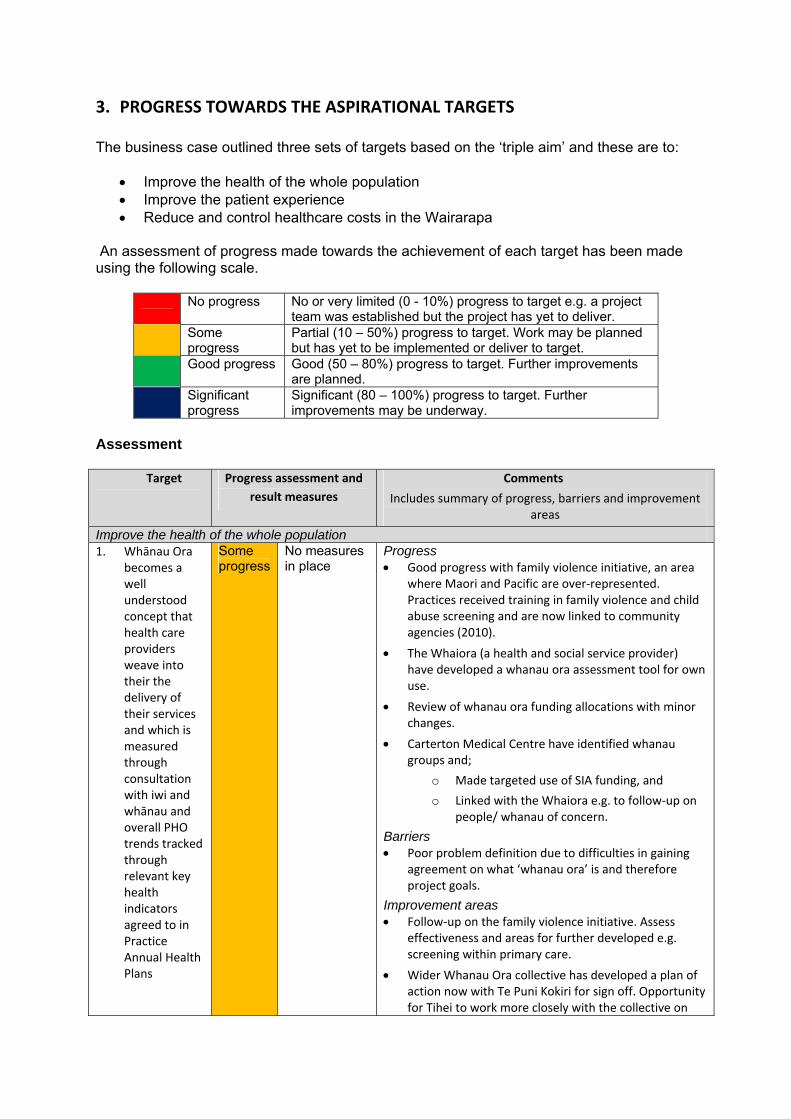
An assessment of progress made towards the achievement of each target has been made using the following scale.
No progress No or very limited (0 - 10%) progress to target e.g. a project
team was established but the project has yet to deliver. Some
progress Partial (10 – 50%) progress to target. Work may be planned but has yet to be implemented or deliver to target.
Good progress Good (50 – 80%) progress to target. Further improvements are planned.
Significant progress
Significant (80 – 100%) progress to target. Further improvements may be underway.
Assessment
Target Progress assessment and
result measures
Comments
Includes summary of progress, barriers and improvement areas
Improve the health of the whole population1. Whānau Ora
becomes a well understood concept that health care providers weave into their the delivery of their services and which is measured through consultation with iwi and whānau and overall PHO trends tracked through relevant key health indicators agreed to in Practice Annual Health Plans
Some progress
No measures in place
Progress Good progress with family violence initiative, an area
where Maori and Pacific are over‐represented. Practices received training in family violence and child abuse screening and are now linked to community agencies (2010).
The Whaiora (a health and social service provider) have developed a whanau ora assessment tool for own use.
Review of whanau ora funding allocations with minor changes.
Carterton Medical Centre have identified whanau groups and;
o Made targeted use of SIA funding, and
o Linked with the Whaiora e.g. to follow‐up on people/ whanau of concern.
Barriers Poor problem definition due to difficulties in gaining
agreement on what ‘whanau ora’ is and therefore project goals.
Improvement areas Follow‐up on the family violence initiative. Assess
effectiveness and areas for further developed e.g. screening within primary care.
Wider Whanau Ora collective has developed a plan of action now with Te Puni Kokiri for sign off. Opportunity for Tihei to work more closely with the collective on
Target Progress assessment and
result measures
Comments
Includes summary of progress, barriers and improvement areas
shared initiatives.
Identify focussed initiatives for action through Tihei e.g. Ministry of Health’s youth strategy, approach to long term conditions.
Progress review of whanau ora funding allocations alongside key initiatives.
Implement whanau ora primary education package being developed by Compass.
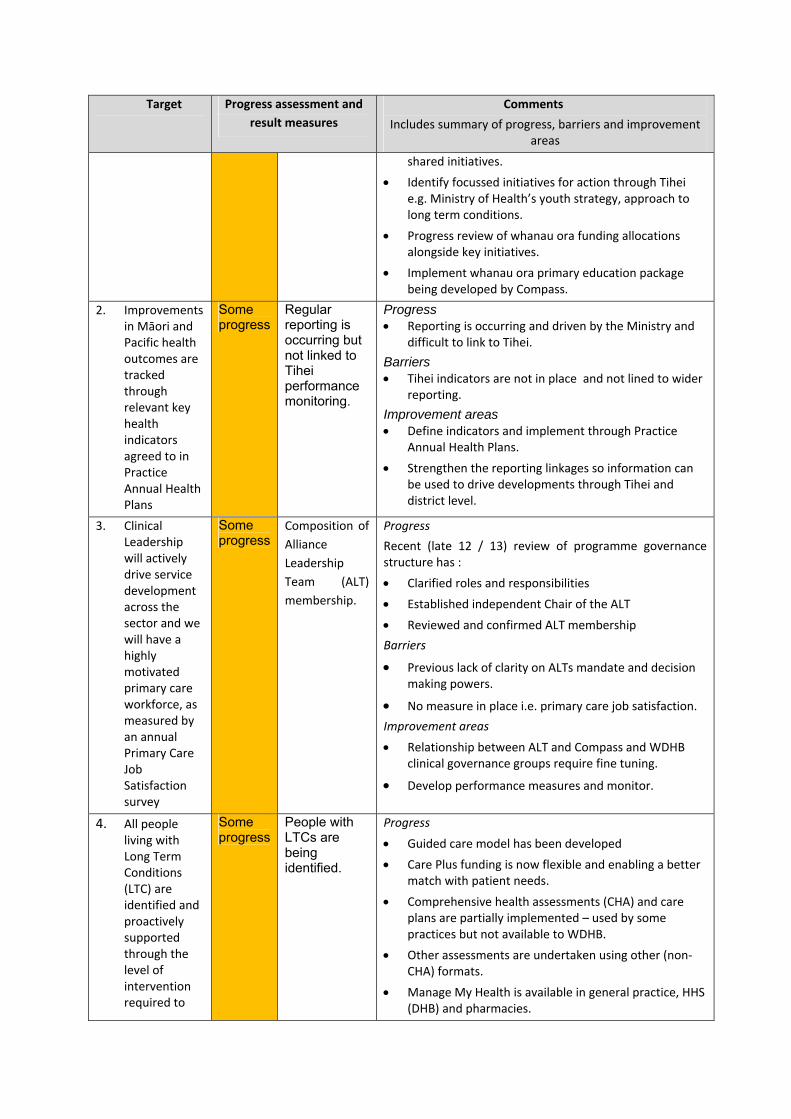
2. Improvements in Māori and Pacific health outcomes are tracked through relevant key health indicators agreed to in Practice Annual Health Plans
Some progress
Regular reporting is occurring but not linked to Tihei performance monitoring.
Progress Reporting is occurring and driven by the Ministry and
difficult to link to Tihei.
Barriers Tihei indicators are not in place and not lined to wider
reporting.
Improvement areas Define indicators and implement through Practice
Annual Health Plans.
Strengthen the reporting linkages so information can be used to drive developments through Tihei and district level.
3. Clinical Leadership will actively drive service development across the sector and we will have a highly motivated primary care workforce, as measured by an annual Primary Care Job Satisfaction survey
Some progress
Composition of
Alliance
Leadership
Team (ALT)
membership.
Progress
Recent (late 12 / 13) review of programme governance structure has :
Clarified roles and responsibilities
Established independent Chair of the ALT
Reviewed and confirmed ALT membership
Barriers
Previous lack of clarity on ALTs mandate and decision making powers.
No measure in place i.e. primary care job satisfaction.
Improvement areas
Relationship between ALT and Compass and WDHB clinical governance groups require fine tuning.
Develop performance measures and monitor.
4. All people living with Long Term Conditions (LTC) are identified and proactively supported through the level of intervention required to
Some progress
People with LTCs are being identified.
Progress
Guided care model has been developed
Care Plus funding is now flexible and enabling a better match with patient needs.
Comprehensive health assessments (CHA) and care plans are partially implemented – used by some practices but not available to WDHB.
Other assessments are undertaken using other (non‐CHA) formats.
Manage My Health is available in general practice, HHS (DHB) and pharmacies.
Target Progress assessment and
result measures
Comments
Includes summary of progress, barriers and improvement areas
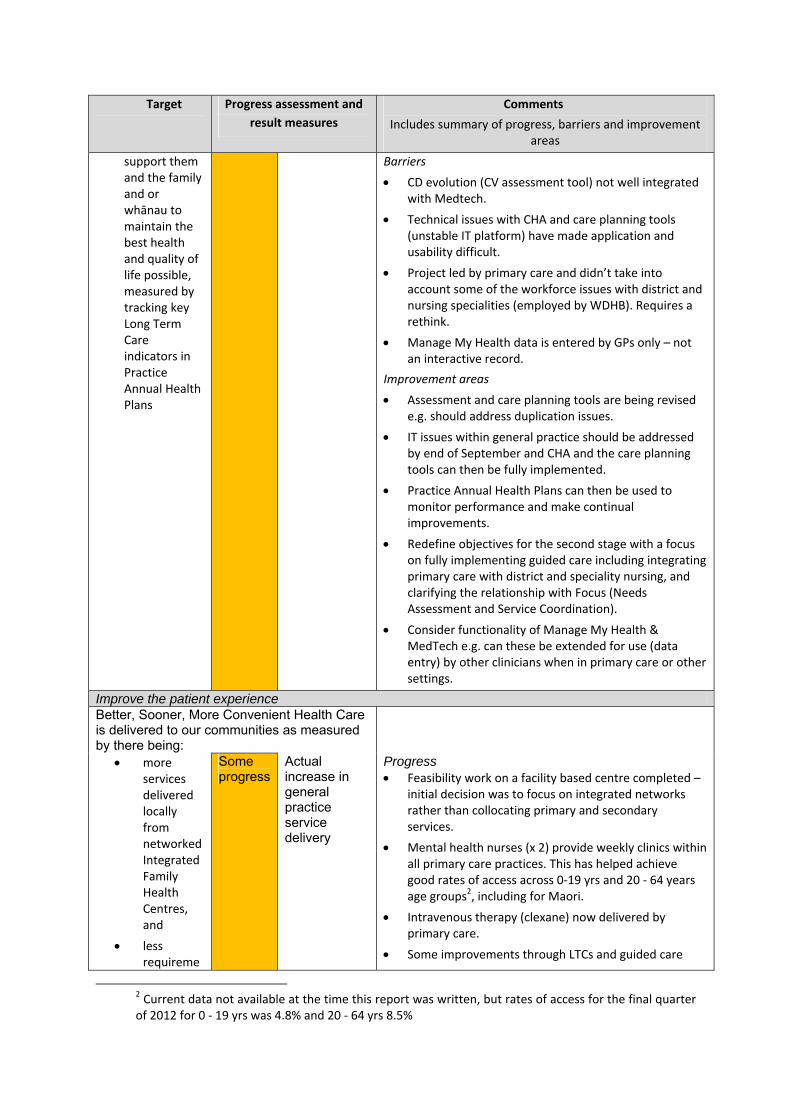
support them and the family and or whānau to maintain the best health and quality of life possible, measured by tracking key Long Term Care indicators in Practice Annual Health Plans
Barriers
CD evolution (CV assessment tool) not well integrated with Medtech.
Technical issues with CHA and care planning tools (unstable IT platform) have made application and usability difficult.
Project led by primary care and didn’t take into account some of the workforce issues with district and nursing specialities (employed by WDHB). Requires a rethink.
Manage My Health data is entered by GPs only – not an interactive record.
Improvement areas
Assessment and care planning tools are being revised e.g. should address duplication issues.
IT issues within general practice should be addressed by end of September and CHA and the care planning tools can then be fully implemented.
Practice Annual Health Plans can then be used to monitor performance and make continual improvements.
Redefine objectives for the second stage with a focus on fully implementing guided care including integrating primary care with district and speciality nursing, and clarifying the relationship with Focus (Needs Assessment and Service Coordination).
Consider functionality of Manage My Health & MedTech e.g. can these be extended for use (data entry) by other clinicians when in primary care or other settings.
Improve the patient experience Better, Sooner, More Convenient Health Care is delivered to our communities as measured by there being:
more services delivered locally from networked Integrated Family Health Centres, and
less requireme
Some progress
Actual increase in general practice service delivery
Progress Feasibility work on a facility based centre completed –
initial decision was to focus on integrated networks rather than collocating primary and secondary services.
Mental health nurses (x 2) provide weekly clinics within all primary care practices. This has helped achieve good rates of access across 0‐19 yrs and 20 ‐ 64 years age groups2, including for Maori.
Intravenous therapy (clexane) now delivered by primary care.
Some improvements through LTCs and guided care
2 Current data not available at the time this report was written, but rates of access for the final quarter of 2012 for 0 ‐ 19 yrs was 4.8% and 20 ‐ 64 yrs 8.5%
Target Progress assessment and
result measures
Comments
Includes summary of progress, barriers and improvement areas
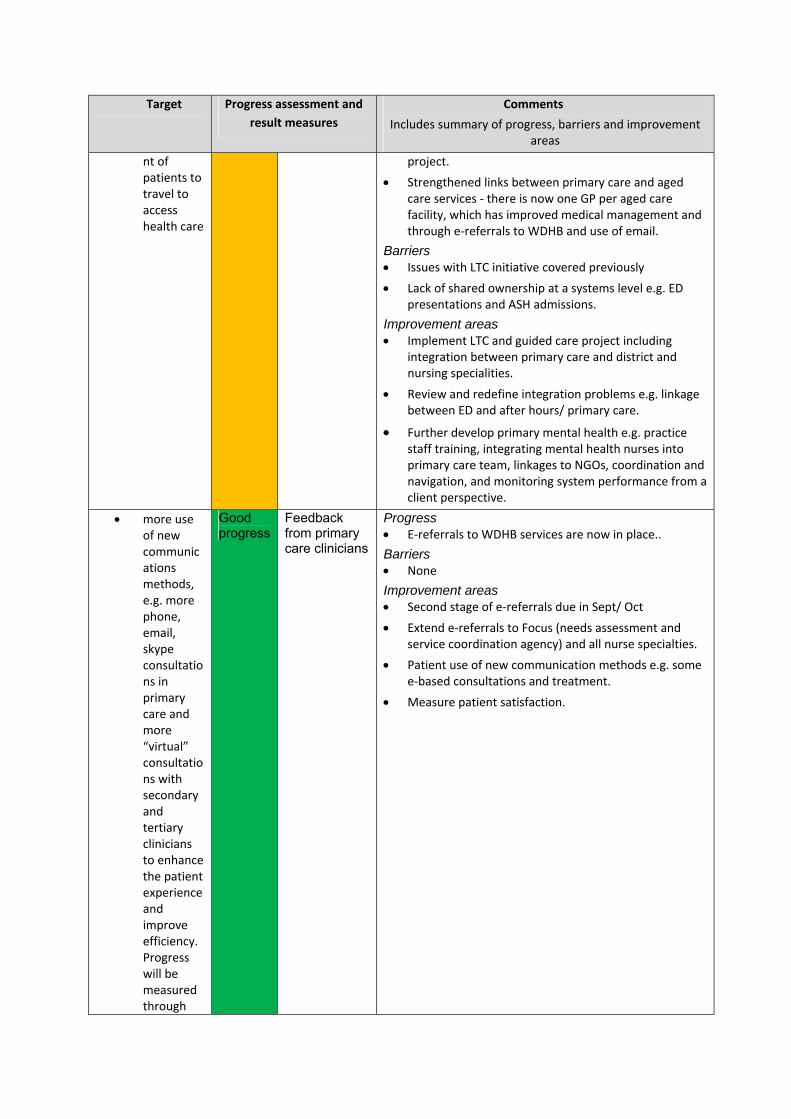
nt of patients to travel to access health care
project.
Strengthened links between primary care and aged care services ‐ there is now one GP per aged care facility, which has improved medical management and through e‐referrals to WDHB and use of email.
Barriers Issues with LTC initiative covered previously
Lack of shared ownership at a systems level e.g. ED presentations and ASH admissions.
Improvement areas Implement LTC and guided care project including
integration between primary care and district and nursing specialities.
Review and redefine integration problems e.g. linkage between ED and after hours/ primary care.
Further develop primary mental health e.g. practice staff training, integrating mental health nurses into primary care team, linkages to NGOs, coordination and navigation, and monitoring system performance from a client perspective.
more use of new communications methods, e.g. more phone, email, skype consultations in primary care and more “virtual” consultations with secondary and tertiary clinicians to enhance the patient experience and improve efficiency. Progress will be measured through
Good progress
Feedback from primary care clinicians
Progress E‐referrals to WDHB services are now in place..
Barriers None
Improvement areas Second stage of e‐referrals due in Sept/ Oct
Extend e‐referrals to Focus (needs assessment and service coordination agency) and all nurse specialties.
Patient use of new communication methods e.g. some e‐based consultations and treatment.
Measure patient satisfaction.
Target Progress assessment and
result measures
Comments
Includes summary of progress, barriers and improvement areas
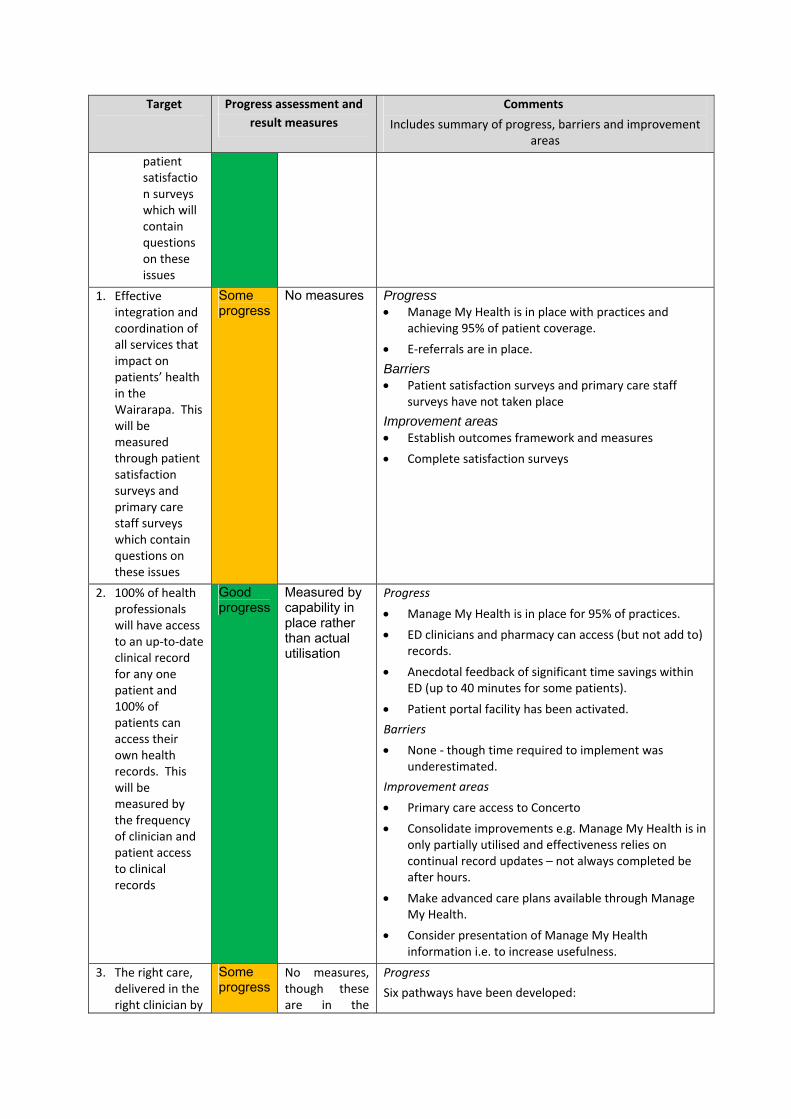
patient satisfaction surveys which will contain questions on these issues
1. Effective integration and coordination of all services that impact on patients’ health in the Wairarapa. This will be measured through patient satisfaction surveys and primary care staff surveys which contain questions on these issues
Some progress
No measures Progress Manage My Health is in place with practices and
achieving 95% of patient coverage.
E‐referrals are in place.
Barriers Patient satisfaction surveys and primary care staff
surveys have not taken place
Improvement areas Establish outcomes framework and measures
Complete satisfaction surveys
2. 100% of health professionals will have access to an up‐to‐date clinical record for any one patient and 100% of patients can access their own health records. This will be measured by the frequency of clinician and patient access to clinical records
Good progress
Measured by capability in place rather than actual utilisation
Progress
Manage My Health is in place for 95% of practices.
ED clinicians and pharmacy can access (but not add to) records.
Anecdotal feedback of significant time savings within ED (up to 40 minutes for some patients).
Patient portal facility has been activated.
Barriers
None ‐ though time required to implement was underestimated.
Improvement areas
Primary care access to Concerto
Consolidate improvements e.g. Manage My Health is in only partially utilised and effectiveness relies on continual record updates – not always completed be after hours.
Make advanced care plans available through Manage My Health.
Consider presentation of Manage My Health information i.e. to increase usefulness.
3. The right care, delivered in the right clinician by
Some progress
No measures, though these are in the
Progress
Six pathways have been developed:
Target Progress assessment and
result measures
Comments
Includes summary of progress, barriers and improvement areas
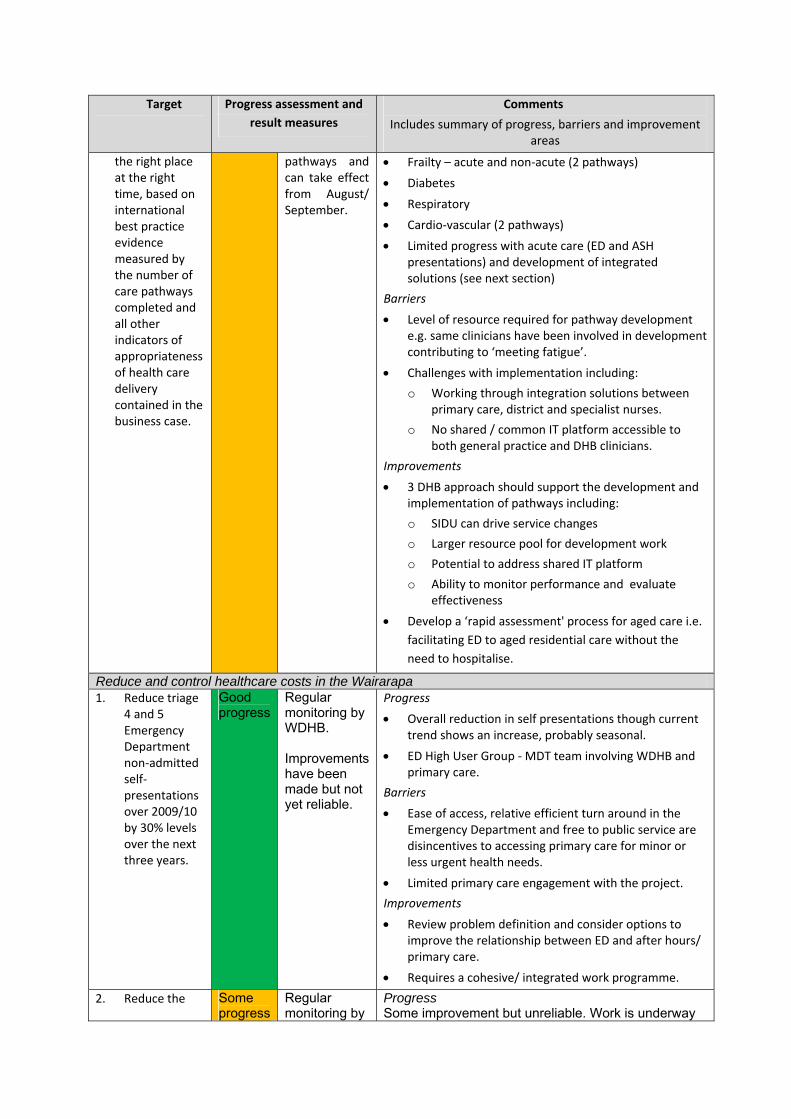
the right place at the right time, based on international best practice evidence measured by the number of care pathways completed and all other indicators of appropriateness of health care delivery contained in the business case.
pathways and can take effect from August/ September.
Frailty – acute and non‐acute (2 pathways)
Diabetes
Respiratory
Cardio‐vascular (2 pathways)
Limited progress with acute care (ED and ASH presentations) and development of integrated solutions (see next section)
Barriers
Level of resource required for pathway development e.g. same clinicians have been involved in development contributing to ‘meeting fatigue’.
Challenges with implementation including:
o Working through integration solutions between primary care, district and specialist nurses.
o No shared / common IT platform accessible to both general practice and DHB clinicians.
Improvements
3 DHB approach should support the development and implementation of pathways including:
o SIDU can drive service changes
o Larger resource pool for development work
o Potential to address shared IT platform
o Ability to monitor performance and evaluate effectiveness
Develop a ‘rapid assessment' process for aged care i.e.
facilitating ED to aged residential care without the
need to hospitalise.
Reduce and control healthcare costs in the Wairarapa1. Reduce triage
4 and 5 Emergency Department non‐admitted self‐presentations over 2009/10 by 30% levels over the next three years.
Good progress
Regular monitoring by WDHB. Improvements have been made but not yet reliable.
Progress
Overall reduction in self presentations though current trend shows an increase, probably seasonal.
ED High User Group ‐ MDT team involving WDHB and primary care.
Barriers
Ease of access, relative efficient turn around in the Emergency Department and free to public service are disincentives to accessing primary care for minor or less urgent health needs.
Limited primary care engagement with the project.
Improvements
Review problem definition and consider options to improve the relationship between ED and after hours/ primary care.
Requires a cohesive/ integrated work programme.
2. Reduce the Some progress
Regular monitoring by
Progress Some improvement but unreliable. Work is underway
Target Progress assessment and
result measures
Comments
Includes summary of progress, barriers and improvement areas
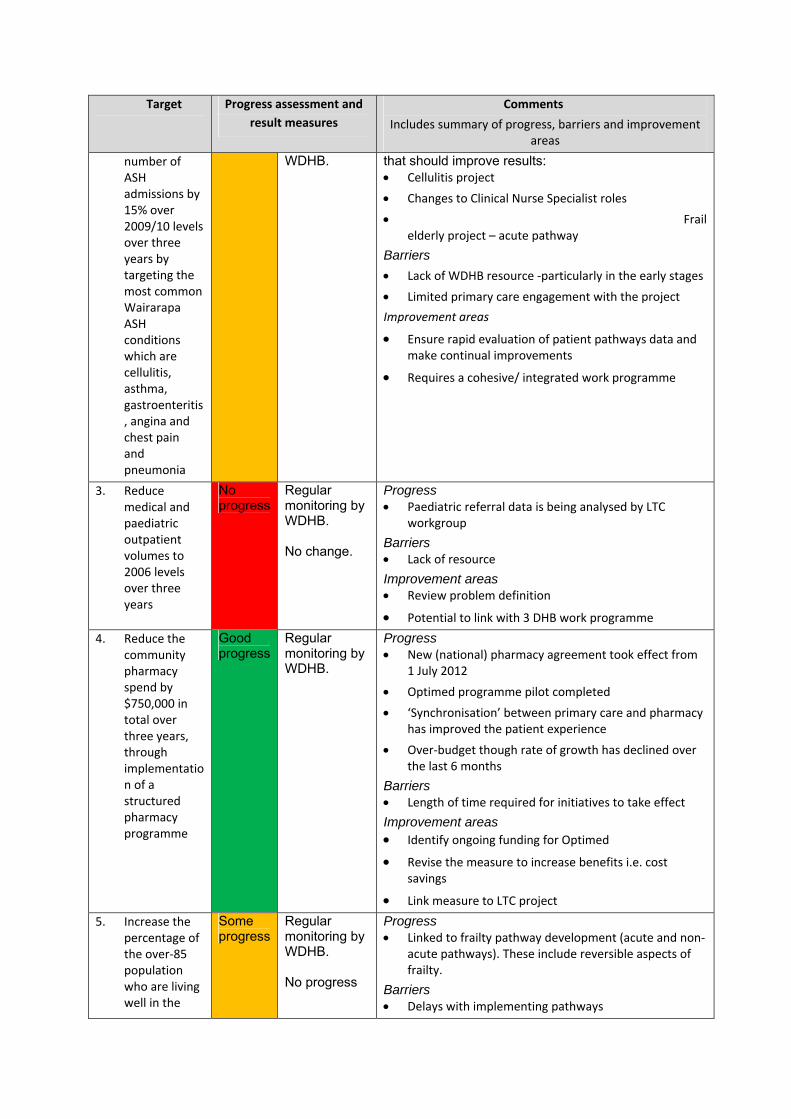
number of ASH admissions by 15% over 2009/10 levels over three years by targeting the most common Wairarapa ASH conditions which are cellulitis, asthma, gastroenteritis, angina and chest pain and pneumonia
WDHB.
that should improve results: Cellulitis project
Changes to Clinical Nurse Specialist roles
Frail elderly project – acute pathway
Barriers
Lack of WDHB resource ‐particularly in the early stages
Limited primary care engagement with the project
Improvement areas
Ensure rapid evaluation of patient pathways data and make continual improvements
Requires a cohesive/ integrated work programme
3. Reduce medical and paediatric outpatient volumes to 2006 levels over three years
No progress
Regular monitoring by WDHB. No change.
Progress Paediatric referral data is being analysed by LTC
workgroup
Barriers Lack of resource
Improvement areas Review problem definition
Potential to link with 3 DHB work programme
4. Reduce the community pharmacy spend by $750,000 in total over three years, through implementation of a structured pharmacy programme
Good progress
Regular monitoring by WDHB.
Progress New (national) pharmacy agreement took effect from
1 July 2012
Optimed programme pilot completed
‘Synchronisation’ between primary care and pharmacy has improved the patient experience
Over‐budget though rate of growth has declined over the last 6 months
Barriers Length of time required for initiatives to take effect
Improvement areas Identify ongoing funding for Optimed
Revise the measure to increase benefits i.e. cost savings
Link measure to LTC project
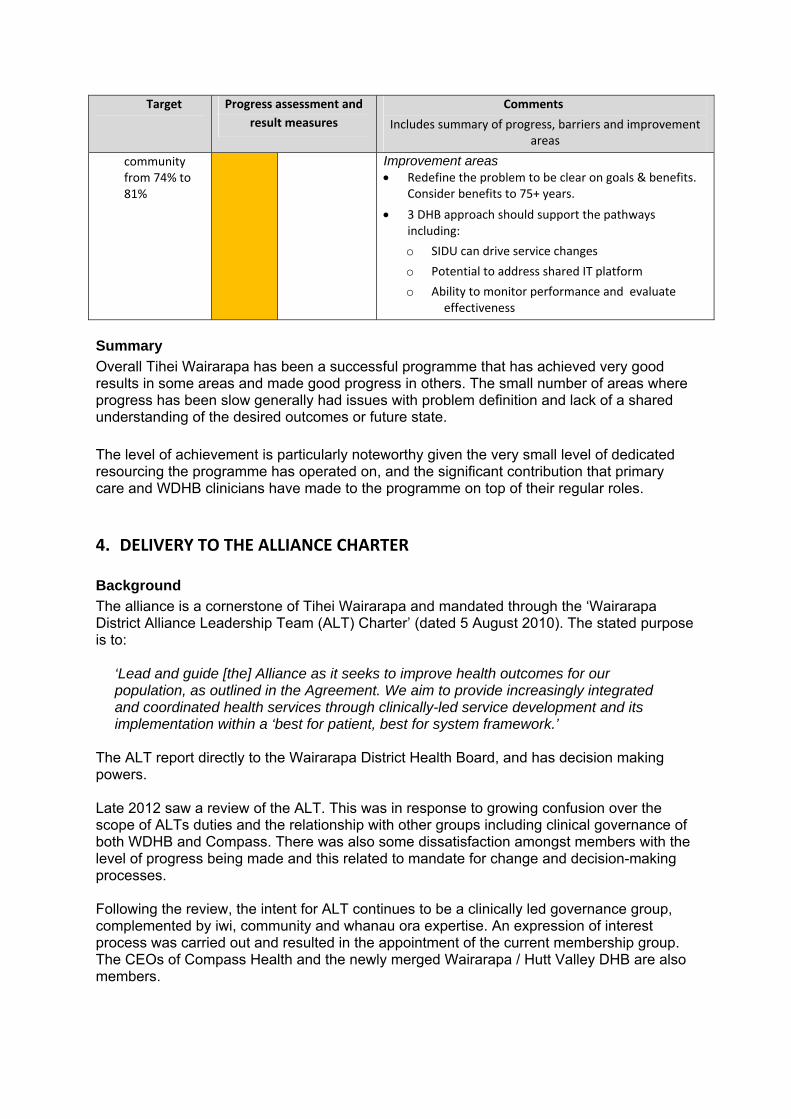
5. Increase the percentage of the over‐85 population who are living well in the
Some progress
Regular monitoring by WDHB. No progress
Progress Linked to frailty pathway development (acute and non‐
acute pathways). These include reversible aspects of frailty.
Barriers Delays with implementing pathways
Target Progress assessment and
result measures
Comments
Includes summary of progress, barriers and improvement areas
community from 74% to 81%
Improvement areas Redefine the problem to be clear on goals & benefits.
Consider benefits to 75+ years.
3 DHB approach should support the pathways including:
o SIDU can drive service changes
o Potential to address shared IT platform
o Ability to monitor performance and evaluate effectiveness
Summary
Overall Tihei Wairarapa has been a successful programme that has achieved very good results in some areas and made good progress in others. The small number of areas where progress has been slow generally had issues with problem definition and lack of a shared understanding of the desired outcomes or future state.
The level of achievement is particularly noteworthy given the very small level of dedicated resourcing the programme has operated on, and the significant contribution that primary care and WDHB clinicians have made to the programme on top of their regular roles.
4. DELIVERY TO THE ALLIANCE CHARTER Background
The alliance is a cornerstone of Tihei Wairarapa and mandated through the ‘Wairarapa District Alliance Leadership Team (ALT) Charter’ (dated 5 August 2010). The stated purpose is to:
‘Lead and guide [the] Alliance as it seeks to improve health outcomes for our population, as outlined in the Agreement. We aim to provide increasingly integrated and coordinated health services through clinically-led service development and its implementation within a ‘best for patient, best for system framework.’
The ALT report directly to the Wairarapa District Health Board, and has decision making powers. Late 2012 saw a review of the ALT. This was in response to growing confusion over the scope of ALTs duties and the relationship with other groups including clinical governance of both WDHB and Compass. There was also some dissatisfaction amongst members with the level of progress being made and this related to mandate for change and decision-making processes. Following the review, the intent for ALT continues to be a clinically led governance group, complemented by iwi, community and whanau ora expertise. An expression of interest process was carried out and resulted in the appointment of the current membership group. The CEOs of Compass Health and the newly merged Wairarapa / Hutt Valley DHB are also members.
The purpose of the ALT has been confirmed as the group responsible for strategy, leadership and direction across the integrated health system. Feedback
There is general agreement that one of Tihei’s most successful elements is the role it has played in further developing relationships and collaboration across the district, including through ALT and the various project teams and flowing through to front line staff. This has increased understanding of the roles and pressures facing primary and secondary care services, and a shared understanding of some (but not all) problems. However there is also agreement that the potential benefits of collaboration are a long way from being realised – ‘the integration question hasn’t been answered yet’ – so much of the value of the gains made to date is that they lay the building blocks for further collaboration and change. Previous ALT members questioned how the group has operated in the past, saying that that it could be difficult to ‘follow the thread’ of the various projects and engage in discussion, or that the same discussions were had multiple times. This could be problematic for maintaining a sense of progress and for decision making – with some members saying that ALT made very few decisions and that these were generally made outside the group by managers. These problems appear to relate to the volume of work (arguably too many workstreams underway at a time) and the programme methodology, and therefore inconsistencies in how the workstreams were managed - for example progress monitoring and reporting has generally been by activity and not always linked to key milestones or decision points. There is still considerable confusion on the relationship between ALT and clinical governance (and to a lesser degree management), and this is recognised as an area for further work and clarification. Both WDHB and Compass have clinical governance boards, and generally this is considered appropriate – i.e. these boards have a wider organisational function with Tihei being just one component of this. The outstanding issue is how the ALT and the clinical governance groups link together, with options being that the GP liaison role is a member of all groups, and the programme director attends the clinical governance groups on a regular or as required basis. The GP liaison person and programme director would then be jointly responsible for making the links and reporting to ALT. Other comments on ALT going forward are:
Concern with the composition of the membership. While the presence of the two CEOs is
valued, there is some concern that this is at the expense of DHB operational managers who
may be able to quickly ‘fix things’ and progress initiatives.
Loss of original drive for change. While it’s inevitable that changes in the original
membership group have occurred overtime, the original passion for integration needs to be
fostered and continue.
5. LESSONS LEARNT OVER THE LAST THREE YEARS The feedback received through the interviews falls into the key themes outlined below. Better, Sooner, More Convenient (BSMC) Tihei Wairarapa originated from the Ministry of Health’s BSMC initiative, which aimed to drive the development of primary and locally driven services. The business case was completed in very tight timeframes and some of the issues that, in hindsight, this created were:
Insufficient analysis of population needs ‐ particularly youth, and the impacts of low
incomes on health needs, and utilisation patterns of primary care practices
A message that Tihei was mainly about primary care and that secondary services were less
important to the initiative (this may have impacted on the buy‐in of some WDHB clinicians)
Failure to consider the wider determinants of health and wellbeing, and relationships with
social services
Some of the aspirational targets were ‘locked in’ to the Ministry of Health’s reporting
requirements, and this limited the ability to review parts of the original case for change as
might otherwise have been appropriate
Scope of change and buy-in Generally there is agreement that the original set of initiatives and aspirational targets was too broad to be successfully implemented in a 3 year timeframe, particularly given the lack of dedicated resources available to support implementation, and the level of change experienced by WDHB over recent months. There is also a view that Tihei lacked a ‘burning platform for change’ shared by both primary care and WDHB staff and therefore agreement on some the initiatives (problem definition, options for change etc) was weak - the acute (ED and ASH) project is an example of this. However, there is also agreement that Tihei created very positive energy and that one of the advantages of not limiting the initial work programme was that it enabled many people to get involved, leading to positive relationship development. While this benefit may be difficult to quantify everyone recognises this as an essential platform to the next steps for Tihei and integration. Integrated Family Health Centre A feasibility study that explored the option of shifting Masterton Medical Centre into WDHB premises was undertaken. At the time there were several barriers that impeded progress on the option including that the Ministry of Health’s policy and willingness to provide financial support for transitional costs was unclear, and that the local vision for integration was still forming so there was some resistance across the sector. The idea hasn’t gone away and there is merit in further exploring options for an Integrated Family Health Centre. Practice Annual Health Plans One of Tihei’s tools for driving change was the introduction of Practice Annual Health Plans. These would be the tool for monitoring performance and outcomes across primary care and thereby assist practices by putting all (Tihei and other) requirements into one place, with the information then available to inform further improvements. While three3 practices now have plans in place the overall the purpose of the plans is questioned, with some viewing these as ‘yet another’ compliance requirement and perhaps not appropriate in a high trust environment. The problem lies with how the plans were implemented. The resource to pull all of the requirements into one place and into a user friendly format weren’t available within Compass or the primary care practices. The implementation of guided care and the pathways is an opportunity to review the purpose of the plans, and to reintroduce them in a more streamlined fashion. Programme management and resources
3 Martinborough, Featherston and Greytown
During the initial stages key WDHB and primary care managers were tasked as project leaders, and most formed project teams. The resource pool mainly consisted of ‘in kind’ contributions with staff in paid positions undertaking work in addition to their regular roles. GPs were paid a set fee for after hours work, and this did not fully compensate for the time and costs involved. In May 2012, the need to put more structure into the programme was recognised and a fulltime programme director was appointed, and she reported jointly to the CEOs of Compass Health and WDHB. This resulted in an improvement in the programme’s organisation and performance but not necessarily results – the work plan was largely established and there was a need to resolve the issues related to ALT and programme governance. The environment also destabilised late 2012 when the CEOs of Compass Health and WDHB both left their positions, and WDHB began a period of change from November 2012. The initial programme director has since resigned and the appointment of a replacement director is in progress. There is full agreement that that the role should continue and is considered critical to the success of the programme over the next two years. Additional resources may be required to support change and developments at various stages of the programme. Change resistance One of the challenges with a programme like Tihei is that those involved in driving and implementing change can also have an interest in maintaining the status quo for a variety of reasons such as protecting work conditions or building ownership. These needs must be balanced against those of patients - the system needs to work for everyone. There is a view that at times staff and provider interests have limited discussion and the options being considered. Ways of opening up discussion to ensure all options are explored should be considered.
6. WHAT COULD HELP MAKE PROGRESS OVER THE NEXT TWO YEARS The following list of suggestions was gathered though interviews. It is not an exhaustive list and is intended as discussion points for the ALT. Overall programme 1) Focus on a small number of prioritised and agreed initiatives at any one time. Focus on
initiatives that drive whole of system change. Ensure there is a common understanding of the
problem/s to be solved and that the change options and preferred solutions are agreed to by all
parties.
2) Formalise the programme structure (project planning and reporting, benefits and evaluation).
This could be done alongside the Service Integration and Development Unit (SIDU) operating
across the DHBs. This would ensure consistency in programme methodology and enable the
linkages to be made at a wider systems level.
Potential work plan 3) Information management – develop and an overarching plan that:
Builds on what’s in place to extend functionality including:
o Information presentation and ease of access
o Non‐primary care users recording information into MedTech (particularly specialist
nurses) and interacting through Manage My Health
o Interactivity – real time
o Patient usage
Considers and makes a decision on an integrated IT tool for long term conditions
Consolidate to ensure information is up‐to‐date and everyone is using the tools
appropriately
4) Guided care ‐ further develop the model for older people and people with long term conditions,
with a focus on integration between the functions of primary care and district and specialist
nursing, and the relationship with Focus (needs assessment and service coordination).
5) Integrated Family Health Centre ‐ reconsider options for collocating primary care with WDHB
services in Masterton.
6) Primary mental health ‐ further develop the model and consider practice staff training,
integrating mental health clinicians into primary care teams, integrating with NGOs,
coordination and navigation, and monitoring system performance from a patient perspective.
7) Whanau ora ‐ review the approach to align with the wider Whanau Ora collective, and to
identify and progress targeted Tihei initiatives e.g. youth or people with long term conditions
within a whanau context.
8) Workforce ‐ this was one of the original business case objectives not progressed for resource
reasons, but still considered an important area for work. Options to consider include:
Sector‐wide recruitment and retention
Resource sharing ‐ options to work across primary and secondary care
Capability development aligned to Tihei goals e.g. whanau ora, primary mental health
Change management 9) Approach to change ‐ take a dynamic approach including:
Start with a blank piece of paper for some initiatives/ options e.g.
o Information management options
o Relationship between WDHB acute services and primary care after hours
Use a proven change methodology such as PDSA (Plan, Do, Study Act) as recommended by
the Institute for Health Improvement (IHI). The methodology works on 90 day cycles and
objectives would be:
o To re‐establish project teams (as necessary)
o To provide needs analysis data to inform the development of a programme of action
o Implement actions from the initial strategy set, and include gathering data on the
impact of the actions and adapting strategies on an ongoing basis.
10) Communication ‐ keep everyone informed and energised through regular updates and
engagement meetings, and by celebrating achievements.
11) Work smart ‐ while solutions need to work for the Wairarapa some development work can take
place at a sub‐regional level e.g. pathways and programme management tools.
12) Annual practice health plans ‐ review the purpose of the plans and implement these with a view
to ensuring they are a tool for driving change and making continual improvements, and
simplifying reporting requirements.





























