Embed Size (px)
Citation preview

Thyroid Storm in the Setting of Subacute Thyroiditis
PGY-2 Case Conference
Jordan Groubert, PGY-2
11/5/2019
1

1. Review Case
2. Discuss Disease Pathogenesis
3. Discuss Differential Diagnosis
4. Discuss Diagnostic Criteria
5. Discuss Treatment
6. Patient Update
Outline
2

History of Present Illness
3

History of Present Illness
• 19 y/o female presented with a 2-3 day history of generalized pain, confusion, nausea, emesis and right upper extremity swelling. On presentation she was encephalopathic, intermittently crying out in pain and only able to answer some yes/no questions. The majority of the history was provided by the patient’s father.
4

Medical History
5

Past Medical History
• IV drug abuse
o Last admitted drug use was 6 months prior, but family was suspicious for active use
o “Pink powder” found at home by her father
• MRSA abscesses
• No prior history of thyroid disorders
6

Past Surgical History
• No prior surgical history
7

Family History
• No pertinent family history
o No known family history of thyroid disorders
8

Social history
• Current 1 ppd smoker, 5 pack-year history
• Denied alcohol use
• IV heroin/fentanyl use
• Lives at home with her father
9

Review of Systems
10

Review of Systems
• ROS positive for
o Generalized pain
o Nausea
o Emesis
o Right upper extremity swelling
• Reliable ROS unable to be obtained upon admission due to encephalopathy
11

Physical Exam
12

Physical exam
• Vitals: Temp 99.3 F, HR 143, RR 40, SpO2 97% RA, BP 93/57 (68)
• General: Ill-appearing, moderate distress, diaphoretic
• HEENT: NCAT, PERRL, EOMI, Poor dentition. No exophthalmos/ophthalmopathy.
• Neck: Diffusely enlarged thyroid with tenderness to palpation, no bruit.
• CV: Tachycardia, regular rhythm, no murmurs
• Thorax: Tachypnea, bilateral crackles, labored respirations
• Abdomen: Bowel sounds present, generalized tenderness, non-distended, no organomegaly, no rashes
• Extremities: Track marks on bilateral upper/lower extremities, no peripheral edema, no pretibial myxedema
• Neuro: Moves all extremities, sensation grossly intact, no focal deficits
• Integument: Track marks
• Psych: anxious and agitated, intermittently crying out in pain, AOx1
13

Labs and Imaging
14

Labs
134
3.6
96 32
0.77162
22
12.5
36.4
23.3 83
Troponin: 1.530
TSH: 0.026
Free T3: 16.9
Free T4: > 6.99
Lactic Acid: 3.7
UDS: negative
15

Imaging
16
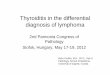
• CT Neck Soft Tissue• Generalized edema throughout the soft tissues of the neck with prominent swelling and edema involving
the thyroid gland. Findings concerning for thyroiditis.
• Thyroid US• Large and heterogenous gland with no normal thyroid tissue appreciated. No focal nodules noted. No
evidence of increased vascularity on color doppler.

Thyroid US
Summa Health Sample Preso17

Hospital Course
• Admitted to the ICU for management of thyrotoxicosis and started on empiric antibiotics for sepsis
o Blood cultures positive for MRSA; TTE showed tricuspid valve endocarditis
• Endocrinology was consulted and started:
o Methimazole
o Propranolol
o Hydrocortisone
o Cholestyramine
• Patient endorsed anterior neck pain, palpitations, diaphoresis and heat intolerance for 2-3 days before presentation
• Thyroid receptor antibody (TRAb) was negative, ruling out Grave’s disease
o Methimazole was stopped
• TPO antibody was negative, ruling out Hashimoto’s thyroiditis
• Repeat thyroid ultrasound continued to show evidence of thyroiditis
o Thyroiditis attributed to septicemia/endocarditis/systemic inflammation
• Patient’s condition gradually improved and steroids were tapered
18 11.05.19

Thyroid Storm
19

Thyroid Storm
• Thyroid storm is a rare, life-threatening manifestation of thyrotoxicosis
o 20-30% mortality rate
o Affecting only 1% of thyrotoxic patients
• Most common in patient’s with an underlying hyperthyroid state (Grave’s Disease, toxic multinodular goiter or solitary toxic adenoma) who have an inciting event
o Thyroid or non-thyroidal surgery
o Infection
o Trauma
o Acute iodine load
o Childbirth
o Irregular use or discontinuation of anti-thyroid drugs (ex. methimazole, propylthiouracil)
• Very few documented cases of thyroid storm in the setting of subacute thyroiditis
20

Presentation
• Patients present with severe signs/symptoms of thyrotoxicosis
o Hyperpyrexia
o Tachycardia
o Heart failure
o Hypotension
o Diarrhea
o Confusion/delirium
o Anxiety/agitation
• Physical exam
o Goiter may or may not be present
• Labs
o Suppressed TSH, elevated Free T3/T4
o Degree of Free T3/T4 elevation doesn’t necessarily correlate with severity of symptoms
Summa Health Sample Preso21 06.06.2016

Pathogenesis
• Excess release of circulating thyroid hormones
• Mechanism of hormone release differs depending on underlying hyperthyroid condition
o Ex. Graves Disease, subacute thyroiditis, toxic multinodular goiter etc.
22

Differential Diagnosis
• Drug intoxication
• Hypertensive emergency/hypertensive encephalopathy
• Infection/sepsis
• Neuroleptic malignant syndrome
• Pheochromocytoma
• Psychosis
Summa Health Sample Preso23 06.06.2016

24
• Diagnosis is based on signs/symptoms of thyroid storm in individuals with suppressed TSH and elevated Free T3/T4
• The Burch-Wartofsky score is used to aid in the diagnosis
• Scoring system:• < 25: thyroid storm unlikely• 25-44: impending thyroid storm• > 45: highly suggestive of thyroid storm
• In this case, the Burch-Wartofsky score was 75
Diagnosis

Workup
• Labs
o TSH, Free T3, Free T4
o TSI or TRAb
• Imaging
o Thyroid ultrasound
o CT neck soft tissue
o Radioiodine uptake and scan
25

Treatment
• Patients require management in the ICU
• Management includes:
o Beta-blockers
• Management of signs/symptoms related to increased adrenergic tone
o Thionamides (methimazole or propylthiouracil)
• Decrease synthesis and peripheral conversion of thyroid hormones
o Glucocorticoids
• Reduce peripheral conversion of T4 to T3 conversion
• Promote vasomotor stability
• Reduce inflammation (if present)
o Bile acid sequestrants
• Decrease enterohepatic recycling of thyroid hormones
o Iodine (iodinated contrast or iodine tablets)
• To be given after administration of anti-thyroid medications to prevent worsening of thyrotoxicosis
• Decrease release of T3 and T4 from the thyroid
26

Subacute Thyroiditis
• Inflammation of the thyroid usually in the setting of viral illness or a post-viral inflammatory process
• Pathogenesis: destruction of thyroid follicles and proteolysis of thyroglobulin causing release of T3 and T4
• Presentation
o Anterior neck pain
o Diffuse goiter with tenderness to palpation
o Signs/symptoms of hyperthyroidism/thyrotoxicosis with associated laboratory abnormalities
• Thyrotoxicosis is usually mild
• Severity of signs/symptoms don’t necessarily correlate with degree of lab abnormalities
• Imaging
o Ultrasound: hypoechoic appearance, may be normal or enlarged
o Radioiodine uptake and scan: low uptake in the hyperthyroid phase
• Treatment:
o Pain control and beta blockers
o Thionamides are not indicated
• Clinical course
o Hyperthyroid Euthyroid Hypothyroid Recovery
Summa Health Sample Preso27

Patient update
• Discharged to acute rehab following complicated ICU course
• No outpatient follow-up to date
28

Acknowledgements
• Ahmad Al-Shoha, MD
• Mansur Assaad, MD
• Bisher Zuhdi, MD
29

References
• Salih AM, Kakamad FH, Rawezh QS, et al. Subacute thyroiditis causing thyrotoxic crisis; a case report with literature review. Int J Surg Case Rep. 2017;33:112-114.
• Swinburne JL, Kreisman SH. A rare case of subacute thyroiditis causing thyroid storm. Thyroid. 2007;17(1):73-6.
• Fatourechi V, Aniszewski JP, Fatourechi GZ, Atkinson EJ, Jacobsen SJ. Clinical features and outcome of subacute thyroiditis in an incidence cohort: Olmsted County, Minnesota, study. J Clin Endocrinol Metab. 2003;88(5):2100-5.
• MKSAP
• Uptodate
30

Questions?
31

Thank you
32

Severe Cardio-Renal Syndrome
Responding to Very High Dose
Lasix DripDan Redle MD, Bisher Zhudi MD, Chris Tanayan MD, Charina Gayomali MD

Overview
Review Case
Pathophysiology
Differentials
Treatment
Patient Update
References

HPI
61 yo M presented to ACH ED 4/3/19 with acute on chronic SOB with cough,
bilateral leg pain, chills, arthralgias, nausea. In ED, vital signs initially
remarkable for increased work of breathing with RR of 22 and patient
required BiPAP.

Medical and Social History
PMH: CAD, HFrEF (25%), Afib,CKD, Apical Thrombus, COPD, T2DM, OSA, DVT,
HTN, HPL, Gout, Back Pain
PSH: CABG, Atrial Ablation, Embolectomy RLE
FMH: Father: Lung Cancer
Social: Single, known hoarder, denied tobacco/EtOH/illicit drug use

Physical Exam
Constitutional: He is oriented to person, place, and time.In moderate respiratory distress
HENT:
Head: Normocephalic and atraumatic. Right Ear: External ear normal. Left Ear: External ear normal.
Nose: Nose normal.
Mouth/Throat: Oropharynx is clear and moist.
Eyes: Pupils are equal, round, and reactive to light. Conjunctivae and EOM are normal.
Neck: Normal range of motion. No JVD present. No tracheal deviation present.
Cardiovascular: Normal rate, Irregularly Irregular Rate, normal heart sounds and intact distal pulses.
Pulmonary/Chest: He is in respiratory distress. He has wheezes.
Abdominal: Soft. Bowel sounds are normal. He exhibits no distension. There is tenderness (mild generalized). There is no rebound. Musculoskeletal: Normal range of motion. He exhibits no tenderness. Positive lower extremity edemaNeurological: He is alert and oriented to person, place, and time.
Skin: Skin is warm and dry. No erythema.
Nursing note and vitals reviewed.

Vitals/Labs
Vitals: T 97.5, HR 82, RR 24, O2 95
Lactic Acid: 1.7
4/3/2019 19:58
Hemoglobin, Art, Extended: 10.0
pH, Arterial: 7.205 (L)
pCO2, Arterial: 52.9 (H)
pO2, Arterial: 471.3 (H)
HCO3, Arterial: 20.4 (L)
TCO2 (calc), Art: 22.1 (L)
Base Excess, Arterial: -7.4 (L)
O2 Sat, Arterial: 99.7
FIO2 Arterial: 100%

Hospital Course
• Admitted 4/3/19-5/1/19
• AHRF 2/2 Influenza, CXR congested -> ICU, BiPAP, BiPaP -> Resp status worsened/CXR
worsened then intubated, Increased diuretic dosages/frequency. Initial wt 281 lbs.
• Diuresis fairly well at first with boluses, then UOP dropped, CXR still well -> Lasix gtt
10 mg/hr ->20 mg/hr-> UOP improved, net negative, CXR Improved, extubated to
NIV, -7.8 L net, On NC, Lasix boluses -> UOP worsening/Cr climbing, Na 160s,
required Free H2O-> Afib RVR overnight-> amio gtt -> resp status worse req BiPAP,
UOP dropped/net positive, CXR more wet, Cr climbing, still had edema -> Lasix gtt
10 mg/hr with bolus Lasix 120 mg, no response
• Consulted Nephrology-> UF vs High dose Lasix gtt? -> already net -8 L, JVD?,
Hypernatremic and less edema but CXR very wet -> 4/13/19 IV Lasix drip 100 mg/hr,
(CVP just before 24 mmHg), Consulted Cardiology
• Patient responded VERY WELL, Over the next 2 days net of -7 L UOP for a total. Able
to wean off Lasix drip and start Bumex 3 mg BID
• by April 18th Net -21 L, off BiPAP, to Floors, did not develop tinnitus, wt now 244 lbs.

Hospital Course
On Floor, patient continued to be net negative with wt decreasing.
4/19: Cr increased, 2.8->3.2, Bumex held
TTE: LVEF 23% with global dysfunction/RV severely dilated with moderate
dysfunction/2 + PVR/PASP 45 mmHG
Cr climbed and peaked at 3.59 4/21, diuretics held up till this time. Bumex 2 mg PO
BID started after.
Decision was made to hold off on LHC/RHC due to severe renal dysfunction
Not deemed a good candidate for dialysis by Nephrology
Palliative Care consulted, patient made a limited code
DC’d to SNF
Patient net – 23.5 L, wt 221 lbs (from 281 lbs)

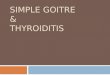
Creatinine, Weight, and Urine Output
Course
Initiation of increased
bolus diuresis, wt 281UOP dropped
4/7/19, started
Lasix Drip at
10/hr, still net
neg, total
Decision to start
Lasix at 100/hr
on 4/13 in
afternoon, CVP
24, started
making urine
4/13/19
morning CXR
wet, no UOP
Cr climbing,
Lasix at 10/hr
no response,
bolus of 120,
no response,
wt 257 lbs
4/12: night
Afib RVR
-7 L over next
two days, total
net negative -
13.8 L since
admission, wt
244
-23.5 L by end of
admission, wt 221
Patient either Euvolemic v.
Hypovolemic. Likely due
diuresis with lagging fluid
shifts. Bumetanide held for a
couple days
Bolus Lasix

Cardio-Renal Syndrome Pathophysiology
Complex interaction between Hemodynamics, RAAS, Sympathetic, HPA Axis, Vasopressin, and Inflammation
Cardiac output is reduced, resulting in venous systemic pressure elevation which is transmitted to the kidneys/other organs, which have impaired perfusion and are so damaged. Reduced cardiac output also reduces perfusion to organs
RASS, Vasopressin, HPA and local/systemic inflammation result, and continue in a downward spiral perpetuating volume overload and end organ damage
These patients have a narrow volume status, BP status and so diuretic window
Diuresis can is needed and may result in improvement, maintenance, or worsening of creatinine initially (but is still needed regardless)
These patients are often diuretic resistant

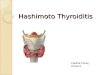
Diagnostic Criteria

Cardio-Renal Syndrome

Cardio-Renal Syndrome

Cardio-Renal Syndrome

Diuretic Resistance
RAAS Activation
Low Albumin/Protein
Nephron Remodeling
Decreased GFR

Differentials
Pure Heart Failure
Pure AKI
MI/Cardiogenic Shock
ARDS
Sepsis/Pneumonia
PE
HRS

Treatment/Management of Acute CRS
Loop Diuretics 1st line
Augment with Thiazides (metolazone, chlorthalidone, HCTZ)
Ultrafiltration (HD/CRRT) if patient cannot make urine after diuretic
challenge
Tolvaptan (when hyponatremic, infrequently used)
Vasodilators (i.e. isordil/hydralazine, nipride drip, avoid ACEi 2/2 AKI)
Inotropes (i.e. dobutamine, avoid milrinone 2/2 AKI)
Swan-Ganz (idk why we didn’t do this…)
CVP (at least we did this)
Echo

Patient Update
Patient appears to be doing OK per chart review
Has had several hospital admissions/ED visits since this past April for HF, gout
flare, and dehydration. He is living at home; family is bringing him to
appointments.
Is seeing Cardiology, Nephrology and Pulmonology

References
Ellison, D. and Felker, M. (2018). Diuretic Treatment in Heart Failure. New England Journal of Medicine, 378(7), pp.683-685.
Rangaswami J, Bhalla V, Blair J E.A., Chang T I., Costa S, Lentine K L., Lerma E V., Mezue K, MolitchM, Mullens W, Ronco C, Tang W Wilson, McCullough, P A. Cardiorenal Syndrome: Classification, Pathophysiology, Diagnosis, and Treatment Strategies: A Scientific Statement From the American Heart Association. Circulation. March 2019;139:840-878. https://www.ahajournals.org/doi/10.1161/CIR.0000000000000664.
Ronco C, Cicoira M, McCullough PA. Cardiorenal Syndrome Type 1 Pathophysiological Crosstalk Leading to Combined Heart and Kidney Dysfunction in the Setting of Acutely Decompensated Heart Failure. Journal of the American College of Cardiology. September 18, 2012;60(12):1031-1042. http://www.onlinejacc.org/content/60/12/1031. Accessed November 11, 2019.
https://www.uptodate.com/contents/cardiorenal-syndrome-definition-prevalence-diagnosis-and-pathophysiology?search=cardiorenal%20syndrome&source=search_result&selectedTitle=1~16&usage_type=default&display_rank=1
https://www.uptodate.com/contents/cardiorenal-syndrome-prognosis-and-treatment?search=cardiorenal%20syndrome&source=search_result&selectedTitle=2~16&usage_type=default&display_rank=2#H17931522