Embed Size (px)
Citation preview

Thyroid Function Tests
Case Study B
Presented by:Owen Naidoo
Abdullah OsmanChristine Tanzil
Ayse Togac

Ms MA (a middle-aged woman) presents to A&E with:
- History of abdominal pain- Vomiting
- Features of sepsis.

Investigations resulted in the diagnosis of:
Ruptured appendix (surgically removed)
Peritonitis

Her post-op recovery was complicated by:
Transient oliguric renal failure
Pneumonia

Her TFT results 6 days post-op were as follows:
FT4 5pmol/L 10-25pmol/L
FT3 <1pmol/L 3-8pmol/L
TSH 6 mU/L 0.4-4mU/L

She did not have clinical symptoms of thyroid dysfunction or a goitre and so
throxine treatment was not commenced.
Thyroxine

Two weeks post-op her TFT results were as follows and still she displayed no clinical signs
of thyroid disorder:
FT4 8pmol/L 10-25pmol/L
TSH 11mU/L 0.4-4mU/L

After a further three weeks, her TFT results were as
follows:
FT4 11pmol/L 10-25pmol/L
TSH 7mU/L 0.4-4mU/L
She also had a strongly positive peroxidase antibody
thyroxine treatment was commenced.

Some definitions… Thyroid Stimulating Hormone (TSH)
The levels of TSH are controlled by the pituitary gland depending on the circulating levels of thyroxine
Synthesises thyroid hormones from iodide and tyrosine residues
Thyroid hormones: These hormones are released into the peripheral
circulation when required through a negative feedback system
T4: is broken down in the peripheral circulation into T3 and r-T3
T3 and r-T3 should be found in the same proportions

What is hypothyroidism?
Hypothyroidism occurs in patients where there are insufficient levels of thyroid hormones
There are two types: Congenital hypothyroidism Acquired hypothyroidism

Congenital hypothyroidism
Primary hypothyroidism This is the most common cause of congenital
hypothyroidism
Secondary hypothyroidism This occurs when the pituitary gland produces
insufficient amounts of TSH (thyroid stimulating hormone)

Acquired hypothyroidism
Acquired hypothyroidism is caused by the thyroid gland being damaged (e.g. cancer therapy etc)
Primary hypothyroidism The most common cause is Hashimoto’s disease
Secondary hypothyroidism Is caused by a pituitary tumour
Tertiary hypothyroidism Is caused by a hypothalmic tumour

Signs & Symptoms…
Weakness/ Lethargy/ Slowness Cold intolerance Memory loss Weight gain Dry skin Change in voice (deepening) Mild anaemia/pernicious anaemia Effusions: pericardial, pleural, peritoneal &
joint spaces

PART 2
TASKS
ANALYSE MA’S RESULTS
ARE THEY CONSISTENT WITH HYPOTHYROIDISM?

MRS MA’S TFT RESULTS
TFT 6 DAYS POST OPP
14 DAYS POST OPP
35 DAYS POST OPP
REFERENCE
FT3 <1 3-8 pmol/L
FT4 5 8 11 10-25 pmol/L
TSH 6 11 7 0.4-4 mU/L
At 35 days tested strongly positive peroxidase antibody thyroxine commenced

SUMMARY OF MA’S TFT’S POST OP
DAY 6 Decreased FT4, elevated TSH
Day 14 Decreased FT4, elevated TSH
Day 35 Normal FT4, elevated TSH

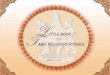
GRAPH SHOWING RELATIONSHIP OF MA’S TSH TO FT4
4
5
6
7
8
9
10
11
12
0 5 10 15 20 25 30 35 40
DAYS POST OP
FT4 (pM)
TSH (mU/L)
FSH (0.4-4 mU/L) FT4 (10-25 pmol/L)

DIAGNOSING MRS MA
WHAT DO WE KNOW: MA does have elevated TSH suggests hypothyroidism Most common cause of HT in the US is Hashimoto’s
Disease. MA is middle aged female likely candidate for
Hashimoto’s Strongly positive peroxidase antibody (an
autoantibody) Positive autoantibodies in 95% of cases of Hashimoto’s Advanced Hashimoto’s: low FT4, high TSH MA low FT4, elevated TSH BUT later normal FT4.

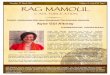
GRAPH SHOWING RELATIONSHIP OF MA’S TSH TO FT4
4
5
6
7
8
9
10
11
12
0 5 10 15 20 25 30 35 40
DAYS POST OP
FT4 (pM)
TSH (mU/L)
FSH (0.4-4 mU/L) FT4 (10-25 pmol/L)

POSSIBLITIES FOR MRS MA
READING TIME TFT RESULTS POSSIBLE DISEASE STATE
Possibly initially Low FT4, low TSH NTI (sepsis etc.)(aka euthyroid sick syndrome)
6 DAYS PO Low FT4, high TSH Recovery phase of NTI, advanced Hashimoto’s
12 DAYS PO Low FT4, high TSH Recovery phase of NTI, advanced Hashimoto’s
35 DAYS PO Normal FT4, high TSH Subclinical hypothyroidism, recovery phase of NTI,

CONCLUSION +ve antibody strongly suggests
Hashimoto’s But why the drastic changes in TFT’s? ?MA has a subclinical hypothyroidism
disorder (typical of early Hashimoto’s disease)
Unknown to patient since asymptomatic. During her illness she suffered from NTI
which decreased her FSH and T4 On recovering, levels return to her regular
levels of subclinical hypothyroidism.

TO TREAT OR NOT TO TREAT
During stay at hospital (NTI) controversial
Are patients TSH values decreasing and T4 values increasing?
If yes no need to treat. If no controversial but guidelines
recommend: treat if TSH>10mU/L or if TSH 5-10 mU/L and +ve peroxidase Ab &/
goitre (AACE, 2002).

WHY DO WE TREAT EVEN IF ASYMPTOMATIC
Avoid progression to overt hypothyroidism (3-20%, increased if +ve Ab)
Decrease CV effects, dyslipidemia, neuropsychiatric events

The Results…
6 days post-op 2 wks post-op 5 wks post-op Normal Range
T45 8 11 10-25 pmol/L
T3< 1 3 – 8 pmol/L
TSH 6 11 7 0.4 – 4 mU/L

What are the likely explanations for this series of TFT results?
Hashimoto’s Thyroiditis Subclinical Hypothyroidism Euthyroid Sick Syndrome (aka
NTI)

1. Hashimoto’s Thyroiditis Refers to autoimmune disorders of the thyroid gland. Antibodies and WBC’s damage the thyroid gland Due to excess WBC’s and fluid in the thyroid gland a
‘goitre’ is produced, leading to destruction of thyroid cells & HYPOTHYROIDISM
Destruction of thyroid gland decreases T4 production and as a results TSH increases which makes the goiter even larger.
In this condition thyroid antibodies and usually low; however this is not the case for Ms MA (‘…..strongly positive peroxidase antibody’)

2. Subclinical Hypothyroidism
Scenario characterised by a normal serum T4 and moderately high TSH levels. (N.B T3 levels are usually normal and thus don’t provide much extra in terms of diagnosis)
Serum antithyroid antibodies against peroxidase are usually, but not always, positive (as witnessed by Ms MA)

3. Euthyroid Sick Syndrome
Situation whereby patients with other non-thyroidal illnesses may have abnormal TFTs, mainly because of decreased peripheral conversion of T4 to T3 and decreased binding to TBG.
Clinical features of Euthyroid Sick Syndrome include low T3; normal or low T4 and variable TSH.

Describe analytical principles behind free T4
measurement…

What is free T4?
Free T4 or thyroxine is unbound and hence biologically active and responsible for the regulation of thyroid function through the pituitary feedback mechanism. Besides being a more specific indicator of thyroid function than total T4, free T4 is not subject to the spontaneous fluctuations or drug-induced changes that occur with total T4.

Principles of free T4 measurement…
Principle methods for measuring free T4 is as follows:
Equilibrium Dialysis (ED) Equilibrium Dialysis:-FT4 measured
directly by a sensitive RIA in the dialysate
Ultrafiltration Direct Immunoassays Free T4 index method

Free T4 determination by Equilibrium Dialysis
The serum is put inside the cylinder where bound is separated from free hormone.
The gold standard for measuring free T4 is overnight equilibrium dialysis of serum containing 125I-T4. -The percentage of free T4 is calculated by determining the total counts in the dialysate divided by the total 125I-T4 added to the serum multiplied by the total T4 concentration

Free T4 determination by Ultrafiltration
Ultrafiltration has almost the same principle as ED.
The serum has labelled T4 and this is filtered against a protein free buffer.
Free T4 concentration is worked out as: radiolabelled iodine is inversely proportional to free T4 concentration.

Free T4 determination by Immunoassays
There is a one step and two step method for calculating free T4 concentration by immunoassay (IAS).
Step 1 method: This method is based on the assumption that structurally modified and labelled analogues of T4 will not bind to serum thyroid hormone binding proteins but will compete with free T4 for binding to the T4 antibody introduced in the assay.

Free T4 determination by Immunoassays (cont)
Radio-labelled T4 analogue is added to anti-T4 antibody.
The serum is added to the anti-T4 antibody simultaneously.
Competition occurs and both T4 is removed.
Then you measure proportion of labelled T4 that became antibody bound.

Step 2 method:
Free T4 in patient serum is removed by binding to T4 antibody, which is attached to a solid phase.
The serum is then removed. Next, Radio-labelled 125I-T4 is incubated
with the solid phase that has unbound sites available.
Radio-labelled 125I-T4 is removed and activity is quantified.

Free T4 determination by Index method
The index method requires two independent tests.
One measuring total serum T4 and the other measuring thyroid hormone-binding ratio or T3 resin uptake.
The free T4 index is then calculated using the total T4 and the TBG level, the thyroid binding ratio, or T3 resin uptake.
The index is directly proportional to the free T4 level.

Advantages and Disadvantages
Equilibrium Dialysis: Advantages: Gold standard, accurate Disadvantages: Time consuming,
expensive, technically demanding Immunoassay:
Advantages: quick compared to ED, higher accuracy than ED, regularly available
Disadvantages: expensive, procedure has to be carried out precisely

What factors can effect T4?
Age Infection Stress Pregnancy

What Drugs can effect T4?
Amiodarone: structurally resembles thyroxine molecule. Decreases serum T4 levels
Phenytoin and Carbamazepine: accelerate clearance of T4 and depress FT4
Propranolol: elevation of serum free T4 levels Lithium: inhibits T4 release. Glucocorticoids: suppress T4 levels