Embed Size (px)
Citation preview

ThrombosisShock 2008

Normal hemostasisThrombosis – factors, morphologyEmbolismShockDICTTP,HUS
Doc. MUDr. L. Boudová, Ph. D.

Hemostasisnormal vesselsmaintain blood fluid, clot-freevessel injuryinduce rapid localized hemostatic plug
Thrombosisinappropriate activation of normalhemostatic processes
Vascular wall, platelets, coagulation cascade

EndotheliumNormal: antithrombotic1. Anticoagulant - heparin-like moleculesthrombomodulin2. Antiplatelet – barrier between plt and ECM;
PGI2, NO, ADPase3. Fibrinolytic – t-PA
Injured, activated: prothrombotic1. Procoagulant – tissue factor2. Platelets - vWF3. Antifibrinolytic - PAI

ThrombosisVirchow's 3Alteration of:
1. Vessel wall - endothelial injury - dominant
2. Blood flow- stasis, turbulence
3. Blood – hypercoagulability
may combine
intravital intravascularclotting

1. Vessel wall – endothelial injury – dominant
exposure of subendothelial collagen + adherence of platelets
exposure of tissue factor, local depletion of prostacyclin and plasminogen activator
• Atherosclerosis – ulceration
• Necrosis – myocardial infarction
• Trauma
• Inflammation – vasculitis
• Hypertension, turbulent flow, bact. endotoxins
• Homocystein, cholesterol, radiation, smoking

2. Alterations in normal blood flow
Normal = laminar
Turbulence – arteries, heart;
combined turb. + stasis (endot. injury + stasis)
Stasis – veins, heart
Ulcerated atherosclerotic plaques – endot. +turb.
Aneurysms – local stasis
Mitral valve stenosis – stasis – left atrial dilation
Hyperviscosity syndromes – polycythemia; sickle cell anemia (occlusions stasis; small vessels)

3. Hypercoagulability
• Primary (genetic)
Mutations in factor V = Leiden mutation
2-15% of popul. APC resistance
antithrombin III, protein C, S deficiencies
fibrinolysis def., hyperhomocysteinemia
↑prothrombin levels - 1%, allelic variations
• Thrombo(embolism) – recurrent, young,
no or insignificant other causes
• Secondary (acquired) - high risk or low risk
Any alteration of coagulation pathway predisposing to thrombosis

3. Hypercoagulability• Secondary (acquired)• ↑ High risk of thrombosis -immobilization, myoc.
infarction, tissue damage (trauma, burns, surgery), cancer, prosthetic cardiac valves, DIC, heparin-induced thrombocytopenia, antiphospholipid antibody syndrome (with/out autoimmune dis. - SLE)
• ↓Lower risk of thrombosis -atrial fibrillation, cardiomyopathy, nephrotic syndrome, hyperestrogenic states, oral contraceptives (3x), pregnancy (8x), sickle cell anemia, smokingThrombotic diathesis - often complicated, multifactorial

Thrombi - overview of morphology, localisationrelationship to the vessel wall, lumen
mural OR occlusive; line of attachmentlocalization anywhere - heart (chambers, valves), arteries,
veins, capillariessizes, shapes, components (colours)
red, white, mixed (coral), hyalinemechanismarteries, heart: endothelial injury, turbulenceveins: stasis

Thrombi
Localization - detailed
Arterial – occlusive; mixed
coronary, cerebral, femoral
atherosclerosis, vasculitis, trauma
Venous – occlusive, long cast; red; 90% legs
autopsy dif. dg. postmortem clot
Heart – valves – vegetations
infective or sterile (rheum., NBTE, SLE)
Heart chambers, aneurysms of heart or aorta
Mural; infarction; embolisation: brain, kidney, spleen

Further fate of thrombi1. Propagation2. Dissolution - fibrinolysis3. Organization and recanalization; fibrosis4. Enz. digestion Puriform. degen.5. !Embolization!6. Calcification
1
2 35
7. Infection

Clinical significance of thrombosis1. Vascular obstruction (mainly arteries)2. Source of embolism (mainly veins)
Veins: mainly lower extremitiesSpf.: trophic changes - cong., edem., pain; ulcersDeep: 50% asympt.! thromboembolism!
Regardless specific clinical setting: high age immobilization
!high risk of venous thrombosis!

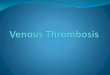
Embolisma detached intravascular mass- solid, liquid, gaseous carried by the blood to a site distant from its origin• Thrombus – 99%• Fat• Gas• Fluid – amniotic; • Atherosclerotic debris, tumor fragments, foreign bodies
VASCULAR BLOCK (ISCHAEMIA INFARCTION)

SOURCE: DEEP LEG VEIN THROMBI
ABOVE THE KNEE
Clinical manifestation
1. Clin. silent (75%), organization, fibrous bridging web
2. Acute cor pulmonale – sudden death (60% circ.)
3. Pulmonary hemorrhage/infarction
4. Pulmonary hypertension (multiple emb.)
Pulmonary thromboembolism
Saddle embolusParadoxical embolism

Systemic thromboembolismEmboli travelling in the syst. arterial circulation
• SOURCE: intracardiac mural thrombi (80%)aort. aneurysms, atherosclerotic plaques, valvular vegetations; paradoxical emboli
• RECIPIENTS: variouslegs (75%), brain (10%), intestines, kidneys, spleen, upper extr.
• CONSEQUENCES: collateral blood supply, tissue vulnerability to ischaemia, size of the occluded vessel MAINLY INFARCTION

Fat embolism• fractures of long bones, soft tissue trauma, burns90% of people with severe skeletal injuriesonly 10% symptomatic
• sudden onset: tachypnea, dyspnea, tachycardia, neurol. symptoms, petechiae; (thrombo, ery ↓)
• mechanical and biochemical injury• may be lethal
• HISTOLOGICAL DIAGNOSIS ?

Air embolismGas bubbles
• Obstetric procedures• Dural venous sinuses• Neck, chest wall trauma
• Decompression sickness - nitrogen bubbles focal ischemia: muscles, joints – bends; brain, heart;lungs - RDS (chokes)treatment: compression chamber
• Chronic decompression sickness – caisson diseasepersistence of gas emboli – multiple foci of ischemic necrosis(heads of femur, tibia, humerus)

Amniotic fluid embolism• Rare but ! High mortality• Mechanism: amniotic fluid in maternal circulation
How: tear in the placental membranes, rupture of uterine veins
• Mother: lungs: diffuse alveolar damagecapillaries: epithelial squamous cells from fetal skin, lanugo hair, fat from vernix caseosa, mucin from fetal respiratory tract and GIT
• Clinically: sudden; severe dyspnea, cyanosis, hypotension, shock, seizures, coma; pulmonary edema, DIC (thrombogenic substances from amniotic fluid);death

SHOCKSystemic hypoperfusion
caused by reduction of cardiac output effective circulating blood volume
hypotension, hypoperfusion, hypoxia
Cellular injury: first reversible
if persistence of shock - irreversible

1. Cardiogenic – pump failure (intrinsic myoc. cause – IM, ventr. arrhytmias, extrinsic compression – tamponade, outflow obstr.- emb.)
2. Hypovolemic - loss of blood or plasma (hemorrhage, burns, trauma)
3. Septic – systemic microbial infection
(G- endotoxic, G+, fungal)
4. Neurogenic – spinal cord injury - VSD
5. Anaphylactic – gener. IgE-med. response, VSD, ↑vascular permeability – ↑vascular bed capacitance
SHOCK

Pathogenesis of septic shockMost G-, endotoxins – lipopolysaccharides
Mononuclear cell activation, cytokines (IL-1, TNF)
Isolate microbes, activate immune system, eradicate microbes but also! further aggravation
cytokines and secondary mediators:
systemic VSD - hypotension,↓myoc. contractility,
↑endothel. injury, RDS, coagulation disorder – DIC
multiorgan system failure

Stages of shock
1. Nonprogressive – neurohumoral compensatory mechanisms, vital organ perfusion
2. Progressive – tissue hypoperfusion, anaerobic glycolysis, lactate acidosis, VSD, ↓cardiac output, anoxic injury of endothelium, DIC risk; vital organs begin to fail
3. Irreversible – lysosomal enzyme leakage

Morphology of shock
Hypoxic injury, multiple organ systems
Brain - ischemic encephalopathy
Heart - coagulation necrosis, hemorrhage
Kidneys - acute tubular necrosis
Lungs - shock lung (normally resistant to hypoxia)
Adrenals - cortical lipid depletion
GIT - hemorrhages and necroses
Liver - fatty change, central hemorrhagic necrosis

secondary complication
of some serious condition consumption coagulopathy
thrombohemorrhagic diathesis
acute, subacute, chronic
Disseminated intravascular coagulation (DIC)

Disseminated intravascular coagulation (DIC)
activation of coagulation sequence
microthrombi
- consumption of platelets and clotting factors
activation of fibrinolysissecondary

DIC Thrombotic and hemorrhagic diathesis
Microthrombi infarctions
depletion of platelets and clotting factors
+ secondary activation of fibrinolysis
hemorrhages
Consequences

Mechanisms of DIC trigger
1. Release of tissue factor or thromboplastic substances
2. Widespread endothelial injury

DIC
1. obstetrics – 50%; abruptio placentae, retained dead fetus, septic abortion, amniotic fluid embolism, toxemia
2. neoplasms – 30%; adenocarcinomas, AML
3. infections – gram-negative sepsis
4. trauma, burns, extensive surgery
5. other – snakebite, heat stroke, giant hemangioma, aortic aneurysm etc.

DIC• Morphology microthrombi
• kidneys hemorrhages
• lungs
• brain
• adrenals
• placenta
CLIN.: microangiopathic hemol. anemia, RDS, neurologic sympt., oliguria, ac. ren. and circul. failure, SHOCK

Thrombotic microangiopathiesthrombotic thrombocytopenic purpura (TTP)hemolytic-uremic syndrome (HUS)
VersusDisseminated intravascular coagulation
Common: hyaline thrombi
!!Differences: DIC: primary importance:
activation of clotting system

Thrombotic microangiopathiesrelated clinical syndromesthrombotic thrombocytopenic purpura (TTP)hemolytic-uremic syndrome (HUS)
ENDOTHELIAL INJURY WIDESPREAD HYALINE MICROTHROMBI
OVERLAP - common features (TTP, HUS):
• thrombocytopenia
• microangiopathic hemolytic anemia
• fever

Thrombotic microangiopathies
TTP
neurological deficits (transient)
renal failureadult womenADAMTS 13 defic.
HUS
mostly no neurol. sympt.acute renal failure DOMINANT!children; E. coli O157:H7, verotoxin
Common: thrombocytopenia, microangiopathic hemolytic anemia, fever