Embed Size (px)
Citation preview

doi:10.1016/j.jcin.2010.06.010 2010;3;911-919 J. Am. Coll. Cardiol. Intv.
Javier Botas, Felipe Hernández, and ESTROFA-2 Study Group Bullones, Jose R. Rumoroso, Bruno García del Blanco, Jose A. Baz, Francisco Bosa,Gomez Jaume, José M. Hernández, Josepa Mauri, Angel Sánchez Recalde, Juan A.
Mariano Larman, Jose F. Diaz, Jaime Elizaga, Javier Martín Moreiras, AlfredoRamón Lopez-Palop, Armando Pérez de Prado, Fernando Rivero, Juan Sanchis,
José M. de la Torre Hernández, Fernando Alfonso, Federico Gimeno, Jose A. Diarte, Sobre Trombosis de Stents Farmacoactivos de Segunda Generacion-2)
Results From the Multicenter Spanish Registry ESTROFA-2 (Estudio Español Thrombosis of Second-Generation Drug-Eluting Stents in Real Practice:
This information is current as of September 22, 2010
by Marie Morice on September 22, 2010 interventions.onlinejacc.orgDownloaded from

http://interventions.onlinejacc.org/cgi/content/full/3/9/911located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by Marie Morice on September 22, 2010 interventions.onlinejacc.orgDownloaded from

TSRE
JFRFJAJJFo
SHS
Oc
BpD
Mca
R2atafipda
Clot
FtCP
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 3 , N O . 9 , 2 0 1 0
© 2 0 1 0 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N I S S N 1 9 3 6 - 8 7 9 8 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . D O I : 1 0 . 1 0 1 6 / j . j c i n . 2 0 1 0 . 0 6 . 0 1 0
hrombosis of Second-Generation Drug-Elutingtents in Real Practiceesults From the Multicenter Spanish Registry ESTROFA-2 (Estudiospanol Sobre Trombosis de Stents Farmacoactivos de Segunda Generacion-2)
osé M. de la Torre Hernandez, MD, PHD,* Fernando Alfonso, MD, PHD,†ederico Gimeno, MD, PHD,# Jose A. Diarte, MD, PHD,**amon Lopez-Palop, MD, PHD,†† Armando Pérez de Prado, MD,‡‡ernando Rivero, MD,‡ Juan Sanchis, MD, PHD,§§ Mariano Larman, MD,� �
ose F. Diaz, MD,¶¶ Jaime Elizaga, MD, PHD,§ Javier Martın Moreiras, MD,##lfredo Gomez Jaume, MD, PHD,*** José M. Hernandez, MD, PHD,†††
osepa Mauri, MD, PHD,§§§ Angel Sanchez Recalde, MD,� Juan A. Bullones, MD,‡‡‡ose R. Rumoroso, MD, PHD,� � � Bruno Garcıa del Blanco, MD,¶¶¶ Jose A. Baz, MD,###rancisco Bosa, MD, PHD,**** Javier Botas, MD, PHD,†††† Felipe Hernandez, MD,¶n behalf of the ESTROFA-2 Study Group
antander, Madrid, Valladolid, Zaragoza, Alicante, León, Valencia, San Sebastian,uelva, Salamanca, Palma de Mallorca, Malaga, Badalona, Bilbao, Barcelona, Vigo,
anta Cruz de Tenerife, and Alcorcón, Spain
bjectives This study sought to evaluate second-generation drug-eluting stent (DES) thrombosis inlinical practice.
ackground First-generation DES are associated with a significant incidence of late thrombosis. There isaucity of data regarding real practice late thrombosis incidence and predictors with second-generationES, zotarolimus-eluting stent (ZES), and everolimus-eluting stents (EES).
ethods A prospective, large-scale, non-industry-linked multicenter registry was designed. Completelinical-procedural data and systematic follow-up of all patients treated with these stents was reported indedicated registry supported by the Spanish Working Group on Interventional Cardiology.
esults From 2005 to 2008, 4,768 patients were included in 34 centers: 2,549 treated with ZES, and,219 with EES. The cumulative incidence of definite/probable thrombosis for ZES was 1.3% at 1 yearnd 1.7% at 2 years and for EES 1.4% at 1 year and 1.7% at 2 years (p � 0.8). The increment of definitehrombosis between the first and second year was 0.2% and 0.25%, respectively. In a propensity scorenalysis, the incidence remained very similar. Ejection fraction (adjusted hazard ratio [HR]: 0.97; 95% con-dence interval [CI]: 0.95 to -0.99; p � 0.008), stent diameter (adjusted HR: 0.37; 95% CI: 0.17to 0.81;� 0.01) and bifurcations (adjusted HR: 2.1; 95% CI: 1.14 to 3.7; p � 0.02) emerged as independent pre-ictors of thrombosis. In the subgroup of patients with bifurcations, the use of ZES was independentlyssociated with a higher thrombosis rate (adjusted HR: 4; 95% CI: 1.1 to 13; p � 0.03).
onclusions In a real practice setting, the incidence of thrombosis at 2 years with ZES and EES wasow and quite similar. The incidence of very late thrombosis resulted lower than was reported in registriesf first-generation DES. In the subset of bifurcations, the use of ZES significantly increased the risk ofhrombosis. (J Am Coll Cardiol Intv 2010;3:911–9) © 2010 by the American College of Cardiology Foundation
rom the *Interventional Cardiology Department, Unidad de Hemodinamica y Cardiologıa Intervencionista, Hospital Universi-ario Marques de Valdecilla, Instituto de Formacion e Investigacion Marqués de Valdecilla, Santander, Spain; †Interventional
ardiology Department, Hospital Clınico San Carlos, Madrid, Spain; ‡Interventional Cardiology Department, Hospital de larincesa, Madrid, Spain; §Interventional Cardiology Department, Hospital Gregorio Maranon, Madrid, Spain; �Interventionalby Marie Morice on September 22, 2010 interventions.onlinejacc.orgDownloaded from

DiTcrgsctwd
yyzseifib
“bamfWnttV
PpttFsmstppgDiCptspacgMsCrrfiwasNSmatWaFcdt
p
CDDCCvCtt#S
PVHHDDoD†
AA
D
Es
Ps
Ss
Zs
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 3 , N O . 9 , 2 0 1 0
S E P T E M B E R 2 0 1 0 : 9 1 1 – 9
de la Torre Hernandez et al.
Registry of Second-Generation DES
912
rug-eluting stents (DES) have proved to be an outstand-ng improvement in the interventional cardiology field.heir known impact on restenosis rates drop in almost every
linical and lesional profile has expanded percutaneousevascularization horizons. Nevertheless, both first-eneration DES, paclitaxel-eluting stents (PES) andirolimus-eluting stents (SES), have been associated with aertain incidence of late thrombosis in trials that was greaterhan that observed with bare-metal stents (1). This incidenceas higher in real practice registries than in randomized trialsue to a frequent off-label use of these DES (2–6).Thrombosis of first-generation DES may occur up to 4
ears after implantation, with an increment after the firstear of 0.4% to 0.6% per year. Second-generation DES,otarolimus-eluting stents (ZES) and everolimus-elutingtents (EES), are already available. They have already beenvaluated in different clinical trials (7–14) and have shownn most of them a similar if not better safety profile thanrst-generation DES (7,8,10–13), but worse results haveeen also reported (9,14). However, once again, large
independent registries, withlong-term follow-up, are neededin order to assess late thrombosisincidence in the real-world clinicalpractice.
Methods
The ESTROFA-2 (Estudio Es-panol Sobre Trombosis deStents Farmacoactivos de Seg-unda Generacion-2) registry isan independent, multicenter,and prospective registry run by a
research hospital network” designed to assess DES throm-osis incidence in real practice. A total of 34 centers allround Spain have been involved. Economic costs andaintenance of the Web-based electronic clinical research
orum were held thanks to the support given by the Spanishorking Group on Interventional Cardiology. All coordi-
ation between the 34 participating centers, the adjudica-ion process, and analyses have been performed centrally athe coordination center Hospital Universitario Marques dealdecilla in Santander, Spain.
ardiology Department, Hospital La Paz, Madrid, Spain; ¶Interventional Cardiologyepartment, Hospital 12 de Octubre, Madrid, Spain; #Interventional Cardiologyepartment, Hospital Clinico de Valladolid, Valladolid, Spain; **Interventionalardiology Department, Hospital Miguel Servet, Zaragoza, Spain; ††Interventionalardiology Department, Hospital San Juan de Alicante, Alicante, Spain; ‡‡Inter-
entional Cardiology Department, Hospital de Leon, Leon, Spain; §§Interventionalardiology Department, Hospital Clinico de Valencia, Valencia, Spain; � �Interven-
ional Cardiology Department, Policlınica Guipúzcoa, San Sebastian, Spain; ¶¶In-erventional Cardiology Department, Hospital Juan Ramon Jiménez, Huelva, Spain;
bbreviations andcronyms
ES � drug-eluting stent(s)
ES � everolimus-elutingtent(s)
ES � paclitaxel-elutingtent(s)
ES � sirolimus-elutingtent(s)
ES � zotarolimus-elutingtent(s)
#Interventional Cardiology Department, Hospital Clinico de Salamanca,alamanca, Spain; ***Interventional Cardiology Department, Hospital Son Dureta, M
interventions.onlinejacc.orgDownloaded from
atient selection. All consecutive patients treated at thearticipating hospitals with either an EES or a ZES, sinceheir introduction in the Spanish market in 2005 to 2006 upo 2008, were prospectively entered in an electronic CRF.or the cases to be considered for final analysis, all lesionshould have been treated with EES or with ZES, with noix. Clinical, angiographic, and procedure features of every
ingle case were filled in by the local investigators. If ahrombosis event was detected in the established follow-uperiods, a wider detailed application form had to be com-leted. Data collection met all national requirements re-arding “data protection law” as well as anonymity.efinitions. All thrombosis recalled in this registry were
ndexed following the well-known Academic Researchonsortium definitions (15). Hyperlipidemia was defined aslasmatic cholesterol greater than 200 mg/dl or previousreatment with statins. Hypertension was defined as eitherystolic pressure greater than 140 mm Hg, or diastolicressure above 90 mm Hg or previous treatment withntihypertensive therapy. Renal function impairment wasonsidered for plasmatic creatinine above 1.5 mg/dl. An-iographic success was defined as TIMI (Thrombolysis Inyocardial Infarction) flow grade 3 along with residual
tenosis below 25%.linical follow-up. Information was obtained from medicaleports and hospital or interventional cardiology departmentegistries. In those cases with no events reported in hospitalles and no recent outpatient clinical visit, phone contactas required. All data regarding vital status, clinical events,
s well as new interventional procedures were, therefore,pecifically collected for the purpose of this investigation.onparticipant centers were contacted when necessary.tatistical analysis. Continuous variables are presented asean � SD. Categorical variables are expressed as percent-
ges. Continuous variables were compared with the Studenttest if the data followed a normal distribution and withilcoxon tests if the data were skewed. Categorical vari-
bles were compared with the chi-squared test or theischer exact test, where indicated. The survival curves wereonstructed with the use of Kaplan-Meier method toescribe the incidence of thrombosis over time, and log rankests were applied to evaluate differences between groups.
Because patients were not randomized to EES or ZES,ropensity scores (conditional probability) for receiving an
alma de Mallorca, Spain; †††Interventional Cardiology Department, Hospitalirgen de la Victoria, Malaga, Spain; ‡‡‡Interventional Cardiology Department,ospital Carlos Haya, Malaga, Spain; §§§Interventional Cardiology Department,ospital Germans Trias i Pujol, Badalona, Spain; � � �Interventional Cardiologyepartment, Hospital de Galdacano, Bilbao, Spain; ¶¶¶Interventional Cardiologyepartment, Hospital Vall d=Hebron, Barcelona, Spain; ###Interventional Cardiol-
gy Department, Hospital Meixoeiro, Vigo, Spain; ****Interventional Cardiologyepartment, Hospital Clinico de Tenerife, Santa Cruz de Tenerife, Spain; and the
†††Interventional Cardiology Department, Fundacion Alcorcon, Alcorcon, Spain.
anuscript received June 8, 2010, accepted June 11, 2010.
by Marie Morice on September 22, 2010

EuAgP
pthp
tiTicopcSt
R
Ar2p1pasgulEw
aF
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 3 , N O . 9 , 2 0 1 0 de la Torre Hernandez et al.
S E P T E M B E R 2 0 1 0 : 9 1 1 – 9 Registry of Second-Generation DES
913
ES rather than a ZES for each patient were calculated bysing baseline covariates within a logistic regression model.
baseline model was defined and included the demo-raphic, clinical, and procedural covariates listed in Table 1.atients were then matched according to their individual
Figure 1. Thrombosis Incidence in Overall Population
Incidence of stent thrombosis: (A) definite stent thrombosis (p � 0.6); (B) defi
Table 1. Clinical and Procedural Characteristics
ZES(n � 2,549)
EES(n � 2,219) p Value
Age, yrs 66.8 � 11.8 66.2 � 11.5 0.07
Women 601 (23.6%) 535 (24.1%) 0.7
Current smoker 744 (29.2%) 604 (27.2%) 0.1
Diabetes 803 (31.5%) 806 (36.3%) 0.0005
HBP 1,529 (60%) 1,303 (58.7%) 0.37
Hypercholesterolemia 1,313 (51.5%) 1,197 (53.9%) 0.1
Renal failure 191 (7.5%) 155 (7%) 0.5
LVEF, % 56.4 � 12.0 56.5 � 13.0 0.9
Previous MI 479 (18.8%) 424 (19.1%) 0.8
Previous PCI 543 (21.3%) 548 (24.7%) 0.006
Previous CABG 160 (6.3%) 164 (7.4%) 0.1
ACS 1,922 (75.4%) 1,529 (68.9%) �0.0001
MI 670 (26.3%) 355 (16%) �0.0001
Lesions treated 1.44 � 0.8 1.47 � 0.76 0.1
Total stent length, mm 34.8 � 23 34.5 � 24 0.6
Stent diameter, mm 2.95 � 0.4 2.98 � 0.4 0.01
Dual therapy, months 11.3 � 1.9 11.6 � 1.5 0.001
Lesions n � 3,670 n � 3,261
Total occlusion 125 (3.4%) 127 (3.9%) 0.2
Restenosis 136 (3.7%) 202 (6.2%) 0.0001
Bifurcation 484 (13.2%) 470 (14.4%) 0.1
Calcified 734 (20%) 668 (20.5%) 0.7
ACS � acute coronary syndrome; CABG � coronary artery bypass graft; EES � everolimus-eluting
stents; HBP � high blood pressure; LVEF � left ventricular ejection fraction; MI � myocardial
infarction; PCI � percutaneous coronary intervention; ZES � zotarolimus-eluting stents.
stent thrombosis (p � 0.24). The blue lines are for the zotarolimus-eluting stent (ZE
interventions.onlinejacc.orgDownloaded from
ropensity scores. The individual propensity score as well asype of stent were incorporated into Cox proportionalazard regression models as a covariate to calculate theropensity adjusted hazard ratio (HR).Identification of predictors of stent thrombosis was done
hrough a Cox proportional hazard regression model includ-ng those variables with p � 0.2 in the univariate analysis.he variable of antiplatelet therapy discontinuation was not
ncluded because that information was not available for allases without stent thrombosis. Only the prescribed periodf dual therapy could be included in this analysis. Allrobability values were 2-sided and values of p � 0.05 wereonsidered statistically significant. The statistical packagePSS version 15.0 (SPSS, Inc., Chicago, Illinois) was usedhroughout.
esults
total of 4,768 patients were prospectively included in theegistry; 2,549 of the patients were treated with ZES and,219 with EES. As a rule, dual antiplatelet therapy wasrescribed for up to 12 months (only 6.4% of EES- and0.6% of ZES-treated patients had dual antiplatelet therapyrescribed for 6 months). Clinical and procedural featuresre described in Table 1. The EES-treated patients werelightly younger, more frequently diabetics, and had areater rate of previous interventions. ZES were more oftensed during an acute coronary syndrome. As for theesional profile, more restenotic lesions were treated withES. Dual antiplatelet treatment recommended durationas slightly shorter for the ZES group.Thrombosis incidence (definite; definite and probable;
nd definite, probable, and possible) curves are displayed inigure 1. Cumulative stent thrombosis incidence for both
probable stent thrombosis (p � 0.8); (C) definite � probable � possible
nite �S) data, and the brown lines are for everolimus-eluting stent (EES) data.
by Marie Morice on September 22, 2010

ksif
oEaiii2o
uOfAttaw
wttime
tmbdSmtwtiZtc
swga19a0ttp
D
Fnsiipatdrpi
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 3 , N O . 9 , 2 0 1 0
S E P T E M B E R 2 0 1 0 : 9 1 1 – 9
de la Torre Hernandez et al.
Registry of Second-Generation DES
914
inds of stents is presented in Table 2. No statisticallyignificant difference was found between the 2 groups. Thencrease in definite stent thrombosis incidence observedrom the first to the second year was 0.2% to 0.25%.
Given the differences observed in the basal characteristicsf the 2 groups, a propensity score matching was performed.ventually, 1,300 patients from each group were selected
nd compared. Clinical and procedural features are detailedn Table 3. After adjusting, baseline characteristics weredentical in the 2 groups. Cumulative stent thrombosisncidence curves for matched groups are presented in Figure
and incidences in Table 4. No difference in the incidencef stent thrombosis was found after the matching process.Definite and probable thrombosis predictors found in
nivariate and multivariate analysis are presented in Table 5.nly bifurcations, ejection fraction, and stent diameter were
ound to be independent thrombosis predictors.ntiplatelet treatment. Inappropriate withdrawal of anti-hrombotic drugs was confirmed in up to 15% of definitehrombosis and 7% of probable thrombosis. However, dualntiplatelet treatment prescription (12 months vs. 6 months)as not found to be a predictor of stent thrombosis.As previously described, there was a subgroup of patients
ith dual therapy indicated during 6 months. These pa-ients were more frequently found in the ZES group. Weherefore decided to analyze stent thrombosis incidence onlyn patients with antiplatelet dual treatment indicated for 12
onths. As presented in Figure 3A, no difference was notedither.
Differences in stent thrombosis incidence between pa-ients with prescription for 6 months and those for 12onths are shown in Figure 3B. This incidence tended to
e greater in the 6-month treated group although theifference was concentrated in the early period.ubgroup analysis. Bifurcation-treated patients developedore cases of thrombosis (Fig. 4A). The use of complex
echniques (2 stents) tended to be higher among those casesith thrombosis (27.5% vs. 13.8%; p � 0.06). The use of
he double stent treatment for bifurcations was comparablen both stent groups (12.8% with EES and 14.9% withES; p � 0.4). As is shown in Figure 4B, a greater stent
hrombosis rate was demonstrated in ZES-treated bifur-
Table 2. Cumulative Incidences of Stent Thrombosis
Definite Def. � Prob. Def. � Prob. � Poss.
ZES EES ZES EES ZES EES
1 month 0.4 0.3 0.8 0.7 0.8 0.7
1 yr 0.8 0.75 1.3 1.4 1.8 1.5
2 yrs 1.0 1.0 1.7 1.75 2.5 2.0
p � 0.6 p � 0.8 p � 0.2
def � definite; poss � possible; prob � probable; other abbreviations as in Table 1.
ations. Bifurcation was the only lesion subset in which interventions.onlinejacc.orgDownloaded from
tatistically significant differences in stent thrombosisere found between stent types (Fig. 5) in matchedroups. This difference was observed both in the earlynd late period. Age (adjusted HR: 1.06, 95% CI: 1.01 to.12; p � 0.04), ejection fraction (adjusted HR: 0.96,5% confidence interval [CI]: 0.92 to 0.99; p � 0.02),nd ZES use (adjusted HR: 4, 95% CI: 1.1 to 13; p �.03) were found to be independent thrombosis predic-ors in bifurcation-treated patients. Based on our results,he double stent technique was not an independentredictor.
iscussion
irst-generation DES have proved to diminish the need forew revascularization in almost every clinical and lesionaletting leading to a spread in its use, even in off-labelndications. Low late thrombosis rates obtained from clin-cal trials have supported safety issues (1). Nevertheless, realractice registries frequently include off-label indicationsnd have consistently revealed a higher late thrombosis ratehan bare-metal stents, with a 1.2% to 1.7% first-yearefinite thrombosis rate and a 0.4% to 0.6% late thrombosisate per year later on (2–6). Mechanisms involved in thisrocess could be lack of long-term endothelialization, pos-tive arterial remodeling leading to late acquired incomplete
Table 3. Clinical and Procedural Characteristics in Propensity ScoreMatched Groups
ZES(n � 1,300)
EES(n � 1,300) p Value
Age, yrs 67.4 � 11.2 67.3 � 11.3 0.8
Women 331 (25.5%) 315 (24.2%) 0.5
Current smoker 347 (26.7%) 346 (26.6%) 0.9
Diabetes 430 (33%) 440 (33.8%) 0.7
HBP 832 (64%) 822 (63.2%) 0.7
Hypercholesterolemia 706 (54.3%) 728 (56%) 0.4
Renal failure 105 (8.1%) 109 (8.4%) 0.8
LVEF, % 57.4 � 12 57.6 � 13 0.8
Previous MI 218 (16.8%) 221 (17%) 0.9
Previous PCI 222 (17%) 212 (16.3%) 0.6
Previous CABG 88 (6.8%) 92 (7%) 0.9
ACS 928 (71.4%) 914 (70.3%) 0.6
MI 177 (13.6%) 165 (12.7%) 0.5
Lesions treated 1.43 � 0.8 1.43 � 0.7 0.9
Total stent length 33.5 � 23 33.2 � 24 0.7
Stent diameter, mm 2.98 � 0.4 2.99 � 0.4 0.5
Dual therapy, months 11.4 � 1.8 11.5 � 1.7 0.2
Lesions n � 1,859 n � 1,865
Total occlusion 71 (3.8%) 75 (4%) 0.8
Restenosis 19 (1%) 26 (1.4%) 0.2
Bifurcation 256 (13.8%) 250 (13.4%) 0.7
Calcified 375 (20.2%) 379 (20.3%) 0.9
Abbreviations as in Table 1.
by Marie Morice on September 22, 2010

st
dlaiEmLip(ECsMVtww
Tcetdsepb
p0(tTEA
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 3 , N O . 9 , 2 0 1 0 de la Torre Hernandez et al.
S E P T E M B E R 2 0 1 0 : 9 1 1 – 9 Registry of Second-Generation DES
915
tent apposition, and persistent local hypersensibility reac-ions possibly due to residual polymer (16).
Second-generation DES are made of new polymers andrugs. Pre-clinical studies show a promising faster endothe-
ialization with EES, compared with SES or PES (17). Inddition, the ultrasonographic analysis of patients with EESn the SPIRIT III (Clinical Evaluation of the Xience Vverolimus Eluting Coronary Stent System in the Treat-ent of Patients with de novo Native Coronary Arteryesions) trials (11) showed only a 1.1% of late acquired
ncomplete stent apposition. The ultrasonographic studieserformed in subgroups of patients in ENDEAVOR IIRandomized Controlled Trial to Evaluate the Safety andfficacy of the Medtronic AVE ABT-578 Eluting Driveroronary Stent in De Novo Native Coronary Artery Le-
ions) and III (Randomized Controlled Trial of theedtronic Endeavor Drug-Eluting Coronary Stent System
ersus the Cypher Sirolimus-Eluting Coronary Stent Sys-em in De Novo Native Coronary Artery Lesions) trialsith ZES yielded a complete and uniform intimal coverageithout late acquired incomplete stent apposition (18).
Figure 2. Thrombosis Incidence in Matched Groups
Incidence of stent thrombosis in matched groups: (A) definite stent thrombosiprobable � possible stent thrombosis (p � 0.4). The blue lines are for the zodata. Abbreviations as in Figure 1.
Table 4. Cumulative Incidences of Stent Thrombosis in Propensity ScoreMatched Groups
Definite Def. � Prob. Def. � Prob. � Poss.
ZES EES ZES EES ZES EES
1 month 0.6 0.3 1.0 0.6 1.0 0.6
1 yr 0.9 0.85 1.5 1.5 2.1 1.6
2 yrs 1.0 1.1 1.7 1.9 2.6 2.35
p � 0.8 p � 0.9 p � 0.4
Abbreviations as in Tables 1 and 2.
interventions.onlinejacc.orgDownloaded from
hese latter results have been confirmed using opticaloherence tomography in the ODESSA (Optical Coher-nce Tomography for DES Safety) trial (19). Despite ofhese findings, these stents have already been evaluated inifferent clinical trials showing disparate results regardingafety comparison with first-generation DES (7–14). Nev-rtheless, the clinical trials carried out to date have not beenowerful enough to point out differences in thrombosis ratesetween stent models.However, EES and ZES significantly differ in their
erformance. Late lumen loss with EES is very low, around.15 mm (10,11), whereas it is greater with ZES, 0.6 mm7,8). Hence, this different efficacy profile may potentiallyranslate into safety issues.hrombosis of ZES in trials. Combined analysis ofNDEAVOR I, II, and III (Multicenter Evaluation ofBT-578 Elution From a Phosphorylcholine-Coated
0.8); (B) definite � probable stent thrombosis (p � 0.9); (C) definite �
us-eluting stent data, and the brown lines are for everolimus-eluting stent
Table 5. Predictors of Stent Thrombosis
HR 95% CI p Value
Univariate analysis
Bifurcations 1.75 1.04–2.9 0.03
EF 0.97 0.95–0.99 0.005
HBP 1.8 1.06–3.0 0.03
Stent diameter 0.4 0.2–0.91 0.03
RF 2.03 1.01–3.9 0.04
Age 1.02 1.003–1.04 0.02
Multivariate analysis
Bifurcations 2.1 1.14–3.7 0.02
EF 0.97 0.95–0.99 0.008
Stent diameter 0.37 0.17–0.81 0.01
s (p �
tarolim
CI � confidence interval; HR � hazard ratio; RF � renal failure; other abbreviations as in Table 1.
by Marie Morice on September 22, 2010

SomofoSSaSo
idad1tT6tpra6
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 3 , N O . 9 , 2 0 1 0
S E P T E M B E R 2 0 1 0 : 9 1 1 – 9
de la Torre Hernandez et al.
Registry of Second-Generation DES
916
tent) trials with a total of 1,317 ZES treated patients,btained an absence of thrombosis after 14 days of deploy-ent and up to 2 years, being the final thrombosis rate of
nly 0.3% (20). However, these results diverge from thoseound in ENDEAVOR IV (Randomized, Controlled Trialf the Medtronic Endeavor Drug-Eluting Coronary Stentystem Versus the Taxus Paclitaxel-Eluting Coronary Stentystem in De Novo Native Coronary Artery Lesions) (9)nd SORT OUT III (Comparison of Zotarolimus-Elutingtents and Sirolimus-Eluting Stents in Patients With Cor-
Figure 3. Thrombosis Incidence and Dual Antiplatelet Therapy Duration
(A) Incidence of definite � probable stent thrombosis in cases with dualantiplatelet therapy prescribed for 12 months (p � 0.5). The blue line isfor the zotarolimus-eluting stent data, and the brown line is for everoli-mus-eluting stent data. (B) Incidence of definite � probable stent throm-bosis in cases with dual antiplatelet therapy prescribed for 12 months or 6months (p � 0.19). The blue line is for 6-month data, and the brown lineis for 12-month data. Abbreviations as in Figure 1.
nary Artery Disease) (14) trials. In the first study (9), interventions.onlinejacc.orgDownloaded from
nvolving 773 ZES- and 775 PES-treated patients, 1-yearefinite plus probable thrombosis rate was 0.1% with PESnd 1% with ZES. In the SORT OUT III (14) study,efinite thrombosis incidence at 18 months was 1.2% in,162 ZES-treated patients and 0.6% in the 1,170 SES-reated patients.hrombosis of EES in trials. In the SPIRIT III study, the69 patients treated with EES showed a global stenthrombosis incidence similar to that of 332 PES-treatedatients. However, a trend toward lower late thrombosisate was noted in EES-treated patients after the first yearnd in those in whom thienopyridine withdrawal took placemonth after the procedure (12).
Figure 4. Thrombosis Incidence in Patients With Bifurcations Treated
(A) Incidence of definite � probable stent thrombosis in cases with and with-out bifurcations treated (p � 0.019). The blue line indicates no bifurcations,and the brown line indicates bifurcations. (B) Incidence of definite � proba-ble stent thrombosis in bifurcations of both stent groups (p � 0.017). Theblue line is for the zotarolimus-eluting stent data, and the brown line is for
everolimus-eluting stent data. Abbreviations as in Figure 1.by Marie Morice on September 22, 2010

dbpyp1
Et1TwTimtfbilad
rmwbsnaowl
8wtwnroEerce
pdahuo
lwDm
gndriDffbcb6
eacErtbfiTcb
p1
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 3 , N O . 9 , 2 0 1 0 de la Torre Hernandez et al.
S E P T E M B E R 2 0 1 0 : 9 1 1 – 9 Registry of Second-Generation DES
917
In the pooled SPIRIT II and III analysis (21), lateefinite plus probable thrombosis rate at 1 year was 0.8% foroth the 892 EES-treated patients and the 410 PES-treatedatients. The larger SPIRIT IV study (22), not publishedet, has shown in 2,459 EES-treated patients a definite plusrobable thrombosis rate at 1 year of 0.29% compared with.06% in PE-treated patients.The COMPARE (Second-Generation Everolimus-
luting and Paclitaxel-Eluting Stents in Real-Life Practice)rial (13), which aimed to compare EES versus PES, found-year thrombosis rate to be significantly lower with EES.his difference was due to a lower subacute thrombosis rate,hereas late thrombosis was similar in both groups (13).hrombosis in second-generation DES registries. After thesenconclusive results and taking into account the already
entioned limitations of clinical trials, it becomes necessaryo evaluate the real practice outcomes including long-termollow-up to assess whether second-generation DES throm-osis rate remains similar to that of first-generation DES orf they differ. Moreover, it is essential to find out whetherate thrombosis rate is comparable in the 2 currentlyvailable second-generation DES, taking into account theirifferent behaviors (lower late lumen loss with EES).To assess these questions, the Rotterdam team has
eported its real practice experience with EES up to 6onths. Six-month outcomes in 649 EES-treated patientsere compared with cohorts of patients treated with eitherare-metal stents, PES, or SES (23). They found notatistically significant differences in thrombosis rates; ofote, no thromboses were detected in EES-treated patientsfter 1 month. However, no conclusions regarding the safetyf the stent profile could be done as the number of patientsas relatively small. In addition, clinical follow-up was
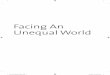
Age > 75 years
Male
HBP
Diabetes
MI
EF<45%
Stent diameter < 3 mm
Total stent length > 50 mm
Bifurcations
1.78 (0.6-5.2)
1.36 (0.67-2.8)
1.06 (0.5-2.2)
1.07 (0.36-3.2)
0.55 (0.09-3.3)
1.66 (0.4-6.8)
1.17 (0.47-2.9)
0.5 (0.12-1.9)
5.4 (1.2-25)
HR 0.1 1 10
ZES better EES better
Figure 5. Forest Plot EES Versus ZES
Differences in thrombosis risk between EES and ZES in clinical and lesionsubsets within matched groups. Abbreviations as in Figure 1.
imited at 6 months. p interventions.onlinejacc.orgDownloaded from
The E-Five Registry (a prospective registry) involved,314 ZES-treated patients in 118 centers. In this registry,ith a follow-up limited to 1 year, definite/probable stent
hrombosis rate was 1.1% (24). However, it was unclearhether patient inclusion was consecutive. In fact, theumber of lesions treated per patient was only 1.2 (in ouregistry this was 1.45, which correlates better with numbersbtained in nonselective global series).STROFA-2 registry. Our ESTROFA-2 registry aimed tovaluate definite plus probable and possible stent thrombosisates for up to 2 years in an ample “all comers” group ofonsecutive cases treated with EES and ZES, with noxclusion criteria.
Clinical and lesional features revealed a standard real-ractice profile. Being a registry, ZES and EES groupsiffer in some characteristics: ZES were used more often incute coronary syndromes (maybe due to a pre-conceivedigher safety profile), whereas EES, were more frequentlysed in diabetics and restenotic lesions (perhaps as the resultf their lower late lumen loss).Thrombosis rates following the different definitions were
ow and comparable between groups. This lack of differenceas confirmed also after matching propensity score analysis.efinite thrombosis rate at 2 years was 1% with an incre-ent between the first and second year of 0.2% to 0.25%.Comparing these results with those obtained in first-
eneration DES registries is intricate as a great amount ofoncontrollable factors could be playing a role. However,efinite thrombosis rate at 1 year in first-generation DESegistries was around 1.2% to 1.7% with a thrombosisncrement after the first year of 0.4% to 0.6% (2–6).
ifferent issues could help to explain this difference apartrom those intrinsic to DES. A better selection of patientsor DES took place after 2006 because of the “late throm-osis DES crisis,” but certainly clinical profile remainsomparable and DES penetration (at least in Spain) haseen even higher in ESTROFA-2 inclusion period (55% to0%) than in ESTROFA inclusion period (35% to 40%).Therapeutic compliance and dual antiplatelet treatment
xtent could also have increased. Indeed, mean time of dualntiplatelet treatment in ESTROFA registry was 8 monthsompared with almost 12 months in ESTROFA-2 (5). InSTROFA, up to 31.6% of definite thromboses were
elated to nontreatment compliance compared with 15% inhe present registry. This statement could be linked to aetter compliance but also to a greater susceptibility ofrst-generation DES to antiplatelet treatment withdrawal.he lack of specific evaluation of antiplatelet treatment
ompliance in these registries remains a caveat that shoulde addressed in future, dedicated registries.Regarding duration of dual antiplatelet treatment, most
atients in this study were instructed to continue it during2 months. There was a small group with only 6-month
rescriptions. These patients were more frequently found inby Marie Morice on September 22, 2010

tsttgcgo
ltBstDfUtrflftSnatihMg
sgfsty
aebcbtp
tTptaot
C
Itwt0SigZt
ATa
RHo3
R
1
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 3 , N O . 9 , 2 0 1 0
S E P T E M B E R 2 0 1 0 : 9 1 1 – 9
de la Torre Hernandez et al.
Registry of Second-Generation DES
918
he ZES group, most probably due to an understood highafety profile. This group showed a nonsignificant trendoward more thrombosis but, paradoxically, it was concen-rated in the early stage. These findings suggest that thisroup could be conformed of patients with worse biologicalonditions and more comorbidities that could lead to areater bleeding risk. Anyway, this variable did not comeut as a predictor in the analysis.Finally, thrombosis predictors detected in our analysis—
ower ejection fraction, lower stent diameter, and bifurca-ions—had already been documented in other studies (2,3).ifurcations have been analyzed in depth, as it was the only
ubset in which statistically significant differences regardinghrombosis rates were observed in among second-generationES. Thrombosis rates in ZES-treated patients with bi-
urcation lesions were greater in both early and late stages.se of ZES was an independent predictor of thrombosis in
he subgroup of patients with bifurcation lesions. Theeason for this could be explained by means of variousactors such as greater late lumen loss (favoring a restenosiseading to a prothrombotic condition) and different plat-orm design. Anyway, the reason remains unknown andhese findings warrant further research.tudy limitations. Being a registry implies observational andonrandomized findings. Stents were assigned by the oper-tor, and even with matching propensity score analysis,here remain underlying variables that could play a rolen the results. That is why the comparison of both groupsas to be done by taking into account this limitation.oreover, the different outcome of the bifurcational sub-
roups in both stent groups should be considered cautiously.Using these results to obtain conclusions regarding
econd-generation DES safety as opposed to first-eneration DES is even tougher. This does not nullify theact that the second-generation DES safety profile in theettings in which they are used nowadays is better thanhe profile revealed by first-generation DES in the previousears.
Antiplatelet treatment compliance was not possible tonalyze. This would have required a very frequent andxhaustive monitoring of every single patient, which waseyond the potential of the registry. The antiplatelet therapyessation would probably be a major determinant of throm-osis, though we do not know how many patients withouthrombosis had discontinuation of therapy in the studyeriod.Patients with previous percutaneous coronary interven-
ion procedures (whatever the stent type) were included.his fact could be a problem in the adjudication of arobable thrombosis event; however, every single case ofhrombosis was carefully analyzed, and we did not have suchconflictive case. Last but not least, the earlier introductionf ZES in the Spanish market implies a longer follow-up of
hese patients than for EES-treated patients.interventions.onlinejacc.orgDownloaded from
onclusions
n a real practice setting with frequent off-label indications,he incidence of thrombosis at 2 years with ZES and EESas low and quite similar. The incidence increase of definite
hrombosis between the first and second years was 0.2% to.25%, which is lower than the rates previously reported forES and PES (0.4% to 0.6%). This finding suggests that the
ncidence of very late thrombosis could be lower for second-eneration DES. In the subset of bifurcations, the use ofES could be associated with a higher risk of thrombosis,
hough this finding warrants further research.
cknowledgmenthe authors thank Dr. Tamara Garcia Camarero for her
ssistance with the statistical analysis.
eprint requests and correspondence: Dr. Jose M. de la Torreernandez, Unidad de Hemodinamica y Cardiologıa Intervenci-
nista, Hospital Universitario Marques de Valdecilla, Santander9012, Spain. E-mail: [email protected].
EFERENCES
1. Stone GW, Moses JW, Ellis SG, et al. Safety and efficacy of sirolimusand paclitaxel-eluting coronary stents. N Engl J Med 2007;356:998–1008.
2. Iakovou I, Schmidt T, Bonizzoni E, et al. Incidence, predictors andoutcome of thrombosis after successful implantation of drug elutingstents. JAMA 2005;293:2126–30.
3. Kuchulakanti PK, Chu WW, Torguson R, et al. Correlates andlong-term outcomes of angiographically proven stent thrombosis withsirolimus and paclitaxel eluting stents. Circulation 2006;113:1108–13.
4. Daemen J, Wenaweser P, Tsuchida K, et al. Early and late coronarystent thrombosis of sirolimus-eluting and paclitaxel-eluting stents inroutine clinical practice: results from a large two-institutional cohortstudy. Lancet 2007;369:667–8.
5. De la Torre-Hernandez JM, Alfonso F, Hernandez F, et al., for theESTROFA Study Group. Drug-eluting stent thrombosis: results fromthe multi-center Spanish registry ESTROFA (Estudio ESpanol sobreTROmbosis de stents Farmacoactivos). J Am Coll Cardiol 2008;51:986–90.
6. Wenaweser P, Daemen J, Zwahlen M, et al. Incidence and correlatesof drug-eluting stent thrombosis in routine clinical practice. J Am CollCardiol 2008;52:1134–40.
7. Fajadet J, Wijns W, Laarman GJ, et al., for the ENDEAVOR IIInvestigators. Randomized, double blind, multicenter study of theEndeavor zotarolimus-eluting phosphorylcholine-encapsulated stentfor the treatment of native coronary artery lesions: clinical andangiographic results of the ENDEAVOR II trial. Circulation 2006;114:798–806.
8. Kandzari DE, Leon MB, Popma JJ, et al., for the ENDEAVOR IIIInvestigators. Comparison of zotarolimus-eluting and sirolimus-eluting stents in patients with native coronary artery disease: a random-ized controlled trial. J Am Coll Cardiol 2006;48:2440–7.
9. Leon MB, Mauri L, Popma JJ, et al., for ENDEAVOR IV Investi-gators. A randomized comparison of the Endeavor zotarolimus-elutingstent versus the TAXUS paclitaxel-eluting stent in de novo nativecoronary lesions. 12 month outcomes from the ENDEAVOR IV trial.J Am Coll Cardiol 2010;55:543–54.
0. Serruys PW, Ruygrook P, Neuzner J, et al. A randomized comparison
of an everolimus-eluting coronary stent with a paclitaxel-elutingcoronary stent: the SPIRIT II trial. EuroIntervention 2006;2:286–94.by Marie Morice on September 22, 2010

1
1
1
1
1
1
1
1
1
2
2
2
2
2
K
AI
JJTNCPMpCpJA
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 3 , N O . 9 , 2 0 1 0 de la Torre Hernandez et al.
S E P T E M B E R 2 0 1 0 : 9 1 1 – 9 Registry of Second-Generation DES
919
1. Stone GW, Midei M, Newman W, et al., for the SPIRIT IIIInvestigators. Comparison of an everolimus-eluting stent and apaclitaxel-eluting stent in patients with coronary artery disease: arandomized trial. JAMA 2008;299:1903–13.
2. Stone GW, Midei M, Newman W, et al., for SPIRIT III Investigators.Randomized comparison of everolimus-eluting and paclitaxel-elutingstents. Two year clinical follow up from the clinical evaluation of theXience V everolimus-eluting coronary stent system in the treatment ofpatients with the novo native coronary artery lesions SPIRIT III trial.Circulation 2009;119:680–6.
3. Kedhi E, Joesoef KS, McFadden E, et al. Second generationeverolimus-eluting stent and paclitaxel eluting stents in real-life prac-tice (COMPARE): a randomised trial. Lancet 2010;375:201–9.
4. Rasmussen K, Maeng M, Kaltoft A, et al., for SORT OUT III StudyGroup. Efficacy and safety of zotarolimus-eluting stent and sirolimus-eluting coronary stents in routine clinical care (SORT OUT III): arandomized controlled superiority trial. Lancet 2010;375:1090–9.
5. Cutlip DE, Windecker S, Mehran R, et al., for Academic ResearchConsortium. Clinical end points in coronary stents trials—a case forstandardized definitions. Circulation 2007;115:2344–51.
6. Jaffe R, Strauss BH. Late and very late thrombosis of drug-elutingstents. Evolving concepts and perspectives. J Am Coll Cardiol 2007;50:119–27.
7. Joner M, Nakazawa G, Finn AV, et al. Endothelial cell recoverybetween comparator polymer-based drug-eluting stents. J Am CollCardiol 2008;52:333–42.
8. Sakurai R, Bonneau HN, Honda Y, Fitzgerald PJ. Intravascularultrasound findings in ENDEAVOR II and ENDEAVOR III. Am JCardiol 2007;100 Suppl 8B:71M–76M.
9. Guagliumi G. Optical coherence tomography for DES safety(ODESSA trial). Paper presented at: Transcatheter Therapeutics;September 2008; Washington, DC. Available at: http://www.tctmd.com/show.aspx?id�69992. Accessed May 15, 2010.
0. Gershlick A, Kandzari DE, Leon MB, et al., for the ENDEAVORInvestigators. Zotarolimus-eluting stents in patients with native coro-nary artery disease: clinical and angiographic outcomes in 1317 pa-tients. Am J Cardiol 2007;100 Suppl 8B:45M–55M.
1. Miu R, Serruys PW, Stone GW, et al. Performance of everolimus-eluting stents: pooled analysis from the SPIRIT trials. J Interven
Cardiol 2009;22:S41–S47. Minterventions.onlinejacc.orgDownloaded from
2. Stone GW. SPIRIT IV. A prospective, randomized trial comparing aneverolimus-eluting stent and a paclitaxel-eluting stent in patients withcoronary artery disease. One year clinical results. Paper presented at:Transcatheter Therapeutics; September 2009; San Francisco, CA.Available at: http://www.tctmd.com/show.aspx?id�84104. AccessedMay 15, 2010.
3. Onuma Y, Kukreja N, Piazza N, et al., for Interventional Cardiologistsof the Thoraxcenter (2000 to 2007). The everolimus-eluting stent inreal world patients. 6 month follow up of the X-SEARCH (Xience VStent Evaluated at Rotterdam Cardiac Hospital) Registry. J Am CollCardiol 2009;54:269–76.
4. Lotan C, Meredith IT, Mauri L, Liu M, Rothman MT, for E-FiveInvestigators. Safety and effectiveness of the Endeavour zotarolimus-eluting stent in real-world clinical practice: 12 month data from theE-Five registry. J Am Coll Cardiol Intv 2009;2:1227–35.
ey Words: coronary � stents � thrombosis.
ppendix: List of Other Participatingnvestigators and Corresponding Centers
uan C. Fernandez Guerrero (Complejo Hospitalario deaén, Jaén, Spain), José Moreu (Hospital Virgen de la Salud,oledo, Spain), Rafael Melgares (Hospital Virgen de lasieves, Ganada, Spain), José M. Vazquez (Hospital de laoruna, La Coruna, Spain), Adolfo Rincon (Hospital Dr.eset, Valencia, Spain), Jose D. Cascon (Hospital Santaaria del Rosell, Cartagena, Spain), Antonio Serra (Hos-
ital del Mar, Barcelona, Spain), Inigo Lozano (Hospitalentral de Asturias, Oviedo, Spain), Ramiro Trillo (Hos-ital Clınico de Santiago, Santiago de Compostela, Spain),esús M. Jiménez Mazuecos (Hospital General de Albacete,lbacete), Eduardo Pinar (Hospital Virgen de la Arrixaca,
urcia, Spain).by Marie Morice on September 22, 2010

doi:10.1016/j.jcin.2010.06.010 2010;3;911-919 J. Am. Coll. Cardiol. Intv.
Javier Botas, Felipe Hernández, and ESTROFA-2 Study Group Bullones, Jose R. Rumoroso, Bruno García del Blanco, Jose A. Baz, Francisco Bosa,Gomez Jaume, José M. Hernández, Josepa Mauri, Angel Sánchez Recalde, Juan A.
Mariano Larman, Jose F. Diaz, Jaime Elizaga, Javier Martín Moreiras, AlfredoRamón Lopez-Palop, Armando Pérez de Prado, Fernando Rivero, Juan Sanchis,
José M. de la Torre Hernández, Fernando Alfonso, Federico Gimeno, Jose A. Diarte, Sobre Trombosis de Stents Farmacoactivos de Segunda Generacion-2)
Results From the Multicenter Spanish Registry ESTROFA-2 (Estudio Español Thrombosis of Second-Generation Drug-Eluting Stents in Real Practice:
This information is current as of September 22, 2010
& ServicesUpdated Information
http://interventions.onlinejacc.org/cgi/content/full/3/9/911including high-resolution figures, can be found at:
References
BLhttp://interventions.onlinejacc.org/cgi/content/full/3/9/911#BIfree at: This article cites 22 articles, 14 of which you can access for
Rights & Permissions
http://interventions.onlinejacc.org/misc/permissions.dtltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://interventions.onlinejacc.org/misc/reprints.dtl
Information about ordering reprints can be found online:
by Marie Morice on September 22, 2010 interventions.onlinejacc.orgDownloaded from