Embed Size (px)
Citation preview

122
THROMBOSIS OF THE INTERNAL CAROTIDARTERY
By G. E. SMYTH, M.D., F.R.C.P.Consultant Physician, Manchester Royal Infirmary
Seen in long-term perspectiye the discovery ofX-rays and their use as a diagnostic agent mustsurely rank as one of the major advances in medi-cine, Though of less immediate practical benefitthan were either anaesthesia or antisepsis, thescientific importance was greater and even now,after more than fifty years, new techniques arestill being evolved with resulting increases inknowledge.Among the many sub-divisions of radiology the
introduction of contrast radiography in exploringthe vascular pattern of organs otherwise inac-cessible, has been one of the more recent and mostfruitful developments. A striking instance is theuse of percutaneous carotid angiography with theconsequent recognition of thrombosis of theinternal carotid artery. No doubt from time totime an inquisitive morbid anatomist had inspectedthe carotid arteries in the neck and found one orother occluded, but the fact passed unrecordedand was doubtless regarded as nothing more thana pathological curiosity. It is interesting, however,to recall that Ramsay Hunt (1914), in discussingcerebral vascular disease referred to the possibilitythat some cases of hemiplegia might be the resultof thrombosis in the carotid vessels and suggestedthat it would be wise for the clinician to examinethe state of the carqtid pulsation in all cases ofsudden hemiplegia. His plea was either ignoredor soon forgotten and we hear no more of thematter until Moniz and his associates (1937),rediscovered thrombosis of the internal carotidartery in the course of their pioneer studies incerebral angiography. The word 'rediscovered'scarcely does justice, however, to their findings,for, in reporting four cases of carotid occlusion,they showed at once that the condition was onewhich could be recognised during life and whichin all probability was by no means excessively rare.Since then a good deal has been learned confirmingtheir pioneer observations and at the present daythe general physician, just as much as the neurolo-gist' has the possibility of carotid occlusion inihind whenever he is confronted with a case ofsudden hemiplegia.
Valuable pathological evidence was brought
forward by Hultqvist (i942). He reported on aseries of 3,500 autopsies in which he examined thecarotid vessels and evidence of occlusion was foundin no less than 91 instances. The majorityoccurred in the sixth and seventh decades and thecondition was about twice as common in men as inwomen. These converging lines, radiological andpathological, indicated that occlusion in thecarctid vessels was relatively common and thatwith an adequate radiological technique it could beclearly demonstrated. Clinical recognition duringlife is, however, another matter and even with therapid gain in experience over the past few years thediagnosis still remains conjectural in the majorityof cases. A large number of case reports haveappeared in recent years, mostly of quite smallseries of cases. Special mention must, however,be made of the admirable review by Cloake (I95I).
Before reviewing the symptomatology it will beadvisable to say something of the pathology of thecondition. It is now accepted that the greatmajority, at least two-thirds, are a primarythrombosis beginning in the carotid sinus, someo.5 cm. distal to the origin of the internal carotidartery (Fig. i). A very small number originate inthe common carotid itself and a few at higherlevels of the internal carotid, in some cases evenas high as the intracranial portion of the vessel.Why the carotid sinus should be the site of pre-dilection is obscure though Hultqvist (q.v.)showed that this region shares with the coronaryvessels and the abdominal aorta an unusualtendency to develop atheroma and to develop itprematurely. In some cases no doubt theprimary lesion in the vessel is an embolus thoughthe relative incidence of this condition is unknownand Hultqvist himself recognised that even atautopsy it was sometimes difficult to determinethis point with certainty.
SymptomatologyFrom the writer's personal experience and from
a survey of the literature it would seem that inrather less than half of the cases the disease showsitself by a sudden and devastating hemiplegia.
copyright. on A
ugust 1, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.32.365.122 on 1 M
arch 1956. Dow
nloaded from

March I956 SMYTH: Thrombosis of the Internal Carotid Artery I23·''::"' "·:·1::1···.:;);:1
:·····l;l···:;i;i
... :·:;ll"ii:iiL·riB:b:lll1·;iei.l.rj;.g ···.::.::::I:; ··;lrr'(ii.ifi::·iiiiili/8PI;::I..
iil!8ii.
II;; rpr
··' .i:::
"r*r.d.·'
*i ..r
:·iii··
FIG. i.-Radiograph showing a very typical example ofocclusion of the internal carotid artery.
SUPERIOR TEMPORALARTERY
I
EXTERNALAUDITORY MEATUS
/ EXTERNALCAROTID ARTERY
STUMP OFINTERNAL CAROTID
Tracing of Fig. i.
This form of the disease is the most immediatelymenacing for full half of these patients may beexpected to die within a few days and the re-mainder are likely to be left with severe anddisabling hemiplegia. In a smaller number ofcases the paresis is less profound and often affectsthe limbs unequally, the arm being more severelyaffected than the leg. In a right-handed personsome degree of dysphasia is to be expected.Hemianopia, either complete or incomplete is,on the whole, rare. On the whole notor symptomsgreatly predominate over sensory. An interestingpoint is that in a fair proportion of cases the onsetof the attack is heralded or even preceded by hoursor days, by a certain degree of headache, localizedabout the temple on the affected side or morediffusely over the side of the head. It must beemphasised, however, that the hemiplegia of itselfdoes not show any striking characteristics oranything which would differentiate it from aclassical hemiplegia resulting from occlusion of themiddle cerebral artery.A fairly common mode of presentation is,
however, by remittent attacks of paresis, eitherhemiparetic or of a more limited range, and insome cases these have extended over a period ofyears. Usually there has been an abrupt onset ofparesis with or without sensory disturbances, last-ing a few days or weeks and followed by a con-siderable degree of recovery. In a very smallproportion of cases the disease has shown itself by amore gradually developing hemiplegia and in twoof the author's cases there was a striking andpredominant sensory disturbance of the arm andhand, slowly increasing over a period of weeks,and presenting a picture highly suggestive of acerebral tumour.
It will be seen that there is no one clinicalpicture characteristic of thrombosis of the internalcarotid artery. At one extreme the picture is thatof an abrupt and devastating hemiplegia differingin no way from classical hemiplegia; at the othera slowly increasing weakness with or withoutsensory loss, involving one side of the body or evenone limb, and simulating closely the picture of aninvasive cerebral tumour. Nevertheless there isone symptom which deserves close attention forthough on the whole rare, it is the sole symptomwhich when present enables the clinical diagnosisto be made with confidence. This is the occur-rence of transitory loss of vision in the eye on theside of the thrombosed vessel. It is not a commonsymptom even when close enquiry is made, thoughit must be admitted that in some cases its appear-ance may have been entirely forgotten by thepatient. These attacks of transitory blindness orclouding of vision may ante-date the onset of themore dramatic hemiparetic phenomena by weeks
B1
copyright. on A
ugust 1, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.32.365.122 on 1 M
arch 1956. Dow
nloaded from

124 POSTGRADUATE MEDICAL JOURNAL March 1956
:iner.:::: I :!'::::':'······"
::a.·r: ilil8i i··11·1:i
i. i*liiiilS I8!·i'i ::.I8H"..;6.·1-'r:2:r:xll-.''"sS.lg.8li. :B.
..: i.:i.?·?.araE,
ii :·i·;·i
i·i .i
:·P
····iil;
.FI .i.iir:·r·: ·i.i
ri;rlr::;::
r-l
pi.in:!piliiil.... liiiici:'· .iii.ih..;.i.
.i
:i I!HY·:::r: ii
:!:iiii iiil :In:'i.arl.paa.g .. I··ii.gp.. ''I':3 :· :::':P'::
i'!!.p· -·Li.: ' ·:':"
I1I. ;ij..*1·.
i·:i:i. ·s
;*i;· ·:.-··:·:.1,..11
li!li:;.sa"..:119.;iiilliir·i ;(:%·t:, ;·: ·k·
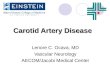
FIG. 2.-Radiograph from a case of occlusion of the internal carotid artery showing thecollateral circulation through the ophthalmic artery and filling of the terminal part of theinternal carotid. There is some filling of the middle cerebral and very good filling ofthe posterior cerebral artery.
or even by years. Its importance lies in the factthat it is indicative of a transitory ischaemia of theretina, and so far as our knowledge extends atpresent the only common cause of such a transitoryand repeated retinal ischaemia is obstruction in theipsilateral internal carotid artery. It is veryinteresting to observe that permanent loss orimpairment of vision in the ipsilateral eye (that is,the eye on the side of the thrombosed vessel),is extremely rare. Indeed at first it seemed as ifpermanent blindness never occurred, but largerexperience has shown that very occasionally thedegree of ischaemia is such that permanent retinaldegeneration and optic atrophy ensue. That thecirculation to the eye so frequently escapespermanent damage must depend on the veryadequate collateral circulation which is establishedby way of the external carotid, the facial artery andthe various ocular branches of the ophthalmicartery (Fig. 2).
POSTERIOR OPHTHALMICCEREBRAL ARTERY a ARTERY
Tracing of Fig. 2.
copyright. on A
ugust 1, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.32.365.122 on 1 M
arch 1956. Dow
nloaded from

March 1956 SMYrH: Thrombosis of the Internal Carotid Arteryv 25
The early reports of thrombosis of the internalcarotid artery contained reference to diminutionof the carotid pulse on the affected side, and it wassuggested that clinical evidence of the occlusionmight be afforded by noting a diminution orobliteration of the pulse, as indeed Ramsay Hunthad originally suggested. Whilst it is true thatthis may have been a valid observation it can bestated quite confidently that this procedure is ofvery little value and a moment's reflection willshow why this is so. The internal and externalcarotid arteries lie in such close proximity in theneck that occlusion of one can scarcely affect thetotal pulsation. In those few cases where a definitediminution of the pulse has been found it is indeedprobable that the common carotid artery wasoccluded.
DiagnosisNot much remains to be said under this heading
for the special features of the disease have beenoutlined in discussing the symptomatology. Itwill be apparent that in the great majority theclinical diagnosis is conjectural. When attacks ofuni-ocular amblyopia have preceded the hemi-plegia the diagnosis may be made with a highdegree of confidence but in other cases, and theyconstitute the great majority, ultimate confirma-tion depends on angiography with demonstrationof the actutal occlusion. It may be mentioned atthis stage that other ancillary modes of investiga-tion have J ot yielded information of decisive value.No characteristic picture is afforded by the electro-encephalog;ram and investigations of the cerebro-spinal flui l, both as regards hydrodynamics andchemistry do not show any constant deviation fromnormal.
it is not within the scope of this paper to deal inany detail with the purely radiological aspects of thesubject. P'rovided the radiological technique isadequate and correctly carried out the method isalmost infallible, though now and again even askilled and experienced radiologist may run intodifficulties. Sometimes instead of entering thelumen the contrast medium becomes arrested in themedia or in the sub-intimal space, producing whatis in effect a dissecting aneurysm. In such casesthe appe rances may be suggestive of an oblitera-tion of the lumen and consequently an incorrectdiagnosis of thrombosis made. An experiencedradiologist, however, will seldom be in any doubtas to the true state of affairs. The appearanceswhich may result from such a faulty injection of thecontrast medium are well shown in Fig. 3. Atthis point it may be well to give a word of cautionagainst too prolonged attempts at inserting theneedle into the carotid artery, or what is equally,
:. '',.:.
Vi
..!,i. ....
=== r ...1;!.......:i
-m:-1 XFIG. 3.-The contrast medium has passed into the sub-
intimal space and is elevating the intima.
if not more, important, repeating the attemptwithin a few days. The writer has seen severalcases where a repeated attempt at angiography,carried out about a week after the first, wasfollowed by sudden and severe extension ofcerebral damage. Whether this is brought aboutby dislodgement of clot from the site of the initialpuncture with consequent embolism, or byintense cerebral ischaemia, the result of cerebralarterial spasm, is by no means clear. Thepractical implication is, however, plain and ifangiography has failed for technical reasons then aperiod of at least ten days should be allowed toelapse before a further attempt is made.
TreatmentUp to the present the great majority of cases
have occurred in middle-aged and elderly patientsand this, coupled with the frequency of evidenceof more generalized cardiovascular disease haslimited treatment to such conservative measures aswould be proper to a cerebral thrombosis of theusual type. In other words treatment hasconsisted in general nursing care, in prevention ofpulmonary and genito-urinary complications andin early physiotherapy and mobilization. Indeedin those cases, and they form the largest group,which present with an abrupt hemiplegia, it isdifficult to see what else would avail, for cerebralsoftening must have already occurred with, as aninevitable consequence, some degree of permanentdisability. Where the symptoms have beenrelatively slight or remittent the neuro-surgeons
copyright. on A
ugust 1, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.32.365.122 on 1 M
arch 1956. Dow
nloaded from

126 POSTGRADUATE MEDICAL JOURNAL March 1956
have been tempted to employ more heroicmeasures. Stellate ganglionectomy and othermeasures designed to denervate the carotid vesselshave been tried, but the general consensus ofopinion remains sceptical. In a recent symposiumon cerebral vascular disease, Bucy (1955) hasexpressed the view that the value of such measuresremains quite unproved. Eastcott, Pickering andRob (I954), have recently reported some successfollowing resection of the thrombosed portion ofthe internal carotid artery but it is too early as yetto form any final opinion of the value of thismethod.
DiscussionAs so often happens the solution of one problem
or even the enlargement of one field of knowledgein a particular direction serves only to presentfurther difficulties and problems and to posefurther questions. In considering internal carotidthrombosis the fundamental question is why suchan occlusion should produce symptoms at all for,as is well known, the carotid vessels may be tied bythe surgeon with impunity. The incidence of anypermanent degree of hemiplegia following acarotid ligation is certainly not greater than5 per cent. It is clear then that in thrombosis ofthe internal carotid artery something more thanthe mere mechanical effect of occlusion has to bereckoned with. Consideration of this paradoxshould put us on our guard against the too readyacceptance of any purely mechanistic explanation.Preoccupation with the occlusion of the internalcarotid artery must not lead us to ignore the restof the cerebral circulation and, in particular, thestate of the carotid vessels on the opposite side andof the Circle of Willis. It is possible that cerebralsoftening following on occlusion of the internalcarotid artery occurs when there is insufficiencyof the circulation through the apparently intactcarotid vessels of the opposite side. Someconfirmation of this hypothesis is afforded by theobservation which has been made on severaloccasions of ischaemic softenings in both cerebralhemispheres in what was apparently a strictlyunilateral internal carotid thrombosis. In suchinstances it seems reasonable to suppose that therelatively intact carotid vessels were unable tomaintain an adequate circulation not only to theopposite cerebral hemisphere via the Circle ofWillis but to their own more particular territory.
In concluding this article it is pertinent to saysomething of the general indications for the
employment of angiography and more particularlyin cases of supposed or suspected thrombosis of theinternal carotid artery. Since in any given case itmay be impossible to decide whether a hemiplegiaof vascular origin is the result of occlusion withinthe middle cerebral artery or the internal carotidartery it would seem on theoretical grounds thatangiography might well be employed in all.Nevertheless despite the relative safety of theprocedure it is doubtful if it should be employedindiscriminately, for there is no doubt that everynow and then, even with the most careful tech-nique, unfortunate accidents happen. There is allthe greater danger of such accidents when dealingwith elderly patients suffering from advancedcardiovascular degeneration. In the author's viewthe method should not be used merely to satisfycuriosity but should be reserved for those caseswhere real doubt exists in the diagnosis and, aboveall, where there is the possibility of some othercondition possibly amenable to radical treatment.In this Centre we have more particularly tended touse angiography in those cases where the possi-bility of a cerebral tumour arose. We have beenloath to submit patients to angiography wherefrom the history it seemed perfectly plain thatthe disease was a vascular accident, always except-ing, of course, those cases where the presence ofintracranial haemorrhage, pain and the likesuggested the possibility of an intracranialaneurysm. It must not be forgotten that hemi-plegia of extremely sudden onset and withoutprior symptoms and without the occurrence ofheadache or alteration of consciousness is by nomeans a great rarity in young adults, and there isno doubt that in some of these cases the hemi-plegia is the consequence of a precocious primaryinternal carotid occlusion. Such attacks, therefore,in young people certainly merit the most carefulinvestigation and it would seem that cerebralangiography should form a necessary part in theirinvestigation.
BIBLIOGRAPHYBUCY, P. C. (I9S),' Cerebral Vascular Disease,' ed. Luckey, E. A.,New York.CLOAKE, P. C. P. (1951), 'Modem Trends in Neurology,' ed.
Feiling, A., London, 480.EASTCOTT, H. H. G., PICKERING, G. W. and ROB, C. G.
(I954), Lancet ii, 994.HUNT, J. R. (I914), Amer. J. Med. Sci., 147, 704.MONIZ, E., LIMA, A. and de LACERDA, R. (1937), Pr. Med.,45,977.HULTQVIST, G. T. (1942), 'Uber Thrombose u. Embolie derArteria carotis,' Stockholm.
copyright. on A
ugust 1, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.32.365.122 on 1 M
arch 1956. Dow
nloaded from