Embed Size (px)
Citation preview
Thrombosis and restenosis after stenting in failed angioplasty: Comparison with elective stenting
The results of Palmaz-Schatz stent implantation in failed angioplasty in 60 consecutive patients were compared with those of elective stent implantation in 100 consecutive patients. Stent implantation was successful in all of the failed group and in 99% of the elective. Stent thrombosis occurred in 16.7% of the failed group and 2% of the elective @ = 0.001). In the failed angioplasty group, stent thrombosis was associated with a greater frequency of preprocedure complex morphology (4OK vs 12% in the nonthrombosis group, p = O.O!i), persistent uncovered dissection after stenting (60% vs 14%, p = 0.004), and greater residual stenosis (39.9% f 25.3% vs 24.9% f 13.06%, p = 0.006) after stenting. Vessel patency was reestablished by angioplasty in 5 of 10 with stent thrombosis. Df these 5 patients, however, 2 suffered repeat stent thrombosis; 1 died suddenly four months later; and restenosis occurred in the remaining 2. Follow-up angiography was performed in 96% of the elective group at 6.3 + 2.6 months and 96% of the failed angioplasty group at 6.4 +- 2.1 months. Restenosis (~50% stenosis) occurred in 32% of the elective group and 60% of the failed angioplasty group (p = 0.041). Multiple logistic regression analysis identified multiple stent implantation (F = 6.75, p = 0.01) and triple-vessel disease (F = 3.46, p = 0.06) as independent positive predictors of restenosis. In conclusion, stent implantation in cases of failed angioplasty could be performed with a success similar to that of elective stent implantation but was associated with a greater frequency of stent thrombosis and restenosis. (AM HEART J 1994;128:12-20.)
J. Brendan Foley, MD, Robert I. G. Brown, MD, and Ian M. Penn, MB London, Ontario, Canada
Coronary artery dissection and inadequate primary dilatation are major predisposing factors to acute oc- clusion during and after coronary angioplasty.1-3 Acute occlusion occurs in 57% of angioplasty pro- cedures and is a result of the interaction among the occlusive properties of coronary artery dissection, thrombus formation, and vascular recoil.4-10 The res- toration of intimal continuity and vessel geometry by intracoronary stent implantation has been proposed as a means of reversing this adverse combination of events.11-15
The results of stent implantation after failed angi- oplasty are unclear. Many of the studies have been multicenter, with a relatively small number of proce- dures performed by a large number of operators.15T I6
From Victoria Hospital, University of Western Ontario.
Received for publication June 25, 1993; accepted Nov. 17, 1993.
Reprint requests: J. Brendan Foley, MD, Cardiac Catheterization Labora- tory, Victoria Hospital, Box 5375, London, Ontario N6A 4G5, Canada.
Copyright @ 1994 by Mosby-Year Book, Inc. oooz-8703/94/$3.00+0 4/l/64634
The results of more than one stent design have been combined in a single paper.17 Moreover, many inves- tigators have failed to differentiate between the results of elective stent implantation and those of stenting in cases of failed angioplasty.15* 16y l8 This heterogeneity makes data regarding a single stent design used in a single center by two operators in both elective and failed angioplasty of importance in helping to determine the role of stent implantation in failed angioplasty. The objective of this investigation was to compare the immediate and long-term safety and efficacy of stent implantation in elective and failed angioplasty performed at a single institution.
METHODS
Since January 1990 our policy has been to consider stent implantation in all cases of failed angioplasty before refer- ral for urgent bypass surgery. The stent used has been the articulated Palmaz-Schatz stent (Johnson & Johnson In- terventional Systems Co., Warren, N. J.).lg Between Jan- uary 1990 and August 1992, intracoronary stent implanta- tion in the setting of failed angioplasty was attempted in 60 patients, representing 5% of all angioplasty procedures
12

Volume 128, Number 1
American Heart Journal Foley, Brown. and Penn 13
over that period. This group consisted of patients who were undergoing angioplasty of a vessel visually estimated at 3 mm or more, who had been counseled before the angio- plasty, and who gave informed consent to stent implanta- tion in the event of failed angioplasty. These patients were compared with the first 100 patients in whom elective stent implantation was attempted at the same institution. Elec- tive stent implantation was performed after obtaining written informed consent for a study aimed to determine the immediate and long-term safety and efficacy of elective stenting. The contraindications to stent implantation in both settings are presented in Table I. Both study proto- cols were approved by the hospital ethics committee, and all data were prospectively collected.
Clinical and angiographic terms as defined in the study are outlined in Table II.20~22 “Failed angioplasty” was de- fined after an adequate trial of conventional balloon dila- tation (i.e., multiple inflations with a balloon-to-vessel ra- tio of 0.9 to l.l:l and a single inflation of at least 60 seconds). A definition of failed angioplasty is difficult; the nature of the patients in the failed angioplasty group was further characterized by the following features: the mean number of inflations before stent implantation was 6.0 f 3.4; the total inflation time was 16.2 + 13.4 minutes; the single longest inflation was 1.7 i 7.2 minutes; and pro- longed inflation with a perfusion balloon catheter (average maximum inflation 10.4 -t 6.6 minutes) was performed in :34 (56.7%).
Twelve-lead electrocardiograms were routinely per- formed before, immediately after, and the morning after the procedure. Creatine phosphokinase (CPK) was rou- tinely measured before, immediately after, 6 hours after, and 18 to 24 hours after the procedure. Additional electro- cardiograms and measurements of cardiac enzymes were performed as clinically indicated. Angiographic follow-up was planned in all patients 6 months after stent implanta- tion or sooner if clinically indicated.
Angiographic measurements. Computerized quantita- tive coronary angiographic analysis (Cardiovascular Mea- surement System, Medis, Nuenen, The Netherlands) was used to measure the reference vessel diameter, the per- centage diameter stenosis, and the minimal luminal diam- eter, before and immediately after the procedure.23* 24 With this system, the region of interest, which includes a segment of angiographically normal vessel proximal and distal to the stenosis, is defined. After identification of the beginning and end of the segment to be analyzed, the cen- ter line is automatically determined. The segment contour is computed with the weighted sum of the first and second derivative functions. The computer-generated estimation of the original vessel outline is used to determine the inter- polated reference vessel diameter. By using the guide catheter as a scaling device, absolute measurements in millimeters are determined. Lesion length is determined from the diameter function on the basis of curvature anal- ysis.
The angiographic view that demonstrated the maximum degree of stenosis was used for all measures of stenosis se- verity. After stent implantation, 3 seconds was allowed at
Table I. Contraindications to stent implantation
Contraindications to elective stent implantation Within 48 hours of an acute myocardial infarction Ostial lesion >30% left main stem stenosis if the target lesion was in the
left circulation Lesion length estimated to be >1.5 cm Angiographic features compatible with thrombus Diffuse disease and poor outflow of the target vessel Contraindications to long-term anticoagulation Patient enrollment in another study
Contraindications to stent implantation in failed angio- plastj
>30%# left main stem stenosis if the target lesron was in the left circulation
Diffuse disease and poor outflow of the target vessel Contraindications to long-term anticoagulation Angiographic features compatible with thrombus (relative
contraindication)
the beginning of each cineangiographic injection to facili- tate stent visualization. All angiographic assessments and measurements were performed by an independent cardiol- ogist experienced in angiographic analysis. The angio- graphic view that demonstrated the maximum stenosis was used for all measures of stenosis severity.
Our previous experience248 with this system of repeated analysis of a random sample of 35 angiograms of angio- plasty complicated by dissection yielded t.he following re- sults. Linear regression analysis for repeated measures of percentage stenosis, minimal luminal diameter, and dis- section length yielded R2 values of 0.78, 0.8, and 0.96, re- spectively. The agreement between readings of American College of Cardiology-American Heart Association (ACC/ AHA) classification (A or Bl, or B2 or Ci, Thrombolysis in Myocardial Infarction Study flow grade, presence or ab- sence of dissection, and dissection classification into sim- ple or complex was 85 % , 91% , loo%, and 85 “b , respec- tively, yielding Kendall’s rank correlation coefficient tau values of 0.79, 0.67, 1, and 0.64.
Procedure. All of the patients received aspirin 325 mg and three doses of dipyridamole 75 mg in the 24 hours be- fore the procedure. In the elective patients, administration of low-molecular-weight dextran 40 was commenced at 100 ml/hr 2 hours before the procedure. In the setting of failed angioplasty, dextran 40 administration was commenced in the cardiac catheterization laboratory, with 200 to 300 ml of dextran 40 rapidly infused before stent implantation.
After the procedure, the dextran 40 infusion was contin- ued at 50 ml/hr until at least 6 hours after removal of the arterial sheath, with a minimum of 1 L infused. Oral anti- coagulation with coumadin was commenced on the day of &ni impiantatlon. Anticoagulation with heparin to main- tain the partial thromboplastin time between 60 and 90 seconds was continued until the prothrombin time was >15 seconds, at which time heparin administration was discon- tinued and the patients discharged. This regimen was al-

14 Foley, Brown, and Penn
Table II. Definitions
July 1994 American Heart Journal
Clinical definitions Failed angioplasty
Unstable angina
Successful stent implantation
Acute stent thrombosis Subacute stent thrombosis Major complications
Minor complications
Q-wave myocardial infarction
Non-Q-wave myocardial infarction
Angiographic definitions Restenosis
Proximal lesion
Lesion character Dissection
Thrombus
(1) Angioplasty complicated by abrupt occlusion, i.e., TIM1 grade 0 or 1 flow in a vessel previously patent with TIM1 grade 2 or 3 Aow20 or (2) a residual steno- sis >50% with or without intimal dissection
(1) Crescendo pattern of angina to include an episode of rest pain; (2) angina at rest of >20 minutes in the absence of myocardial infarction; or (3) persistent postinfarction unstable angina
Stent delivery to the intended site with >20% reduction in the percentage diam- eter stenosis with a final residual stenosis <50 %, without major complications
Stent thrombosis within 24 hours of stent implantation Stent thrombosis between 24 hours and 1 month Death, Q-wave myocardial infarction, need for urgent bypass surgery, stent
thrombosis, bleeding complications that require cessation of anticoagulation or transfusion or surgery, or stent embolisation or stent deployment at a site dis- tant from that intended
Non-Q-wave infarctions and bleeding problems that do not require interruption in anticoagulation or surgical intervention
Development of pathologic Q waves in two or more contiguous leads, associated with a significant elevation in CPK (>230 U/L) and a positive MB isoenzyme (>13 U/L and 5% of total CPK).
Elevation in CPK with a positive MB isoenzyme, without the development of pathologic Q waves
250% Stenosis at or immediately adjacent to site of stent implantation at fol- low-up angiography
Lesion location before the first major diagonal in the left anterior descending ar- tery, before the origin of right ventricular branch in the right coronary artery, and before the first marginal branch in the circumflex coronary artery
According to modified ACCIAHA classification21 (1) No dissection; (2) simple dissection: grade 1A intraluminal filling defect, grade
1B extraluminal cap extravasation; and (3) complex dissection: grade 2A non- linear spiral defect, grade 2B luminal defect with multiple irregular borders, and grade 2C obstructive dissectio@
(1) A filling defect surrounded by contrast at site of high grade stenosis; (2) lu- minal staining at site of high-grade stenosis or total occlusion; or (3) upward convexity or irregularity without vessel tapering at site of an abrupt occlusion22
TIMI, Thrombolysis in Myocardial Infarction Study; CPK, creatine phosphokinase; ACC-AHA, American College of Cardiology-American Heart Associ- ation.
tered in the last 11 patients in the failed angioplasty group: anticoagulation with heparin was continued until the pro- thrombin time was >16 seconds; the heparin infusion was then reduced by half for an additional 6 hours, at which time it was discontinued if the prothrombin time was still >16 seconds; and the patients remained in hospital for an additional 12 to 24 hours. After discharge, the patients were maintained on coumadin; aspirin 325 mg once per day; dipyridamole 75 mg three times per day; a calcium antag- onist; and misoprostol 200 M twice per day for 1 month. Anticoagulation was continued to maintain the prothrom- bin time between 15 and 18 seconds; prothrombin time was checked at least twice per week by the patient’s family doctor.
Statistical analysis. Results are presented as means f SD. A value of p I 0.05 was considered statistically sig- nificant. Within-group comparisons of continuous vari- ables before and after the procedure were performed with two-tailed paired t tests. Comparisons between groups
were performed with unpaired two-tailed t tests, chi- squared tests, Fisher’s exact tests, and Wilcoxon rank sum tests where appropriate. Multivariate analysis by multiple logistic regression with stent thrombosis and restenosis as the dependent variables was performed to identify vari- ables independently related to outcome. Only those vari- ables significant at the p < 0.1 level on univariate analysis were entered into the logistic regression model. Data from patients who died, who suffered acute or subacute stent thrombosis that was not successfully reopened, or who went to bypass surgery were excluded from the restenosis analysis. Statistical analysis was performed with the Sta- tistical Analysis System (version 6.04, SAS Institute, Gary, N. C.).
RESULTS
Stents were successfully implanted in 99% of pa- tients undergoing elective stenting and in 100% of
Volume 128, Number 1
American Heart Journal Foley, Brown,. and Penn 15
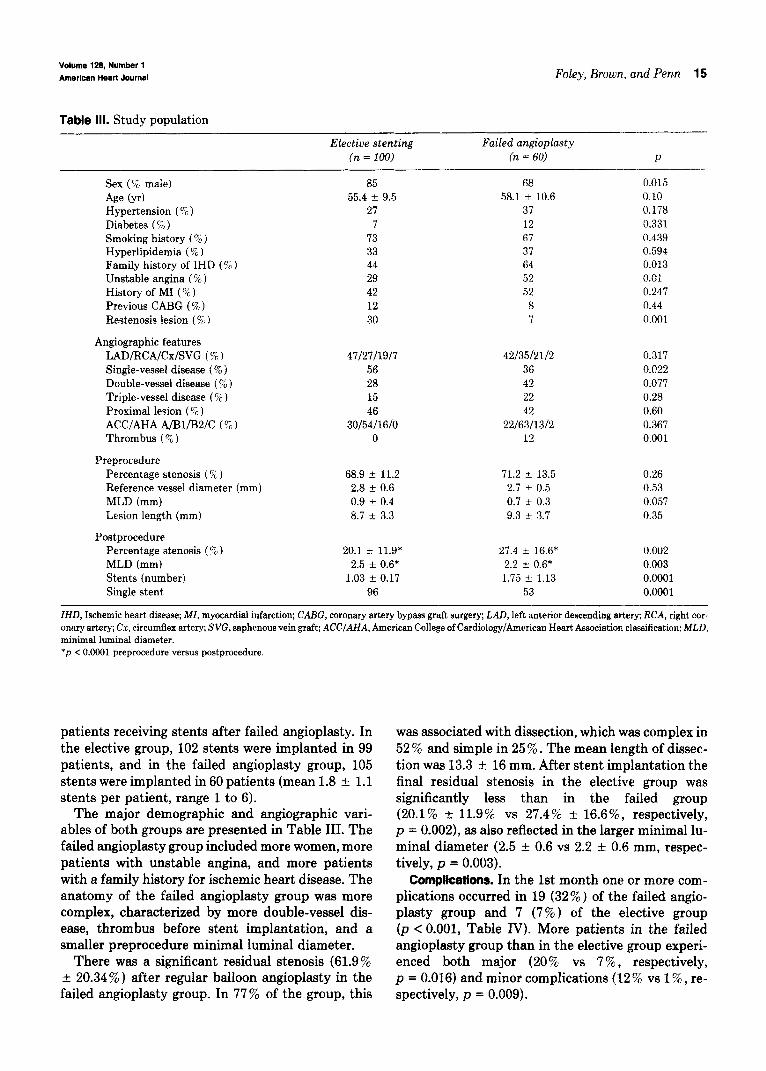
Table III. Study population
Elective stenting Failed angioplasty (n = 100) (n = 60) P
Sex (% male)
Age (yr) Hypertension (“T’ ) Diabetes (“;) / Smoking history ( % ) Hyperlipidemia (% ) Family history of IHD (% ) Unstable angina (%) History of MI (% ) Previous CABG (% ) Restenosis lesion ( % )
Angiographic features LAD/RCA/Cx/SVG (% ) Single-vessel disease (%) Double-vessel disease (%) Triple-vessel disease (% ) Proximal lesion (% ) ACC/AHA A/Bl/BS/C (% ) Thrombus ( $ )
Preprocedure Percentage stenosis ( % ) Reference vessel diameter (mm) MLD (mm) Lesion length (mm)
Postprocedure Percentage stenosis (% ) MLD (mm) Stents (number) Single stent
85 55.4 f 9.5
27
73 33 44 29 42 12 30
4712711917 42/35/21/2 0.317 56 36 0.022 28 42 0.077 15 22 0.28 46 42 0.60
30/54/16/0 22/63/13/2 0.367 0 12 0.001
68.9 + 11.2 71.2 + 13.5 0.26 2.8 + 0.6 2.7 rf- 0.5 0.53 0.9 + 0.4 0.7 k 0.3 0.057 8.7 rt 3.3 9.3 + 3.7 0.35
20.1 f 11.9* 27.4 f 16.6* 0.002 2.5 + 0.6* 2.2 e 0.6* 0.003
1.03 f 0.17 1.75 i 1.13 0.0001 96 53 0.0901
68 58.1 I!I 10.6
37 12 67 37 64 52 52
8
0.015 0.10 0.178 0.331 0.439 0.594 0.013 0.01 0.247 0.44 0.001
IHD, Ischemic heart disease; MI, myocardial infarction; CABG, coronary artery bypass graft surgery; LAD, left anterior descending artery; RCA, right cor- onary artery; Cx, circumflex artery; SW, saphenous vein graft; ACCIAHA, American College of Cardiology/American Heart Association classitication; MLD, minimal luminal diameter. *p < 0.0001 preprocedure versus postprocedure.
patients receiving stents after failed angioplasty. In the elective group, 102 stents were implanted in 99 patients, and in the failed angioplasty group, 105 stents were implanted in 60 patients (mean 1.8 +- 1.1
stents per patient, range 1 to 6). The major demographic and angiographic vari-
ables of both groups are presented in Table III. The failed angioplasty group included more women, more patients with unstable angina, and more patients with a family history for ischemic heart disease. The anatomy of the failed angioplasty group was more complex, characterized by more double-vessel dis- ease, thrombus before stent implantation, and a smaller preprocedure minimal luminal diameter.
There was a significant residual stenosis (61.9% r 20.34% ) after regular balloon angioplasty in the failed angioplasty group. In 77% of the group, this
was associated with dissection, which was complex in 52 % and simple in 25 % . The mean length of dissec- tion was 13.3 + 16 mm. After stent implantation the final residual stenosis in the elective group was significantly less than in the failed group (20.1% + 11.9% vs 27.4% +- 16.6%) respectively, p = O-002), as also reflected in the larger minimal lu- minal diameter (2.5 f 0.6 vs 2.2 it 0.6 mm, respec- tively, p = 0.003).
Compkations. In the 1st month one or more com- plications occurred in 19 (32%) of the failed angio- plasty group and 7 (7%) of the elective group (p < 0.001, Table IV). More patients in the failed angioplasty group than in the elective group experi- enced both major (20 % vs 7 % , respectively, p = 0.016) and minor complications (12 % vs 1% , re- spectively, p = 0.009).
16 Foley, Brown, and Penn July 1994
American Heart Journal
i Stent Thrombosis /
I I reopened reopened
I I
CABG (n-1) (no MI)
no MI non-Q MI
I
reopened (n=l) (non-Q MI)
unable to maintain patency (n=l) (Q-wave MI)
subacute
1 ! thrombosis
n-7
‘\ unable to reopen (n=2)
CABG (n=i)
(1 non-Q MI) (non-0 MI)
(1 no MI) I
reopened tn.41 (2 non-0 MI) (2 Q-wave MI)
reocclude (n=2)
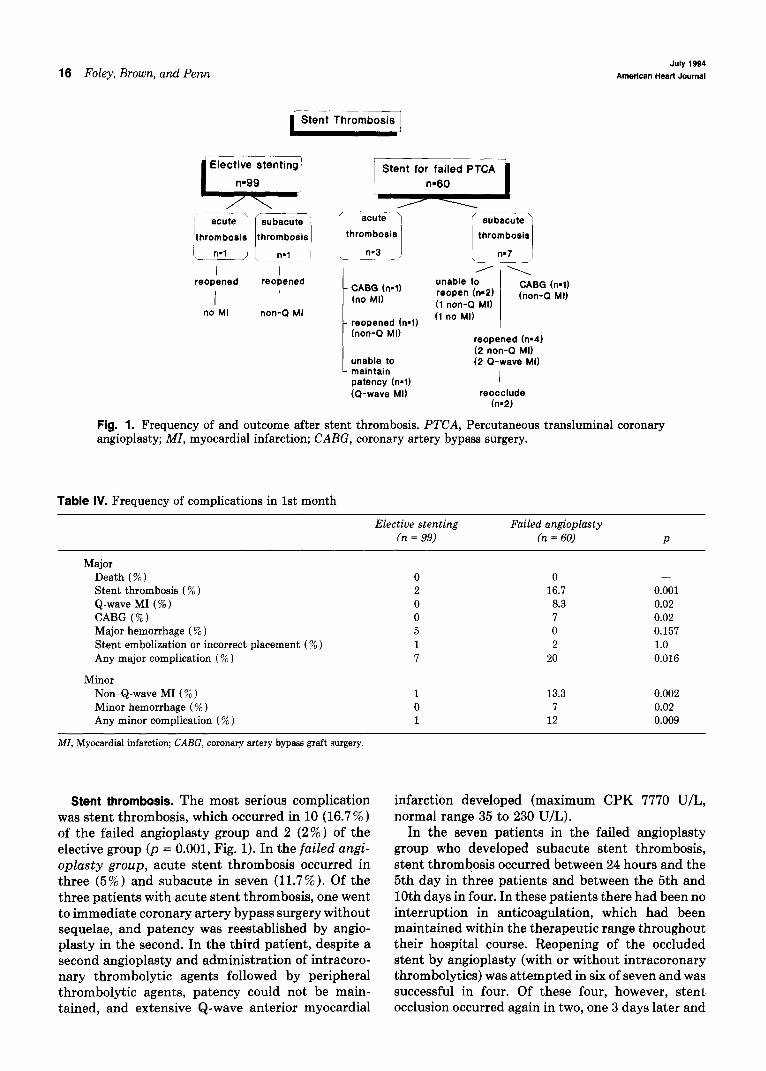
Fig. 1. Frequency of and outcome after stent thrombosis. PTCA, Percutaneous transluminal coronary angioplasty; MI, myocardial infarction; CABG, coronary artery bypass surgery.
Table IV. Frequency of complications in 1st month
Elective stenting Failed angioplasty fn = 99) (n = 60) P
Major Death (% ) 0 0 - Stent thrombosis (%) 2 16.7 0.001 Q-wave MI (%) 0 8.3 0.02 CABG (%) 0 7 0.02 Major hemorrhage (%) 5 0 0.157 Stent embolization or incorrect placement (% ) 1 2 1.0 Any major complication (% ) 7 20 0.016
Minor Non-Q-wave MI (% ) 1 13.3 0.002 Minor hemorrhage (%) 0 7 0.02 Any minor complication (%) 1 12 0.009
MI, Myocardial infarction; CAEG, coronary artery bypass graft surgery.
Stent thrombosis. The most serious complication was stent thrombosis, which occurred in 10 (16.7 % ) of the failed angioplasty group and 2 (2%) of the elective group lp = 0.001, Fig. 1). In the failed angi- oplasty group, acute stent thrombosis occurred in three (5%) and subacute in seven (11.7 %). Of the three patients with acute stent thrombosis, one went to immediate coronary artery bypass surgery without sequelae, and patency was reestablished by angio- plasty in the second. In the third patient, despite a second angioplasty and administration of intracoro- nary thrombolytic agents followed by peripheral thrombolytic agents, patency could not be main- tained, and extensive Q-wave anterior myocardial
infarction developed (maximum CPK 7770 U/L, normal range 35 to 230 U/L).
In the seven patients in the failed angioplasty group who developed subacute stent thrombosis, stent thrombosis occurred between 24 hours and the 5th day in three patients and between the 5th and 10th days in four. In these patients there had been no interruption in anticoagulation, which had been maintained within the therapeutic range throughout their hospital course. Reopening of the occluded stent by angioplasty (with or without intracoronary thrombolytics) was attempted in six of seven and was successful in four. Of these four, however, stent occlusion occurred again in two, one 3 days later and
Volume 128, Number 1
Am&cm Heart Journal Foley, Brown, and Penn 17
Percent of Population
100
90
60
60 1 I/ Elective q - Pre
L.-J 0 - Poet n - Follow-up
Failed PTCA
l -Pre l-----l l - Poet L - Follow-up
Percent stenosis
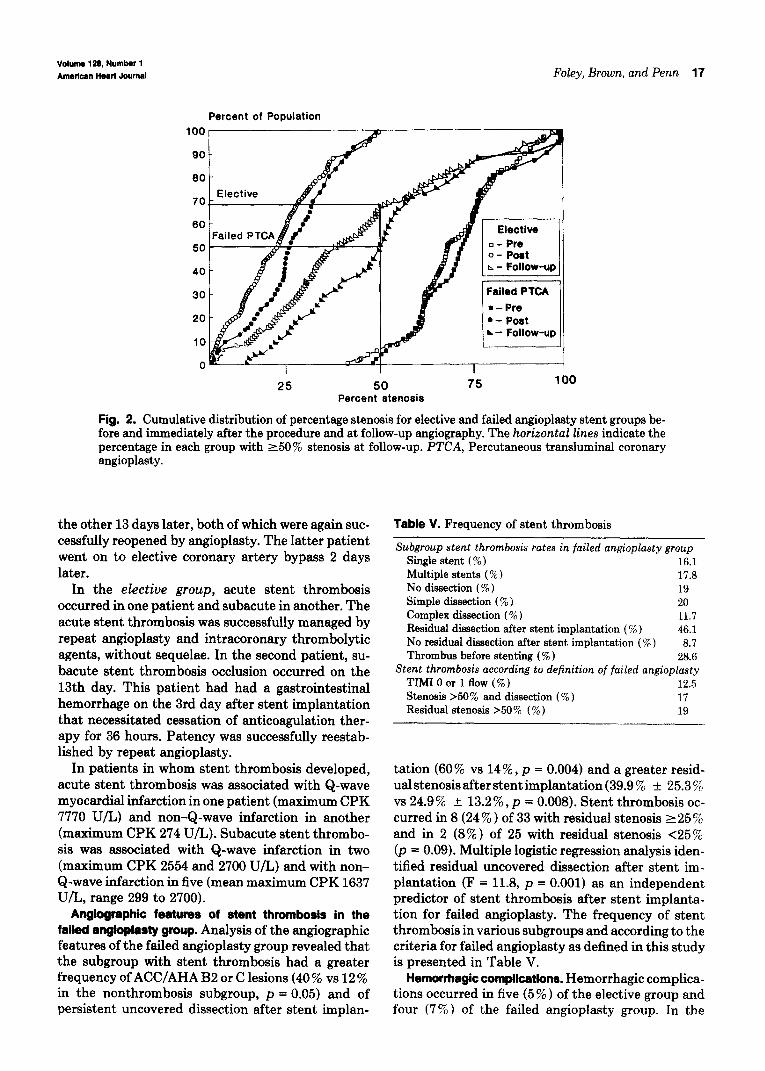
Fig. 2. Cumulative distribution of percentage stenosis for elective and failed angioplasty stent groups be- fore and immediately after the procedure and at follow-up angiography. The horizontal lines indicate the percentage in each group with 250% stenosis at follow-up. PTCA, Percutaneous transluminal coronary angioplasty.
the other 13 days later, both of which were again suc- cessfully reopened by angioplasty. The latter patient went on to elective coronary artery bypass 2 days later.
In the elective group, acute stent thrombosis occurred in one patient and subacute in another. The acute stent thrombosis was successfully managed by repeat angioplasty and intracoronary thrombolytic agents, without sequelae. In the second patient, su- bacute stent thrombosis occlusion occurred on the 13th day. This patient had had a gastrointestinal hemorrhage on the 3rd day after stent implantation that necessitated cessation of anticoagulation ther- apy for 36 hours. Patency was successfully reestab- lished by repeat angioplasty.
In patients in whom stent thrombosis developed, acute stent thrombosis was associated with Q-wave myocardial infarction in one patient (maximum CPK 7770 U/L) and non-Q-wave infarction in another (maximum CPK 274 U/L). Subacute stent thrombo- sis was associated with Q-wave infarction in two (maximum CPK 2554 and 2700 U/L) and with non- Q-wave infarction in five (mean maximum CPK 1637 U/L, range 299 to 2700).
Angiogfaphic features of stent thrombosis in the failed angiopksty group. Analysis of the angiographic features of the failed angioplasty group revealed that the subgroup with stent thrombosis had a greater frequency of ACC/AHA B2 or C lesions (40 % vs 12 % in the nonthrombosis subgroup, p = 0.05) and of persistent uncovered dissection after stent implan-
table V. Frequency of stent thrombosis
Subgroup stent thrombosis rates in failed angioplasty group Single stent ( % ) 16.1 Multiple stents ( % ) 17.8 No dissection ( % ) 19 Simple dissection ( % ) 20 Complex dissection ( % ) 11.7 Residual dissection after stent implantation (%) 46.1 No residual dissection after stent implantation ( W ) 8.7 Thrombus before stenting (% ) 28.6
Stent thrombosis according to definition of failed angioplasty TIMIOor lflow (%) 12.5 Stenosis >50% and dissection ( % ) 17 Residual stenosis >50 % (%) 19
--
tation (60% vs 14%) p = 0.004) and a greater resid- ual stenosis after stent implantation (39.9 % f 25.3 % vs 24.9% f 13.2%) p = 0.008). Stent thrombosis oc- curred in 8 (24 % ) of 33 with residual stenosis 225 % and in 2 (8% ) of 25 with residual stenosis <25% (p = 0.09). Multiple logistic regression analysis iden- tified residual uncovered dissection after stent im- plantation (F = 11.8, p = 0.001) as an independent predictor of stent thrombosis after stent implanta- tion for failed angioplasty. The frequency of stent thrombosis in various subgroups and according to the criteria for failed angioplasty as defined in this study is presented in Table V.
Hemorrhagic complications. Hemorrhagic complica- tions occurred in five (5 % ) of the elective group and four (7%) of the failed angioplasty group. In the
July 1994
18 Foley, Brown, and Penn American Heart Journal
elective group, gastrointestinal hemorrhage occurred in three patients; all three necessitated cessation of anticoagulation, and two required transfusion. Arte- rial puncture-site hematomas requiring surgical in- tervention occurred in three patients. One patient suffered both a gastrointestinal hemorrhage and an arterial puncture-site hematoma. In the failed angi- oplasty group, one patient suffered a minor gas- trointestinal hemorrhage that did not require cessa- tion of anticoagulation therapy or transfusion, and three developed arterial puncture-site hematomas with pseudoaneurysm formation. One of these closed spontaneously, and the other two were closed with graded Doppler ultrasound-guided external com- pression.
Death. One patient in the failed angioplasty group died during the follow-up period. This patient had had long-standing occlusions of the proximal right coronary and left anterior descending coronary ar- teries and a patent saphenous vein graft to the first marginal branch of the circumflex artery. Three stents were implanted in his native circumflex coro- nary artery for a 34-mm-long complex dissection. Stent thrombosis developed 7 days after the proce- dure and was successfully reopened by angioplasty, but the patient died suddenly out of the hospital 4 months later.
Restenosis. Angiographic follow-up was performed in 97 (98%) of 99 of the elective group 6.3 + 2.6 months after stent implantation and in 50 (96%) of 52 of eligible patients in the failed angioplasty group at 6.4 + 2.1 months. The remaining patients in the failed angioplasty group were not eligible for contin- ued study for the following reasons: three had docu- mented stent thrombosis that was not reopened; four had gone to bypass surgery; and one died 4 months after stent implantation. Two patients in both groups who were asymptomatic were unwilling to undergo follow-up coronary angiography. The restenosis rate in the failed angioplasty group was significantly higher than in the elective group, at 25 (50 % ) of 50 versus 32 (32.9%) of 97, respectively (p = 0.041; Fig. 2). A repeat angioplasty was successful in 26 of 27 at- tempted in the elective group and in all 18 attempted in the failed group and was not associated with any complications. The remainder of the patients, except for two in the failed group, had minimal or no symp- toms and were treated medically. The remaining two patients had coronary artery bypass performed be- cause of stent restenosis associated with progression of disease in nonstented areas.
In the restenosis group, the patients tended to be older (58.5 f 10.1 vs 55.4 + 10.1 years, p = 0.0741, had a greater frequency of triple-vessel disease
(26.8% vs 12.5%) p = 0.03); and had a greater num- ber of stents per patient (1.38 + 0.73 vs 1.14 + 0.58, p = 0.045). In the failed angioplasty group, resteno- sis occurred in 56 % of those with multiple stents and in 44% of those with single stents (p = 0.156). Res- tenosis occurred in four of five patients in whom stent thrombosis was successfully treated by angioplasty with or without thrombolytic agents, and the fifth patient died suddenly 4 months after the procedure. For the study population as a whole, multiple logis- tic regression analysis identified multiple stent im- plantation (F = 6.75, p = 0.01) and triple-vessel dis- ease (F = 3.46, p = 0.06) as independent positive predictors of restenosis. Six months after stent im- plantation, 61.9% of the elective group and 41.4% of the failed group were free of either major complica- tions or restenosis (p = 0.013).
DISCUSSION
Our results highlight the marked differences in the immediate and long-term efficacy of stent implanta- tion in elective and failed angioplasty. This impor- tant feature has not been emphasized previously. The literature to date has been clouded by analysis of only small numbers of cases and by the combination of the results of stent implantation in failed angioplasty with those of elective stenting.12* 13p 15s 161 l8 Herrmann et a1.25 reported a stent thrombosis rate of 16 % after implantation of the Palmaz-Schatz stent in cases of failed angioplasty. Their multicenter experience of unplanned or nonelective Palmaz-Schatz stent im- plantation in the United States over a 31-month pe- riod is similar to ours, which comes from a single center, with stents implanted by one of two primary operators. Similar results for stent implantation in failed angioplasty were reported by Lincoff et al. for the Gianturco-Roubin stent (Cook, Inc., Blooming- ton, Ind.) with an in-hospital stent reocclusion rate of 13 % 2s; however, a lower rate, 9 (7.6% ) of 115, for the same stent was reported by Roubin et a1.14
Our results demonstrate that stent thrombosis in cases of failed angioplasty is associated with greater residual stenosis after stent implantation and with failure to cover all of the dissection. Meticulous attention to detail, to ensure that all of the dissection is covered and that the residual stenosis is minimized, is critically important in reducing the potential for stent thrombosis. Accurate positioning of the Pal- maz-Schatz stent in failed angioplasty is often made more difficult when impaired flow and coronary artery dissection obscure the angiographic land- marks within the vessel. This difficulty is com- pounded by the radiolucent character of the stent and is complicated further if more than one stent is

Volume 128, Number 1 American Heart Journal Foley, Brown, and Penn 19
to be implanted. These complicating features high- light the importance of training those planning to implant stents, especially in the difficult scenario of failed angioplasty.
Our results, from a single center and including only stents implanted by one of two primary operators, emphasize the differences between elective and failed angioplasty stent implantation. Our data reflect the experience of stent implantation in cases of failed angioplasty from the inception of our stent program to our current state of knowledge. During this time, all patients with a vessel visually estimated at ~3 mm, in whom angioplasty had failed, were considered as candidates for stent implantation. The diameter of the vessels when measured by computerized quanti- tative coronary angiography was <3 mm: 2.8 + 0.6 mm in the elective group and 2.7 + 0.5 mm in the failed angioplasty group. This is more a reflection of the inaccuracy of visual estimation of reference ves- sel diameter than an indicator of an intention to stent smaller vessels. In contrast to others, however, we did not find that vessel diameter was a predictor either of stent thrombosis or of restenosis.27 Details of the mode of measurement of reference vessel diameter are not presented by that group. Our practice now is to consider stent implantation for failed angioplasty in vessels in which the operator is comfortable inflating a 3-mm balloon.
In our population neither lesion length nor length of dissection was a contraindication to stent implan- tation in failed angioplasty. This important feature is further emphasized by the finding that 47% of the failed angioplasty group required more than one stent to cover the target segment of coronary artery completely. Thus, the need for multiple stent im- plantation is a reflection of the length of the dissec- Cons to be treated. This is in contrast to the experi- ence of Herrmann et al., in which only 20% of the group received more than one Palmaz-gchatz stent,25 and the experience of Roubin et al. and Lincoff et al., in which 10 80 and 8%, respectively, received more than one Gianturco-Roubin stent.14s 26 In our experi- ence, the stent thrombosis rate was similar in those with single (16.1%) and multiple stents (17.8%); however, multiple stent implantation was identified by multiple logistic regression analysis to be the strongest predictor of restenosis.
subset of patients, either acutely at the time of stent thrombosis or as a planned procedure soon after the stent has been reopened. From a theoretical point of view, the high frequency of restenosis is this small group of patients highlights the potential role of thrombus as an initiator or promoter of restenosis after stent implantation.
The combination of our high angiographic fol- low-up rate (>95% in both groups) and the use of computerized quantitative coronary angiography provides us with insight into the frequency of rest- enosis after elective and failed angioplasty stent implantation. The restenosis rate that we have en- countered for elective stent implantation, 32%) is similar to that reported for balloon angioplasty,28* 2y and our restenosis rate in failed angioplasty was 50 % . Restenosis is not eliminated by stent implantation, but until the results of randomized trials of stent im- plantation versus balloon angioplasty in the elective and failed angioplasty settings are available, the role of stent implantation in restenosis will remain un- clear.
In conclusion, we have found that the Palmaz- Schatz stent could be implanted in cases of failed angioplasty with a success rate similar to that of elective stent implantation. However, stent implan- tation in failed angioplasty was associated with an increased frequency of stent thrombosis and a higher restenosis rate. Thus although stent implantation provided an efficient means of rescue in failed angi- oplasty, until the problem of stent thrombosis is re- solved, it may need to be considered a bridge to by- pass surgery in certain patients.
We thank Nancy Murray-Parsons, RN, and Joanne White, RN, for assistance in data collection, and the members of the cardiac catheterization laboratory, the cardiac ward, and the film library for their assistance and cooperation.
In our series, five patients in the failed angioplasty group developed stent thrombosis that was success- fully reopened by angioplasty techniques. Two went on to experience reocclusion; one died 4 months later; and restenosis occurred in the other two. From a practical point of view, these findings lead one to consider the option of coronary bypass surgery in this
REFERENCES
1. Detre KM, Holmes DR, Holubkov R, Cowley MJ, Bourassa MG, Faxon DP, Dorros GR, Bentivoglio LG, Kent K, Mvler R. Incidence and consequences of periprocedural occlusion: the 1985-1986 National Heart, Lung, and Blood Institute Percu- taneous Transluminal Coronary Angioplast y Registry. Circu- lation 1990;82:739-50.
2. Black AJR, Namay DL, Niederman AL, Lembo NJ, Roubin GS, Douglas JS, King SB. Tear or dissection after coronary angioplasty: Morphologic correlates of an ischemic complica- tion. Circulation 1989;79:1035-42.
3. Waller BF, Orr CM, Pinkerton CA, Van Tassel J, Peters T, Slack J. Coronary balloon angioplasty dissections: “The good the bad and the ugly.” J Am Co11 Cardiol 1992:20:701-6.
4. Leimgruber PP, Roubin GS, Anderson HV, Bredlau CE, Whitworth HB, Douglas JS. Kine SB. Greuntzie AR. Influence of intimal dissection on rester&is after successful coronary angioplasty. Circulation 1985;72:530-5.
5. Rowe MH, Hinohara T, White NW, Robertson GC, Selmon MR, Simpson dB. Comparison of dissection rates and angio-
20 Foley, Brown, and Penn July 1994
American Heart Journal
graphic results following directional coronary atherectomy and coronary angioplasty. Am J Cardiol 1990;66:49-53.
6. Ellis SG, Bates ER, Schaible T, Harlan FW, Pitt B, Top01 E.
ley S, Buchbinder M, Top01 EJ, Schatz RA. Restenosis after placement of the Palmaz-Schatz stent in native coronary ar- teries. Circulation 1992;86:1836-44.
Prospects for the use of the platelet glycoprotein IIb/IIIa re- 20. Chesebro JH, Knatterud G, Roberts R, Borer J, Cohen LS, ceptor to prevent postangioplasty restenosis and thrombosis. Dalen J, Dodge HT, Francis CK, Hillis D, Ludbrook P, Markis J Am Co11 Cardiol 1991;17:89B-95B. JE, Mueller H, Passamani ER, Powers ER, Rao AK, Robert-
7. Schwartz L, Bourassa MG, Lesperance J, Aldridge HF, Kazim son T, Ross A, Ryan TJ, Sobel BE, Willerson J, Williams DO, F, Salvatori VA, Henderson M, Bonan R, David P. Aspirin and Zaret BL, Braunwald E. Thrombolysis in Myocardial Infarc- dipyridamole in the prevention of restenosis after percutane- tion Trail, Phase I: a comparison between intravenous tissue ous transluminal coronary angioplasty. N Engl J Med 1988; plasminogen activator and intravenous streptokinase. Circu- 3181717-9. lation 1987;76:142-54.
8. Rensig BJ, Hermans WR, Strauss BH, Serruys PW. Regional differences in elastic recoil after percutaneous transluminal coronary angioplasty: a quantitative angiographic study. J Am Co11 Cardiol 1991;17:34B-8B.
9. Fischell TA, Derby G, Tse TM, Stadius ML. Coronary artery vasoconstriction routinely occurs after percutaneous translu- minal coronary angioplasty. Circulation 1988;78:1323-34,
10. de Feyter PJ, van den Brand M, Jaarman G, van Domburg R, Serruys PW, Suryapranata H. Acute coronary occlusion dur- ing and after percutaneous transluminal coronary angioplasty. Circulation 1991;83:927-36.
21. Ellis SG, Vandormeal MG, Cowley MJ, DiSciascio G, Deli- gonul U, Top01 E, Bulle TM, the Multivessel Angioplasty Prognosis Study Group. Coronary morphology and clinical determinants of procedural outcome with angioplasty for multivessel coronary disease. Circulation 1990;82:1193-202.
22. Freeman MR, Williams AE, Chisholm RJ, Armstrong PW. Intracoronary thrombus and complex morphology in unstable angina. Circulation 1989;80:17-23.
11. Ellis SG, Top01 EJ. Intracoronary stents: will they fulfil their promise as an adjunct to angioplasty? J Am Co11 Cardiol1989; 13:1425-30.
12. Sigwart U, Puel J, Mirkovitch V, Joffre F, Kappenberger L. Intravascular stents to prevent occlusion and restenosis after transluminal angioplasty. N Engl J Med 1987;316:701-6.
13. Sigward U, Urban P, Golf S, Kaufmann U, Imbert C, Fischer A, Kappenberger L. Emergency stenting for acute occlusion after coronary balloonangioplasty. Circulation 1988;78:1121-7.
14. Roubin GS, Cannon AD, Agrawal SK, Macander PJ, Dean LS, Baxley WA, Breland J. Intracoronary stenting for acute and threatened closure complicating percutaneous transluminal coronary angioplasty. Circulation 1992;85:916-27.
15. Fischman D, Savage M, Leon M, Schatz R, Ellis S, Cleman M, Teirstein P, Walker C, Bailey S, Hirshfeld JW, Goldberg S. Effect of intracoronary stenting on intimal dissection after balloon angioplasty: results of quantitative and qualitative coronary analysis. J Am Co11 Cardiol 1991;18:1445-51.
16. Serruys PW, Strauss B, Beatt KJ, Bertrand ME, Puel J, Rickards AF, Meier B, Goy JJ, Vogt P, Kappenberger L, Sig- wart U. Angiographic follow-up after placement of a self-ex- panding coronary artery stent. N Engl J Med 1991;324:13-7.
17. Ver Lee PN, Muller DW, Popma JJ, Ellis S, Top01 EJ. A com- parison of clinical and quantitative angiographic outcomes of coronary stenting in elective and emergency settings: a single center experience. Coronary Artery Dis 1991;2:945-51.
18. Colombo A, Maiello L, Thomas J, Zerboni S, Di Summa M, Finci L. Coronary stenting: single institution experience with the initial 100 cases using the Palmas-Schatz stent. Cath Car- diovasc Diagn 1992;26:1?1-6.
19. Ellis SG, Savage M, Fischman D, Bairn D, Leon M, Goldberg S, Hirshfeld JW, Cleman MW, Teirstein PS, Walker C, Bai-
23. Reiber JHC, Serruys PW, Kooijman CJ, Wijns W, Slager CJ, Gerbrands JJ, Schuurbiers JCH, den Boer A, Hugenholtz PG. Assessment of short-, medium-, and long-term variations in arterial dimensions from computer-assisted quantitation of coronary cineangiograms. Circulation 1985;71:280-8.
24. Zwet PMJ, van der Pinto IMF, Serruys PW, Reiber JHC. A new approach for the automated definition of path lines in digitized coronary angiograms. Int J Cardiac Imaging 1990; 5:75-83.
24a. Foley TB, Sridhar K, Dawdy J, Konstantinou C, Brown RIG, Penn I. Pros and cons of perfusion balloons in failed an- gioplasty. Cathet Cardiovasc Diagn 1994;31:264-9.
25. Herrmann HC, Buchbinder M, Clemen MW, Fischman D, Goldberg S, Leon MB, Schatz RA, Tiersteun P, Walker CM, Hirshfeld JW. Emergent use of balloon-expandable coronary artery stenting for failed percutaneous transluminal coronary angioplasty. Circulation 1992;86:812-9.
26. Lincoff AM, Top01 EJ, Chapejis AT, George BS, Candela RJ, Muller DW, Zimmerman CA, Ellis SG. Intracoronary stenting compared with conventional therapy for abrupt vessel closure complicating coronary angioplasty: a matched case-control study. J Am Co11 Cardiol 1993;21:866-75.
27. Agrawal SK, Hearn JA, Liu MW, Cannon AD, Bilodeau L, Iyer SS, Baxley WA, Dean LS, Roubin GS. Stent thrombosis and ischemic complications following coronary artery stenting. [Abstract]. Circulation 1992;86:1-113.
28. Bairti I, Roy L, Meyer F. Double-blind, randomized, con- trolled trial of fish oil supplements in prevention of recurrence of stenosis after coronary angioplasty. Circulation 1992;85: 950-6.
29. MERCATOR Study Group. Does the new angiotensin con- verting enzyme inhibitor cilaxapril prevent restenosis after percutaneous transluminal coronary angioplasty? Circulation 1992;86:100-10.





























