Embed Size (px)
Citation preview

Thromboprophylaxis and other
peri-operative issues
Alison Street
Malaysia April 2010

Peri-Operative Medicine
• An emerging specialty?!
• Management of co-morbidities and the particular issues of
- medication continuity
- thromboprophylaxis
- blood products
- discharge planning
As involves the Haematologist

Outline
• Bridging Anticoagulation
• Assessment of the risks and benefits of continuing or discontinuing anti-platelet agents
• Reversal of oral anticoagulants
• Thromboprophylaxis in surgical, medical and cancer patients
• Strategies for implementation and audit of hospital-wide systems

Perioperative Anticoagulation
• Requires consideration of the clinical consequences of
– risks of thromboembolism
– risks of anticoagulant therapy/bleeding
• VTE has estimated permanent death or disability rate in 5% of patients
• Arterial thromboembolism results in death or major disability in 70% patients
• Mitral Valve thrombosis is fatal in 15% pts
• Post operative bleeding has a fatality rate of 3% (Spyropoulos et al 2005)

REFERENCE
CHEST/133/6/ June, 2008 Supplement
[1]
Prevention of Venous Thromboembolism.
ACCP Evidence-Based Clinical Practice
Guidelines (8th edition)

Underlying values and
preferences
In patients at high and moderate risk of cardio-vascular and venous thrombo-embolic events, the recommendations reflect a relatively high value on prevention of adverse thrombotic events
In patients at low risk they reflect a relatively high value on the prevention of bleeding

Bridging anticoagulation

How to Bridge, a classic approach
• Withhold OAC for 5 days prior to procedure
• Administer heparin/LMWH beginning as INR falls (usually 1-2 days) prior to the procedure. Intensity depends on clinical “preference”
• Cease IV UFH 6 hours prior / sc LMWH 24 hours prior to procedure
• OAC could be restarted within 12-24 hours of end of procedure if there is no excessive bleeding; IV heparin is usually started without bolus (often at thromboprophylactic doses) with surgeon’s approval
• LMWH has advantage in that it
– Allows for home administration
– Reduced incidence of HITS
– Reduced hospital costs


LMWH or UFH?
• No evidence to recommend UFH or LMWH over the other for bridging therapy
• Kovacs et al Circulation 2004 – prospective multi-centre cohort study of 224 pts at high risk of arterial embolism on warfarin bridged with LMWH
– 8 pts (3.6%) episodes of thromboembolism;
– 15 (6.7%) episodes of major bleeding – 8 intraoperatively or early postoperatively before LMWH was restarted;
– no deaths
– Conclusion – bridging with LMWH feasible

There are many other approaches
• Use of low-dose Vitamin K replacement
• Use of Prothrombin Complex
Concentrates
• What is the role in bridging therapy of new
oral anticoagulants?
These all need further study

3.0 Perioperative Management of Patients Who Are Receiving Bridging Anticoagulation
3.1 In patients who require temporary interruption of VKAs and are to receive bridging anticoagulation, from a cost-containment perspective we recommend the use of SC LMWH administered in an outpatient setting where feasible instead of inpatient administration of IV UFH (Grade 1C).
• Underlying values and preferences: This recommendation reflects a consideration not only of the trade-off between the advantages and disadvantages of SC LMWH and IV UFH as reflected in their effects on clinical outcomes (LMWH at least as good, possibly better), but also the implications in terms of resource use (costs) in a representative group of countries (substantially less resource use with LMWH).
3.2 In patients who are receiving bridging anticoagulation with therapeutic-dose SC LMWH, we recommend administering the last dose of LMWH 24 h before surgery or a procedure over administering LMWH closer to surgery (Grade 1C); for the last preoperative dose of LMWH, we recommend administering approximately half the total daily dose instead of 100% of the total daily dose (Grade 1C). In patients who are receiving bridging anticoagulation with therapeutic-dose IV UFH, we recommend stopping UFH approximately 4 h before surgery over stopping UFH closer to surgery (Grade 1C).

Summary
• Await trials for good evidence basis for “bridging” protocol recommendations
• Need to assess risk of thromboembolism versus the risk of bleeding in each patient
• Most patients can undergo dental procedures and diagnostic endoscopy without alteration of their OAC regimen.
• Bridging therapy is most often indicated within 1 month of VTE or stroke or coronary events and in patients with mitral valve prostheses

Continuity/Discontinuity of Anti-
platelet medications

4.0 Perioperative Management of Patients Who Are Receiving Antiplatelet Therapy
4.2 In patients who require temporary interruption of aspirin- or clopidogrel-containing drugs before surgery or a procedure, we suggest stopping this treatment 7 to 10 days before the procedure over stopping this treatment closer to surgery (Grade 2C).
4.3 In patients who have had temporary interruption of aspirin therapy because of surgery or a procedure, we suggest resuming aspirin approximately 24 h (or the next morning) after surgery when there is adequate hemostasis instead of resuming aspirin closer to surgery (Grade 2C). In patients who have had temporary interruption of clopidogrel because of surgery or a procedure, we suggest resuming clopidogrel approximately 24 h (or the next morning) after surgery when there is adequate hemostasis instead of resuming clopidogrel closer to surgery (Grade 2C).
4.4 In patients who are receiving antiplatelet drugs, we suggest against the routine use of platelet function assays to monitor the antithrombotic effect of aspirin or clopidogrel (Grade 2C).

Cardiac stents
• Early noncardiac surgery after coronary stent placement is associated with an increased risk of major adverse cardiac events
– 20% perioperative mortality rate (Vicenzi et al Brit J Anaesthes 2006)
• Concern about late thrombosis in coronary stents which might be attributable to interruption of antiplatelet therapy
• Cessation of antiplatelet therapy increases the relative risk of coronary thrombosis by 90:1 (Broad et al Brit J Anaesthes 2007)
• About 5% of pts who undergo coronary stenting require some form of noncardiac surgery within 1 year after stenting

What to do with clopidogrel peri-
procedurally?
ASK THE CARDIOLOGIST
And when would you ask the haematologist?

6.2. For patients receiving aspirin, clopidogrel, or both, are undergoing surgery and have excessive or life-threatening perioperative bleeding, we suggest transfusion of platelets or administration of other prohemostatic agents (Grade 2C).
The Perioperative Management of Antithrombotic Therapy., James D. Douketis, et.al. CHEST 2008,
133:299S-339.,

And about anticoagulant reversal
• Vitamin K antagonists
reversal strategies dependent on urgency/
thrombotic vs bleeding risk of procedure/
availability of factor replacement products
(FFP, PTX) etc
• Policies required
• Newer anticoagulants have no antidotes

• AND IN PATIENTS NOT ALREADY ON
ANTICOAGULANT OR ANTI-PLATELET
THERAPIES….

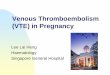
VTE – Attributable Risks
0%5%
10%15%20%25%30%35%40%45%50%
Hos
pita
lizat
ion
Can
cer
Traum
aCCF
Paralys
isSTP
Medical
Surgical
Recent hospitalization accounts for about 50% of all cases of VTE
Heit J Thromb Haemostas 2005


Risk Stratification of
Procedures
• HIGH RISK
Proximal DVT 10-20%
Pulmonary embolism 4-10%
(5% fatal)
• MODERATE RISK
Proximal DVT 2-4%
Pulmonary embolism 1-2%

Risk Stratification of
Procedures
• LOW RISK
• Proximal DVT <0.5%
• Pulmonary embolism 0.2%

Risk Stratification (surgery)
• Surgical patients – high risk
– Orthopaedic surgery of pelvis, hip or lower limb
– Multiple trauma
– Major surgery and age >60 years
– Major surgery and age 40-60 years with medical risk factors

Early Postoperative VTE rates(the baseline risk from clinical trial control groups)
Surgery
for
% with
DVT
% with
PE
Total Proximal Total Fatal
THR 42 – 57 18 – 36 0.9 – 28 0.1 – 2.0
TKR 41 – 85 5 – 22 1.5 – 10 0.1 – 1.7
Hip # 46 – 60 23 – 30 3 – 11 2.5 – 7.5
DVT rates reported in clinical trials with mandatory venography, published since 1980,
where patients received no prophylaxis or placebo. From WH Geerts et al, 7th ACCP
Conference, Chest 2004; 126: 338S – 400S



Risk Stratification medical
• Medical patients – high risk
– Age >60 years
– Ischaemic stroke
– History of VTE
– Decompensated heart failure
– Active cancer
– Acute on chronic lung disease
– Acute on chronic inflammatory disease

Frequency of VTE in Medical
Patients
Without prophylaxis:Frequencies of DVT
Screened by Fibrinogen uptake test (FUT) : 15%Venogram 15%Doppler ultrasound exam 5-7%

The need for prophylaxis
• Do we all need to implement systems to
assess and treat patients and how do we
best do it?
• Increasingly suggested by local experts
(eg APSTH) that the incidence of VTE in
Asian populations may have been under-
reported in past literature

Chemical and mechanical
methods
• Choice dependent on risk assessment of clotting vs bleeding and
• Presently dominated by LMWH because of proven efficacy and safety, long-familiarity and relative ease of administration
• Recent concerns of fatal anaphylaxis in dialysis patients in US due to excessive chondroitin sulphation, a quality issue which has now been addressed

What will we achieve?
• With implementation of
thromboprophylaxis to inpatients at high
medical risk and/or surgical risk, we
reduce the incidence and complications of
VTE
• For how long and with what intensity of
anticoagulation?

Initial or extended prophylaxis after
THR (TKR) (meta-analysis of 7 comparisons)
5-7 weeks (n = 1047) -v- 1-2 weeks (n = 854) of LMWH or UFH
1 - 2
wks
5 - 7
wks
OR NNT/H
Subclinical DVT 19.6% 9.6% 0.48
0.36-0.63
10
Subclinical proximal
DVT
9.1% 2.9% 0.33
0.21-0.51
16
Symptomatic VTE 3.3% 1.3% 0.38
0.24-0.61
50
Minor (no major)
bleeding
2.5% 3.7% 1.56
1.08-2.26
83
From JW Eikelboom et al, Lancet 2001; 358: 9-15

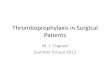
What Dose of LMWH in medical
patients?
0
2
4
6
8
10
12
14
16
All VTE Proximal DVT PE
Placebo
Enoxaparin 20 mg
Enoxaparin 40 mg
P<0.001
P=0.04
NS
14.9%
5.5% 4.9%
1.7%
15.0%
4.5%
RRR=63%
RRR=65%
Pa
tie
nts
ex
pe
rie
nc
ing
eve
nts
(%
)
RRR, relative risk reduction Samama et al. N Engl J Med 1999;341:793-800
Reduced dose if low body weight
or impaired renal function

How do we develop guidelines?
• Taking into account robustness of data
• Need to also be aware of costs in:
- Implementation
- Adverse drug effects
- Price to society
- Inconvenience to patients
Answers vary between surgeons and specialties.
Guidelines should be designed to permit audit, and
consider the implications for resources and
medicolegal / coronial concerns

Systems development
a multidisciplinary approach
• Engagement of all stakeholders in
guideline development
• Sponsorship by clinical leaders
• Education including that of patients
• Risk Assessment and prescription
“forcers”
• Audit and links to hospital accreditation



REFERENCES
CHEST/133/6/ June, 2008 Supplement[1]
Prevention of Venous Thromboembolism. ACCP Evidence-Based Clinical Practice Guidelines (8th edition)
NH&MRC Guidelines (Australia) Dec 2009
www.nhmrc.gov.au

Not far from Shangri La

THANK YOU



High Risk Surgical and
Medical Audit Example
Heparin & mechanical
Heparin
Mechanical
Inadequate
Division of Surgery Division of Medicine

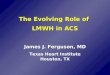
Bridging Therapy
Douketis Thromb Res 2003

VTE Prophylaxis in Cancer Patients
Authors Tumour No. of pts VTE incidence
Brandes et al Glioma 75 24.0%
Weijl et al Germ cell 179 8.4%
Ottinger et al NH Lymphoma 593 6.6%
Von Temelhoff et al Ovarian 47 10.6%
Zangari et al, 2004 M. Myeloma,
thalidomide + chemotherapy 34%
thalidomide + dexa 9%
chemotherapy 14%
What are the roles for LMWH as prophylaxis/ treatment in cancer?

Venous Thromboembolism
• If PE or Proximal DVT within past 2 weeks OR if the risk of bleeding during therapeutic heparin/LMWH is considered unacceptable - a temporary vena caval filter should be inserted
• Within the first month after acute episode of VTE
– the risk of postoperative VTE is > risk of bleeding associated with perioperative UFH/LMWH (Kearon et al NEJM 1997)
– Pre and Postoperative bridging IV UFH/ LMWH results in a net reduction in serious morbidity

Venous Thromboembolism
• In the absence of anticoagulation - Within 3 months after proximal DVT the recurrence risk is approx 50%
• Aim to defer any elective surgery until after 3 months of anticoagulation if possible
• 1 month of warfarin reduces the “spontaneous” recurrence risk to about 10%
• 3 months of warfarin reduces the risk to 5 %
• Stopping anticoagulation in the first month after an acute event is associated with a 40% risk of recurrence
• Risk of recurrence is highest in patients with cancer, chronic diseases and APS; homozygosity for Factor V Leiden; combined heterozygosity for Factor V and prothrombin gene mutation

Venous Thromboembolism
• Surgery creates a highly thrombotic state - risk of VTE after surgery is increased up to 100 fold postoperatively
• Decision on bridging depends on time since previous thrombosis and recurrence risk in that patient
• Unprovoked VTE associated with 10 - 27% recurrence risk per year
• Provoked VTE associated with 2-5% recurrence risk per year
• Pts with recurrent VTE, a hereditary hypercoagulable state or active cancer - recurrence risk approx 15% per year (Kearon et al NEJM 1997)

VTE Prophylaxis in Ischaemic
Stroke
LWMH is more effective than LDUH in ischaemic stroke with lower
limb weakness
VTE incidenceEnoxaparin (n=666) UFH (n=669) p40mg/d 5000U bid
NIHSS score <14 8.3% 14.0% p=0.004
NIHSS score >14 16.3% 29.7% p=0.004
RR 0.57, (95% CI 0.44-0.76, p=0.0001)
Intracranial and major extra-cranial bleed LMWH 1%, UFH 1%
An important single study but meta-analyses not all supportive
PREVAIL Sherman et al: Lancet 369: 1413-15, 2007