Embed Size (px)
Citation preview
Acute Stroke Thrombolysis (Southland)TIME IS BRAIN
All patients must have had a Stroke Diagnosis Form (79592) completed before proceeding This document is only to be used where there is the initial intention to thrombolyse. If there is no intent
to thrombolyse then please use Acute Stroke Pathway (Southland) (79593) documentation
It is vital that the details in this document be considered carefully, but one must act quickly as benefits of thrombolysis are likely to be greatest the earlier the treatment is given.
Blood glucose: _____ Rule out hypoglycaemia masquerading as stroke.
Blood pressure: _____ Note: Systolic ≥ 185 or diastolic ≥ 110 on repeated measures will need addressing.
(Give labetolol 10 mg IV bolus, then start an infusion at 2mg/ minute. Place labetolol 100mg (20mL) in 80 mL 0.9% sodium chloride solution to get a 1:1 solution (100mg labetolol in 100mL solution))
Temperature: ________(no evidence of sepsis, sub-acute bacterial endocarditis)
Stroke Thrombolysis Inclusion Criteria:1. Rapid onset FOCAL neurological deficit – likely due to stroke Yes No
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 1 of 31
Acute Stroke Throm
bolysis (Southland) MR
1392 V1
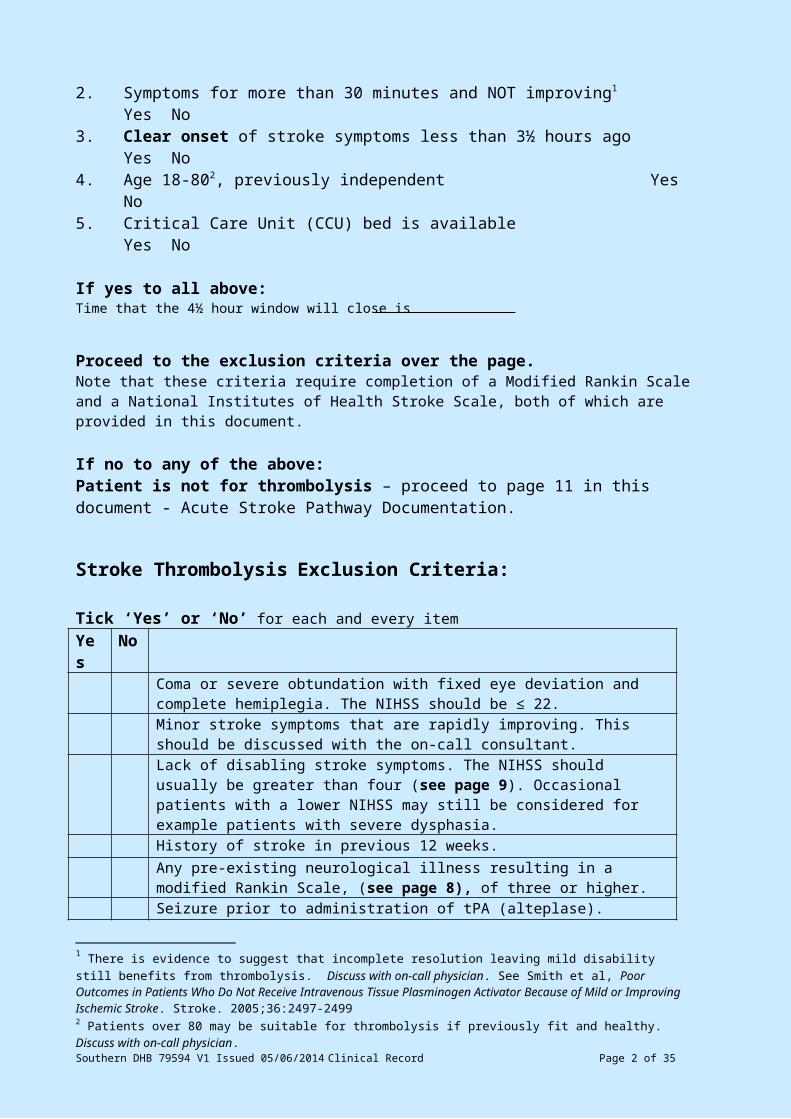
2. Symptoms for more than 30 minutes and NOT improving1 Yes No3. Clear onset of stroke symptoms less than 3½ hours ago Yes No4. Age 18-802, previously independent Yes No5. Critical Care Unit (CCU) bed is available Yes No
If yes to all above:Time that the 4½ hour window will close is
Proceed to the exclusion criteria over the page.Note that these criteria require completion of a Modified Rankin Scale and a National Institutes of Health Stroke Scale, both of which are provided in this document.
If no to any of the above: Patient is not for thrombolysis – proceed to page 11 in this document - Acute Stroke Pathway Documentation.
Stroke Thrombolysis Exclusion Criteria:
Tick ‘Yes’ or ‘No’ for each and every itemYes No
Coma or severe obtundation with fixed eye deviation and complete hemiplegia. The NIHSS should be ≤ 22.Minor stroke symptoms that are rapidly improving. This should be discussed with the on-call consultant.Lack of disabling stroke symptoms. The NIHSS should usually be greater than four (see page 9). Occasional patients with a lower NIHSS may still be considered for example patients with severe dysphasia. History of stroke in previous 12 weeks.Any pre-existing neurological illness resulting in a modified Rankin Scale, (see page 8), of three or higher.Seizure prior to administration of tPA (alteplase).Previously known intracranial or subarachnoid hemorrhages, arteriovenous malformation, aneurysm, or previously known intracranial neoplasm that is terminal or would increase the risk of intracranial bleeding after tPA (alteplase), or may confound neurological assessment.Clinical presentation suggestive of subarachnoid hemorrhage, even if the initial CT is normal. Hypertension: systolic blood pressure ≥ 185mmHg; or diastolic blood pressure > 110mmHg on repeated measures prior to administration of tPA (alteplase).NB - tPA (alteplase) may be given if the BP is able to be cautiously lowered to these levels within 4.5 hours. Presumed septic embolus. Myocardial infarction within past 30 days.Biopsy of a parenchymal organ or surgery that would increase the risk of unmanageable (e.g. uncontrolled by local pressure) bleeding after the administration of tPA (alteplase) in the past 30 days. Recent trauma, with internal injuries/ulcerative wounds in the past 30 days. Any hemorrhage in the last 30 days that would increase the risk of unmanageable (e.g. uncontrolled by local pressure) bleeding after the
1 There is evidence to suggest that incomplete resolution leaving mild disability still benefits from thrombolysis. Discuss with on-call physician. See Smith et al, Poor Outcomes in Patients Who Do Not Receive Intravenous Tissue Plasminogen Activator Because of Mild or Improving Ischemic Stroke. Stroke. 2005;36:2497-24992 Patients over 80 may be suitable for thrombolysis if previously fit and healthy. Discuss with on-call physician.Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 2 of 31
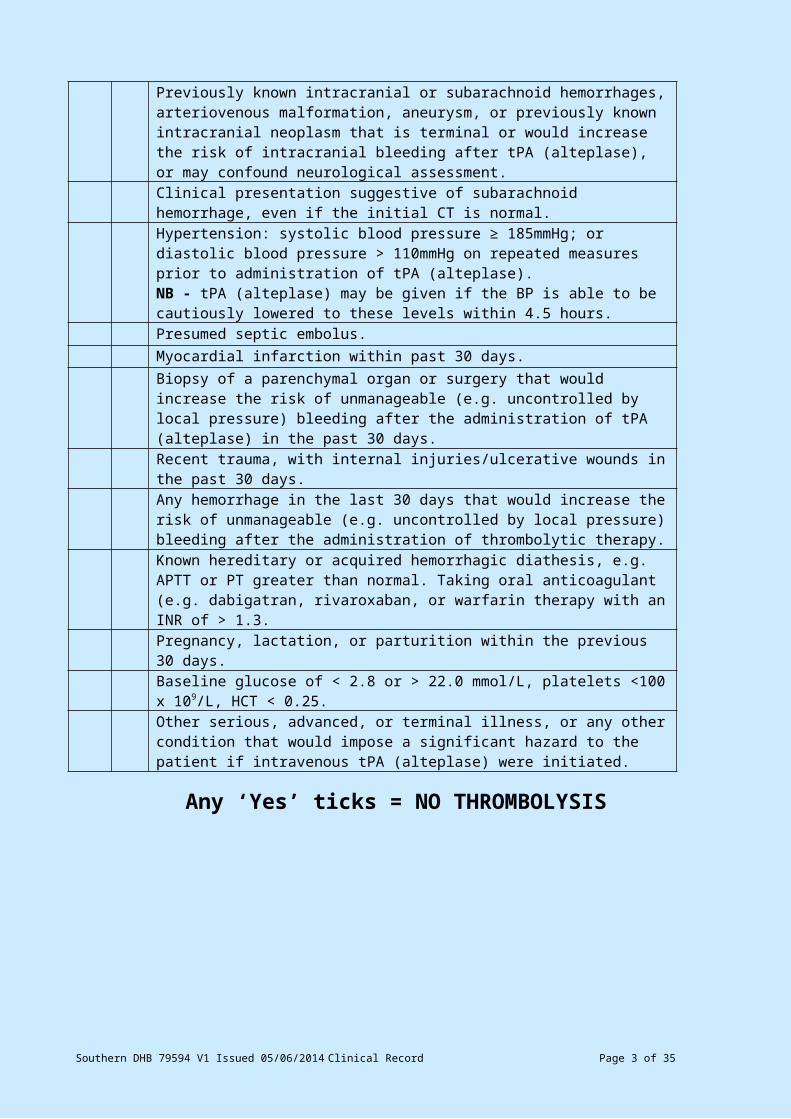
administration of thrombolytic therapy.Known hereditary or acquired hemorrhagic diathesis, e.g. APTT or PT greater than normal. Taking oral anticoagulant (e.g. dabigatran, rivaroxaban, or warfarin therapy with an INR of > 1.3. Pregnancy, lactation, or parturition within the previous 30 days. Baseline glucose of < 2.8 or > 22.0 mmol/L, platelets <100 x 109/L, HCT < 0.25. Other serious, advanced, or terminal illness, or any other condition that would impose a significant hazard to the patient if intravenous tPA (alteplase) were initiated.
Any ‘Yes’ ticks = NO THROMBOLYSIS
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 3 of 31
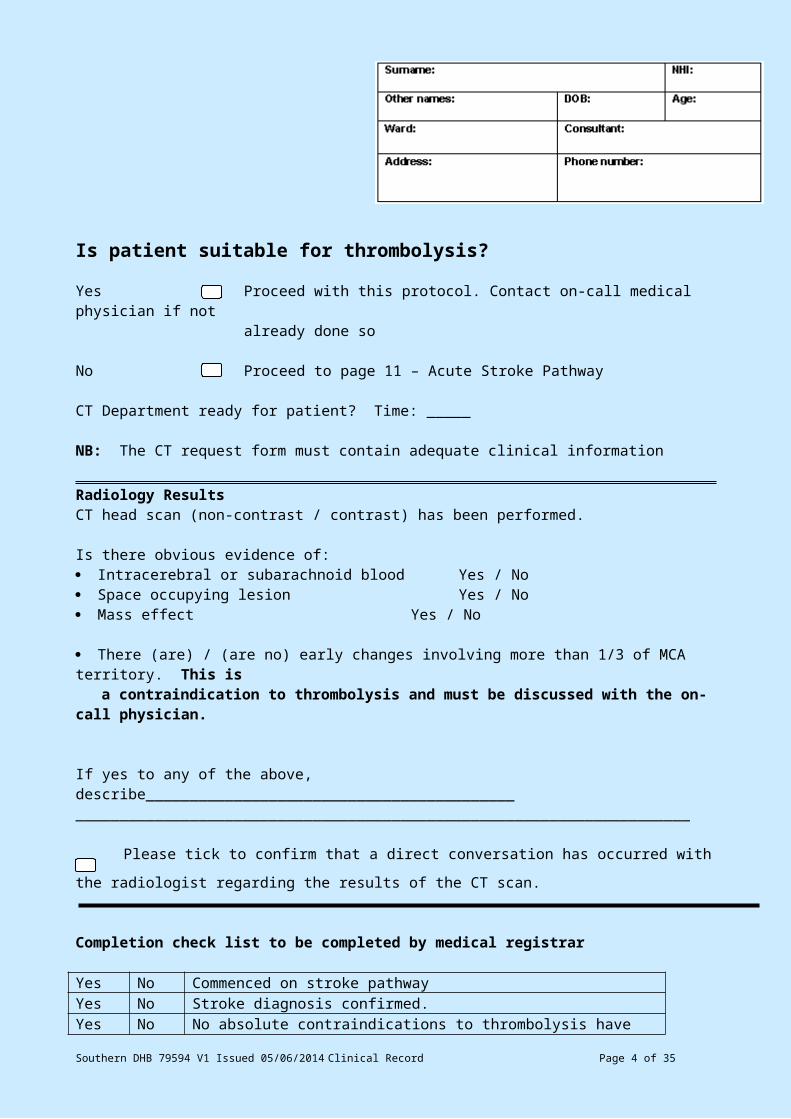
Is patient suitable for thrombolysis?
Yes Proceed with this protocol. Contact on-call medical physician if notalready done so
No Proceed to page 11 – Acute Stroke Pathway
CT Department ready for patient? Time: _____
NB: The CT request form must contain adequate clinical information
Radiology ResultsCT head scan (non-contrast / contrast) has been performed.
Is there obvious evidence of: Intracerebral or subarachnoid blood Yes / No Space occupying lesion Yes / No Mass effect Yes / No
There (are) / (are no) early changes involving more than 1/3 of MCA territory. This is a contraindication to thrombolysis and must be discussed with the on-call physician.
If yes to any of the above, describe________________________________________________________________________________________________________________
Please tick to confirm that a direct conversation has occurred with the radiologist regarding
the results of the CT scan.
Completion check list to be completed by medical registrar
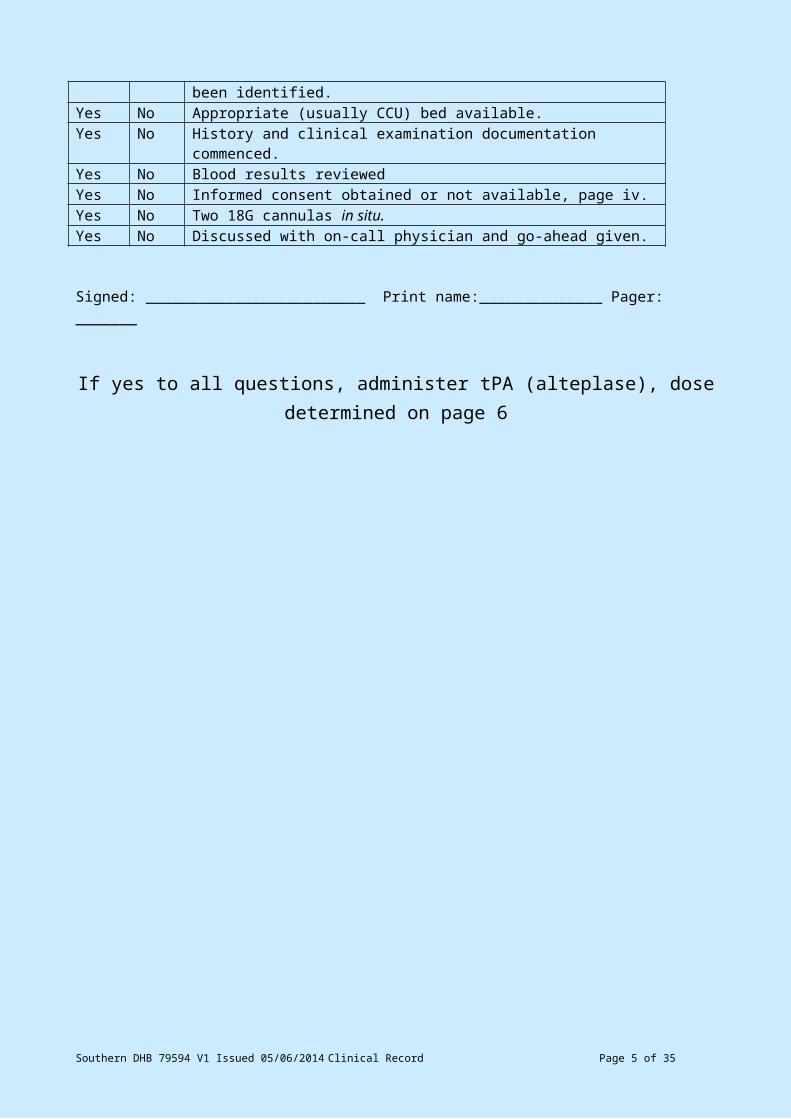
Yes No Commenced on stroke pathwayYes No Stroke diagnosis confirmed.Yes No No absolute contraindications to thrombolysis have been identified.Yes No Appropriate (usually CCU) bed available.Yes No History and clinical examination documentation commenced.Yes No Blood results reviewedYes No Informed consent obtained or not available, page iv.Yes No Two 18G cannulas in situ.Yes No Discussed with on-call physician and go-ahead given.
Signed: _________________________ Print name:______________ Pager: _______
If yes to all questions, administer tPA (alteplase), dose determined on page 6
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 4 of 31
Consent for Acute Stroke Treatment with tPA (alteplase)
Treatment Information
Your doctors have determined that you have had a stroke, and that you might benefit from treatment with tPA (tissue plasminogen activator).
Your stroke has been caused by a blockage to a blood vessel in the brain. The blockage to the blood vessel is caused by a blood clot. tPA is a drug which causes blood clots to dissolve (thrombolysis) and may help restore blood flow to your brain. The treatment is given intravenously (through a ‘drip’) over one hour. If it is to be used, this treatment must be given within 4½ hours of the first sign of stroke.
Thrombolysis with tPA under strictly controlled conditions is an internationally recommended treatment for acute stroke. This treatment is estimated to result in one more patient recovering full independence after a stroke for every eight patients treated. Other patients may get smaller benefits. But thrombolysis with tPA can also cause bleeding into the brain and worsening of the stroke. This occurs to around one in 20 patients treated with tPA. On occasion, this bleeding may cause death.
Your consent for treatment with this medication is voluntary (your choice). If you do not wish to receive this treatment, you will receive full standard hospital treatment for stroke, which may include aspirin or other anticoagulants.
Consent for Treatment with Intravenous tPA
I have read and understood the treatment information regarding the use of tPA for acute stroke. I understand that tPA does not benefit all patients with stroke and can cause worsening of stroke in some people.
I have had a chance to have my questions answered about this treatment.
I consent to treatment of myself / my relative with intravenous tPA for stroke.
Signed: _________________________Print: ______________________________________
Date: ____/____/____ Capacity: patient / next-of-kin / other (state):_________________
Witness:_____________________________Print:___________
Date: ____/____/____
q ____________________________Verbal consent only: from: reason:
q Treatment without formal consent: reason:_________________________
(Note: Treatment without consent can only occur in exceptional cases and must be justifiable ,e.g. clear clinical indication in young patient but with inability to get necessary consent)Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 5 of 31
Consent for Acute Stroke Treatment with tPA (ALTEPLASE)
(Patient’s copy – to be removed, completed and given to the patient)
Treatment Information
Your doctors have determined that you have had a stroke, and that you might benefit from treatment with tPA (tissue plasminogen activator).
Your stroke has been caused by a blockage to a blood vessel in the brain. The blockage to the blood vessel is caused by a blood clot. tPA is a drug which causes blood clots to dissolve (Thrombolysis) and may help restore blood flow to your brain. The treatment is given intravenously (through a ‘drip’) over one hour. If it is to be used, this treatment must be given within 4½ hours of the first sign of stroke.
Thrombolysis with tPA under strictly controlled conditions is an internationally recommended treatment for acute stroke. This treatment is estimated to result in one more patient recovering full independence after a stroke for every eight patients treated. Other patients may get smaller benefits. But thrombolysis with tPA can also cause bleeding into the brain and worsening of the stroke. This occurs to around one in 20 patients treated with tPA. On occasion, this bleeding may cause death.
Your consent for treatment with this medication is voluntary (your choice). If you do not wish to receive this treatment, you will receive full standard hospital treatment for stroke, which may include aspirin or other anticoagulants.
Consent for Treatment with Intravenous tPA
I have read and understood the treatment information regarding the use of tPA for acute stroke. I understand that tPA does not benefit all patients with stroke and can cause worsening of stroke in some people.
I have had a chance to have my questions answered about this treatment.
Consent to treatment of myself / my relative with intravenous tPA for stroke was obtained by:
Signed: _________________________Print: ______________________________________
Date: ____/____/____ Capacity: patient / next-of-kin / other (state):_________________
Witness: _____________________________Print:___________
Date: ____/____/____
q _______________________________Verbal consent only: from: reason:
q Treatment without formal consent: reason:_________________________
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 6 of 31
Note: Treatment without consent can only occur in exceptional cases and must be justifiable, e.g. clear clinical indication in young patient but with inability to get necessary consent)
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 7 of 31
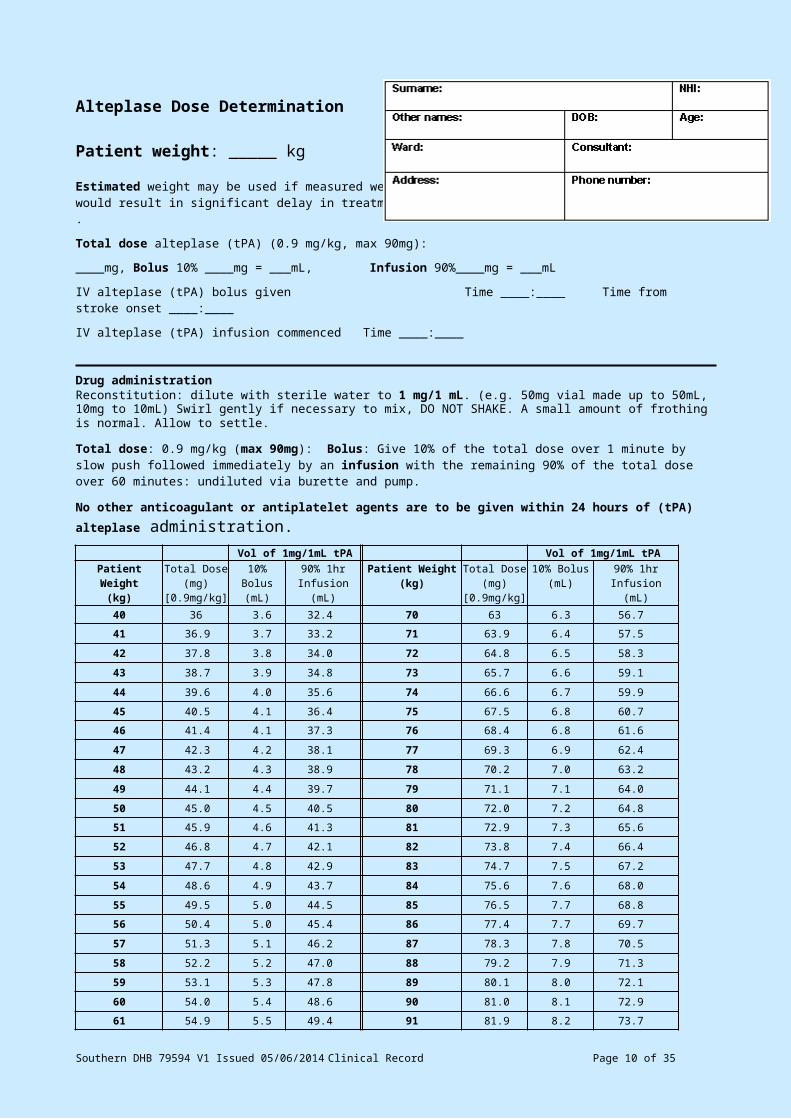
Alteplase Dose Determination
Patient weight: _____ kg
Estimated weight may be used if measured weightwould result in significant delay in treatment.
Total dose alteplase (tPA) (0.9 mg/kg, max 90mg):
____mg, Bolus 10% ____mg = ___mL, Infusion 90%____mg = ___mL
IV alteplase (tPA) bolus given Time ____:____ Time from stroke onset ____:____
IV alteplase (tPA) infusion commenced Time ____:____
Drug administrationReconstitution: dilute with sterile water to 1 mg/1 mL. (e.g. 50mg vial made up to 50mL, 10mg to 10mL) Swirl gently if necessary to mix, DO NOT SHAKE. A small amount of frothing is normal. Allow to settle.
Total dose: 0.9 mg/kg (max 90mg): Bolus: Give 10% of the total dose over 1 minute by slow push followed immediately by an infusion with the remaining 90% of the total dose over 60 minutes: undiluted via burette and pump.
No other anticoagulant or antiplatelet agents are to be given within 24 hours of (tPA) alteplase administration.Vol of 1mg/1mL tPA Vol of 1mg/1mL tPA
Patient Weight(kg)
Total Dose(mg)
[0.9mg/kg]
10% Bolus(mL)
90% 1hr Infusion
(mL)
Patient Weight(kg)
Total Dose(mg)
[0.9mg/kg]
10% Bolus(mL)
90% 1hr Infusion(mL)
40 36 3.6 32.4 70 63 6.3 56.7
41 36.9 3.7 33.2 71 63.9 6.4 57.5
42 37.8 3.8 34.0 72 64.8 6.5 58.3
43 38.7 3.9 34.8 73 65.7 6.6 59.1
44 39.6 4.0 35.6 74 66.6 6.7 59.9
45 40.5 4.1 36.4 75 67.5 6.8 60.7
46 41.4 4.1 37.3 76 68.4 6.8 61.6
47 42.3 4.2 38.1 77 69.3 6.9 62.4
48 43.2 4.3 38.9 78 70.2 7.0 63.2
49 44.1 4.4 39.7 79 71.1 7.1 64.0
50 45.0 4.5 40.5 80 72.0 7.2 64.8
51 45.9 4.6 41.3 81 72.9 7.3 65.6
52 46.8 4.7 42.1 82 73.8 7.4 66.4
53 47.7 4.8 42.9 83 74.7 7.5 67.2
54 48.6 4.9 43.7 84 75.6 7.6 68.0
55 49.5 5.0 44.5 85 76.5 7.7 68.8
56 50.4 5.0 45.4 86 77.4 7.7 69.7
57 51.3 5.1 46.2 87 78.3 7.8 70.5
58 52.2 5.2 47.0 88 79.2 7.9 71.3
59 53.1 5.3 47.8 89 80.1 8.0 72.1
60 54.0 5.4 48.6 90 81.0 8.1 72.9
61 54.9 5.5 49.4 91 81.9 8.2 73.7
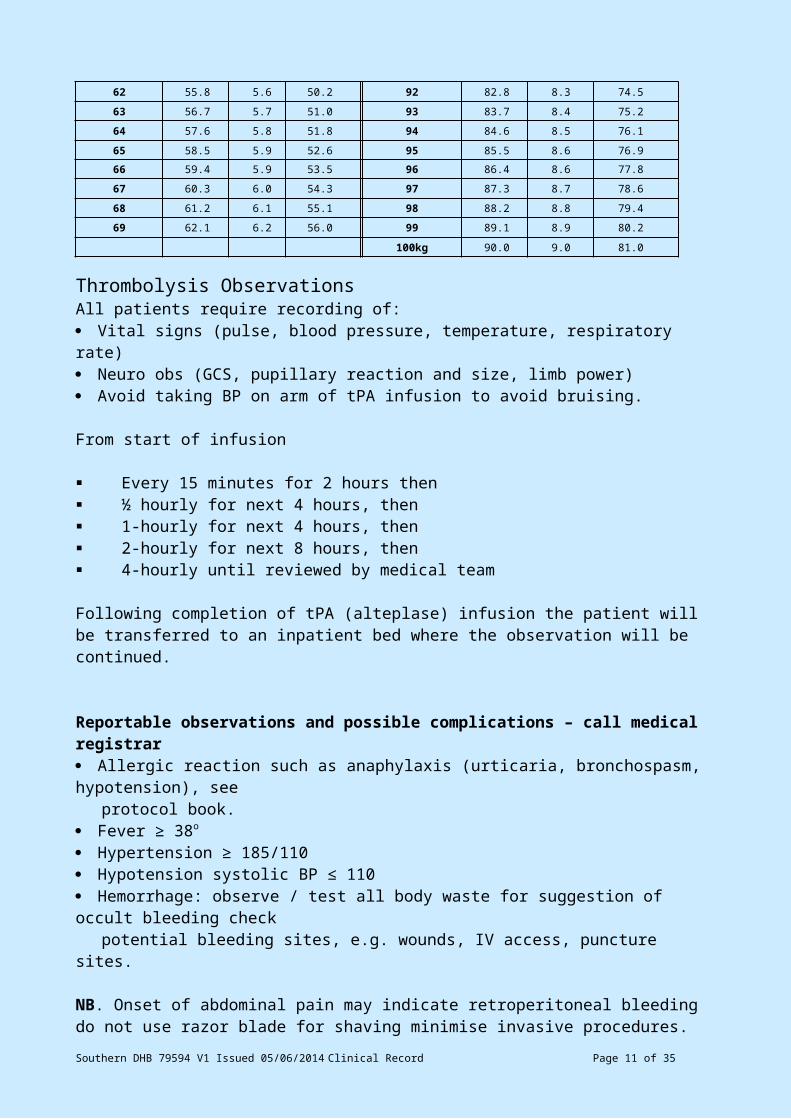
62 55.8 5.6 50.2 92 82.8 8.3 74.5
63 56.7 5.7 51.0 93 83.7 8.4 75.2
64 57.6 5.8 51.8 94 84.6 8.5 76.1
65 58.5 5.9 52.6 95 85.5 8.6 76.9
66 59.4 5.9 53.5 96 86.4 8.6 77.8
67 60.3 6.0 54.3 97 87.3 8.7 78.6
68 61.2 6.1 55.1 98 88.2 8.8 79.4
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 8 of 31
69 62.1 6.2 56.0 99 89.1 8.9 80.2
100kg 90.0 9.0 81.0
Thrombolysis ObservationsAll patients require recording of: Vital signs (pulse, blood pressure, temperature, respiratory rate) Neuro obs (GCS, pupillary reaction and size, limb power) Avoid taking BP on arm of tPA infusion to avoid bruising.
From start of infusion
Every 15 minutes for 2 hours then ½ hourly for next 4 hours, then 1-hourly for next 4 hours, then 2-hourly for next 8 hours, then 4-hourly until reviewed by medical team
Following completion of tPA (alteplase) infusion the patient will be transferred to an inpatient bed where the observation will be continued.
Reportable observations and possible complications – call medical registrar Allergic reaction such as anaphylaxis (urticaria, bronchospasm, hypotension), see
protocol book. Fever ≥ 38o
Hypertension ≥ 185/110 Hypotension systolic BP ≤ 110 Hemorrhage: observe / test all body waste for suggestion of occult bleeding check
potential bleeding sites, e.g. wounds, IV access, puncture sites.
NB. Onset of abdominal pain may indicate retroperitoneal bleeding do not use razor blade for shaving minimise invasive procedures.
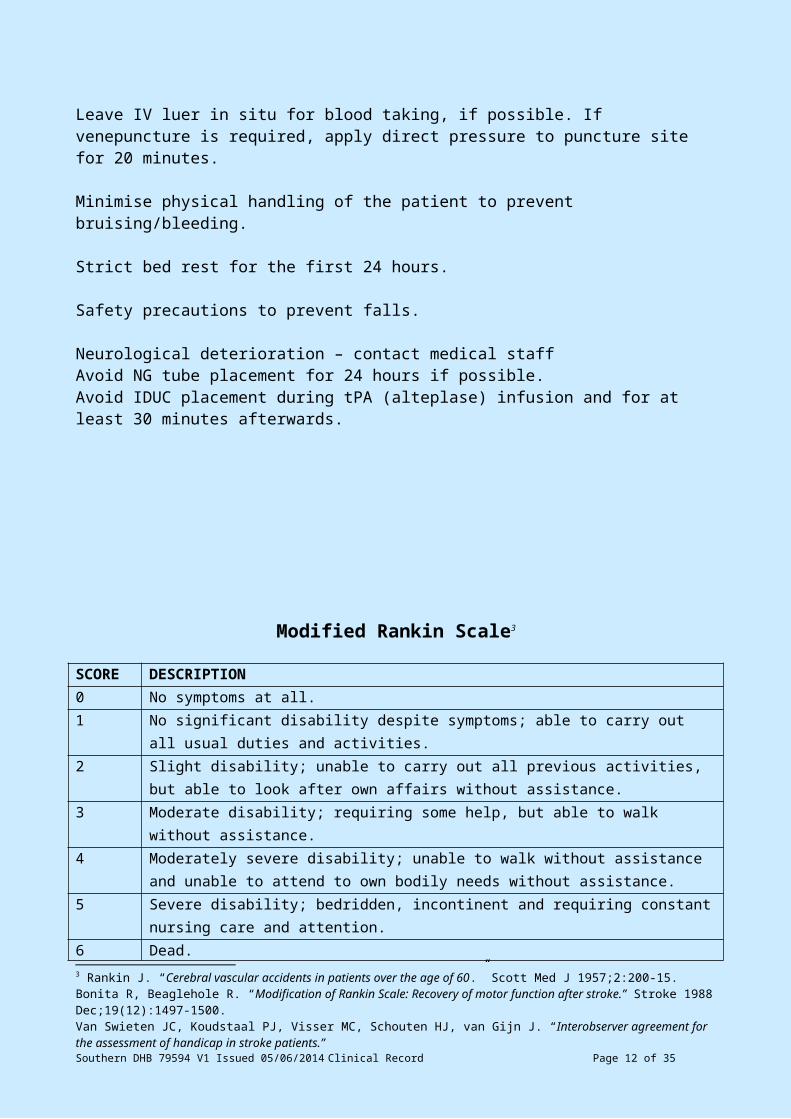
Leave IV luer in situ for blood taking, if possible. If venepuncture is required, apply direct pressure to puncture site for 20 minutes.
Minimise physical handling of the patient to prevent bruising/bleeding.
Strict bed rest for the first 24 hours.
Safety precautions to prevent falls.
Neurological deterioration – contact medical staffAvoid NG tube placement for 24 hours if possible.Avoid IDUC placement during tPA (alteplase) infusion and for at least 30 minutes afterwards.
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 9 of 31
Modified Rankin Scale3
SCORE DESCRIPTION0 No symptoms at all.1 No significant disability despite symptoms; able to carry out all usual duties and
activities.2 Slight disability; unable to carry out all previous activities, but able to look after own
affairs without assistance.3 Moderate disability; requiring some help, but able to walk without assistance.4 Moderately severe disability; unable to walk without assistance and unable to attend to
own bodily needs without assistance.5 Severe disability; bedridden, incontinent and requiring constant nursing care and
attention.6 Dead.
TOTAL (0–6): ____
3 Rankin J. “Cerebral vascular accidents in patients over the age of 60.” Scott Med J 1957;2:200-15.Bonita R, Beaglehole R. “Modification of Rankin Scale: Recovery of motor function after stroke.” Stroke 1988 Dec;19(12):1497-1500.Van Swieten JC, Koudstaal PJ, Visser MC, Schouten HJ, van Gijn J. “Interobserver agreement for the assessment of handicap in stroke patients.”Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 10 of 31
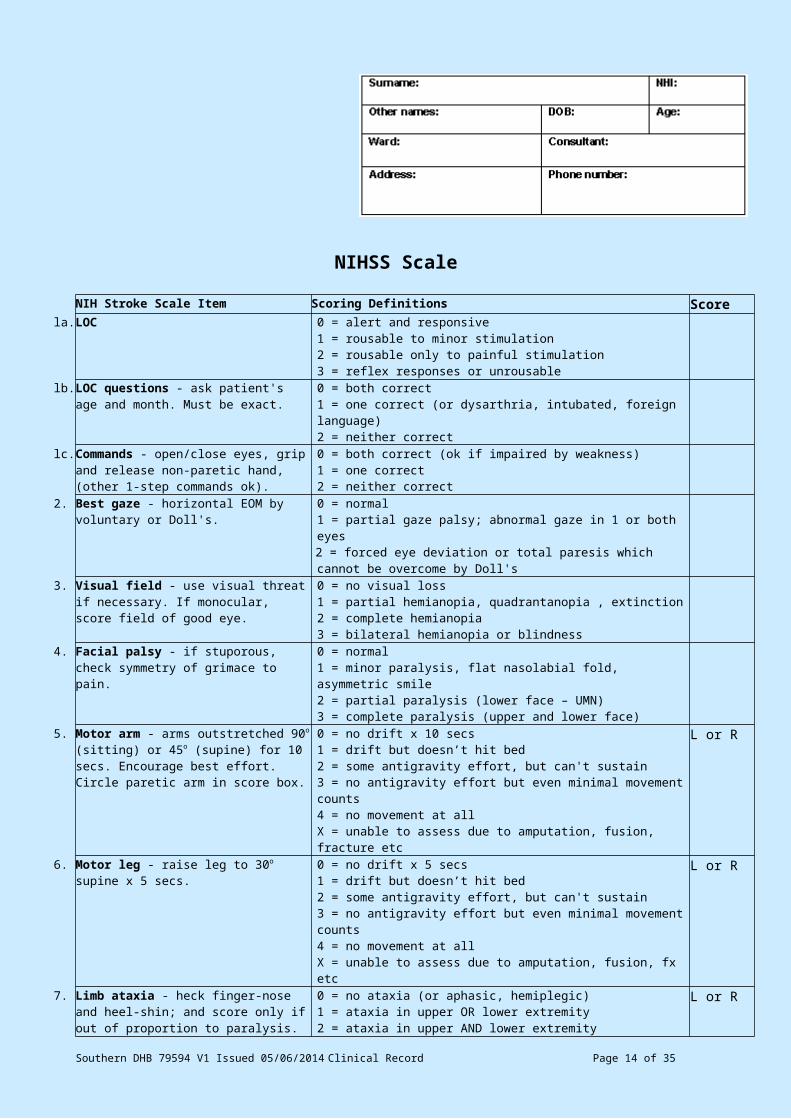
NIHSS ScaleNIH Stroke Scale Item Scoring Definitions ScoreLOC 0 = alert and responsive
1 = rousable to minor stimulation2 = rousable only to painful stimulation3 = reflex responses or unrousable
LOC questions - ask patient's age and month. Must be exact.
0 = both correct1 = one correct (or dysarthria, intubated, foreign language)2 = neither correct
Commands - open/close eyes, grip and release non-paretic hand, (other 1-step commands ok).
0 = both correct (ok if impaired by weakness)1 = one correct2 = neither correct
Best gaze - horizontal EOM by voluntary or Doll's.
0 = normal1 = partial gaze palsy; abnormal gaze in 1 or both eyes2 = forced eye deviation or total paresis which cannot be overcome by Doll's
Visual field - use visual threat if necessary. If monocular, score field of good eye.
0 = no visual loss1 = partial hemianopia, quadrantanopia , extinction2 = complete hemianopia3 = bilateral hemianopia or blindness
Facial palsy - if stuporous, check symmetry of grimace to pain.
0 = normal1 = minor paralysis, flat nasolabial fold, asymmetric smile2 = partial paralysis (lower face – UMN)3 = complete paralysis (upper and lower face)
Motor arm - arms outstretched 90o (sitting) or 45o (supine) for 10 secs. Encourage best effort. Circle paretic arm in score box.
0 = no drift x 10 secs1 = drift but doesn’t hit bed2 = some antigravity effort, but can't sustain3 = no antigravity effort but even minimal movement counts4 = no movement at allX = unable to assess due to amputation, fusion, fracture etc
L or R
Motor leg - raise leg to 30o supine x 5 secs. 0 = no drift x 5 secs1 = drift but doesn’t hit bed2 = some antigravity effort, but can't sustain3 = no antigravity effort but even minimal movement counts4 = no movement at allX = unable to assess due to amputation, fusion, fx etc
L or R
Limb ataxia - heck finger-nose and heel-shin; and score only if out of proportion to paralysis.
0 = no ataxia (or aphasic, hemiplegic)1 = ataxia in upper OR lower extremity2 = ataxia in upper AND lower extremityX = unable to assess due to amputation, fusion, fracture etc
L or R
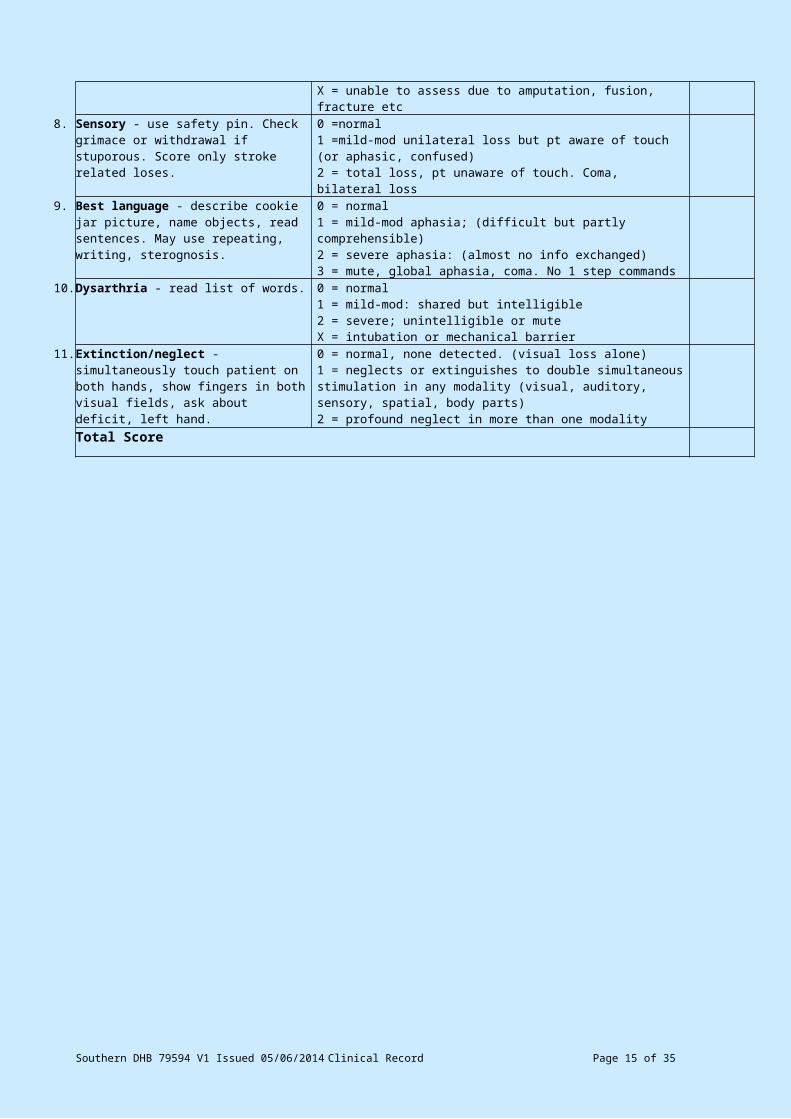
Sensory - use safety pin. Check grimace or withdrawal if stuporous. Score only stroke related loses.
0 =normal1 =mild-mod unilateral loss but pt aware of touch (or aphasic, confused)2 = total loss, pt unaware of touch. Coma, bilateral loss
Best language - describe cookie jar picture, name objects, read sentences. May use repeating, writing, sterognosis.
0 = normal1 = mild-mod aphasia; (difficult but partly comprehensible)2 = severe aphasia: (almost no info exchanged)3 = mute, global aphasia, coma. No 1 step commands
10. Dysarthria - read list of words. 0 = normal1 = mild-mod: shared but intelligible2 = severe; unintelligible or muteX = intubation or mechanical barrier
11. Extinction/neglect - simultaneously touch patient on both hands, show fingers in both visual fields, ask about deficit, left hand.
0 = normal, none detected. (visual loss alone)1 = neglects or extinguishes to double simultaneous stimulation in any modality (visual, auditory, sensory, spatial, body parts)2 = profound neglect in more than one modality
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 11 of 31
Total Score
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 12 of 31
Acute Stroke Pathway (Southland) – TIME IS BRAIN
Medical Guidelines for On-going Management
Physiological parametersThe hospital uses an early warning system that triggers defined responses.
** Refer to Early Warning Score (EWS) Severity Scoring System **
Swallow Screening All stroke admissions should be screened for the presence of dysphagia. The screening tool is
attached to this document for your convenience. If the patient fails the water component, make them ‘nil by mouth’ (NBM).
Please do not chart oral drugs if you make the patient NBM. If you do order NBM make a decision about ongoing hydration.
Aspirin
Aspirin naïveIf you make the patient NBM, administer three 100mg Cardiprin tablets (300mg) to be left to dissolve in the mouth (not sublingual) with no extra water and chart on-going 100mg daily oral Cardiprin. These are 100mg and formulated to dissolve on the tongue with no water. If the patient is able to swallow, administer 300mg of standard aspirin and chart aspirin 100mg daily.
Already on aspirinIf you make the patient NBM, chart on-going 100mg daily Cardiprin to dissolve in the mouth (with no added water and not sublingual). If the patient is able to swallow chart their usual drug and dose.
Note: Administration to a patient NBM assumes they are managing their own saliva production.
Nasogastric tubesWe would not generally favour placing a nasogastic tube before the first 48-72 hours of admission.
PyrexiaChart paracetamol for pyrexia > 37.5.
Blood pressureGive normal saline for hypotensionConsider treating > 220/120 for ischaemic stroke and > 180/105 for intracranial haemorrhage.
SteroidsThere is no indication for using steroids specifically for the management of acute stroke.
InvestigationsConsider carotid duplex studies for anterior circulation strokes that are operative candidates.Consider echocardiogram.
Medications consider: Antiplatelet agents (aspirin, dipyridamole, clopidrogrel) or indications for warfarin Antihypertensive drugs and goal BP Use of statins
DrivingEnsure patients and family (as appropriate) are aware of driving restrictions.
Occult arrhythmias
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 13 of 31
If in apparent sinus rhythm, three separate ECG’s must be obtained on consecutive days.
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 14 of 31
Clinical Documentation
Must include the following: Presenting problem(s) symptoms/duration History of presenting problem Past History including consideration of following risk factors:
Diabetes Smoker or ex-smoker Previous stroke Migraine Previous TIA’s Epilepsy Hypertension HRT/oral contraceptive Ischaemic heart disease High alcohol
(male > 4 drinks/day, female > 2 drinks/day) Recent MI Hyperlipideamia Atrial fibrillation Other serious illness Peripheral vascular disease Depression/anxiety Valvular disease
Current social history Family history Review of systems Medication history Drug reactions and allergies Examination
o Glasgow Coma Score (see appendix)o Vital signso Skino Lymph nodeso Endocrineo Cardiovascular system
Pulseso Respiratoryo Abdominalo Genito-urinaryo Musculoskeletalo Neurology
Abbreviated Mental Test Score (see appendix) Level of consciousness Orientation Swallow screening (see appendix for assessment tool) Language Cranial nerves (see appendix) Muscle tone Power (see appendix) Reflexes Co-ordination (see appendix) Sensory testing Baseline Modified Rankin Score (see appendix)
o Imaging and diagnostic resultso Main problemo Differential diagnosiso Problem listo Lab resultso Plan – must include
Daily 12 lead ECG for first 3 days Modified Rankin Score on day 3 Stroke classification at discharge (see appendix) Observe for urinary incontinence
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 15 of 31
o Give clear directives to nursing staff if NBM orderedo Give clear indication if DNR order needed and if necessary put in plac
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 16 of 31
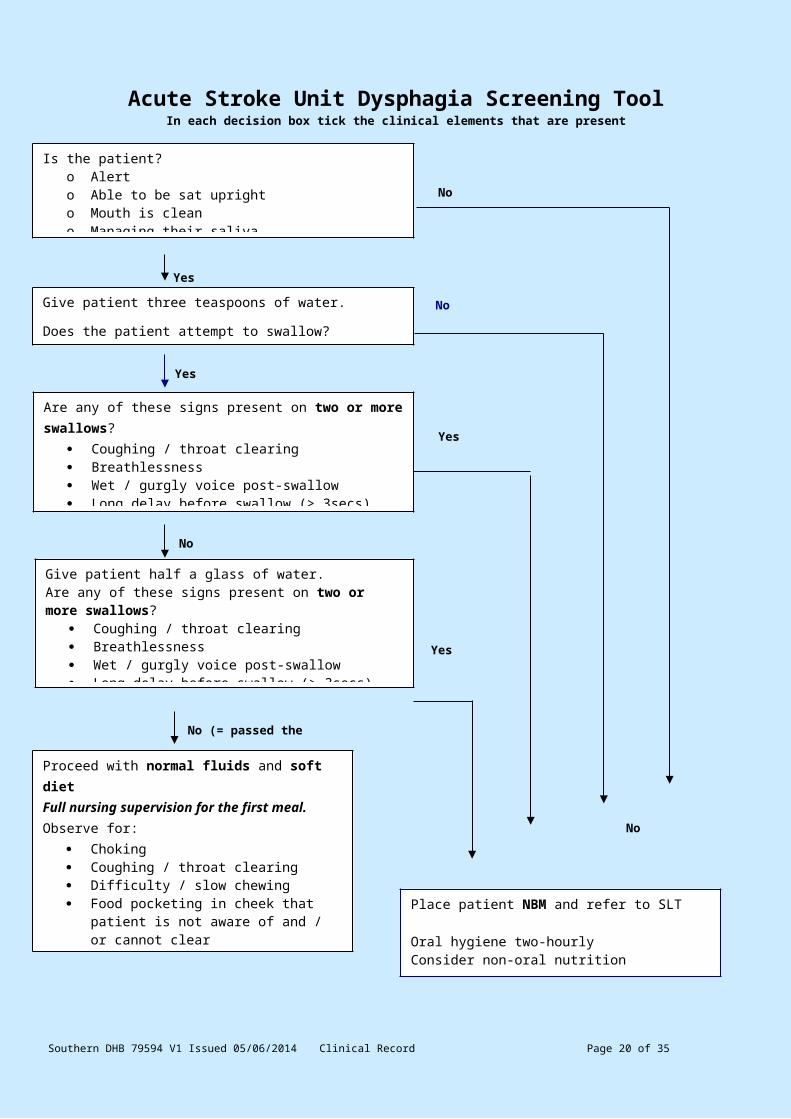
Acute Stroke Unit Dysphagia Screening ToolIn each decision box tick the clinical elements that are present
Dysphagia screen performed by : ______________________________ Date: ______________Time: ____________
Plan: _____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 17 of 31
Are any of these signs present on two or more swallows? Coughing / throat clearing Breathlessness Wet / gurgly voice post-swallow Long delay before swallow (> 3secs) Multiple swallows (3 or more)
Give patient half a glass of water.Are any of these signs present on two or more swallows?
Coughing / throat clearing Breathlessness Wet / gurgly voice post-swallow Long delay before swallow (> 3secs) Multiple swallows (3 or more)
Proceed with normal fluids and soft dietFull nursing supervision for the first meal.Observe for:
Choking Coughing / throat clearing Difficulty / slow chewing Food pocketing in cheek that patient is not
aware of and / or cannot clear Food falling out of mouth Fatigue Three or more swallows to clear
Is the patient?o Alerto Able to be sat uprighto Mouth is cleano Managing their saliva
Place patient NBM and refer to SLT
Oral hygiene two-hourlyConsider non-oral nutritionRepeat screen in 24 hours if not yet seen by SLT
No (= passed the screen)
Yes
No
Give patient three teaspoons of water.
Does the patient attempt to swallow?
Yes
Yes
No
No
Yes
No
Clinical Notes
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 18 of 31
Clinical N
otes M
R 4
Date
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 19 of 31
Clinical Notes
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 20 of 31
Clinical N
otes M
R 4
Date
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 21 of 31
Clinical Notes
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 22 of 31
Clinical N
otes M
R 4
Date
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 23 of 31
Clinical Notes
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 24 of 31
Clinical N
otes M
R 4
Date
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 25 of 31
Clinical Notes
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 26 of 31
Clinical N
otes M
R 4
Date
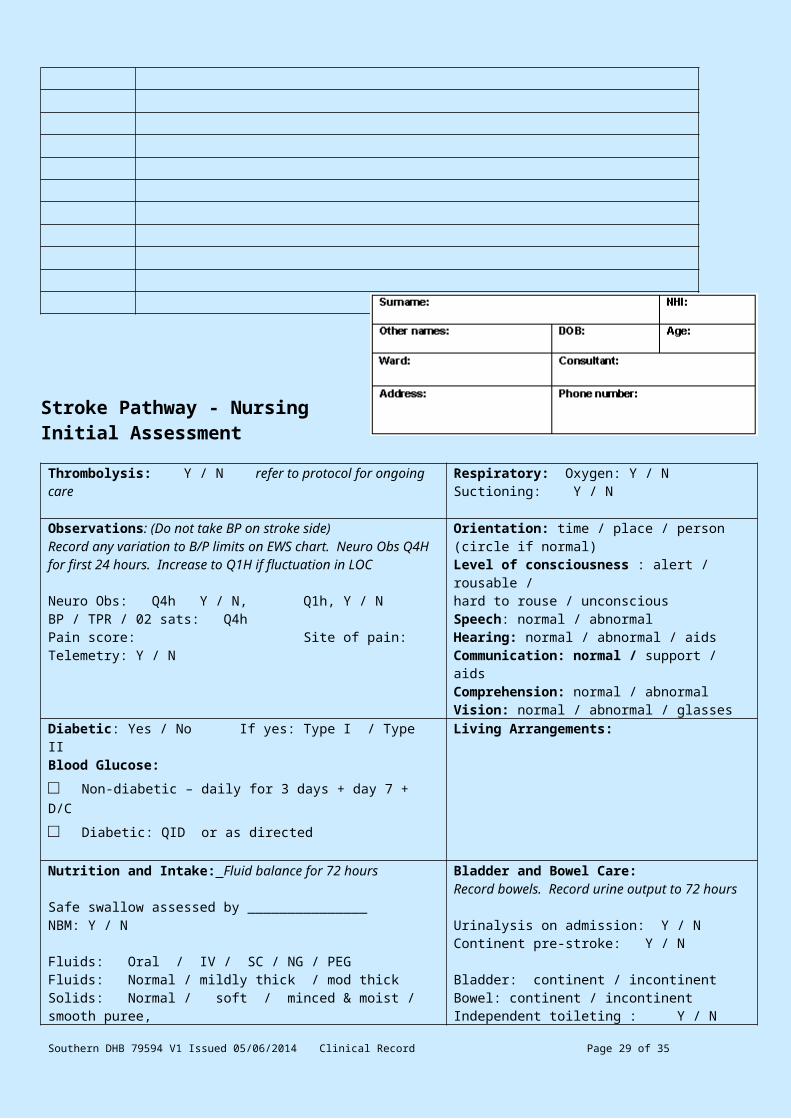
Stroke Pathway - Nursing Initial Assessment
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 27 of 31
Thrombolysis: Y / N refer to protocol for ongoing care Respiratory: Oxygen: Y / N Suctioning: Y / N
Observations: (Do not take BP on stroke side)Record any variation to B/P limits on EWS chart. Neuro Obs Q4H for first 24 hours. Increase to Q1H if fluctuation in LOC
Neuro Obs: Q4h Y / N, Q1h, Y / NBP / TPR / 02 sats: Q4hPain score: Site of pain:Telemetry: Y / N
Orientation: time / place / person (circle if normal)Level of consciousness : alert / rousable / hard to rouse / unconsciousSpeech: normal / abnormal Hearing: normal / abnormal / aidsCommunication: normal / support / aids Comprehension: normal / abnormalVision: normal / abnormal / glasses
Diabetic: Yes / No If yes: Type I / Type II Blood Glucose: □ Non-diabetic – daily for 3 days + day 7 + D/C
□ Diabetic: QID or as directed
Living Arrangements:
Nutrition and Intake: Fluid balance for 72 hours
Safe swallow assessed by _______________NBM: Y / N
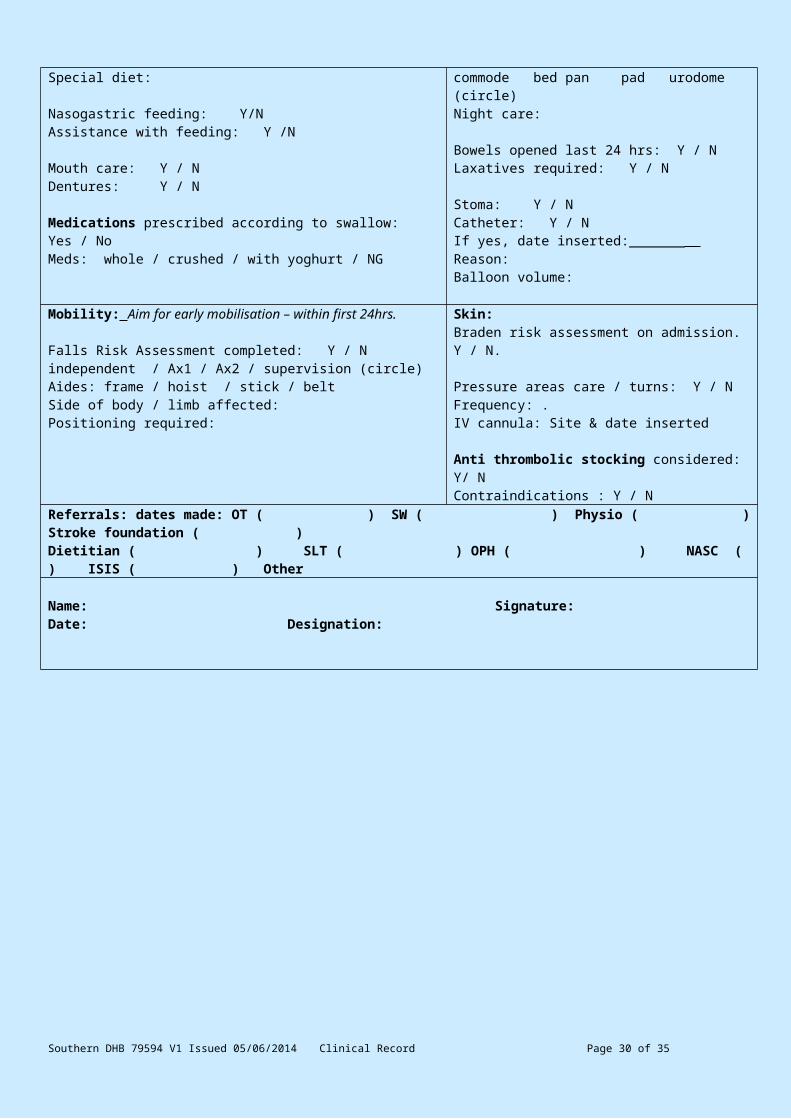
Fluids: Oral / IV / SC / NG / PEGFluids: Normal / mildly thick / mod thickSolids: Normal / soft / minced & moist / smooth puree, Special diet:
Nasogastric feeding: Y/NAssistance with feeding: Y /N
Mouth care: Y / NDentures: Y / N
Medications prescribed according to swallow: Yes / NoMeds: whole / crushed / with yoghurt / NG
Bladder and Bowel Care:Record bowels. Record urine output to 72 hours
Urinalysis on admission: Y / NContinent pre-stroke: Y / N
Bladder: continent / incontinent Bowel: continent / incontinentIndependent toileting : Y / Ncommode bed pan pad urodome (circle)Night care:
Bowels opened last 24 hrs: Y / NLaxatives required: Y / N Stoma: Y / N Catheter: Y / NIf yes, date inserted:_______ Reason:Balloon volume:
Mobility: Aim for early mobilisation – within first 24hrs.
Falls Risk Assessment completed: Y / N independent / Ax1 / Ax2 / supervision (circle)Aides: frame / hoist / stick / belt Side of body / limb affected: Positioning required:
Skin:Braden risk assessment on admission. Y / N.
Pressure areas care / turns: Y / N Frequency: . IV cannula: Site & date inserted
Anti thrombolic stocking considered: Y/ NContraindications : Y / N
Referrals: dates made: OT ( ) SW ( ) Physio ( ) Stroke foundation ( ) Dietitian ( ) SLT ( ) OPH ( ) NASC ( ) ISIS ( ) Other
Name: Signature: Date: Designation:
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 28 of 31
Appendices
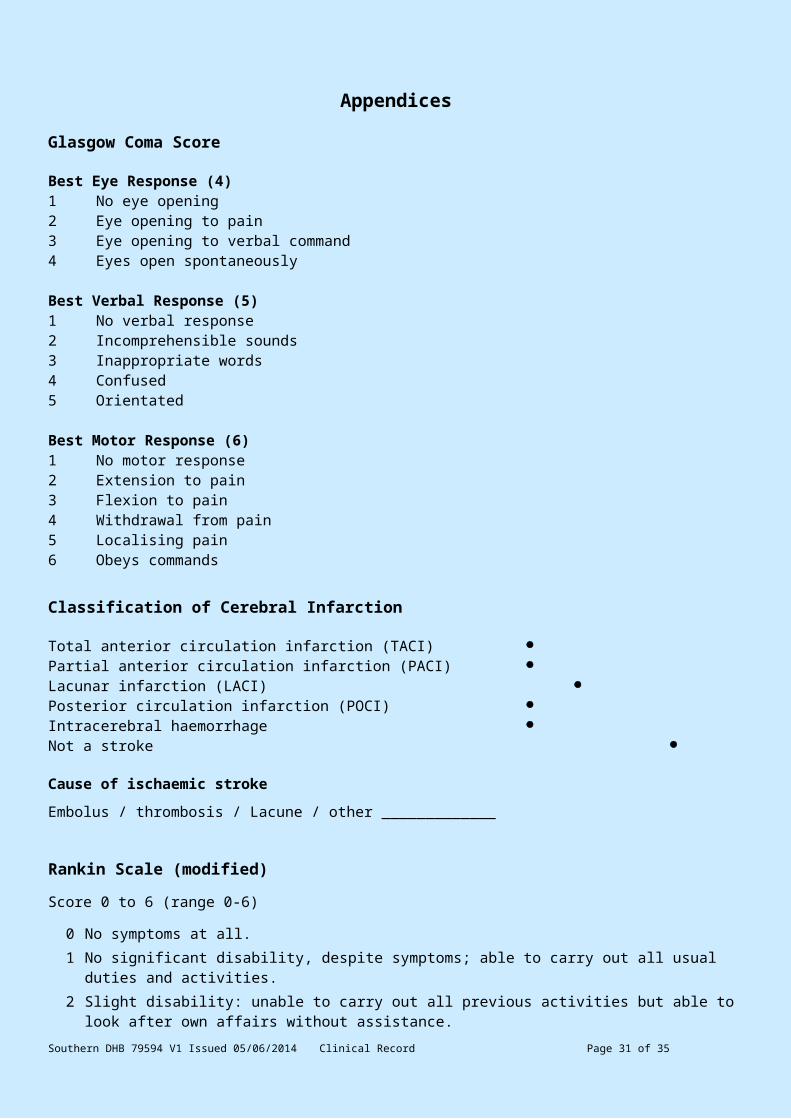
Glasgow Coma Score
Best Eye Response (4)1 No eye opening2 Eye opening to pain3 Eye opening to verbal command4 Eyes open spontaneously
Best Verbal Response (5)1 No verbal response2 Incomprehensible sounds3 Inappropriate words4 Confused5 Orientated
Best Motor Response (6)1 No motor response2 Extension to pain3 Flexion to pain4 Withdrawal from pain5 Localising pain6 Obeys commands
Classification of Cerebral Infarction
Total anterior circulation infarction (TACI) Partial anterior circulation infarction (PACI) Lacunar infarction (LACI) Posterior circulation infarction (POCI) Intracerebral haemorrhage Not a stroke
Cause of ischaemic stroke
Embolus / thrombosis / Lacune / other _____________
Rankin Scale (modified)
Score 0 to 6 (range 0-6)
0 No symptoms at all.1 No significant disability, despite symptoms; able to carry out all usual duties and activities.2 Slight disability: unable to carry out all previous activities but able to look after own affairs without
assistance.3 Moderate disability: requiring some help, but able to walk without assistance.4 Moderately severe disability: unable to walk without assistance and unable to attend to own bodily
needs without assistance.5 Severe disability: bedridden, incontinent and requiring constant nursing care and attention.6 Dead.
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 29 of 31
Abbreviated Mental Test Score
Question ScoreWhat is your age? (1 point)What is the time to the nearest hour? (1 point)Give the patient an address, and ask him or her to repeat it at the end of the test. (1 point)What is the year? (1 point)What is the name of this hospital? (1 point)Can the patient recognise two persons (the doctor, nurse, home help, etc? -1 point)What is your date of birth? (day and month is sufficient - 1 point)In what year did World War I begin? (Other dates can be used, with a preference for dates some time in the past. – 1 point)Name the present monarch or prime minister. (Or alternatively, the question "When did you come to New Zealand? " has been suggested – 1 point)Count backwards from 20 down to 1. (1 point)Total
Co-ordination Assessment
R UL finger–nose rapid alternating movement Normal AbnormalL UL finger–nose rapid alternating movement Normal AbnormalR LL heel–shin Normal AbnormalL LL heel–shin Normal AbnormalTandem walking Normal AbnormalGait Normal AbnormalBalance sitting Normal Abnormal Standing Normal Abnormal
Cranial Nerve Testing
II - Visual fields Normal AbnormalIII, IV & VI - PERLA Yes No Gaze palsy No Yes Diplopia No Yes Ptosis (R) (L) No Yes Nystagmus No YesV - Facial sensation Normal AbnormalV – Motor functionVII - Facial movements Normal AbnormalVIII - Hearing Normal AbnormalIX, X - Palatal movement Normal Abnormal Cough Strength
Normal Abnormal
XII - Tongue movements Normal Abnormal
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 30 of 31
Power Assessment
o 0: No contraction; paralysis o 1: Trace of contraction
o 2: Moves if gravity is eliminated
o 3: Moves against gravity
o 4: Moves against gravity and against some resistance
o 5: Normal strength
Required Pulses
Pulses R L
Carotids
Radial
Femoral
Popliteal
Post tibial
Dorsalis pedis
0 = pulse absent1 = faint / reduced2 = normal
Southern DHB 79594 V1 Issued 05/06/2014 Clinical Record Page 31 of 31











![Thrombolysis ImPlementation in Stroke (TIPS): evaluating the ...€¦ · stroke [6] and 62% of these reporting their stroke as their main disabling condition [6]. Stroke was the under-lying](https://img.pdfslide.us/doc/110x75/6079039cc75a7c5ba47f2235/thrombolysis-implementation-in-stroke-tips-evaluating-the-stroke-6-and.jpg)