Embed Size (px)
Citation preview
CHEST CONDITIONS
Thromboembolic Disorders: Guidancefor Return-to-PlayPatrick J. Depenbrock, MD
Abstract:Venous thromboembolism (VTE) is a major cause of morbidity andmortality. Treatment for VTE in athletes is similar to nonathletes. Earlytreatment of deep venous thrombosis (DVT) with bed rest and antico-agulation has given way to anticoagulation with early mobilization.Thrombolysis, preferably catheter-directed thrombolysis (CDT), may beused in select patients with upper extremity DVT (UEDVT). Surgicalprocedures should be reserved for those athletes with UEDVT who failinitial therapy. Compression devices are advocated for the treatment ofpostthrombotic symptoms (PTS) in lower extremity DVT (LEDVT) andUEDVT. Athletes with DVT should be encouraged to start a gradual re-turn to activities of daily living (ADD the day they begin anticoagulationtherapy. A structured return-to-training program with progressive in-crease in intensity can begin shortly after ADL mastery, provided theathlete is monitored carefully for recurrence of VTE. Athletes shouldnot engage in contact or collision sports until anticoagulation therapy iscomplete.
disorders in competitive athletes. Whileanticoagulation treatment guidelinesare well established for DVT, no return-to-play guidelines currently exist forathletes with venous thrombosis. Addi-tionally, no randomized controlled trials(RCT) or large cohort studies exist thatdocument the safe timing of exercise inthe DVT recovery process. This articlediscusses the evidence for safe return-to-exercise and competition for athleteswith DVT.
INTRODUCTIONDeep venous thrombosis (DVT) occurs annually in one
in 1000 people among the general U.S. population (6,8,13).DVT, with its associated complications, is a significantsource of morbidity and mortality. While physical activityand exercise appear to be protective against thromboem-bolic disorders, case reports of DVT in atbletes do exist (1).Examples from published literature include lower extremityDVT (LEDVT) in triathletes (19,25), soccer players (6), run-ners (13), and a military cadet (8), as well as cases of upperextremity DVT (UEDVT) in football linemen (23), weightlifters (13), and baseball pitchers (9). Despite case reports, noestimates are available for the incidence of thromboembolic
Primary Care Sports Medicine Faculty, Family Medicine ResidencyClinic, Carl R. Darnall Army Medical Center. Fort Hood. TX
Address for correspondence: Patrick J. Depenbrock, MD,Primary Care Sports Medicine Faculty. Fannily Medicine Residency Clinic,Carl R. Darnall Army Medical Center, 3600Ó Darnall Loop, Fort Hood.TX 76544 (E-mail; [email protected]).
1537-890X/1002/78-83 'Current Sports Medicine Reports iCopyright © 2011 by the American College of Sports Medicine
EPIDEMIOLOGYDVT affects more than 250,000 peo-
ple in the United States each year. Atleast 116,000 people are diagnosed withtheir first DVT each year (8). The esti-
• ~ mated incidence of DVT from all causesis 0.5 to 1.6T000~^ year~\ a number
that may be underestimated because of tbe number ofasymptomatic DVT and inaccuracies of clinical diagnosis (6).In the general population, the majority of DVT occur in thelower extremity. UEDVT is rare, occurring in approximately2100,000"^ personsyr"^ but is the most common vascularcondition among athletes (8).
Delayed presentation with DVT is not uncommon. Morethan 50% of outpatients diagnosed with DVT wait at least3 d before seeking medical attention (8). Complications ofDVT include death, pulmonary embolus (PE), recurrentDVT, and posttbrombotic syndrome (PTS). Morbidity andmortality can be bigh. One to five percent of patients pres-enting witb DVT will die from all-cause complications,mainly pulmonary embolism (25). In one study, 30% ofpatients presenting with their first DVT died within 30 d(8). Up to 50% of patients with DVT develop a PE (2).Despite optimal anticoagulant therapy, DVT symptoms suchas leg swelling can take up to several weeks to subside. Asmany as 40% of patients with DVT develop PTS, symptomsof which include cbronic leg pain, leg heaviness, leg swell-ing, and leg cramping aggravated with standing and allevi-ated with recumbence and elevation (21). PTS usually occursin the first 6 months following DVT diagnosis, but its ef-fects can last for years (27). Approximately 20% to 50% ofpatients witb LEDVT and 1Í% to 25% of patients with
78 Volume 10 " Number 2 • March/April 201 1 Thromboembolic Disorders
UEDVT develop PTS (6,9,10,23). PTS can be difficult todistinguish from recurrent occult thrombosis. The severity ofsymptoms may vary over time, and the most extreme mani-festation is venous ulcers of the lower leg.
PATHOPHYSIOLOGYThrombosis development is summarized by Virchow's
Triad of endothelial injury, blood stasis, and increased bloodviscosity. These three clot-predisposing factors initiate a cas-cade of procoagulant reactions that culminate with the for-mation of a thrombus. Endothelial injury has been highlightedas a primary factor in case reports of athletes with LEDVTinvolving acute traumatic knee dislocation and repetitivecyclist leg motion over a bicycle scat (6,8,13). Muscle hyper-trophy impinging on blood vessels, causing both blood stasisand endothelial injury, has been implicated in both LEDVTand UEDVT (6,8,9,13,23). Compression of the subclavianvein by cervical ribs, clavicular anomalies, and musculofas-cial bands also have been reported in cases of UEDVT (alsotermed "effort thrombosis" or Paget Schroctter Syndrome).Increased blood viscosity, traditionally implicated in patientswith hypercoagulable disorders, also plays a role in patientswith erythrocytosis and marked dehydration (13).
RISK FACTORSStandard risk factors for DVT are immobilization, preg-
nancy, recent surgery, malignancy, older age, smoking, hyper-coagulable states, connective tissue disorders, sex steroidadministration, severe dehydration, and major trauma (6,13).Competitive athletes often arc placed under conditions wherethey are exposed to several risk factors. These risk factorscan include orthopedic trauma, postinjury immobilization,frequent and prolonged travel, hemoconccntration after exer-tion, and polycythemia as seen with altitude training andexogenous Epo administration (13). While cast immobiliza-tion, hypoxic training, air travel, doping, misuse of nutri-tional supplements, and pathologic training potentially maycontribute to an increased risk of thrombosis, there is nostrong evidence to suggest that these factors clearly predis-pose the competitive athlete to thrombosis (1,10,13). Casereports have described athletes presenting with UEDVT afterpitching and following heavy upper-body workouts involv-ing repetitive arm abduction (9,23). Literature also describesathletes who presented with LEDVT following poplitealcontusion, car rides longer than 3 h, and elective abortion(6,8,13). However, there is no consensus that elite athletesas a whole are at higher risk for venous thromboembo-lism (VTE). More study is needed.
CLINICAL PRESENTATIONPublished case reports describe athletes presenting with
DVT following heavy bouts of exertion, after competitiontravel, and orthopedic injury sustained during competition(6,13,19,23,25). Some cases have reported DVT in athletesfollowing only mild to moderate activity (6). Patients withVTE typically present with complaints of limb edema andpain that is increased with provocative maneuvers. Low-grade fever, venous distension, increased limb circumfer-ence, extremity cyanosis, and tender palpable cords maybe noticed (6,7,11,23).
DIAGNOSISClinical examination has low sensitivity (11%) and a low
predictive value (25%) for DVT; however, it has demon-strated moderate to high specificity (76%-85%) (8). His-tory and physical exam findings alone have a predictivevalue of only 15% (18). Clinical prediction algorithms,which rely on the initial risk stratification of athletes basedon pretest probability, have been developed to facilitate thediagnosis of VTE (9a). Pretest probability of DVT may beestimated by a well-validated clinical prediction rule, such asthe Wells model, which takes into account the clinical fea-tures of active cancer (1 point), lower extremity paralysis,paresis, or immobilization (1 point), recent surgery with bedrest for 3 d (1 point), localized deep vein tenderness (1 point),full length leg swelling (1 point), unilateral calf swelling>3 cm (1 point), pitting edema (1 point), collateral superficialveins (1 point), and probable alternative diagnosis (—2 points)(26). A score of zero is considered low risk, while a score ofone point or higher is considered moderate or high. Athleteswith a moderate to high probability should undergo duplexvenous ultrasound with compression to rule out LEDVT.Athletes with a low pretest probability may be screened firstwith a highly sensitive D-dimer assay. DVT is ruled out inlow-risk athletes with a negative D-dimer assay. Those low-risk athletes with a positive D-dimer must have DVT ruledout via compression duplex ultrasound (18). Ultrasound isthe initial test of choice because it is noninvasive, and it hashigh sensitivity (93% for proximal LEDVT, 96% for UEDVT)and specificity (98% for proximal LEDVT, 93.5% forUEDVT) in the investigation of peripheral DVT (14,17). Ifinitial ultrasound results are negative and DVT is stronglysuspected, ultrasound should be repeated in 3 to 7 d (18).Additionally, computed tomography (CT) venography (sen-sitivity 89%-100%; specificity 94%-100%) or magneticresonance (MR) angiography (sensitivity 100%; specificity100%) can be used to confirm the diagnosis (13,14,18).
TREATMENTLEDVT
Anticoagulation remains the mainstay of VTE therapywhether the patient is a competitive athlete or a member ofthe general population. It maintains the patency of venouscollaterals, reduces thrombus propagation, and reduces theincidence of thrombus embolization (11,13). Anticoagu-lation is begun with subcutaneous low molecular weightheparin (LMWH) or unfractionated heparin (UEH), andconcurrent initiation of a vitamin K antagonist (VKA) likewarfarin. LMWH or UEH is continued for at least 5 d anddiscontinued once a therapeutic international normalizedratio (INR) range of 2.0 to 3.0 has been achieved for 24 h(8). In patients with DVT, the dose of VKA should beadjusted to maintain an INR range of 2.0 to 3.0 (target of2.i) for all treatment durations. Eor patients with DVTsecondary to a transient risk factor, anticoagulation withVKA is continued for 3 months (11). Patients with unpro-voked (i.e., idiopathic) DVT should be anticoagulated witha VKA for at least 3 months, then undergo risk-to-benefitratio evaluation for long-term therapy. Patients with a firstunprovoked VTE that is a proximal DVT, and in whomrisk factors for bleeding are absent and for whom goodanticoagulation monitoring is achievable, should undergo
www.acsm-csmr.org Current Sports Medicine Reports 7 9

long-term anticoagulation when this is consistent withpatient preference. For patients witli a first unprovoked distalDVT, 3 months of anticoagulation is sufficient (11). Inpatients with extensive acute proximal DVT {e.g., iliofem-oral DVT with symptoms <14 d) who have a low bleedingrisk, CDT followed by balloon angioplasty and stent place-ment may be used to reduce acute symptoms and post-thrombotic morbidity, provided adequate expertise andresources are available (11).
UEDVTAlthough no RCT have evaluated the use of anticoagula-
tion for the initial treatment of UEDVT, several small pro-spective cohort studies have reported low rates of recurrentDVT, PE, and major bleeds using treatment protocols forUEDVT similar to those for patients with LEDVT (11,13,23).Thus, for patients with acute UEDVT, the American Collegeof Chest Physicians (ACCP) recommends anticoagulationtreatment as described for LEDVT. Although some studiesreport good success of thrombolytic therapy in establishingearly and maintaining late venous patency, the overall qual-ity of evidence remains low (11). It has been suggested thatcatheter-directed thrombolysis (CDT) may reduce PTS in ath-letes with UEDVT. It also has been ¡suggested that CDT mayyield higher rates of clot resolution and reduces risk of seri-ous bleeding compared with systemic thrombolysis (11,13).However, the largest prospective study examining CDTreported a substantial follow-up recurrence rate of 23%(11). More study is needed to determine whether thromboly-tic therapy is superior to anticoagulation in important clinicalend points such as PE, recurrent VTE, bleeding, and PTS. TheACCP recommends against routine use of systemic or CDTtherapy for most patients with UEDVT. However, in selectpatients with acute UEDVT who present with severe symp-toms of recent onset {i.e., less than 7 d) and who pose a lowrisk of bleeding, CDT may be used for initial treatment, pro-vided appropriate expertise and resources are available (11).
SurgeryA number of surgical reviews have advocated for throm-
bolysis and angioplasty or stent placement followed by earlyor late surgical decompression of thoracic outlet syndrome.However, the data and safety of these approaches are limitedand derived from small, uncontrolled case series (9,11,23).For most patients with acute UEDVT, the ACCP recom-mends against the routine use of catheter extraction, surgicalthrombectomy, transluminal angioplasty, stent placement,staged approacb of lysis followed by interventional or sur-gical procedure, or superior vena cava filter placement. Theseinterventions, however, including surgical decompression incases of obstruction to thoracic vascular structures, may beconsidered in athletes with acute UEDVT and severe persis-tent symptoms who have failed conservative measures,including anticoagulation, structured physical therapy,weight loss, and nonsteroidal àntiinflammatory drugs(NSAID) (11,13).
Compression TherapyVenous compression devices long have been used in the
initial treatment of LEDVT, despite a paucity of evidence-
based literature to support their use. However, combined datafrom five trials over the last 10 yr suggest that the use of ve-nous compression reduces the incidence of PTS (2,10,15).Mild to moderate PTS decreased from 37% to 22%, andsevere PTS decreased from 12% to 5% (15). Overall, thenumber needed to treat with venous compression to preventone episode of PTS was five (15). Given the potentially debil-itating effects of PTS and the low potential for harm, theACCP recommends elastic compression stockings with anankle pressure gradient of 30 to 40 mm Hg for the preven-tion of PTS in patients with symptomatic proximal LEDVT.Compression therapy should be started as soon as possibleafter initiating anticoagulation and should be continued fora minimum of 2 yr. The treatment of PTS has been evaluatedonly in small or methodologically flawed trials. Based onlimited data, for patients with severe edema of the leg due toPTS, a course of intermittent pneumatic compression is sug-gested. For patients with mild edema, elastic compressionstockings are recommended (11).
Unlike lower extremity PTS, no controlled studies haveevaluated the effectiveness of elastic bandages or compres-sion sleeves in the prevention of upper extremity PTS. Thusthe routine use of elastic compression is not recommendedfor the prevention of PTS after UEDVT (11). Likewise fortreatment of upper extremity PTS, there exist no controlledstudies evaluating the effectiveness of elastic bandages orcompression sleeves. Anecdotal evidence, however, existssuggesting that patients with upper extremity PTS may derivesymptomatic relief from elastic bandages or compressionsleeves. Since their use is unlikely to cause harm, elastic ban-dages and compression sleeves are recommended in patientswith UEDVT who have persistent pain and edema (11).
PROGNOSIS/COMPLICATIONSPatients with VTE who undergo anticoagulation experi-
ence marked reductions in complications of VTE comparedwith those who remain untreated. Although radiographical-ly demonstrable clot lysis occurs in only 50% of anticoag-ulated patients (6), heparin (UFH or LMWH) significantlyreduces clot propagation, recurrent PE, and mortality (11).Mortality is high when anticoagulation is not used. Weight-appropriate unmonitored LMWH administered subcutane-ously is as effective and as safe as intravenous UFH. In fact,a recent analysis of 17 studies demonstrated that LMWHwas associated with fewer thrombotic complications andless major bleeding than UEH (11).
While many previously active patients with LEDVT at-tempt return to an active lifestyle, the long-term clinicaloutcomes often are complicated by persistent symptoms.One study found that 82% of patients with their first DVTsuffered from recurrent symptoms at a mean follow-up of6.6 yr (27). As previously mentioned, early ambulation andcompression therapy may mitigate these symptoms. The gen-eral knowledge concerning quality of life and burden of ill-ness in these patients is not known. More study is needed.
For patients with UEDVT, the overall prognosis is good.Of patients treated with thrombolysis, 80% to 90% returnedto a long-term asymptomatic state (13). It also appears thatthe prognosis with anticoagulation is favorable. In a liter-ature review of more than 2,500 patients, no superiority of
80 Volume 10 • Number 2 • March/April 2011 Thromboembolic Disorders
treatment was found between anticoagulation alone andthrombolysis for the general treatment of UEDVT (23).
In cases of external compression such as thoracic outletsyndrome or clavicular impingement, patients appear to ben-efit from acute correction of the anatomy. One study reportedthat all patients who underwent first rib resection were free oflong-term symptoms. Another study that examined UEDVTin elite baseball players found that four players who under-went first rib resection were able to return-to-play at previ-ous levels or better (11). While the overall data are positive,they are admittedly limited. Thus, it is suggested that surgicaldecompression be reserved for patients with severe persistentsymptoms after failing conservative therapy (11,23).
RETURN TO-ACTIVITY/PLAYTraditionally, patients with active DVT were hospitalized
and placed on bed rest for 7 to 10 d for fear of PE develop-ment in those who remain active. Soreness often precludeda return to daily activities in the first few weeks after DVT,especially in patients entering their sixth and seventh decadesof life. Thus, sedentary patients generally followed a gradual6-wk return to daily activities. Over the last two decades,however, this plan of care has been challenged, particularlyfor athletes. The early treatment of acute DVT with bed restand anticoagulation has given way to anticoagulation withearly mobilization (2,10,11,22).
Randomized trials and observational studies suggest thata majority of patients with DVT may begin ambulationwithin 24 hours of anticoagulation provided they haveadequate cardiopulmonary reserve and no clinical evidenceof active pulmonary embolism (2,10,21). Evidence suggeststhat these patients who ambulate early are not at higher riskfor developing PE, nor does it aggravate acute DVT symp-toms. In fact, early walking may reduce the risk of DVTextension, improve the resolution of DVT symptoms, andreduce the long-term symptoms of PTS. Provided thatimmediate rest, elevation, and anticoagulation have re-duced the initial edema and inflammation, it thus seemsprudent to permit, and even encourage, the athlete withDVT to engage in light ambulation as tolerated within thefirst 1 to 2 d after beginning anticoagulation.
While data for anticoagulation and early mobilizationexist, data guiding return to physical activity are sparse.There are no RCT investigating when it is safe to returnto sport following VTE. There are no expert consensus-derived clinical practice guidelines on the topic.
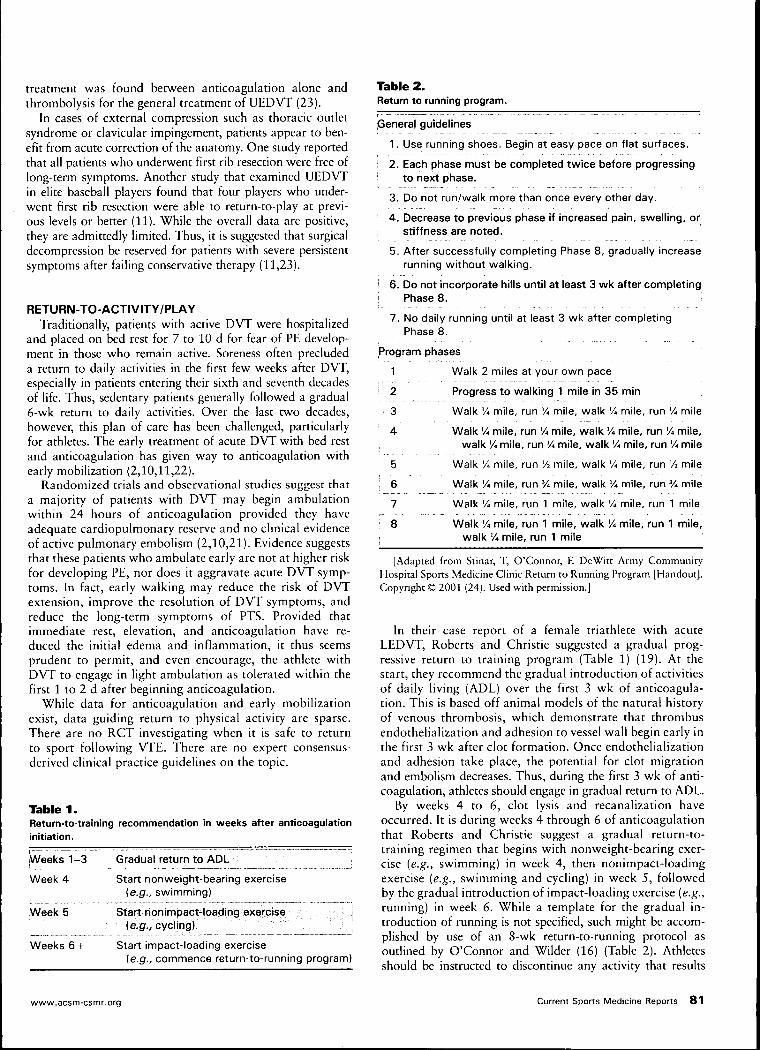
Table 1 .Return-to-training recommendation in weeks after anticoagulationinitiation.
Table 2.Return to running program.
Weeks 1-3
Week 4
Week 5
Weeks 6 +
Gradual return to ADL
Start nonweight-bearing exercise(e.g., swimming)
Start nonimpact-loading exercise(e.g., cycling)
Start impact-loading exercise(e.g., commence return-to-running program)
General guidelines
1. Use running shoes. Begin at easy pace on flat surfaces.
! 2. Each phase must be completed twice before progressing' to next phase.
3. Do not run/walk more than once every other day.
\ 4 . Decrease to previous phase if increased pain, swelling, or; stiffness are noted.
5. After successfully completing Phase 8, gradually increaserunning without walking.
I 6. Do not incorporate hills until at least 3 wk after completing] Phase 8.
7. No daily running until at least 3 wk after completingPhase 8.
Program phases
1 Walk 2 miles at your own pace
' 2 Progress to walking 1 mile in 35 min
• 3 Walk 'Ä mile, run % mile, walk 'A mile, run Vi mile
'• 4 Walk Yi mile, run % mile, walk 'A mile, run 'A mile,
, walk 'A mile, run % mile, walk 'A mile, run '/« mile
5 Walk 'A mile, run 'A mile, walk 'A mile, run 'A mile
: 6 Walk 'A mile, run % mile, walk 'A mile, run Vi mile
7 Walk % mile, run 1 mile, walk 'A mile, run 1 mile
: 8 Walk 'A mile, run 1 mile, walk 'A mile, run 1 mile,j walk 'A mile, run 1 mile
[Adapted from Stinar, T, O'Connor, R DeWitt Army CommunityHospital Sports Medicine Clinic Return to Running Program [Handout].Copyright® 2001 (24). Used with permission.)
In their case report of a female triathlete with acuteLEDVT, Roberts and Christie suggested a gradual prog-ressive return to training program (Table 1) (19). At thestart, they recommend the gradual introduction of activitiesof daily living (ADL) over the first 3 wk of anticoagula-tion. This is based off animal models of the natural historyof venous thrombosis, which demonstrate that thrombusendothelialization and adhesion to vessel wall begin early inthe first 3 wk after clot formation. Once endothelializationand adhesion take place, the potential for clot migrationand embolism decreases. Thus, during the first 3 wk of anti-coagulation, athletes should engage in gradual return to ADL.
By weeks 4 to 6, clot lysis and recanalization haveoccurred. It is during weeks 4 through 6 of anticoagulationthat Roberts and Christie suggest a gradual return-to-training regimen that begins with nonweight-bearing exer-cise (e.g., swimming) in week 4, then nonimpact-loadingexercise (e.g., swimming and cycling) in week 5, followedby the gradual introduction of impact-loading exercise (e.g.,running) in week 6. While a template for the gradual in-troduction of running is not specified, such might be accom-plished by use of an 8-wk return-to-running protocol asoudined by O'Connor and Wilder (16) (Table 2). Athletesshould be instructed to discontinue any activity that results
www.acsm-csmr.org Current Sports Medicine Reports 8 1
in return of symptoms or signs and report any blood loss orbruising. While on warfarin, athletes will need weekly INRlabs until a stable INR has been reached, at which point labmonitoring can be performed on a rnonthly basis (11).
Individuals with acute VTE should not participate in colli-sion or contact sports. Individuals in noncontact sports mayparticipate after appropriate counseling, unless that sport isa suspected cause for VTE or has additional environmentalrisks (e.g., SCUBA diving) (11).
Those with UEDVT who are determined to have an under-lying cause for thrombus should not participate in aggravat-ing activities until any structural abnormalities have beencorrected (13).
If individuals have completed a course of anticoagulationand a hypercoagulability laboratory evaluation (as neededfor a positive family history of VTE or personal history ofrecurrent idiopathic VTE) is negative, return-to-play withgradual increase in intensity is recommended with carefulmonitoring for recurrent VTE and management of PTS.Strong recommendations should be given to the athleteabout the possible instigating factors that may have led tothe initial event so that appropriate preventative measurescan be instituted (13).
PREVENTIONMultiple studies have demonstrated the effectiveness of
graduated compression stockings in the prevention of DVTin hospitalized patients (20). The study of graduated com-pression stockings in athletes is limited to a few small tread-mill studies of healthy runners. Two studies found nosignificant physiologic benefit, while a third found that run-ning performance was improved at anabolic and metabolicthresholds (4,5,12). Significantly decreased incidence of de-layed onset muscle soreness and greater subjective comfortin runners wearing low-grade compression stockings werebenefits noted in other studies (3,4). None of the studiesinvolving athletes, however, evaluated the role of compres-sion stockings in the primary prevention of DVT.
The role of exercise in the prevention of VTE has been thesubject of much scrutiny. Chronic sports participation orendurance training is associated with overall decrease in riskof venous thrombosis and a reduction in various markersof coagulation. Light to moderate exercise thus is likely tobe of benefit. However, there is enhanced platelet reactivityand coagulation in response to vigorous exercise (1). Sincevigorous exercise is an integral part of the elite athlete'straining regimen, some suggest that this may place elite ath-letes at a higher risk for thrombosis.
While there is not conclusive evidence that properly hy-drated athletes have a decreased iricidence of VTE, there isevidence of increased incidence of VTE in hemoconcentratedor polycythemic individuals. When combined with the obser-vation that there is enhanced platelet reactivity and coagu-lation in response to vigorous exercise, it would seem prudentto recommend sufficient oral intake, particularly for thoseengaging in high-intensity workouts.
Those who suffer competition injury requiring immobi-lization greater than 3 d should receive early prophylac-tic anticoagulation in addition tOi physical antithromboticmeasures (13). Eor athletes with a history of DVT using air
travel, LMWH should be considered for prevention of DVTrecurrence. In addition, Eichner has recommended eightstrategies for prevention of clots. These include sitting in seatsthat allow leg extension, hourly aisle walks, not crossinglegs, wearing of loose clothing, hydration with water or juices,consuming low-fat meals, fidgeting, and thinning blood withaspirin or LMWH if prone to clotting (7).
CONCLUSIONVenous thromboembolism can occur in athletes follow-
ing strenuous exertion, prolonged air or automobile travel,and orthopedic injury. While it is not known whether eliteathletes are at higher risk for VTE, the nature of their train-ing and competition schedules exposes them to various riskfactors. A high index of suspicion is needed to diagnosisVTE in the athlete, as many patients do not exhibit hall-mark signs, and the rates of short- and long-term compli-cations are high (6,8,18). Those athletes diagnosed withVTE should undergo anticoagulation therapy. Selected casesmay warrant alternate additional therapies or procedures.Compression therapy and rapid mobilization are crucial toshorter recovery times and decreased long-term complica-tions. Return-to-play should follow a structured program ofgradual increased activity as tolerated by the patient. Morestudy, preferably RCT or large cohort studies, is needed toexamine the safe timing of return-to-play in the VTE recov-ery process.
References1. Adams M, Williams A, Fell J. Exercise in the fight against thrombosis:
friend or foe? Semin. Thromb. Hemost. 2009; 36(3):261-8.
2. Aldrich D, Hunt DP. When can the patient with deep venous thrombosisbegin to ambulate? Phys. Ther. 2004; 84(31:268-73.
3. Ali A, Caine M, Snow B. Graduated compression stockings: physio-logical and perceptual responses during and after exercise. J. SportsSei. 2007; 25(4):413-9.
4. All A, Creasy R, Edge J. Physiologic effects of wearing graduatedcompression stockings during running. Eur. J. Appl. Physiol. 2010;109(6):1017-25.
6. Berry M, Bailey S. Simpkins L, TeWinkle J. The effects of elastic tightson the post-exercise response. Can. J. Sport Sei. 1990; 16(41:244-8.
6. Echlin P, Upshur R, McKeag D, Jayatilake H. Traumatic deep veinthrombosis in a soccer player: a case study. Thrombosis J. 2004; 2:8.
7. Eichner R. Athletes in airplanes: some are born to clot. Sports Med. Dig.2000; 22:140-42.
8. Fink M, Stoneman P. Deep vein thrombosis in an athletic military cadet.J. Orthop. Sports. Phys. Ther. 2006; 36(9):386-97.
9. Hurley W, Comins S, Green R, Canizzaro J. A traumatic subclavian veinthrombosis in a collegiate baseball player. J. Athl. Train. 2006; 4112):198-200.
9a. Institute for Clinical Systems Improvement. Venous thromboembolismdiagnosis and treatment. 10th ed., Feb 2010. Deep vein thrombosisIDVT) diagnosis algorithm. Available at: http://www.icsi.org/venous_thromboembolism/venous_thromboembolism_4.html. Accessed March8,2011.
10. Kahn SR, Shrier I, Kearon C. Physical activity in patients with deepvenous thrombosis: a systematic review. Thromb. Res. 2008; 122(6);763-73.
11. Kearon C, Kahn S, Agnelli G, et al. Antithrombotic therapy for ve-nous thromboembolic disease: American College of Chest Physiciansevidenced-based clinical practice guidelines 18th edition). Chest. 2008;133:464-646.
12. Kemmler W, von Stengel S, Kockritz C, et al. Effect of compressionstockings on running performance in men runners. J. Strength Cond.Res. 2009; 23(1):101-6.
82 Volume 10 • Number 2 • March/April 2011 Thromboembolic Disorders
13. Meyering C, Howard T. Hypercoagulability in athletes. Curr. SportsMed. Rep. 2004; 3l2);77-83.
14. Miller JC. Diagnosis of lower extremity deep venous thrombosis. Radiol.Rounds. 2005; 3(5): 1-3.
15. Musani MH, Matta F, Yaekoub AY, et al. Venous compression for pre-vention of postthrombotic syndrome; a meta-analysis. Am. J. Med.2010; 123(8):735-40.
16. O'Connor F, Wilder R. Textbook of Running Medicine. New York:McGraw-Hill; 2001. p. 696.
17. Prandoni P, Polistena P, Bernardi E, ei al. Upper-extremity deep veinthrombosis: risk factors, diagnosis and complications. Arch. Intern.Med. 1997; 157:57-62.
18. Ramzi DW, Leeper KV. DVT and pulmonary embolism: part I — diagnosis.Am. Fam. Phys. 2004; 69(12):2829-36.
19. Roberts WO, Christie DWI. Return to training and competition after deepvenous calf thrombosis. Med. Sei. Sports Exerc. 1992; 24(11:2-5.
20. Sachdeva A, Dalton M, Amaragiri S, Lees T. Elastic compressionstockings for prevention of deep vein thrombosis. Coch. Data. Syst.Rev. 2010; 7|7):CD001484.
21 . Shrier I, Kahn SR. Effect of physical activity after recent deep venousthrombosis: a cohort study. Med. Sei. Sports Exerc. 2005; 37(4):630-4.
22. Shrier I, Kahn SR, Steele RJ. Effect of early physical activity on long-term outcome after venous thrombosis. Clin. J. Sport Med. 2009;19(6):487-93.
23. Snead D, Marberry K, Rowdon G. Unique treatment regimen for effortthrombosis in the nondominant extremity of an overhead athlete. J. Athl.Train. 2009; 44(1):94-7.
24. Stinar T, O'Connor F. DeWitt Army Community Hospital Sports Medi-cine Clinic Return to Running Program IHandoutl. 2001.
25. Tao K, Davenport M. Deep venous thromboembolism in a triathlete.J. Emerg. Med. 2010; 38(3):351-53.
26. Wells PS, Anderson DR. Value of assessment of pretest probability ofdeep-vein thrombosis in clinical management. Lancet. 1997; 350(9094):1795-98.
27. Ziegler S, Schillinger M, Maca T, Minar E. Post-thrombotic syndromeafter the primary event of deep venous thrombosis 10 to 20 years ago.Thromb. Res. 2001; 101:23-33.
www.acsm-csmr.org Current Sports Medicine Reports 8 3
Copyright of Current Sports Medicine Reports is the property of American College of Sports Medicine and its
content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's
express written permission. However, users may print, download, or email articles for individual use.

Hypercoagulability in AthletesChristopher Meyering, DO and Thomas Howard, MD*
Address*DeWitt Army Community Hospital, 9051 Farrell Road, Suite GC 11, Ft. Belvoir, VA 22060, USA. E-mail: [email protected]
Current Sports Medicine Reports 2004, 3:77–83Current Science Inc. ISSN 1537-890xCopyright © 2004 by Current Science Inc.
IntroductionAn active 42-year-old man was diagnosed with a lowerextremity deep vein thrombosis (DVT) and appropriatelyanticoagulated. He asked when and how to return to hisnormal physical activity; he did so and anticoagulation wasdiscontinued 3 months later. Soon after, he was diagnosedwith a recurrent DVT, and subsequently found to be pro-tein S-deficient. In another case, an active 55-year-old manwas diagnosed with atrial fibrillation and placed on long-term warfarin therapy. He asked if it was safe to run amarathon while on warfarin.
These two vignettes highlight questions about the man-agement of coagulation and coagulation disorders in athletes.Does athletic competition increase an athlete’s thromboticrisk? Who should we screen and how? When can athletesreturn to activity and what limitations should be advised?
Venous thrombosis is a common disorder that affectsone in 1000 per year [1] and can be associated with signifi-cant sequelae. Embolization is a significant risk and theacute symptoms of pain and swelling can be debilitating.Post-thrombotic syndrome may occur in as many as 60%of patients with DVT [2] and presents as chronic pain,edema, induration, pigmentation, venectasia, varicosis,and venous ulcers.
Remembering Virchow’s triad of stasis, endothelialinjury, and hypercoagulability will help one identify riskfactors for thrombosis. Athletes, especially elite athletes,are placed under conditions in which they are exposed toseveral of these risk factors such as trauma, immobilizationafter injury, frequent travel, hemoconcentration afterexertion, and polycythemia. Female athletes on oralcontraceptives have an added risk for thrombosis. Severalarticles [3–5] have been published regarding preventativemeasures for venous thromboembolism (VTE) in athletes,and multiple studies have outlined the most appropriatetreatment for an acute VTE [6••,7•,8•]. However, little hasbeen published regarding recommendations for athleteswho have had a VTE concerning activity and how theyshould be managed afterward.
Persons with a hypercoagulable disorder are at anadded risk for an acute thrombotic event. Activated proteinC (APC) resistance is the most common cause for heredi-tary thrombophilia and is most commonly associated witha factor V Leiden mutation (90%–95%) [9••]. Presence ofthis gene results in inability for APC to inactivate factors Vand VIII, which in turn leads to unchecked coagulation[9••]. Allele frequency in the general population of whiteEuropean subjects is 4%, but in nonwhite populations isextremely uncommon [9••]. The relative risk of thrombo-sis for carriers of the factor V mutation is thought to beincreased seven times for heterozygotes and 80 times forhomozygotes [10]. Another mutation involves a singlenucleoside transition in the gene for prothrombin (pro-thrombin 20210A mutation). This mutation results inapproximately 30% higher prothrombin levels in heterozy-gotes compared with healthy controls, which is presumedto be the mechanism for its thrombotic effects [11]. Preva-lence of this mutation among healthy controls has variedin studies from 0.7% to 6.0%, and its presence has beenassociated with a relative risk of thrombosis of 2.8 [12].This prothrombin 20210A mutation is uncommon in non-white populations [9••]. Antithrombin (AT) III, protein Cand S deficiencies are also associated with thrombophilia.Gene frequency in the population for AT III, and proteins
Risk factors for thromboembolism are well known, and athletes are placed under conditions that can result in exposure to several of these risk factors, which include travel, trauma, immobilization, hemoconcentration, and polycythemia. Presence of a genetic hypercoagulable disorder adds additional risk. Overall management is no different than in nonathletes. Thrombolysis is strongly recommended for upper extremity deep venous thrombosis (DVT) coupled with surgical decompression of obstructive structures if indicated. Thrombolytic therapy does not appear to be necessary for treatment of lower extremity DVT. Prevention of DVT with travel can be achieved through general techniques such as leg exercises, hydration, and loose fitting clothes. Aspirin before travel shows some benefits of protection, but individuals at higher risk may need low molecular weight heparin. Athletes should be screened during preparticipation physicals for thromboembolic risk. Individuals on anticoagulation therapy should not participate in collision or contact sports. Return to play with gradual increase in intensity is recommended with careful monitoring for recurrent venous thromboembolism and management of post-thrombotic symptoms.

78 Chest Conditions
C and S is 0.1%, 0.33%, and 0.5%, respectively. Protein Sdeficiency has been related to 1.4% to 7.5% of hypercoag-ulability cases and protein C deficiency to 1.4% to 8.6%[13]. AT III is associated with 0.5% to 4.9% [7•] of casesalthough the risk for thrombosis with this deficiency ishigher [14]. Hyperhomocysteinemia has been shown to bea risk for venous thrombosis and corresponds to an oddsratio of 2.5 when compared with healthy controls [9••].Elevated levels of factors VIII and XI have also been foundto result in a fivefold and 2.2-fold increased risk, respec-tively [9••], although the genetic relation of these elevatedlevels is being investigated. A study by Hilberg et al. [15]examined the prevalence of the main causes of hereditarythrombophilia in a German National athletic team andconcluded that gene frequencies for these disorders corre-sponded to the general population.
EtiologyThere are three major influences that predispose to throm-bosis: injury to the endothelium, alterations in blood flow,and alterations in the blood itself. Endothelial damageresults in local procoagulant functions [16]. Initial endo-thelial injury activates platelets, resulting in adhesion tosubendothelial collagen with von Willebrand’s factor,shape changes, and aggregation (interadherence) [17].These events lead to the release of several stored products,such as ADP and fibrinogen, and the synthesis of throm-boxane A2. The complex that is formed in turn activatesseveral coagulation factors in the intrinsic coagulationpathway. In addition, injured cells release tissue factor,which activates the extrinsic coagulation cascade. Both theintrinsic and extrinsic coagulation pathways entail a seriesof transformations of proenzymes to activated enzymes,ultimately resulting in formation of thrombin, whichconverts soluble fibrinogen into insoluble fibrin.
Several case studies have been published about the rela-tionship of thrombosis and exercise [17–21]. Primary upper-extremity deep venous thrombosis (UEDVT) is thought to berelated to trauma to the subclavian vein [22]. Heavy upperextremity exertion results in microtrauma to the axillo-subcla-vian vein leading to activation of the coagulation cascade[6••,22], and has been termed effort thrombosis or Paget-Schroetter syndrome. Compression and stress of the subcla-vian vein can also develop in athletes with hypertrophiedmuscles who do heavy lifting or repetitively abduct their arms[6••]. Similar motions are commonly seen in rowing, wres-tling, weight lifting, baseball, softball, gymnastics, basketball,hockey, tennis, golf, football, handball, squash, boxing,swimming, volleyball, and parachute jumping [6••,23].Additional risk factors for UEDVT are the presence of cervicalribs, long transverse processes of the cervical spine, musculo-fascial bands, and clavicular or first rib anomalies, which allfavor subclavian vein compression [24].
Several case reports of lower extremity thrombosis inathletes have also been published [21,25]. Mechanisms of
injury to endothelium include knee dislocation, ischemiafrom muscle hypertrophy, and repetitive microtrauma suchas cyclist leg motion over seats [26]. Muscle hypertrophy canalso lead to compression of venous structures, leading tostasis. Other risks for lower extremity thrombosis includeinjury associated with surgery or cast immobilization.
Risk FactorsHemoconcentrationThe significance of the contribution of hemoconcentrationto thrombotic events is undetermined, although anincrease in concentration has been demonstrated in severalstudies [26,27]. Adequate hydration during and afterexercise decreases this effect. Because most hemoconcen-tration is short lived with exercise, it may not be significantunless combined with other thrombotic risk factors.
Injury and immobilizationRecent trauma has been demonstrated to be associatedwith a 13-fold increased risk of VTE [28] in a population-based study. A higher incidence has been associated withhead injury, lower extremity or pelvic fractures, and spinalcord injury. Even minor injuries resulting in minor traumato endothelium can result in thrombosis as seen withPaget-Schroetter syndrome [22].
Stasis can localize coagulation proenzymes makingthem more likely to be converted to enzymes [29].Meissner et al. [29] observed that patients with venousthromboembolism had a higher prevalence if immobilizedfor greater than 3 days. In addition they suggested in theirdiscussion that hypercoagulability might persist for at least1 month after injury after noting persistent elevations inmarkers for activated coagulation. However, their studysuggested that duration of immobilization and obesitywere the only significant predictors of thromboembolismin injured patients [29].
TravelAthletes are traveling longer distances to tournaments,matches or games. A recent case control study by Ferrari etal. [30••] examined subjects who had a VTE and comparedthem with controls. They found that a history of recenttravel by air, train, or car was found four times morefrequently in the VTE group. Most commercial aircraft arepressurized to about 8000 feet of altitude. This results inmild hypoxia that may be concerning in certain medicalconditions. Two studies by Bendz et al. [31,32] examinedthe association between acute hypoxia seen during air-plane flights and activation of coagulation and found thatmarkers of activated coagulation transiently increased bytwo- to eightfold when subjects were rapidly exposed to ahypoxic and hypobaric environment of 76 kPa. Travelduration longer than 4 hours within the previous 2months was also seen as an independent risk factor in15.5% of patients presenting with a VTE [33].

Hypercoagulability in Athletes • Meyering and Howard 79
ErythrocytosisTraining at high altitudes or simulating living in a high-altitude environment using modified hypoxic chambers isa technique used to increase the hemoglobin and hemat-ocrit, and possibly improve performance when competingat sea level. Multiple studies have demonstrated that thereis an increase in hemoglobin synthesis and a greaterconcentration in persons exposed to high-altitude environ-ments [32,34,35,36••]; however, there is little publishedregarding the effects of this high concentration. A study byJha et al. [36••], examined the incidence of stroke in ahigh-altitude area over several years. Although the subjectswere not elite athletes, they were young soldiers of armedforces serving at altitudes greater than 4270 m. Stroke inci-dence was 13.7 per 1000 in high altitude compared with1.05 per 1000 in low altitude, and 75% of cases were foundto have polycythemia [36••]. This supports the idea thaterythrocytosis may increase susceptibility to thrombus.
Multiple articles and commentaries have related theincreased viscosity effects of recombinant human erythropoi-etin (rhEpo) to stroke and death of athletes [37–39]. Berglundand Ekblom [40] investigated the effects rhEpo on blood pres-sure and found that rhEpo induced a significant increase insystolic blood pressure of 14 mm Hg during exercise.
Platelet adhesiveness and aggregability changes afterexercise Platelet adhesion to sites of endothelial injury isclosely followed by platelet aggregation (platelet interad-herence). Once the primary aggregation begins, thrombinis generated and the coagulation cascade is set in motion.Todd et al. [41] compared healthy older and younger menafter exercise and found that older men have an increase inthromboxane B2 levels 30 minutes after exercise, and maybe more predisposed to platelet activation. Another studyby Wang et al. [42] examined the difference that moderateand strenuous endurance exercise has on platelet aggrega-tion and adhesiveness. In their active healthy group, plate-let adhesiveness and aggregation were enhanced by severeexercise and aggregation was decreased by moderate exer-cise. However, Ahmadizad and El-Sayed [43] state that theevidence for this increase in activation and function is notclear, as there have been studies that show an increase, adecrease, or no significant change after endurance exercise.
Hormonal therapyOral contraceptives are commonly used not only for birthcontrol but also for medical management of amenorrheaand osteoporosis in the female athlete triad. Venousthrombosis has become less common with low-dosepreparations of oral contraceptives, but their use still addsa significant fourfold increased risk. For athletes with agenetic thrombophilia the risk is even higher. Vanden-broucke et al. [44] found that women who used low-dosecontraceptives and had a heterozygous factor V Leidenmutation had a 30-fold increased risk for thrombosis andthose with a homozygous mutation had an estimated 100-fold increased risk.
ScreeningInitial evaluation of athletes during preparticipation exami-nations should focus on thrombotic episodes in familymembers or any personal history of thrombotic events. Thehistory should identify the use of prothrombotic drugs suchas oral contraceptives, hormone replacement therapy, or epo-gen, and unusual training practices such as high-altitudetraining. For athletes with a positive personal or family his-tory of a thromboembolic event, it may be reasonable toreview records for a prior evaluation [9••]. Appropriate eval-uation for high-risk thrombotic states should include AT III,protein C, and protein S levels, in addition to presence ofantiphospholipid antibodies, factor V Leiden, and prothrom-bin 20210A mutations and homocysteine levels [7•,9••].Any laboratory evaluation that has not been done should beordered. Routine screening for athletes without any signifi-cant history is not recommended. Hilberg et al. [15] state intheir discussion of APC resistance that screening elite athletesis necessary to identify individuals at high risk so that mea-sures for preventing thrombosis can be taken. This recom-mendation stems from the prevalence of APC resistance inthe study group that was consistent with the prevalence inthe general white population coupled with the previouslymentioned added risks. Individual consideration should bemade based upon the ethnicity of the athlete, as theincidence of prothrombin 20210A and factor V Leiden innonwhite populations is low [7•,9••].
DiagnosisTypical complaints of patients with VTE include edemaand discomfort in the affected limb, and increased painwith provocative maneuvers. Physical examination mayshow low-grade fever, cyanosis in the limb, a tender palpa-ble cord, edema with increased limb circumference, andpossibly venous distention. Objective testing should beperformed to confirm or exclude the diagnosis. Duplexultrasound is the initial test of choice because it is noninva-sive and has a high sensitivity and specificity for peripheralDVT [6••,45]. If ultrasound results are negative and DVT isstrongly suspected, further studies include venography andmagnetic resonance angiography [6••].
ManagementThe mainstay of therapy is anticoagulation. Anticoagulationmaintains the patency of venous collaterals, reduces propa-gation of the thrombus, and reduces the incidence of embo-lic phenomenon [6••,7•,9••,46]. Initial medications shouldbe either low molecular weight heparin (LMWH) or unfrac-tionated heparin with concurrent initiation of warfarin[6••,7•,9••]. INR should be maintained between 2.0 and 3.0[47••]. Patients with first episode of VTE that have a revers-ible or time-limited risk factor should be treated for at least 3months, whereas those with an idiopathic VTE should betreated for 6 months. Patients with continuing risk factors or

80 Chest Conditions
with recurrent VTE should be treated for 12 months orlonger. Anyone with three or more episodes of VTE should beon indefinite anticoagulation [47••]. Once medications havebeen started and symptoms of pain and swelling arecontrolled, patients may ambulate [48].
In athletes with UEDVT, it has been recommended thatthrombolysis be strongly considered to prevent the long-term effects of post-thrombotic syndrome manifested bychronic arm and hand aching and swelling [6••,7•,46,49,50•]. Catheter-directed thrombolysis is recommendedover systemic thrombolysis as it achieves higher rates ofcomplete clot resolution with lower doses of medicationand reduces the risk of serious bleeding [6••,51]. The timeof symptom onset to initiation of thrombolysis influencesthe success rate. The best success occurs if thrombolysis isbegun within 7 days of onset of symptoms [7•,8•,21,46],although longer times (up to 3 weeks) have also been suc-cessful [21,50•,51].
In lower extremity DVT, the use of thrombolytictherapy is controversial as most patients treated with onlyanticoagulants have uncomplicated courses. Thrombolyt-ics may be considered for patients without contraindica-tions who have significant swelling and symptoms [52]. Ifused, they should be started at the earliest opportunity.Conservative measures such as graduated compressionstockings have been shown to reduce the incidence of post-thrombotic syndrome in patients with lower extremityDVT [2], and may also be added.
If thoracic obstruction to vascular structures contributedto an UEDVT, further therapy involving conservative mea-sures versus decompression of the restriction may be neces-sary [6••,8•,46,49,50•,51]. Joffe and Goldhaber [6••] reporta preference of conservative therapy involving structuredphysical therapy, weight loss if needed, and nonsteroidal anti-inflammatory drugs rather than early surgical decompressionafter thrombolysis. If indicated, decompression involvessurgical resection of part of the first rib or clavicle or lysis ofdense adhesions around the subclavian vein [6••,51]. Theaim is to relieve positional pinching by the subclavius muscleand the lower fibers of the anterior scalene against the first rib[46]. The exact timing of when to perform the decompressionis still debated. Some advocate early decompression afterthrombolysis during the same admission [45,46], but mostcases are determined on the flow quality and severity ofresidual symptoms [8•,46,49]. Following decompression,subclavian stenting can also be performed for those athleteswith persistent venous strictures [49,50•], but their long-termeffectiveness has not been extensively studied. Stenting priorto decompression should not be attempted as positionalpinching can lead to damage of the stent and a high risk ofrecurrent thrombosis [46].
PrognosisA total of 80% to 90% of patients treated in the abovemanner for UEDVT returned to a long-term asymptomatic
state, so overall prognosis is good [21,45], although fail-ures have been reported in case studies [17,19]. Yilmaz etal. [8•] reported that all patients who underwent first ribresection were symptom free after long-term evaluation.DiFelice et al. [53] examined cases of effort thrombosis inelite baseball players and found that four players withUEDVT who underwent first rib resection were able toreturn to play at or above previous levels. Arko et al. [25]investigated 26 patients who had vascular complaints as aresult of various athletic competitions and found that 11 of14 patients with an arterial injury were able to return totheir prior level of competition, and 12 of 12 patients withUEDVT returned to their usual level of activity.
If the cause of the VTE is determined to be from a throm-bophillic disorder such as factor V Leiden, antiphospholipidsyndrome, AT III deficiency, or protein C or S deficiency pro-thrombin 20210A mutation the prognosis is not as clear. Therisk of primary or repeat embolism with these disorders canbe high [9••,13] as previously mentioned, althoughDe Stefano et al. [54] found that heterozygous carriers offactor V Leiden had no increase in recurrent thrombosis com-pared with controls. Individuals with more than one geneticdefect (ie, factor V Leiden and prothrombin mutation), withtwo or more spontaneous VTEs, life-threatening VTE, pres-ence of antiphospholipid antibody syndrome, or AT III defi-ciency should receive long-term anticoagulation according torecent recommendations [6••,13,54–56]. Two completedtrials have shown continued efficacy with full-dose warfarin(INR 2.0–3.0), although rates of major bleeding were highduring extended therapy [57•]. Recent studies examininglong-term, low-intensity warfarin therapy with INR of 1.5 to2.0 appears to be an effective method for preventing recurrentVTE [57•] and may be considered for athletes who travel, buttheir indication in patients with hypercoagulable states is notclear and is probably not recommended. In addition, a morerecent study comparing low-intensity therapy with conven-tional therapy found that conventional therapy was moreeffective in preventing recurrent VTE, and there was no reduc-tion in risk of clinically significant bleeding for patients usinglow-intensity therapy [58•].
PreventionThe key for preventing VTE is attention to general tech-niques to avoid clotting. Studies investigating a decreasedincidence of VTE in athletes who are properly hydratedcompared with those who are dehydrated were not foundin a literature search. However, evidence lends toward theincreased incidence of VTE with individuals who arehemoconcentrated as seen in individuals who are poly-cythemic; therefore, sufficient oral intake is recommended.
Individuals who are injured during competition andare subsequently immobilized should receive early pro-phylactic anticoagulation if rapid mobilization is notanticipated within 3 days, in addition to physical anti-thrombotic measures [10].

Hypercoagulability in Athletes • Meyering and Howard 81
Multiple studies have recommended the use of LMWH[3,4,15,31] for the prevention of venous thrombosis dur-ing airplane flights for those at an increased risk, but thecost is high. Aspirin may also show some benefits of pro-tection [59], but its effectiveness is much less than LMWH[31,59]. Hilberg et al. [3,4,15] have recommended in sev-eral publications the use of LMWH and/or leg exercisesduring flights. In addition, Eichner [5] has recommendedeight strategies for prevention of clots on flights, whichinclude sitting in seats that allow leg extension, hourlyaisle walks, not crossing legs, loose clothing, hydrationwith water or juices, low-fat meals, fidgeting, and thinningblood with an aspirin or LMWH if prone to clotting.
Athletes who participate in high-altitude training orutilize a hypoxic or altitude sleep tent should be warnedregarding their use and the increased risk of thrombo-embolism. These athletes should be monitored whileutilizing these devices by following the hemagram.
Clearance for ParticipationIn general, the guidance for clearing athletes to participate incompetition if a blood disorder is suspected or determinedhas been minimal [60]. Athletes that are found to have apositive family or personal history of VTE should be evalu-ated further prior to participation, as the risk for an event forthose with a genetic hypercoagulable disorder is high.
Individuals with an acute VTE on continued anticoagu-lation therapy should not participate in activities involvedwith collision or contact and strong recommendations onrisks of continuing limited contact activities should bemade. Individuals involved in noncontact sports mayparticipate after appropriate counseling unless that activityis a suspected cause for VTE, or has additional environ-mental risks (such as scuba diving). One case presentationby Roberts and Christie [61] listed a return-to-training regi-men for a triathlete with a calf DVT. Their suggestion wasreturn to activities of daily living over the first 3 weeks oftreatment, followed by the following gradual increase intraining intensity: Swimming for 1 week, then swimmingand cycling for 1 week, then gradual increase in running.Any activity that resulted in return of thrombosis symp-toms should be discontinued.
Those with UEDVT who are determined to have anunderlying cause for thrombus should not participate inaggravating activities until any structural abnormalitieshave been corrected.
If individuals have completed a course of anticoagula-tion and a hypercoagulability laboratory evaluation isnegative, return-to-play with gradual increase in intensityis recommended with careful monitoring for recurrent VTEand management of post-thrombotic symptoms. Strongrecommendations should be given to the athlete, however,about the possible instigating factors that may have led tothe initial event, so that appropriate measures for preven-tion can be instituted.
ConclusionsUsing these guidelines to manage our two scenarios, the 42-year-old man with the lower extremity DVT returned to activ-ities of daily living after several weeks of anticoagulation withno symptoms of thrombosis. He began physical activity start-ing with no impact, gradually increasing to previous levelsover several weeks with monitoring for any recurrence ofsymptoms. After completing 3 months anticoagulation, ahypercoagulable work-up was ordered. He had a recurrentDVT while awaiting results, and was found to be protein S-deficient, warranting life-long warfarin therapy. At thepatient’s request, his children were screened for protein Sdeficiency and one son was also deficient. This lead to coun-seling regarding choice of activities, management after injuryor surgery, and techniques to prevent VTE.
Our second patient with atrial fibrillation on long-termwarfarin therapy was cleared to participate in the marathonwith cautions about appropriate monitoring of his INR,and signs and symptoms of hemorrhagic complications.
Hypercoagulability and thromboembolic events are notrestricted to the nonactive population. Sports and primary careproviders should have a comfort level and a good understand-ing of these conditions and their relationship to the athlete’schosen activity so they can render appropriate advice aboutrestrictions, prophylaxis, and preventative measures.
AcknowledgmentThe authors thank Dr. E. Randy Eichner for his criticalreview and input for this article.
References and Recommended ReadingPapers of particular interest, published recently, have been highlighted as:• Of importance•• Of major importance
1. Goldhaber SZ: Epidemiology of pulmonary embolism and deep vein thrombosis. In Haemostasis and Thrombosis. Edited by Bloom AL, Forbes CD, Thomas DP, Tuddenham EG. New York: Chrurchill Livingstone; 1994:1327.
2. Brandjes DPM, Buller HR, Heijboer H, et al.: Randomised trial of the effect of compression stockings in patients with symp-tomatic proximal-vein thrombosis. Lancet 1997, 349:759–762.
3. Hilberg T, Moessmer G, Hartard M, Jeschke D: APC resistance in an elite female athlete. Med Sci Sports Exerc 1998, 30:183–184.
4. Hilberg T, Moessmer G, Hartard M, Jeschke D: APC resistance in high elite athletes. Med Sci Sports Exerc 1998, 30(Suppl):279.
5. Eichner ER: Athletes in airplanes: some are born to clot. Sports Med Dig 2000, 22:140–142.
6.•• Joffe HV, Goldhaber SZ: Upper-extremity deep venous thrombosis. Circulation 2002, 106:1874–1880.
Discussion of pathophysiology and current treatment of UEDVT.7.• Prandoni P, Bernardi E: Upper extremity deep vein thrombo-
sis. Curr Opin Pulm Med 1999, 5:222–230.Offers additional opinion regarding UEDVT management.
8.• Yilmaz EN, Vahl AC, van Heek NT, et al.: Long-term results of local thrombolysis followed by first rib resection: an encouraging clinical experience in treatment of subclavian vein thrombosis. Vasc Surg 2000, 34:17–23.
Offers additional opinion regarding UEDVT management.
82 Chest Conditions
9.•• Federman DG, Kirsner RS: An update on hypercoagulable disorders. Arch Intern Med 2001, 161:1051–1056.
Reviews most hypercoagulable disorders and their frequencies.10. Rosendaal FR, Koster T, Vandenbrouke JP, Reitsma PH: High
risk of thrombosis in patients homozygous for factor V Leiden (activated protein C resistance). Blood 1995, 85:1504–1508.
11. Huisman MV, Rosendaal F: Thrombophilia. Curr Opin Hematol 1999, 6:291–297.
12. Poort SR, Rosendaal FR, Reitsma PH, Bertina RM: A common genetic variant in the 3’-untranslated region of the prothrom-bin gene is associated with elevated plasma prothrombin lev-els and an increase in thrombosis. Blood 1996, 88:3698–3703.
13. Harris JM, Abramson N: Evaluation of recurrent thrombosis and hypercoagulability. Am Fam Physician 1997, 56:1591–1600.
14. Lane DL, Mannucci PM, Bauer KA: Inherited thrombophilia: part 1. Thromb Haemost 1996, 76:651–662.
15. Hilberg T, Jeschke D, Gabriel HHW: Hereditary thrombophilia in elite athletes. Med Sci Sports Exerc 2002, 34:218–221.
16. Ware JA, Heistad DA: Platelet-endothelium interactions. N Engl J Med 1993, 328:628–635.
17. Bliss S, Weinberger S, Meier M, Saint S: The unusual suspect. N Engl J Med 2002, 347:1876–1881.
18. Hagen TJ, Jenkinson DM, Rundell KW: Upper extremity pain-bodybuilding. Med Sci Sports Exerc 2002, 34(Suppl 1):S137.
19. King FJ, Patel B, Nicholas JJ: Effort thrombosis syndrome (Paget-Schroetter syndrome) presenting as multiple pulmonary emboli. Am J Phys Med Rehabil 2000, 79:212.
20. Simon LM: Leg pain-marathon runner. Med Sci Sports Exerc 2002, 34(Suppl 1):S44.
21. deWeber K: Effort thrombosis with sepsis. Physician Sportsmed 1999, 27:74–86.
22. Sotta RP: Vascular problems in the proximal upper extremity. Clin Sports Med 1990, 9:379–388.
23. Nemmers DW, Thorpe PE, Knibbe MA, et al.: Upper extremity venous thrombosis: case report and literature review. Orthop Rev 1990, 19:164–172.
24. Parziale JR, Akelman E, Weiss AP, et al.: Throacic outlet syndrome. Am J Orthop 2000, 29:353–360.
25. Arko FR, Harris EJ, Zarins CK, Olcott C IV: Vascular complications in high-performance athletes. J Vasc Surg 2001, 33:935–942.
26. Ertl AC, Bernauer EM, Hom CA. Plasma volume shifts with immersion at rest and two exercise intensities. Med Sci Sports Exerc 1991, 23:450–457.
27. Whittlesey MJ, Maresh CM, Armstrong LE, et al.: Plasma volume responses to consecutive anaerobic exercise tests. Int J Sports Med 1996, 17:268–271.
28. Heit JA, Silverstein MD, Mohr DN, et al.: Risk factors for deep vein thrombosis and pulmonary embolism: a population-based case-control study. Arch Intern Med 2000, 160:809–815.
29. Meissner MH, Chandler WL, Elliott JS: Venous thromboembo-lism in trauma: a local manifestation of systemic hyper-coagulability? J Trauma 2003, 54:224–231.
30.•• Ferrari E, Chevallier T, Chapelier A, Baudouy M: Travel as a risk factor for venous thromboembolic disease: a case-control study. Chest 1999, 115:440–444.
Provides support for association between travel and thromboembolism.31. Bendz B, Sevre K, Andersen TO, Sandset PM: Low molecular
weight heparin prevents activation of coagulation in a hypobaric environment. Blood Coagul Fibrinolysis 2001, 12:371–374.
32. Bendz B, Rostrup M, Sevre K, et al.: Association between hypobaric hypoxia and activation of coagulation in human beings. Lancet 2000, 356:1657–1658.
33. Kim V, Spandorfer J: Epidemiology of venous thromboembo-lic disease. Emerg Med Clin North Am 2001, 19:839–859.
34. Berglund B: High-altitude training. Aspects of haematological adaptation. Sports Med 1992, 14:289–303.
35. Powell FL, Garcia N: Physiological effects of intermittent hypoxia. High Alt Med Biol 2000, 1:125–136.
36.•• Jha SK, Anand AC, Sharma V, et al.: Stroke at high altitude: Indian experience. High Alt Med Biol 2002, 3:21–27.
Gives support to idea that polycythemia increases susceptibility to thrombus.
37. Eichner ER: Better dead than second. J Lab Clin Med 1992, 120:359–360.
38. Spivak JL: EPO in thalassemia minor: is it doping? Sports Med Dig 2002, 24:103.
39. Shaskey DJ, Green GA: Sports haematology. Sports Med 2000, 29:27–38.
40. Berglund B, Ekblom B: Effect of recombinant human erythro-poietin treatment on blood pressure and some haematologi-cal parameters in healthy men. J Int Med 1991, 229:125–130.
41. Todd MK, Goldfarb AH, Kauffman RD, Burleson C: Combined effects of age and exercise on thromboxane B2 and platelet activation. J Appl Physiol 1994, 76:1548–1552.
42. Wang J, Jen CJ, Kung H, et al.: Hypertension/exercise: Different effects of strenuous exercise and moderate exercise on plate-let function in men. Circulation 1994, 90:2877–2885.
43. Ahmadizad S, El-Sayed M: The effects of graded resistance exercise on platelet aggregation and activation. Med Sci Sports Exerc 2003, 35:1026–1032.
44. Vandenbroucke JP, Koster T, Briet E, et al.: Increased risk of venous thrombosis in oral-contraceptive users who are carri-ers of factor V leiden mutation. Lancet 1994, 344:1453–1457.
45. Urschel HC Jr, Razzuk MA: Paget-Schroetter syndrome: what is the best management? Ann Thorac Surg 2000, 69:1663–1668.
46. Sharafuddin MJ, Sun S, Hoballah JJ: Endovascular manage-ment of venous thrombotic diseases of the upper torso and extremities. J Vas Interv Radiol 2002, 13:975–990.
47.•• Schulman S: Care of patients receiving long-term anticoagu-lant therapy. N Engl J Med 2003, 349:675–683.
Review of studies for long-term therapy with warfarin. Discusses benefits and risks for low- and high-dose warfarin therapies.48. Partsch H, Blatter W: Compression and walking versus bed rest
in the treatment of proximal deep venous thrombosis with low molecular weight heparin. J Vasc Surg 2000, 32:861–868.
49. Adelman MA, Stone DH, Riles TS, et al.: A multidisciplinary approach to the treatment of Paget-Schroetter syndrome. Ann Vasc Surg 1997, 11:149–154.
50.• Kreienberg PB, Chang BB, Darling RC III, et al.: Long-term results in patients treated with thrombolysis, thoracic inlet decompression, and subclavian vein stenting for Paget-Schroetter syndrome. J Vasc Surg 2001, 33:S100–S105.
Provides prognosis for patients with UEDVT.51. Hicken GJ, Ameli M: Management of subclavian-axillary vein
thrombosis: a review. Can J Surg 1998, 41:13–25.52. Lensing AWA, Prandoni P, Prins MH, Buller HR: Deep-vein
thrombosis. Lancet 1999, 353:479–485.53. DiFelice GS, Paletta GA Jr, Phillips BB, Wright RW: Effort
thrombosis in the elite throwing athlete. Am J Sports Med 2002, 30:708–712.
54. De Stefano V, Martinelli I, Mannucci PM, et al.: The risk of recurrent deep venous thrombosis among heterozygous carriers of both factor V Leiden and the G20210A prothrombin mutation. N Engl J Med 1999, 341:801–806.
55. Khamashta MA, Cuadrado MJ, Mujic F, et al.: The management of thrombosis in the antiphospholipid-antibody syndrome. N Engl J Med 1995, 332:993–997.
56. Allaart CF, Poort SR, Rosendaal FR, et al.: Increased risk of venous thrombosis in carriers of hereditary protein C deficiency defect. Lancet 1993, 341:134–138.
57.• Ridker PM, Goldhaber SZ, Danielson E, et al.: Long-term, low-intensity warfarin therapy for prevention of recurrent venous thromboembolism. N Engl J Med 2003, 348:1425–1434.
Important for discussion of long-term management for patients with recurrent thromboembolism.58.• Kearon C, Ginsberg JS, Kovacs MJ, et al.: Comparison of
low-intensity warfarin therapy with conventional-intensity warfarin therapy for long-term prevention of recurrent venous thromboembolism. N Engl J Med 2003, 349:631–639.
Important for discussion of long-term management for patients with recurrent thromboembolism.

Hypercoagulability in Athletes • Meyering and Howard 83
59. Pulmonary Embolism Prevention (PEP) Trial Collaborative Group: Prevention of pulmonary embolism and deep vein thrombosis with low dose aspirin: Pulmonary Embolism Prevention (PEP) trial. Lancet 2000, 355:1295–1302.
60. American Academy of Pediatrics Committee on Sports Medicine and Fitness: Medical conditions affecting sports participation. Pediatrics 2001, 107:1205–1209.
61. Roberts WO, Christie DM, Jr: Return to training and competition after deep venous calf thrombosis. Med Sci Sports Exerc 1992, 24:2–5.
REVIEW Open Access
Management of venous thromboembolism:an updateSiavash Piran and Sam Schulman*
From The 9th Congress of the Asian-Pacific Society on Thrombosis and HemostasisTaipei, Taiwan. 6-9 October 2016
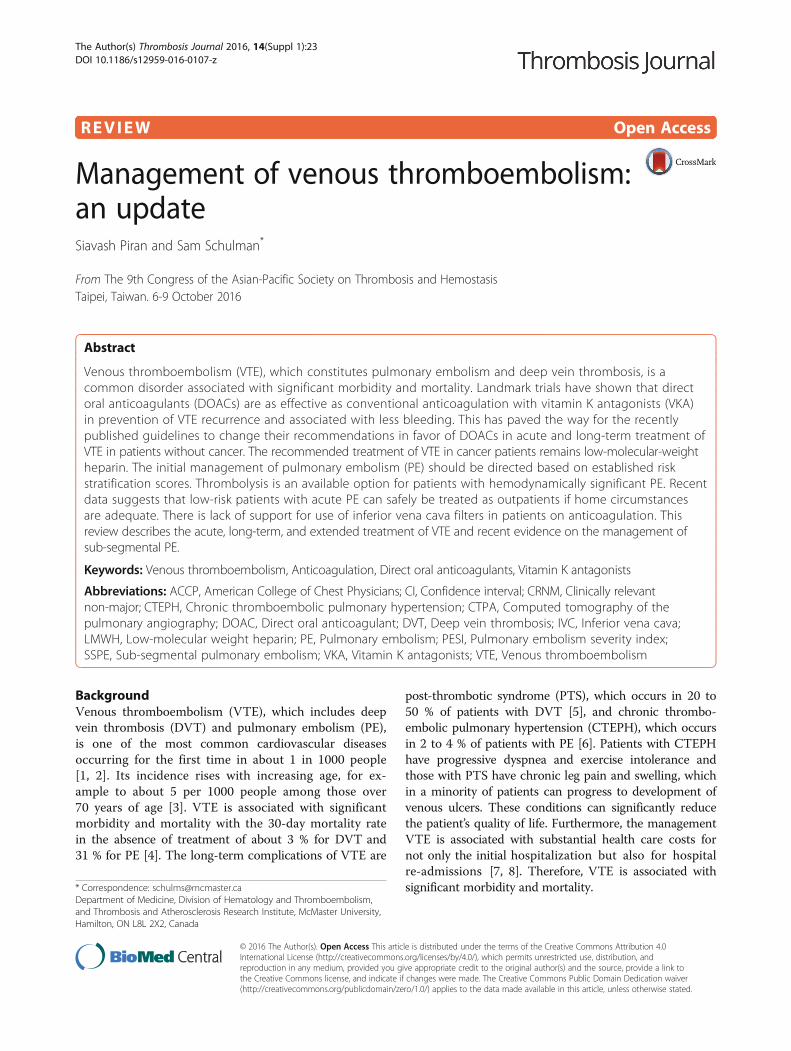
Abstract
Venous thromboembolism (VTE), which constitutes pulmonary embolism and deep vein thrombosis, is acommon disorder associated with significant morbidity and mortality. Landmark trials have shown that directoral anticoagulants (DOACs) are as effective as conventional anticoagulation with vitamin K antagonists (VKA)in prevention of VTE recurrence and associated with less bleeding. This has paved the way for the recentlypublished guidelines to change their recommendations in favor of DOACs in acute and long-term treatment ofVTE in patients without cancer. The recommended treatment of VTE in cancer patients remains low-molecular-weightheparin. The initial management of pulmonary embolism (PE) should be directed based on established riskstratification scores. Thrombolysis is an available option for patients with hemodynamically significant PE. Recentdata suggests that low-risk patients with acute PE can safely be treated as outpatients if home circumstancesare adequate. There is lack of support for use of inferior vena cava filters in patients on anticoagulation. Thisreview describes the acute, long-term, and extended treatment of VTE and recent evidence on the management ofsub-segmental PE.
Keywords: Venous thromboembolism, Anticoagulation, Direct oral anticoagulants, Vitamin K antagonists
Abbreviations: ACCP, American College of Chest Physicians; CI, Confidence interval; CRNM, Clinically relevantnon-major; CTEPH, Chronic thromboembolic pulmonary hypertension; CTPA, Computed tomography of thepulmonary angiography; DOAC, Direct oral anticoagulant; DVT, Deep vein thrombosis; IVC, Inferior vena cava;LMWH, Low-molecular weight heparin; PE, Pulmonary embolism; PESI, Pulmonary embolism severity index;SSPE, Sub-segmental pulmonary embolism; VKA, Vitamin K antagonists; VTE, Venous thromboembolism
BackgroundVenous thromboembolism (VTE), which includes deepvein thrombosis (DVT) and pulmonary embolism (PE),is one of the most common cardiovascular diseasesoccurring for the first time in about 1 in 1000 people[1, 2]. Its incidence rises with increasing age, for ex-ample to about 5 per 1000 people among those over70 years of age [3]. VTE is associated with significantmorbidity and mortality with the 30-day mortality ratein the absence of treatment of about 3 % for DVT and31 % for PE [4]. The long-term complications of VTE are
post-thrombotic syndrome (PTS), which occurs in 20 to50 % of patients with DVT [5], and chronic thrombo-embolic pulmonary hypertension (CTEPH), which occursin 2 to 4 % of patients with PE [6]. Patients with CTEPHhave progressive dyspnea and exercise intolerance andthose with PTS have chronic leg pain and swelling, whichin a minority of patients can progress to development ofvenous ulcers. These conditions can significantly reducethe patient’s quality of life. Furthermore, the managementVTE is associated with substantial health care costs fornot only the initial hospitalization but also for hospitalre-admissions [7, 8]. Therefore, VTE is associated withsignificant morbidity and mortality.* Correspondence: [email protected]
Department of Medicine, Division of Hematology and Thromboembolism,and Thrombosis and Atherosclerosis Research Institute, McMaster University,Hamilton, ON L8L 2X2, Canada
© 2016 The Author(s). Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
The Author(s) Thrombosis Journal 2016, 14(Suppl 1):23DOI 10.1186/s12959-016-0107-z

Initial managementThe initial management of patients with a PE should bebased on risk stratification of the patient into low, inter-mediate, or high risk for 30-day mortality based on estab-lished risk scores such as pulmonary embolism severityindex (PESI) or its simplified version (simplified PESI) [9,10]. Low risk patients, who are hemodynamically stable,can be treated as outpatients if home circumstances areadequate [11, 12]. At the other extreme, patients with acutePE and hypotension or patients with DVT-associatedphlegmasia of the lower leg should be considered for treat-ment with thrombolytic agents [13, 14].
Oral anticoagulantsAnticoagulants are the mainstay treatment of VTE and aregiven in three phases of acute, long-term (in the first3 months), and extended treatment [14]. For many yearsinitial treatment was started with a parenteral anticoagu-lant, for example low-molecular-weight heparin (LMWH),overlapping with a vitamin K antagonist (VKA), such aswarfarin. The combination was continued for at least 5 daysuntil the achievement of therapeutic anticoagulation withinternational normalized ratio of 2 to 3 [14]. Although con-ventional therapy with VKAs is effective and safe, it hassome limitations including delayed onset, need for parentaldaily injections, and interactions with dietary vitamin Kand numerous drugs. Over the past 5 years, 4 direct oralanticoagulants (DOACs) have been approved for acute andlong-term treatment of VTE [15–20]. The DOACs werecompared with conventional therapy and found to be as ef-fective in prevention of VTE recurrence and associatedwith less bleeding. The recently published American Col-lege of Chest Physicians (ACCP) guidelines have changedtheir recommendations in favor of DOACs in acute andlong-term treatment of VTE in patients without cancer[21]. In patients with cancer associated VTE, the recom-mended anticoagulation remains LMWH over VKA [21].The aim of this review is to (1) describe the initial man-
agement of patients with acute PE including the role ofthrombolytic agents in hemodynamically unstable patientsand at the other extreme outpatient management of lowrisk patients, (2) summarize the evidence on acute, long-term, and extended treatment of VTE comparing DOACsversus VKA, and (3) review the recent data on the manage-ment of sub-segmental PE and the lack of support for useof inferior vena cava filters in patients on anticoagulation.
ReviewAcute and long-term treatment of venousthromboembolismThrombolytic and interventional treatment for acute venousthromboembolismAnticoagulant therapy alone is recommended overthrombolysis for most patients with an acute DVT with
exception for those with extensive iliofemoral or proximalDVT at high risk of limb ischemia [14, 21]. Thrombolytictherapy (systemic or catheter-directed) increase clot lysisand reduce the incidence of PTS compared to anticoagu-lation alone [22, 23]. However, this is at the expense ofhigher rate of major bleeding and no difference in rate ofrecurrent VTE or mortality [22–24]. Massive proximalDVT or iliofemoral thrombosis associated with limb-threatening ischemia or severe symptomatic swelling maybe treated with thrombolysis. Thrombolysis can be con-sidered only after objective diagnosis of the DVT and in apatient with low bleeding risk. The CaVenT trial random-ized 209 patients with iliofemoral DVT to catheter di-rected therapy (CDT) versus anticoagulation. They foundthat the patients treated with CDT had significantly lessPTS at 2 years compared with those treated with anticoa-gulation (41 versus 56 %) [22]. Another study randomized32 patients with iliofemoral DVT to receive either CDT orsystemic thrombolysis, followed by anticoagulation [25].The patients who were treated with CDT had less refluxin both the deep and superficial veins and more patientshad venous valvular competence preserved compared withpatients who underwent systemic thrombolysis. A large,multicenter trial (the ATTRACT trial) is currently under-way that randomizes patients to receive pharmaco-mechanical catheter-directed thrombolysis (PCDT) plusstandard therapy with anticoagulation versus standardtherapy alone [26]. It will investigate whether PCDTshould be routinely utilized to prevent PTS in patientswith symptomatic proximal DVT [26].Systemic thrombolysis is a widely accepted treatment
for PE in patients with persistent hypotension (e.g., sys-tolic blood pressure <90 mmHg for 15 min) and not athigh risk of bleeding [14, 21]. The use of thrombolytictherapy in intermediate risk patients with acute PEassociated with right ventricle (RV) dysfunction is con-troversial. The RV dysfunction is confirmed by echo-cardiogram or computed tomography and a positivetroponin I/T. The potential indication for thrombolysisin this group is based on evidence that patients with se-vere RV dysfunction have worse prognosis than thosewithout RV dysfunction [27]. Three recently publishedtrials have examined the role of systemic thrombolysis inintermediate risk patients [28–30]. In the ModeratePulmonary Embolism Treated Thrombolysis (MOPETT)trial, 121 patients were randomly assigned to receiveheparin (unfractionated or LMWH) alone or the com-bination of tissue type plasminogen activator (tPA) plusheparin [28]. Compared to the heparin group, treatmentwith tPA resulted in lower rates of pulmonary hyperten-sion and significantly lower pulmonary artery systolicpressures at 28 months. The rates of bleeding, recurrentPE, and mortality was similar in both groups [28]. In an-other trial comparing the combination of LMWH plus
The Author(s) Thrombosis Journal 2016, 14(Suppl 1):23 Page 108 of 163

an intravenous bolus of tenecteplase versus LMWHalone in intermediate risk PE patients, those treated withtenecteplase had fewer adverse outcomes and betterfunctional capacity at 90 days [29]. In a large multicenterrandomized trial (PEITHO), 1005 intermediate risk pa-tients with PE were randomized to tenecteplase and hep-arin or to heparin therapy alone [30]. Thrombolysistherapy led to reduction in the primary composite out-come of death or cardiovascular collapse at seven daysafter randomization although it increased major bleeding(including intracranial bleeding) with no overall gainedbenefit from thrombolysis [30]. A meta-analysis of 16trials comprising 2115 intermediate risk patients re-ported that 59 patients would need to be treated withthrombolysis to prevent one death, while a major bleed-ing occurs with every 18 patients treated [13]. Furtherstudies are needed to identify subgroups of intermediaterisk patients who will benefit from systemic thrombo-lytic therapy.CDT may be used in patients with acute PE at in-
creased risk of bleeding as a lower dose of a thrombo-lytic agent is infused directly into the pulmonary arteryvia a catheter [31]. CDT is also effective in lowering pul-monary arterial pressure and improving RV function[32]. In a randomized controlled trial of 59 patients withacute intermediate risk PE, ultrasound-assisted catheter-directed thrombolysis followed by heparin was comparedto treatment with heparin alone [33]. At 24 h, CDT im-proved the hemodynamics compared to anticoagulation.At 90 days of follow-up, there was no difference in mor-tality or major bleeding between the two groups [33].Most of the evidence is limited by small sample size andof low quality compared to the available evidence forsystemic thrombolysis. Systemic thrombolysis is there-fore currently recommended over CDT in patients withacute PE who are candidates for thrombolysis [21].
Outpatient treatment of venous thromboembolismHome therapy is commonly employed for patients withan acute DVT in clinical practice with a few exceptions.Several randomized controlled trials and meta-analyses,which have compared home therapy with LMWH versusinpatient therapy with intravenous unfractionated heparin,suggest that outpatient therapy is safe and feasible in mostpatients with acute DVT [34–36]. Outpatient therapyshould not be selected for those with massive symptom-atic DVT, high risk of bleeding, or hemodynamic instabil-ity due to concurrent symptomatic PE [37].The outpatient treatment of acute PE is suggested with
grade 2B evidence in the most recent ACCP guidelinesin low-risk patients with adequate home circumstances[21]. The decision for outpatient management should takeinto account the patient’s clinical condition, bleeding risk,their preference, and the available home support. Risk
stratification scores such as PESI or simplified PESI maybe utilized to identify low-risk patients without RV dys-function who are potential candidates for short in-hospitalstay or entirely outpatient management [11, 12, 38]. Withthe recent changed recommendations in favor of DOACsfor acute and long-term VTE treatment, future researchshould focus on the safety and efficacy of DOACs in out-patient management of acute VTE.
Vitamin K antagonists versus direct oral anticoagulantsFour DOACs including dabigatran, rivaroxaban, apixa-ban, and edoxaban were compared with conventionaltherapy in the RE-COVER I and II, EINSTEIN-DVT andPE, AMPLIFY, and Hokusai-VTE trials, respectively[15–20]. The study design was double-blinded in all trialsexcept for the ENSTEIN trials, which used a prospective,randomized, open-label, blinded end point evaluation de-sign. The study designs and treat protocols are comparedin Table 1. The study populations were similar in thesetrials. In the dabigatran and edoxaban trials, parentalanticoagulation was added to both DOAC and conven-tional therapy arms, and after at least 5 days patients wereswitched to the DOAC. Therefore, in clinical practice, pa-tients should be initiated on parenteral anticoagulationand either switched to dabigatran or edoxaban after 5 daysor it should be overlapped with a vitamin K antagonist. Incontrast, in the rivaroxaban and apixaban trials DOACswere started without the need for initial parental anticoa-gulation. The primary efficacy outcome was recurrentVTE or VTE-related mortality in all 6 trials. The primarysafety outcome was either major bleeding or a compositeof major and clinically relevant non-major bleeding(CRNMB). The efficacy and safety outcomes of these trialsare listed in Table 2. All of the trials excluded patientswith severe renal dysfunction, those with active bleedingor at high risk of bleeding, and patients already on thera-peutic anticoagulation. A recent pooled analysis of these 6trials reported that DOACs have similar efficacy as VKAin treatment of acute VTE and significantly lower risk ofmajor bleeding than VKA [39]. Recurrent VTE occurredin 2 % of those given DOAC versus 2.2 % in patients thatreceived VKA (relative risk [RR] 0.90; 95 % confidenceinterval [CI], 0.77 – 1.06) [39]. A 39 % reduction in risk ofmajor bleeding was reported in DOAC recipients com-pared to those who received VKA therapy (RR 0.61; 95 %CI, 0.45 – 0.83). Compared with recipients of VKA ther-apy, intracranial bleeding, fatal bleeding, and CRNMBwere significantly reduced in the DOAC group [39]. Giventhe better safety profile of DOACs with less major bleed-ing, similar efficacy in prevention of recurrent VTE, andthe convenience of administration of DOACs, the recentACCP guidelines suggested DOACs over VKA for theacute and long-term treatment of VTE in patients withoutcancer [21].
The Author(s) Thrombosis Journal 2016, 14(Suppl 1):23 Page 109 of 163
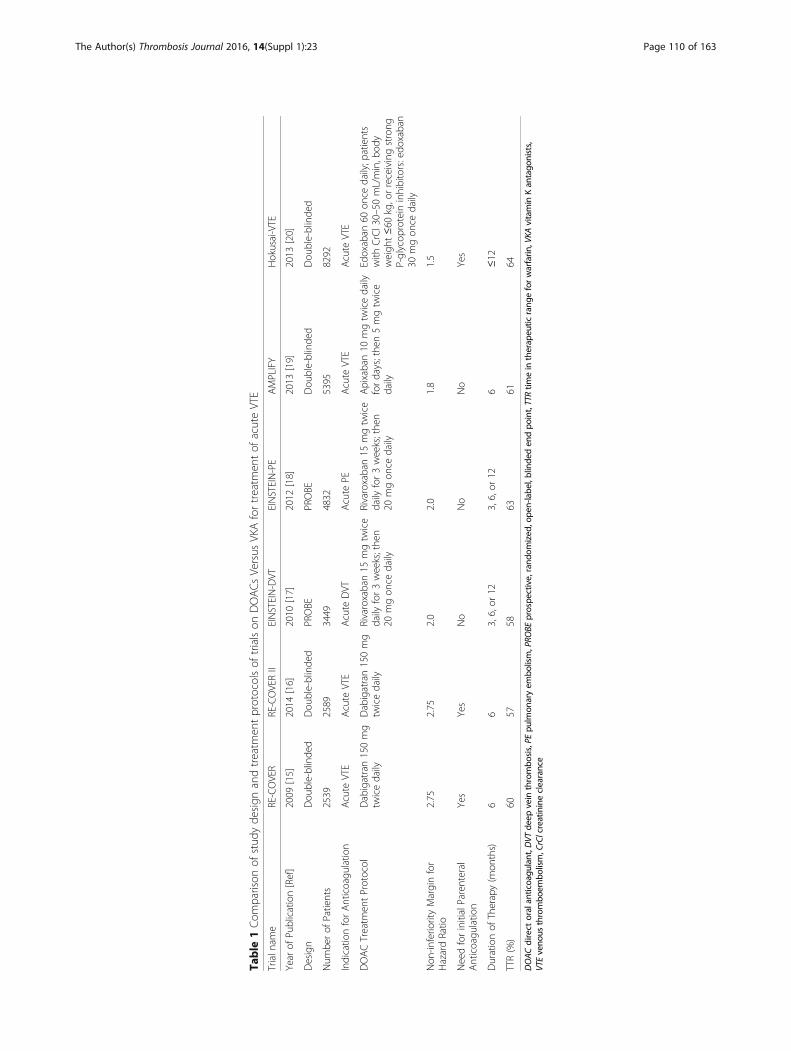
Table
1Com
parison
ofstud
yde
sign
andtreatm
entprotocolsof
trialson
DOACsVersus
VKAfortreatm
entof
acuteVTE
Trialn
ame
RE-COVER
RE-COVERII
EINSTEIN-DVT
EINSTEIN-PE
AMPLIFY
Hokusai-VTE
Year
ofPu
blication[Ref]
2009
[15]
2014
[16]
2010
[17]
2012
[18]
2013
[19]
2013
[20]
Design
Dou
ble-blinde
dDou
ble-blinde
dPROBE
PROBE
Dou
ble-blinde
dDou
ble-blinde
d
Num
berof
Patients
2539
2589
3449
4832
5395
8292
Indicatio
nforAnticoagu
latio
nAcute
VTE
Acute
VTE
Acute
DVT
Acute
PEAcute
VTE
Acute
VTE
DOACTreatm
entProtocol
Dabigatran150mg
twicedaily
Dabigatran150mg
twicedaily
Rivaroxaban15
mgtw
ice
daily
for3weeks;the
n20
mgon
cedaily
Rivaroxaban15
mgtw
ice
daily
for3weeks;the
n20
mgon
cedaily
Apixaban10
mgtw
icedaily
fordays;the
n5mgtw
ice
daily
Edoxaban
60on
cedaily;p
atients
with
CrCl30–50
mL/min,b
ody
weigh
t≤60
kg,orreceivingstrong
P-glycop
rotein
inhibitors:edo
xaban
30mgon
cedaily
Non
-inferio
rityMarginfor
HazardRatio
2.75
2.75
2.0
2.0
1.8
1.5
NeedforinitialParenteral
Anticoagu
latio
nYes
Yes
No
No
No
Yes
Durationof
Therapy(m
onths)
66
3,6,or
123,6,or
126
≤12
TTR(%)
6057
5863
6164
DOACdirect
oralan
ticoagu
lant,D
VTde
epvein
thrombo
sis,PE
pulm
onaryem
bolism,PRO
BEprospe
ctive,rand
omized
,ope
n-labe
l,blinde
den
dpo
int,TTRtim
ein
therap
eutic
rang
eforwarfarin
,VKA
vitamin
Kan
tago
nists,
VTEveno
usthrombo
embo
lism,CrClcreatinineclearance
The Author(s) Thrombosis Journal 2016, 14(Suppl 1):23 Page 110 of 163
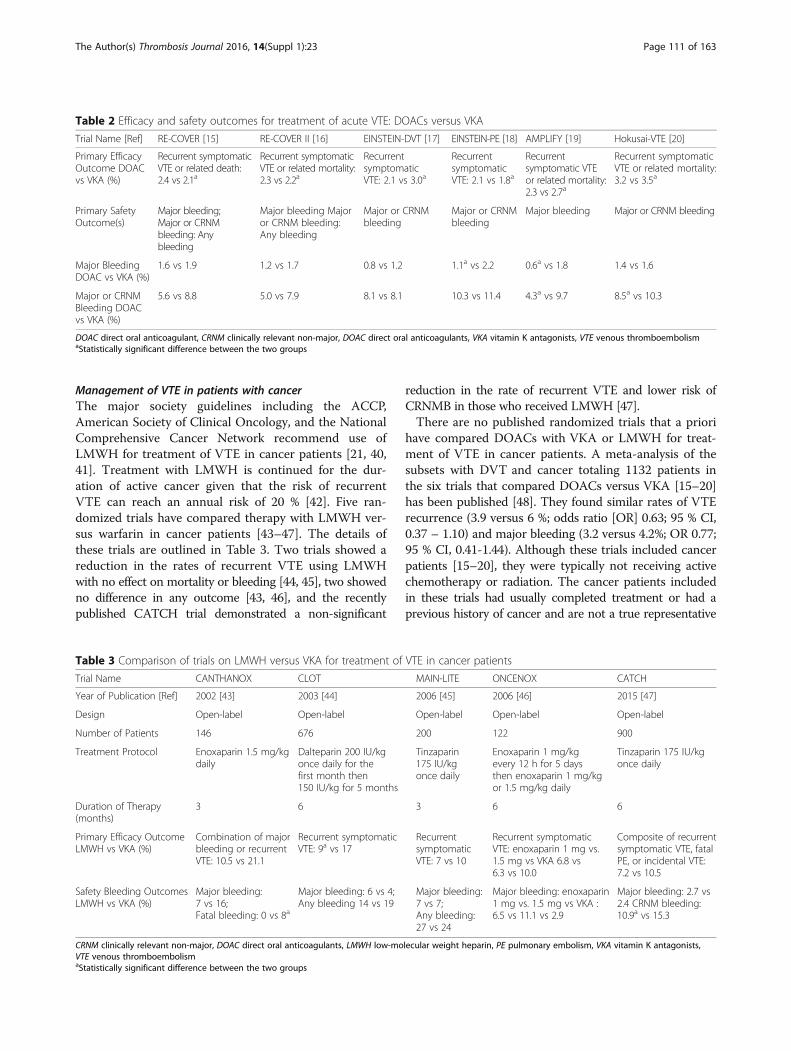
Management of VTE in patients with cancerThe major society guidelines including the ACCP,American Society of Clinical Oncology, and the NationalComprehensive Cancer Network recommend use ofLMWH for treatment of VTE in cancer patients [21, 40,41]. Treatment with LMWH is continued for the dur-ation of active cancer given that the risk of recurrentVTE can reach an annual risk of 20 % [42]. Five ran-domized trials have compared therapy with LMWH ver-sus warfarin in cancer patients [43–47]. The details ofthese trials are outlined in Table 3. Two trials showed areduction in the rates of recurrent VTE using LMWHwith no effect on mortality or bleeding [44, 45], two showedno difference in any outcome [43, 46], and the recentlypublished CATCH trial demonstrated a non-significant
reduction in the rate of recurrent VTE and lower risk ofCRNMB in those who received LMWH [47].There are no published randomized trials that a priori
have compared DOACs with VKA or LMWH for treat-ment of VTE in cancer patients. A meta-analysis of thesubsets with DVT and cancer totaling 1132 patients inthe six trials that compared DOACs versus VKA [15–20]has been published [48]. They found similar rates of VTErecurrence (3.9 versus 6 %; odds ratio [OR] 0.63; 95 % CI,0.37 – 1.10) and major bleeding (3.2 versus 4.2%; OR 0.77;95 % CI, 0.41-1.44). Although these trials included cancerpatients [15–20], they were typically not receiving activechemotherapy or radiation. The cancer patients includedin these trials had usually completed treatment or had aprevious history of cancer and are not a true representative
Table 3 Comparison of trials on LMWH versus VKA for treatment of VTE in cancer patients
Trial Name CANTHANOX CLOT MAIN-LITE ONCENOX CATCH
Year of Publication [Ref] 2002 [43] 2003 [44] 2006 [45] 2006 [46] 2015 [47]
Design Open-label Open-label Open-label Open-label Open-label
Number of Patients 146 676 200 122 900
Treatment Protocol Enoxaparin 1.5 mg/kgdaily
Dalteparin 200 IU/kgonce daily for thefirst month then150 IU/kg for 5 months
Tinzaparin175 IU/kgonce daily
Enoxaparin 1 mg/kgevery 12 h for 5 daysthen enoxaparin 1 mg/kgor 1.5 mg/kg daily
Tinzaparin 175 IU/kgonce daily
Duration of Therapy(months)
3 6 3 6 6
Primary Efficacy OutcomeLMWH vs VKA (%)
Combination of majorbleeding or recurrentVTE: 10.5 vs 21.1
Recurrent symptomaticVTE: 9a vs 17
RecurrentsymptomaticVTE: 7 vs 10
Recurrent symptomaticVTE: enoxaparin 1 mg vs.1.5 mg vs VKA 6.8 vs6.3 vs 10.0
Composite of recurrentsymptomatic VTE, fatalPE, or incidental VTE:7.2 vs 10.5
Safety Bleeding OutcomesLMWH vs VKA (%)
Major bleeding:7 vs 16;Fatal bleeding: 0 vs 8a
Major bleeding: 6 vs 4;Any bleeding 14 vs 19
Major bleeding:7 vs 7;Any bleeding:27 vs 24
Major bleeding: enoxaparin1 mg vs. 1.5 mg vs VKA :6.5 vs 11.1 vs 2.9
Major bleeding: 2.7 vs2.4 CRNM bleeding:10.9a vs 15.3
CRNM clinically relevant non-major, DOAC direct oral anticoagulants, LMWH low-molecular weight heparin, PE pulmonary embolism, VKA vitamin K antagonists,VTE venous thromboembolismaStatistically significant difference between the two groups
Table 2 Efficacy and safety outcomes for treatment of acute VTE: DOACs versus VKA
Trial Name [Ref] RE-COVER [15] RE-COVER II [16] EINSTEIN-DVT [17] EINSTEIN-PE [18] AMPLIFY [19] Hokusai-VTE [20]
Primary EfficacyOutcome DOACvs VKA (%)
Recurrent symptomaticVTE or related death:2.4 vs 2.1a
Recurrent symptomaticVTE or related mortality:2.3 vs 2.2a
RecurrentsymptomaticVTE: 2.1 vs 3.0a
RecurrentsymptomaticVTE: 2.1 vs 1.8a
Recurrentsymptomatic VTEor related mortality:2.3 vs 2.7a
Recurrent symptomaticVTE or related mortality:3.2 vs 3.5a
Primary SafetyOutcome(s)
Major bleeding;Major or CRNMbleeding: Anybleeding
Major bleeding Majoror CRNM bleeding:Any bleeding
Major or CRNMbleeding
Major or CRNMbleeding
Major bleeding Major or CRNM bleeding
Major BleedingDOAC vs VKA (%)
1.6 vs 1.9 1.2 vs 1.7 0.8 vs 1.2 1.1a vs 2.2 0.6a vs 1.8 1.4 vs 1.6
Major or CRNMBleeding DOACvs VKA (%)
5.6 vs 8.8 5.0 vs 7.9 8.1 vs 8.1 10.3 vs 11.4 4.3a vs 9.7 8.5a vs 10.3
DOAC direct oral anticoagulant, CRNM clinically relevant non-major, DOAC direct oral anticoagulants, VKA vitamin K antagonists, VTE venous thromboembolismaStatistically significant difference between the two groups
The Author(s) Thrombosis Journal 2016, 14(Suppl 1):23 Page 111 of 163

of all cancer patients. The Hokusai VTE-cancer random-ized open label trial is currently underway and will examinewhether edoxaban is non-inferior to LMWH for treatmentof VTE in cancer patients [49].
Extended treatment of venous thromboembolismExtended anticoagulation can be employed in patientswith unprovoked VTE to reduce the risk of recurrentVTE if the benefit/risk ratio favors continuation of antic-oagulation while taking into account patient’s risk ofbleeding. All DOACs except for edoxaban have beencompared with placebo in randomized trials for ex-tended secondary VTE prevention beyond the initialthree months of anticoagulation [17, 50, 51]. The detailsof these trials are compared in Table 4. All trials showedmarked superiority of the DOACs over placebo for theprevention of recurrent VTE without significant increasein major bleeding [17,50, 51]. However, compared to theplacebo arms, all DOACs had higher rate of CRNMB[17, 50, 51]. Duration of extended anticoagulation was 6to 12 months in the EINSTEIN [17] and AMPLIFY-Extension [50] studies and 6 months in the RE-SONATEtrial [51]. Two doses of apixaban were evaluated in theAMPLIFY-Extension trial and the rate of bleeding waslower for apixaban 2.5 mg twice daily than 5 mg twicedaily [50]. A single regimen of rivaroxban (20 mg oncedaily) and dabigatran (150 mg twice daily) was used inthe EINSTEIN and RE-SONATE studies.Dabigatran is the only DOAC that has been compared
with warfarin for extended VTE prevention in the RE-MEDY trial [51]. Dabigatran was non-inferior to war-farin in prevention of recurrent VTE (1.8 versus 1.3 %,hazard ratio [HR] 1.44; 95 % CI, 0.78–2.64) and had asignificantly lower rate of major bleeding or CRNMB(HR 0.54; 95 % CI, 0.41–0.71). These results demonstrated
that DOACs are effective in secondary VTE preventionwith no significant increase in major bleeding. The ACCPguidelines recommend no change in the choice of anti-coagulant agent in patients who need extended anticoagu-lation after the first 3 months of therapy [21]. Given theobserved lower bleeding risk, the dose of apixaban may bereduced to 2.5 mg twice daily after the initial treatment.Aspirin has been also evaluated in secondary VTE pre-
vention in patients with first unprovoked VTE who havecompleted anticoagulant treatment. In this setting, ran-domized trials and a meta-analysis reported a 30 % re-duction in rates of recurrent VTE compared to placeboor observation [52–55]. The ACCP guidelines suggestthat aspirin is an available option in patients with unpro-voked VTE that are stopping anticoagulant therapy ifthere are no contraindications to use of aspirin [21].However, aspirin is not recommended as an alternativeto anticoagulant therapy [21].
Treatment of VTE in special situationsManagement of sub-segmental pulmonary embolismThe increase in utilization of a highly sensitive com-puted tomography pulmonary angiography (CTPA) hasled to detection of incidental asymptomatic PE or smallsub-segmental PE [56]. Whether or not patients withsub-segmental pulmonary embolism (SSPE) should beanticoagulated is controversial. It is unclear whether theSSPE detected by CTPA are artifacts and therefore falsepositive [57]. Furthermore, an isolated SSPE likely doesnot have the same risk of progression or VTE recurrenceas a single segmental or lobar PE [57]. There are cur-rently no published randomized trials for treatment ofpatients with SSPE. Retrospective studies have reportedVTE recurrence in only a small number of patients withSSPE and without DVT, who were not anticoagulated.
Table 4 Comparison of extended duration DOAC trials
Trial Name EINSTEIN-EXTENSION AMPLIFY-EXT RE-MEDY RE-SONATE
Year of Publication [Ref] 2010 [17] 2013 [50] 2013 [51] 2013 [51]
Design Double-blinded Double-blinded Double-blinded Double-blinded
Comparison Arm Placebo Placebo Warfarin Placebo
Number of Patients 1197 2486 2866 1353
Treatment Protocol Rivaroxaban 20 mgonce daily
Apixaban 5 mg or 2.5twice daily
Dabigatran 150 mgtwice daily
Dabigatran 150 mgtwice daily
Duration of Therapy (months) 6 to12 12 6 to 36 6
Primary Efficacy OutcomeDOAC vs VKA or Placebo (%)
Recurrent symptomaticVTE: 1.3a vs 7.1
Recurrent symptomaticVTE or all-cause mortality:3.8a vs 4.2a vs 11.6
Recurrent symptomaticVTE or related mortality:1.8a vs 1.3
Recurrent symptomaticVTE or related mortality:0.4a vs 5.6
Major Bleeding DOAC vsVKA or Placebo (%)
0.7 vs 0 0.2 vs 0.1 vs 0.5 0.9 vs 1.8 0.3 vs 0
Major and CRNM BleedingDOAC vs VKA or Placebo (%)
6.0a vs 1.2 3.2 vs 4.3 vs 2.7 5.6a vs 10.2 5.3a vs 1.8
DOAC direct oral anticoagulant, CRNM clinically relevant non-major, DOAC direct oral anticoagulants, VKA vitamin K antagonists, VTE venous thromboembolismaStatistically significant difference between the two groups
The Author(s) Thrombosis Journal 2016, 14(Suppl 1):23 Page 112 of 163
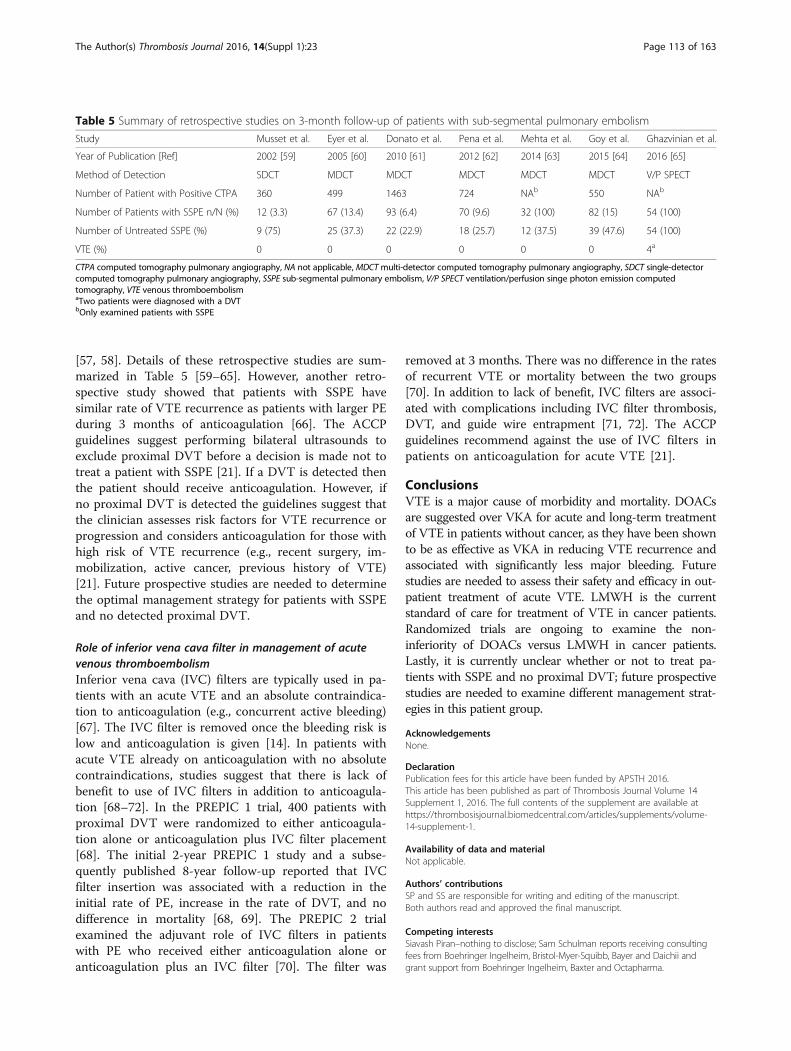
[57, 58]. Details of these retrospective studies are sum-marized in Table 5 [59–65]. However, another retro-spective study showed that patients with SSPE havesimilar rate of VTE recurrence as patients with larger PEduring 3 months of anticoagulation [66]. The ACCPguidelines suggest performing bilateral ultrasounds toexclude proximal DVT before a decision is made not totreat a patient with SSPE [21]. If a DVT is detected thenthe patient should receive anticoagulation. However, ifno proximal DVT is detected the guidelines suggest thatthe clinician assesses risk factors for VTE recurrence orprogression and considers anticoagulation for those withhigh risk of VTE recurrence (e.g., recent surgery, im-mobilization, active cancer, previous history of VTE)[21]. Future prospective studies are needed to determinethe optimal management strategy for patients with SSPEand no detected proximal DVT.
Role of inferior vena cava filter in management of acutevenous thromboembolismInferior vena cava (IVC) filters are typically used in pa-tients with an acute VTE and an absolute contraindica-tion to anticoagulation (e.g., concurrent active bleeding)[67]. The IVC filter is removed once the bleeding risk islow and anticoagulation is given [14]. In patients withacute VTE already on anticoagulation with no absolutecontraindications, studies suggest that there is lack ofbenefit to use of IVC filters in addition to anticoagula-tion [68–72]. In the PREPIC 1 trial, 400 patients withproximal DVT were randomized to either anticoagula-tion alone or anticoagulation plus IVC filter placement[68]. The initial 2-year PREPIC 1 study and a subse-quently published 8-year follow-up reported that IVCfilter insertion was associated with a reduction in theinitial rate of PE, increase in the rate of DVT, and nodifference in mortality [68, 69]. The PREPIC 2 trialexamined the adjuvant role of IVC filters in patientswith PE who received either anticoagulation alone oranticoagulation plus an IVC filter [70]. The filter was
removed at 3 months. There was no difference in the ratesof recurrent VTE or mortality between the two groups[70]. In addition to lack of benefit, IVC filters are associ-ated with complications including IVC filter thrombosis,DVT, and guide wire entrapment [71, 72]. The ACCPguidelines recommend against the use of IVC filters inpatients on anticoagulation for acute VTE [21].
ConclusionsVTE is a major cause of morbidity and mortality. DOACsare suggested over VKA for acute and long-term treatmentof VTE in patients without cancer, as they have been shownto be as effective as VKA in reducing VTE recurrence andassociated with significantly less major bleeding. Futurestudies are needed to assess their safety and efficacy in out-patient treatment of acute VTE. LMWH is the currentstandard of care for treatment of VTE in cancer patients.Randomized trials are ongoing to examine the non-inferiority of DOACs versus LMWH in cancer patients.Lastly, it is currently unclear whether or not to treat pa-tients with SSPE and no proximal DVT; future prospectivestudies are needed to examine different management strat-egies in this patient group.
AcknowledgementsNone.
DeclarationPublication fees for this article have been funded by APSTH 2016.This article has been published as part of Thrombosis Journal Volume 14Supplement 1, 2016. The full contents of the supplement are available athttps://thrombosisjournal.biomedcentral.com/articles/supplements/volume-14-supplement-1.
Availability of data and materialNot applicable.
Authors’ contributionsSP and SS are responsible for writing and editing of the manuscript.Both authors read and approved the final manuscript.
Competing interestsSiavash Piran–nothing to disclose; Sam Schulman reports receiving consultingfees from Boehringer Ingelheim, Bristol-Myer-Squibb, Bayer and Daichii andgrant support from Boehringer Ingelheim, Baxter and Octapharma.
Table 5 Summary of retrospective studies on 3-month follow-up of patients with sub-segmental pulmonary embolism
Study Musset et al. Eyer et al. Donato et al. Pena et al. Mehta et al. Goy et al. Ghazvinian et al.
Year of Publication [Ref] 2002 [59] 2005 [60] 2010 [61] 2012 [62] 2014 [63] 2015 [64] 2016 [65]
Method of Detection SDCT MDCT MDCT MDCT MDCT MDCT V/P SPECT
Number of Patient with Positive CTPA 360 499 1463 724 NAb 550 NAb
Number of Patients with SSPE n/N (%) 12 (3.3) 67 (13.4) 93 (6.4) 70 (9.6) 32 (100) 82 (15) 54 (100)
Number of Untreated SSPE (%) 9 (75) 25 (37.3) 22 (22.9) 18 (25.7) 12 (37.5) 39 (47.6) 54 (100)
VTE (%) 0 0 0 0 0 0 4a
CTPA computed tomography pulmonary angiography, NA not applicable, MDCTmulti-detector computed tomography pulmonary angiography, SDCT single-detectorcomputed tomography pulmonary angiography, SSPE sub-segmental pulmonary embolism, V/P SPECT ventilation/perfusion singe photon emission computedtomography, VTE venous thromboembolismaTwo patients were diagnosed with a DVTbOnly examined patients with SSPE
The Author(s) Thrombosis Journal 2016, 14(Suppl 1):23 Page 113 of 163
Consent for publicationThe authors consent to publication. No other consents are applicable.
Ethics approval and consent to participateNot applicable.
Published: 4 October 2016
References1. White RH. The epidemiology of venous thromboembolism. Circulation.
2003;107(23 Suppl 1):14–8.2. Martinez C, Cohen AT, Bamber L, Rietbrock S. Epidemiology of first and
recurrent venous thromboembolism: a population-based cohort study inpatients without active cancer. Thromb Haemost. 2014;112:255–63.
3. ISTH Steering Committee for World Thrombosis Day. Thrombosis: a majorcontributor to global disease burden. Thromb Res. 2014;134:931–8.
4. Søgaard KK, Schmidt M, Pedersen L, Horváth-Puhó E, Sørensen HT. 30-yearmortality after venous thromboembolism: a population-based cohort study.Circulation. 2014;130:829–36.
5. Prandoni P, Lensing AW, Cogo A, Cuppini S, Villalta S, Carta M, et al. Thelong-term clinical course of acute deep venous thrombosis. Ann InternMed. 1996;125:1–7.
6. Pengo V, Lensing AW, Prins MH, Marchiori A, Davidson BL, Tiozzo F, et al.Incidence of chronic thromboembolic pulmonary hypertension afterpulmonary embolism. N Engl J Med. 2004;350:2257–64.
7. LaMori JC, Shohieber O, Mody SH, Bookhart BK. Inpatient resource use andcost burden of deep vein thrombosis and pulmonary embolism in theUnited States. Clin Ther. 2015;37:62–70.
8. Spyropoulos AC, Lin J. Direct medical costs of venous thromboembolismand subsequent hospital readmission rates: an administrative claims analysisfrom 30 managed care organizations. J Manag Care Pharm. 2007;13:475–86.
9. Donzé J, Le Gal G, Fine MJ, Roy PM, Sanchez O, Verschuren F, et al. Prospectivevalidation of the Pulmonary Embolism Severity Index. A clinical prognosticmodel for pulmonary embolism. Thromb Haemost. 2008;100:943–8.
10. Jiménez D, Aujesky D, Moores L, Gómez V, Lobo JL, Uresandi F, et al.Simplification of the pulmonary embolism severity index forprognostication in patients with acute symptomatic pulmonary embolism.Arch Intern Med. 2010;170:1383–9.
11. Zondag W, Kooiman J, Klok FA, Dekkers OM, Huisman MV. Outpatientversus inpatient treatment in patients with pulmonary embolism: ameta-analysis. Eur Respir J. 2013;42:134–44.
12. Piran S, Le Gal G, Wells PS, Gandara E, Righini M, Rodger MA, et al.Outpatient treatment of symptomatic pulmonary embolism: a systematicreview and meta-analysis. Thromb Res. 2013;132:515–9.
13. Chatterjee S, Chakraborty A, Weinberg I, Kadakia M, Wilensky RL, Sardar P,et al. Thrombolysis for pulmonary embolism and risk of all-cause mortality,major bleeding, and intracranial hemorrhage: a meta-analysis. JAMA. 2014;311:2414–21.
14. Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ,et al. Antithrombotic therapy for VTE disease: Antithrombotic therapy andprevention of thrombosis, 9th ed: American College of Chest Physiciansevidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e419S–94.
15. Schulman S, Kearon C, Kakkar AK, Mismetti P, Schellong S, Eriksson H, et al.Dabigatran versus warfarin in the treatment of acute venousthromboembolism. N Engl J Med. 2009;361:2342–52.
16. Schulman S, Kakkar AK, Goldhaber SZ, Schellong S, Eriksson H, Mismetti P,et al. Treatment of acute venous thromboembolism with dabigatran orwarfarin and pooled analysis. Circulation. 2014;129:764–72.
17. EINSTEIN Investigators, Bauersachs R, Berkowitz SD, Brenner B, Buller HR,Decousus H, et al. Oral rivaroxaban for symptomatic venousthromboembolism. N Engl J Med. 2010;363:2499–510.
18. EINSTEIN-PE Investigators, Büller HR, Prins MH, Lensin AW, Decousus H,Jacobson BF, et al. Oral rivaroxaban for the treatment of symptomaticpulmonary embolism. N Engl J Med. 2012;366:1287–97.
19. Agnelli G, Buller HR, Cohen A, Curto M, Gallus AS, Johnson M, et al. Oralapixaban for the treatment of acute venous thromboembolism. N Engl JMed. 2013;369:799–808.
20. Hokusai-VTE Investigators, Büller HR, Décousus H, Grosso MA,Mercuri M, Middeldorp S, et al. Edoxaban versus warfarin for thetreatment of symptomatic venous thromboembolism. N Engl J Med.2013;369:1406–15.
21. Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al.Antithrombotic therapy for VTE disease: CHEST guideline and expert panelReport. Chest. 2016;149:315–52.
22. Enden T, Haig Y, Kløw NE, Slagsvold CE, Sandvik L, Ghanima W, et al.Long-term outcome after additional catheter-directed thrombolysis versusstandard treatment for acute iliofemoral deep vein thrombosis (the CaVenTstudy): a randomised controlled trial. Lancet. 2012;379:31–8.
23. Watson L, Broderick C, Armon MP. Thrombolysis for acute deep veinthrombosis. Cochrane Database Syst Rev. 2014;1, CD002783.
24. Bashir R, Zack CJ, Zhao H, Comerota AJ, Bove AA. Comparative outcomes ofcatheter-directed thrombolysis plus anticoagulation vs anticoagulationalone to treat lower-extremity proximal deep vein thrombosis. JAMA InternMed. 2014;174:1494.
25. Laiho MK, Oinonen A, Sugano N, Harjola VP, Lehtola AL, Roth WD, et al.Preservation of venous valve function after catheter-directed and systemicthrombolysis for deep venous thrombosis. Eur J Vasc Endovasc Surg. 2004;28:391.
26. Vedantham S, Goldhaber SZ, Kahn SR, Julian J, Magnuson E, Jaff MR, et al.Rationale and design of the ATTRACT Study: a multicenter randomized trialto evaluate pharmacomechanical catheter-directed thrombolysis for theprevention of postthrombotic syndrome in patients with proximal deepvein thrombosis. Am Heart J. 2013;165:523–30.e3.
27. Grifoni S, Olivotto I, Cecchini P, Pieralli F, Camaiti A, Santoro G, et al. Short-term clinical outcome of patients with acute pulmonary embolism, normalblood pressure, and echocardiographic right ventricular dysfunction.Circulation. 2000;101:2817–22.
28. Sharifi M, Bay C, Skrocki L, Rahimi F, Mehdipour M. Moderate pulmonaryembolism treated With thrombolysis (from the “MOPETT” Trial). Am JCardiol. 2013;111:273–7.
29. Kline JA, Nordenholz KE, Courtney DM, Kabrhel C, Jones AE, RondinaMT, et al. Treatment of submassive pulmonary embolism withtenecteplase or placebo: cardiopulmonary outcomes at 3 months:multicenter double-blind, placebo-controlled randomized trial. JThromb Haemost. 2014;12:459–68.
30. Meyer G, Vicaut E, Danays T, Agnelli G, Becattini C, Beyer-Westendorf J, et al.Fibrinolysis for patients with intermediate-risk pulmonary embolism. N EnglJ Med. 2014;370:1402–11.
31. McCabe JM, Huang PH, Riedl L, Eisenhauer AC, Sobieszczyk P. Usefulnessand safety of ultrasound-assisted catheter-directed thrombolysis forsubmassive pulmonary emboli. Am J Cardiol. 2015;115:821–4.
32. Kuo WT, Banerjee A, Kim PS, DeMarco Jr FJ, Levy JR, Facchini FR, et al.Pulmonary embolism response to fragmentation, embolectomy, andcatheter thrombolysis (PERFECT): initial results from a prospectivemulticenter registry. Chest. 2015;148:667–73.
33. Kucher N, Boekstegers P, Müller OJ, Kupatt C, Beyer-Westendorf J, Heitzer T,et al. Randomized, controlled trial of ultrasound-assisted catheter-directedthrombolysis for acute intermediate-risk pulmonary embolism. Circulation.2014;129:479–86.
34. Koopman MM, Prandoni P, Piovella F, Ockelford PA, Brandjes DP, van derMeer J, et al. Treatment of venous thrombosis with intravenousunfractionated heparin administered in the hospital as compared withsubcutaneous low-molecular-weight heparin administered at home. TheTasman Study Group. N Engl J Med. 1996;334:682–7.
35. Levine M, Gent M, Hirsh J, Leclerc J, Anderson D, Weitz J, et al. Comparisonof low-molecular-weight heparin administered primarily at home withunfractionated heparin administered in the hospital for proximal deep-veinthrombosis. N Engl J Med. 1996;334:677–81.
36. Segal JB, Bolger DT, Jenckes MW, Krishnan JA, Streiff MB, Eng J, et al.Outpatient therapy with low molecular weight heparin for the treatment ofvenous thromboembolism: a review of efficacy, safety, and costs. Am J Med.2003;115:298–308.
37. Douketis JD. Treatment of deep vein thrombosis: what factors determineappropriate treatment? Can Fam Physician. 2005;51:217–23.
38. Aujesky D, Roy PM, Verschuren F, Righini M, Osterwalder J, Egloff M, et al.Outpatient versus inpatient treatment for patients with acute pulmonaryembolism: an international, open-label, randomised, non-inferiority trial.Lancet. 2011;378:41–8.
39. van Es N, Coppens M, Schulman S, Middeldorp S, Büller HR. Direct oralanticoagulants compared with vitamin K antagonists for acute venousthromboembolism: evidence from phase 3 trials. Blood. 2014;124:1968–75.
40. Lyman GH, Khorana AA, Kuderer NM, Lee AY, Arcelus JI, Balaban EP, et al.Venous thromboembolism prophylaxis and treatment in patients with
The Author(s) Thrombosis Journal 2016, 14(Suppl 1):23 Page 114 of 163

cancer: American Society of Clinical Oncology clinical practice guidelineupdate. J Clin Oncol. 2013;31:2189–204.
41. Engman CA, Zacharski LR. Low molecular weight heparins as extendedprophylaxis against recurrent thrombosis in cancer patients. J Natl ComprCanc Netw. 2008;6:637–45.
42. Prandoni P, Lensing AW, Piccioli A, Bernardi E, Simioni P, Girolami B, et al.Recurrent venous thromboembolism and bleeding complications duringanticoagulant treatment in patients with cancer and venous thrombosis.Blood. 2002;100:3484–8.
43. Meyer G, Marjanovic Z, Valcke J, Lorcerie B, Gruel Y, Solal-Celigny P, et al.Comparison of low-molecular-weight heparin and warfarin for thesecondary prevention of venous thromboembolism in patients with cancer:a randomized controlled study. Arch Intern Med. 2002;162:1729–35.
44. Lee AY, Levine MN, Baker RI, Bowden C, Kakkar AK, Prins M, et al.Low-molecular-weight heparin versus a coumarin for the prevention ofrecurrent venous thromboembolism in patients with cancer. N Engl J Med.2003;349:146–53.
45. Hull RD, Pineo GF, Brant RF, Mah AF, Burke N, Dear R, et al. Long-termlow-molecular-weight heparin versus usual care in proximal-vein thrombosispatients with cancer. Am J Med. 2006;119:1062–72.
46. Deitcher SR, Kessler CM, Merli G, Rigas JR, Lyons RM, Fareed J, et al.Secondary prevention of venous thromboembolic events in patients withactive cancer: enoxaparin alone versus initial enoxaparin followed bywarfarin for a 180-day period. Clin Appl Thromb Hemost. 2006;12:389–96.
47. Lee AY, Kamphuisen PW, Meyer G, Bauersachs R, Janas MS, Jarner MF, et al.Tinzaparin vs warfarin for treatment of acute venous thromboembolism inpatients with active cancer: A randomized clinical trial. JAMA. 2015;314:677–86.
48. Vedovati MC, Germini F, Agnelli G, Becattini C. Direct oral anticoagulants inpatients with VTE and cancer: a systematic review and meta-analysis. Chest.2015;147:475–83.
49. van Es N, Di Nisio M, Bleker SM, Segers A, Mercuri MF, Schwocho L, et al.Edoxaban for treatment of venous thromboembolism in patients withcancer. Rationale and design of the Hokusai VTE-cancer study. ThrombHaemost. 2015;114:1268–76.
50. Agnelli G, Buller HR, Cohen A, Curto M, Gallus AS, Johnson M, et al.Apixaban for extended treatment of venous thromboembolism. N Engl JMed. 2013;368:699–708.
51. Schulman S, Kearon C, Kakkar AK, Schellong S, Eriksson H, Baanstra D, et al.Extended use of dabigatran, warfarin, or placebo in venousthromboembolism. N Engl J Med. 2013;368:709–18.
52. Becattini C, Agnelli G, Schenone A, Eichinger S, Bucherini E, Silingardi M,et al. Aspirin for preventing the recurrence of venous thromboembolism.N Engl J Med. 2012;366:1959–67.
53. Brighton TA, Eikelboom JW, Mann K, Mister R, Gallus A, Ockelford P, et al.Low-dose aspirin for preventing recurrent venous thromboembolism.N Engl J Med. 2012;367:1979–87.
54. Simes J, Becattini C, Agnelli G, Eikelboom JW, Kirby AC, Mister R, et al.Aspirin for the prevention of recurrent venous thromboembolism: theINSPIRE collaboration. Circulation. 2014;130:1062–71.
55. Castellucci LA, Cameron C, Le Gal G, Rodger MA, Coyle D, Wells PS, et al.Efficacy and safety outcomes of oral anticoagulants and antiplatelet drugsin the secondary prevention of venous thromboembolism: systematicreview and network meta-analysis. BMJ. 2013;347:f5133.
56. Wiener RS, Schwartz LM, Woloshin S. When a test is too good: how CTpulmonary angiograms find pulmonary emboli that do not need to befound. BMJ. 2013;347:f3368.
57. Carrier M, Righini M, Le Gal G. Symptomatic subsegmental pulmonaryembolism: what is the next step? J Thromb Haemost. 2012;10:1486–90.
58. Stein PD, Goodman LR, Hull RD, Dalen JE, Matta F. Diagnosis andmanagement of isolated subsegmental pulmonary embolism: review andassessment of the options. Clin Appl Thromb Hemost. 2012;18:20–6.
59. Musset D, Parent F, Meyer G, Maître S, Girard P, Leroyer C, et al. Diagnosticstrategy for patients with suspected pulmonary embolism: a prospectivemulticentre outcome study. Lancet. 2002;360:1914–20.
60. Eyer BA, Goodman LR, Washington L. Clinicians' response to radiologists’reports of isolated subsegmental pulmonary embolism or inconclusiveinterpretation of pulmonary embolism using MDCT. AJR Am J Roentgenol.2005;184:623–8.
61. Donato AA, Khoche S, Santora J, Wagner B. Clinical outcomes in patientswith isolated subsegmental pulmonary emboli diagnosed by multidetectorCT pulmonary angiography. Thromb Res. 2010;126:e266–70.
62. Pena E, Kimpton M, Dennie C, Peterson R, LE Gal G, Carrier M. Difference ininterpretation of computed tomography pulmonary angiography diagnosisof subsegmental thrombosis in patients with suspected pulmonaryembolism. J Thromb Haemost. 2012;10:496–8.
63. Mehta D, Barnett M, Zhou L, Woulfe T, Rolfe-Vyson V, Rowland V, et al.Management and outcomes of single subsegmental pulmonary embolus: aretrospective audit at North Shore Hospital. New Zealand Intern Med J.2014;44:872–6.
64. Goy J, Lee J, Levine O, Chaudhry S, Crowther M. Sub-segmental pulmonaryembolism in three academic teaching hospitals: a review of managementand outcomes. J Thromb Haemost. 2015;13:214–8.
65. Ghazvinian R, Gottsäter A, Elf J. Is it safe to withhold long-termanticoagulation therapy in patients with small pulmonary emboli diagnosedby SPECT scintigraphy? Thromb J. 2016;14:12.
66. den Exter PL, van Es J, Klok FA, Kroft LJ, Kruip MJ, Kamphuisen PW, et al. Riskprofile and clinical outcome of symptomatic subsegmental acutepulmonary embolism. Blood. 2013;122:1144–9.
67. White RH, Brunson A, Romano PS, Li Z, Wun T. Outcomes after vena cavafilter use in non-cancer patients with acute venous thromboembolism:A population-based study. Circulation. 2016;133:2018–29.
68. Decousus H, Leizorovicz A, Parent F, Page Y, Tardy B, Girard P, et al. Aclinical trial of vena caval filters in the prevention of pulmonary embolismin patients with proximal deep-vein thrombosis. Prévention du Risqued’Embolie Pulmonaire par Interruption Cave Study Group. N Engl J Med.1998;338:409–15.
69. PREPIC Study Group. Eight-year follow-up of patients with permanent venacava filters in the prevention of pulmonary embolism: the PREPIC(Prevention du Risque d’Embolie Pulmonaire par Interruption Cave)randomized study. Circulation. 2005;112:416–22.
70. Mismetti P, Laporte S, Pellerin O, Ennezat PV, Couturaud F, Elias A, et al.Effect of a retrievable inferior vena cava filter plus anticoagulation vsanticoagulation alone on risk of recurrent pulmonary embolism: arandomized clinical trial. JAMA. 2015;313:1627–35.
71. Streiff MB. Vena caval filters: a comprehensive review. Blood. 2000;95:3669–77.72. Wu A, Helo N, Moon E, Tam M, Kapoor B, Wang W. Strategies for prevention
of iatrogenic inferior vena cava filter entrapment and dislodgement duringcentral venous catheter placement. J Vasc Surg. 2014;59:255–9.
• We accept pre-submission inquiries
• Our selector tool helps you to find the most relevant journal
• We provide round the clock customer support
• Convenient online submission
• Thorough peer review
• Inclusion in PubMed and all major indexing services
• Maximum visibility for your research
Submit your manuscript atwww.biomedcentral.com/submit
Submit your next manuscript to BioMed Central and we will help you at every step:
The Author(s) Thrombosis Journal 2016, 14(Suppl 1):23 Page 115 of 163