Embed Size (px)
Citation preview

ThrombocytopeniaThrombocytopeniaRahul Bhagat PGY1
01/24/12

Practical Importance of Assessing Practical Importance of Assessing ThrombocytopeniaThrombocytopenia
• 1/3 of all hematology consults are for 1/3 of all hematology consults are for thrombocytopeniathrombocytopenia
• 5 to 10% of all hospital patients are 5 to 10% of all hospital patients are thrombocytopenic in the ICU the number thrombocytopenic in the ICU the number increases to 35%increases to 35%
• Thrombocytopenic patients in the hospital Thrombocytopenic patients in the hospital suffer a twofold greater mortality rate than suffer a twofold greater mortality rate than those who are notthose who are not

Thrombocytopeina
• Definition: platelets < 150,000 • Normal platelets 150,000 - 450,000 • 2.5% of the normal population will have platelet
count lower than “normal” which is NOT abnormal• Platelets live for 8-10 days • Younger platelets are larger and work better

Platelets can be seen as individual structures forming on the periphery of this megakaryocyte

Clusters or chains of platelets are shed from the megakaryocyte and carried off into the bloodstream

Stratifying levels of thrombocytopeniaStratifying levels of thrombocytopenia
• The primary reason for evaluating thrombocytopenia The primary reason for evaluating thrombocytopenia is to assess the risk of bleeding and assess the is to assess the risk of bleeding and assess the presence of underlying disorders (TTP, HIT etc.)presence of underlying disorders (TTP, HIT etc.)– < 20 K increased risk of bleeding< 20 K increased risk of bleeding– 20K to 50 K rarely have increase risk of 20K to 50 K rarely have increase risk of
spontaneous bleeding but increase risk of spontaneous bleeding but increase risk of bleeding from proceduresbleeding from procedures
– 50K to 100K no increased risk of spontaneous 50K to 100K no increased risk of spontaneous bleeding and can undergo most proceduresbleeding and can undergo most procedures

Relation of bleeding risk and platelet countRelation of bleeding risk and platelet count
• Bleeding time increases in a linear fashion below a Bleeding time increases in a linear fashion below a platelet count of 100 Kplatelet count of 100 K
• Tagged RBC -> fecal blood lossTagged RBC -> fecal blood loss – 10 K 5 cc/day10 K 5 cc/day– 5 to 10 K 10 cc/day5 to 10 K 10 cc/day– < 5 K 50 cc/day< 5 K 50 cc/day

Organization of ThrombocytopeniaOrganization of Thrombocytopenia
• Decrease ProductionDecrease Production– Marrow DamageMarrow Damage
• AplasiaAplasia• DrugsDrugs• MalignancyMalignancy
– Congenital DefectsCongenital Defects– Ineffective ProductionIneffective Production
• B12, Folic Acid DefB12, Folic Acid Def
• Increase DestructionIncrease Destruction– Non ImmuneNon Immune
• DICDIC• TTPTTP• HELLPHELLP
– ImmuneImmune• ITPITP• HITHIT• SLE, AIDSSLE, AIDS• TTPTTP

Causes of Thrombocytopenia: Decreased Production
Marrow suppression (usually pancytopenic):– Post viral: parvo, Hep B/C, EBV, varicella, measles, mumps,
rubella, MMR vaccine, CMV, toxo, mono, influenza – Sepsis– Aplastic anemia– Direct megakaryocyte damage: HIV– Direct toxicity to bone marrow: XRT, chemo, alcohol– Marrow infiltration: lymphoma, Myelofibrosis, mets, TB
– Meds with toxic effect: (non immune mediated)• Thiazides, estrogens, septra, chemo, cimetidine, famotidine

Decreased Production (Continued)
– Malignancies: Myelodysplasia syndrome (age >60…usually anemic/leukopenic), leukemia, myeloma
– B12 or Folate deficiency (rare)– Congenital (Wiskott-Aldrich, Fanconi syndrome,
Bernard-Soulier)– PNH

Reasons to Suspect a Congenital Platelet Disorder
• Persistence of neonatal thrombocytopenia or onset of bleeding symptoms in childhood
• Family history of thrombocytopenia or mucocutaneous bleeding
• Platelet count unresponsive to typical treatments for ITP

A VERY common cause of “thrombocytopenia”

Work up
• First rule out pseudothrombocytopenia (EDTA agglutinin autoantibody mediated Platelet clumping
seen in 0.1%-0.2% of all blood draws)*Examine the smear*Repeat with heparinized/citrated tube*Repeat with fingerstick directly applied to slide*Note: pseudothrombocytopenia often accompanied by
falsely high WBC (machine counts platlet clumps as WBCs)

Work up• History
– Meds, meds meds– Alcohol– Nutrition– Travel– HIV risk factors– ? Occult malignancy– Bleeding history (gums,
menses, surgical complications).
– Family History
• Physical– Examine spleen– Detailed skin exam,
looking for• Petechiae: Red pinheads• Purpura: Purple confluent
petechaie• ecchymoses
– Look for lymphadenopathy



Work up (Continued)
• Peripheral smear– large platelets (hign MPV on CBC) imply increased
destructionearly release from marrow (ITP)– Normal/small platelets suggest reduced BM response– Schistocytes (fragmented RBCs): MAHA– Can reveal blasts– Treardrop RBC, nucleated RBCs can suggest marrow
invasion (tumor/fibrosis/granuloma)– Marcrocytosis with hypersegmented polys can suggest
Vitamin B/folate deficiency

Work up (Continued)
• PT/PTT (high in MAHA/DIC…liver disease)• LDH (hemolysis/MAHA)• Bun/Creatinine (HUS/TTP)• Consider HIV, ANA if clinical suspicion• Consider toxo, EBV, CMV serologies if lymphadenopathy,
splenomegaly, or “B” symptoms• Consider HIV(initial disease manifestation in 10%)• Consider ANA if clinical suspicion

Work up (continued)
• Bone marrow biopsy?– More definitively answers the “production vs. destruction”
question– Generally indicated in unexplained thromocytopenia if
platelet count low enough (5-10K) to be at risk for major bleeding…
*UNLESS age < 60, thrombocytopenia is isolated, and history/PE, and smear suggest the
diagnosis (of exclusion) of ITP.*If age > 60, and suspect likely ITP, BM biopsy generally indicated to r/o myleodysplasia

Immune Mediated Thrombocytopenia Immune Mediated Thrombocytopenia PurpuraPurpura
• ITP is defined as isolated thrombocytopenia with no clinically ITP is defined as isolated thrombocytopenia with no clinically apparent associated conditions or other causes of apparent associated conditions or other causes of thrombocytopeniathrombocytopenia
• ITP is a high prevalence disease ITP is a high prevalence disease – 16 to 27 per million per year16 to 27 per million per year
• Incidence increases with ageIncidence increases with age• Female predominance under the age of 60 Female predominance under the age of 60 • It can have an abrupt onset or insidious onset. It is generally It can have an abrupt onset or insidious onset. It is generally
abrupt in onset with childrenabrupt in onset with children

Pathogenesis of ITPPathogenesis of ITP
• Increased platelet destruction caused by Increased platelet destruction caused by antiplatelet antibodiesantiplatelet antibodies
• Lack of compensatory response by Lack of compensatory response by megakaryocytes due to suppressive effect of megakaryocytes due to suppressive effect of antiplatelet antibodiesantiplatelet antibodies
• Pathogenesis was proved by Harrington when Pathogenesis was proved by Harrington when he infused himself with plasma from a women he infused himself with plasma from a women with ITPwith ITP

Evaluation of ITPEvaluation of ITP
• Features consistent with the diagnosis of ITPFeatures consistent with the diagnosis of ITP– Thrombocytopenia with normal or slightly large plateletsThrombocytopenia with normal or slightly large platelets– Normal RBC morphology and number (may have Normal RBC morphology and number (may have
associated iron def or thallasemia etc.)associated iron def or thallasemia etc.)– Normal white cell number and morphologyNormal white cell number and morphology– Splenomegaly rare Splenomegaly rare
• Features not consistent with the diagnosis of ITPFeatures not consistent with the diagnosis of ITP– Giant plateletsGiant platelets– RBC abnormalities ie schisotocytesRBC abnormalities ie schisotocytes– Leukocytosis or LeukopeniaLeukocytosis or Leukopenia

Laboratory evaluation of ITPLaboratory evaluation of ITP
• Not MuchNot Much– Bone Marrow not very helpful as initial testBone Marrow not very helpful as initial test
• May be helpful in patient over 50 years and concerned May be helpful in patient over 50 years and concerned about MDSabout MDS
• If patient has failed initial treatment and diagnosis is in If patient has failed initial treatment and diagnosis is in questionquestion
– TSH and HIV test helpful, Peripheral Smear helpfulTSH and HIV test helpful, Peripheral Smear helpful

Management of ITPManagement of ITP
• Most patients with ITP do not have clinically Most patients with ITP do not have clinically significant bleedingsignificant bleeding– Risk of intracranial bleed 0.1 to 1% (This is an Risk of intracranial bleed 0.1 to 1% (This is an
overestimate)overestimate)– Wet Purpura ie epistaxis, gingival bleeding is a risk Wet Purpura ie epistaxis, gingival bleeding is a risk
factor for major bleedingfactor for major bleeding
• In asymptomatic patients with platelets In asymptomatic patients with platelets counts greater then 20 K observation is counts greater then 20 K observation is reasonablereasonable


Treatment of ITP
• If platelets > 20,000 and no bleeding…generally observe
• Steroids, benefit approx 2/3 of patients…but takes 3 weeks
• IVIG works more quickly (several days, and lasts several weeks)…used generally in actively bleeding patients while waiting for steroids to work
• Immunosupressive agents/splenectomy

Acute Pharmacologic Management of ITPAcute Pharmacologic Management of ITP
• SteroidsSteroids– Prednisone 1mg/kg/day with taper over 2 to 3 Prednisone 1mg/kg/day with taper over 2 to 3
monthsmonths– Decadron 40 mg/day x 4 daysDecadron 40 mg/day x 4 days– Solumedrol 1 gram/day x 2 daysSolumedrol 1 gram/day x 2 days
• AntibodiesAntibodies– IVIG 1 gram/day x 2 daysIVIG 1 gram/day x 2 days– Anti-D 50 mcg/kg IV x1Anti-D 50 mcg/kg IV x1

Chronic Management of ITPChronic Management of ITP• SplenectomySplenectomy
– Immunize with Pneumovax, Hib, Meningococcal Immunize with Pneumovax, Hib, Meningococcal
• Chronic Anti-D therapy Chronic Anti-D therapy – Does not put the disease in remissionDoes not put the disease in remission
• RituximabRituximab• EltrombopagEltrombopag
– FDA approved 2008FDA approved 2008– Agonist of TpoR receptor (target of thrombopoietin)Agonist of TpoR receptor (target of thrombopoietin)
• ObservationObservation

TTP Thrombotic Thrombocytopenia TTP Thrombotic Thrombocytopenia PurpuraPurpura
• TTP is characterized by microangiopathic TTP is characterized by microangiopathic hemolytic anemia and profound intravascular hemolytic anemia and profound intravascular platelet clumpingplatelet clumping
• The disease was first reported in 1923 at Beth The disease was first reported in 1923 at Beth Israel in NYCIsrael in NYC– 16 year old girl who presented with anemia, 16 year old girl who presented with anemia,
petechiae, coma and deathpetechiae, coma and death– Terminal arterioles and capillaries were occluded Terminal arterioles and capillaries were occluded
by hyaline thrombi mostly composed of plateletsby hyaline thrombi mostly composed of platelets

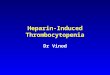
Figure 2. Peripheral smear showing RBC fragmentation consistent with a microangiopathic hemolytic process

Clinical and Lab Manifestations of TTPClinical and Lab Manifestations of TTP
• Severe thrombocytopenia and hemolytic anemia Severe thrombocytopenia and hemolytic anemia with one or several fragmented red cells with one or several fragmented red cells
• Neurologic manifestations, abdominal painNeurologic manifestations, abdominal pain• Fever and renal abnormalities occur in the minority Fever and renal abnormalities occur in the minority
of patientsof patients• Thrombocytopenia range from <30 K to 100 KThrombocytopenia range from <30 K to 100 K• Elevated LDHElevated LDH• Initially coagulation studies are normalInitially coagulation studies are normal

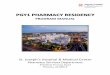
Proposed Relation among the Absence of ADAMTS 13 Activity in Vivo, Excessive Adhesion and Aggregation of Platelets, and Thrombotic Thrombocytopenic Purpura

Treatment of TTPTreatment of TTP
• Infusion of FFP 30 cc/kg/day until ready for Infusion of FFP 30 cc/kg/day until ready for plasma exchangeplasma exchange
• Daily plasma exchange with FFPDaily plasma exchange with FFP• Steroids (Prednisone 1 mg/kg/day)Steroids (Prednisone 1 mg/kg/day)• Red Blood Cells if neededRed Blood Cells if needed• Platelets only if absolutely necessaryPlatelets only if absolutely necessary

Increased Destruction: MEDICATIONS
• Mechanism of medthrombocytopenia is accelerated platelet destruction via drug dependent antibody
• Don’t forget about OTC meds, remedies– ASA, NSAIDS– Quinine (tonic water)
• Many, many meds can cause thrombocytopenia…and list constantly growing
• Median recovery after d/c of med is 5-7 days• If plts <10,000 or bleeding…transfuse (class 1B rec)

MedicationsThe Main Offenders
Heparin** AmiodaroneValproic acid/Carbamazepine Amphotericin BGold salts VancomycinQuinine/quinidine CimetidineBactrim/sulfonamides PhenytoinPenicillin/Beta lactams Clopidogril Interferon DigoxinGP 2b/3a inhibitors (abciximab) FluconazoleLinezolid Ranititidine

Heparin Induced ThrombocytopeniaHeparin Induced Thrombocytopenia
• Described in 1958 by Rodger Weismann and Described in 1958 by Rodger Weismann and Richard Tobin after extracting platelet fibrin Richard Tobin after extracting platelet fibrin thrombi that formed after 1 to 2 week course thrombi that formed after 1 to 2 week course of heparinof heparin
• HIT is the presence of a multimolecular HIT is the presence of a multimolecular complex between platelet factor 4, and complex between platelet factor 4, and heparinheparin
• HIT is associated with thrombosis despite HIT is associated with thrombosis despite profound thrombocytopeniaprofound thrombocytopenia


HIT
• Incidence: 0.2-5% of patients exposed to Heparin
• Factors predisposing one to HIT:– Longer duration of Heparin– Use of UFH (rather than LMWH/lovenox)– Surgical patient > medical patient– Female > male

Clinical Features of HITClinical Features of HIT
• TimingTiming– Onset between days 5 and 10 after heparin Onset between days 5 and 10 after heparin
initiationinitiation– Rapid onset if previously exposed to heparinRapid onset if previously exposed to heparin
• Thrombocytopenia nadir between 15K to 150KThrombocytopenia nadir between 15K to 150K• >50% develop a new thrombosis both venous >50% develop a new thrombosis both venous
and arterialand arterial• Absence of petechiaeAbsence of petechiae

Diagnosis of HITDiagnosis of HIT
• Clinical Suspicion (greater then 50% drop in Clinical Suspicion (greater then 50% drop in platelets in the setting of heparin use)platelets in the setting of heparin use)
• Laboratory StudiesLaboratory Studies– Platelet Activation Studies (Complicated and Platelet Activation Studies (Complicated and
physiologic)physiologic)– PF4/Polyanion Studies (Less time consuming but PF4/Polyanion Studies (Less time consuming but
not necessarily physiologic)not necessarily physiologic)• Even without evidence of thrombosis patient Even without evidence of thrombosis patient
should get lower extremity dopplersshould get lower extremity dopplers

Treatment of HITTreatment of HIT
• Removal of all Heparin productsRemoval of all Heparin products• Begin direct thrombin inhibitor (DTI) Begin direct thrombin inhibitor (DTI)
(Argatroban or Refludan)(Argatroban or Refludan)• Treat with DTI until platelet count normalizes Treat with DTI until platelet count normalizes
then may begin anticoaguation with coumadinthen may begin anticoaguation with coumadin• Fondaparinux (Arixtra) is a reasonable agent Fondaparinux (Arixtra) is a reasonable agent
to use for DVT prophylaxis in patient with to use for DVT prophylaxis in patient with history of HIThistory of HIT

What platelet level is “safe” ??
– Plts > 50K: surgery safe (except neurosurg)– Plts 30-50K: risk of major bleeding low. Rarely
have purpura.– Plts 10-30K: risk of mild-moderate bleeding
(especially with more extensive trauma).– Plts <10K: high risk for spontaneous hemorrhage
(esp if <5K). These patients have spontaneous bruising, and maybe petechiae…
• Avoid IM injections, rectal exams, enemas

When NOT to transfuse platelets
• Transfusions may induce immune resistance• Generally transfusions not given in conditions
of platelet destruction:– HUS/TTP– APLA unless severe– HIT CNS bleed or– DIC urgent invasive– Severe ITP procedure required

When TO transfuse platelets
• If platelets < 10,000 (risk of spont. Bleeding)• If <20,000 and active bleeding• If <40-50,000 prior to an invasive procedure
• Surgery -Childbirth• Central line -Tooth extraction• Thoracentesis
• If <100,000 prior to neurosurgery/epidural anesthesia
• 1 “unit” of platelets (“phoresed unit”) raises platelet count by about 20,000

Conclusion
• Think about thrombocytopenia in terms of etiology (destruction, decreased production, and “other”)
• History (especially MEDS) essential• Always rule out psuedo-thrombocytopenia• Peripheral smear tells you a lot• Think before you transfuse

Practical Aspects for the management of Practical Aspects for the management of thrombocytopeniathrombocytopenia
• What is an adequate platelet count for procedures?What is an adequate platelet count for procedures?– Routine Dentistry >10KRoutine Dentistry >10K– Dental Extraction >30KDental Extraction >30K– Regional Dental Block >30KRegional Dental Block >30K– Minor Surgery >50KMinor Surgery >50K– Major Surgery>80KMajor Surgery>80K– Epidural is okay at platelet count 50K for patient with ITPEpidural is okay at platelet count 50K for patient with ITP
• The target platelet count for a bleeding patient is The target platelet count for a bleeding patient is generally >40Kgenerally >40K
• Prophylactic platelet transfusions for platelets < 10KProphylactic platelet transfusions for platelets < 10K

Chief Complaint
• Patient is a 85 year old Caucasian female who presented to the ER with a chief complaint of generalized weakness x 3 months and 3 episodes of spontaneous epistaxis

History of Present Illness
85F totally independent in ADLs presented with 3 weeks of generalized fatigue, dizziness, lightheadedness
She reports having a spontaneous nosebleed the night prior to admission, bleeding for 4 hours, quantified 1 cup bright red blood
Patient c/o exertional dyspnea, needing 5-10 minutes of rest after 50-100 feet of walking.
She reports diffuse bruising over her upper and lower extremities for 3 months
She has been constantly tired, sleeping more.Denies fever, chills, chest pain

Medications
NKDA• Meclizine 25 QID since
11/11• Torsemide 25 OD• Synthroid 88mcg OD• Vytorin 10/20mg QHS• Lorazepam 0.5mg BID• Cymbalta 60mg OD• Lisinopril 5mg OD

Social History
• No history of tobacco or alcohol use• Patient independent in ADLs, lives alone,
drives• Father had leukemia at age 52

Physical Exam• VS: BP 112/43, Pulse 89, RR 18, T 98.0, SpO2 94% on RA, 0/10 pain• Gen: Patient seen resting in bed in NAD• Skin: diffuse >3cm ecchymosis over UE, >100 petechiae diffusely• HEENT: NCAT, PERRLA. No conjuctival pallor. No oropharyngeal
exudates. Petechiae visualized over soft palate.• Neck: No jugular venous distention, LAD, bruits• Chest: CTA B/L• CV: S1, S2 present,RRR. 2/6 systolic ejection murmur left parasternal
border. PMI nondisplaced. Pulses 2+ bilaterally. No peripheral edema.• Abdomen: Soft, tender to epigastrium, obese. No rebound tenderness.
Bowel sounds present. No shifting dullness• Ext: No clubbing, cyanosis, or erythema. No calf tenderness, palpable
nodules, or cords• Neuro: A&Ox3. Cranial nerves intact. Sensation intact. No focal deficits.
Decreased auditory acuity. Increasing forgetfulness

Labs
140 104 82 3.8 25 1.42 83
9.1
6.2 1026.7
Mg 2.8Phos 2.6
AST: 29ALT: 20Alk Phos: 36T. Bili: 0.9
RDW 17.1MCV 100.8AnisocytosisPolychromasiaMacrocytosis

• No acute intracranial process
• Moderate global cerebral atrophy



CT Abdomen
• Hepatomegaly with abnormal contour raises the possibility of underlying cirrhosis or hepatocellular disease.
• Excess vascularity in the left adrenal region may be due to underlying portal hypertension with variceal shunting.
• Suspect chronic partial small bowel obstruction.

• The patient vomited 1 episode coffee-ground emesis in ER, hemoccult grossly positive
• She was started on PRBC, platelet transfusion, transferred to ICU
• She was stepped down the following day and had no additional episodes of vomiting

Assessment/Plan• Profound symptomatic thrombocytopenia
– Secondary to ITP vs TTP vs MDS vs leukemia– Transfuse blood products as needed– Consult hematology
• Acute blood loss anemia– EGD, GI consult– Zofran, Protonix

Followup
• Patient underwent bone marrow biopsy on 1/16
• Histologic analysis demonstrated megaloblastic erythropoesis, ringed sideroblasts, hyposegmented granulocytes, moderate cellularity, without excess blasts
• Flow cytometry pending

Treatment
• Patient received 5 doses of IVIG and prednisone with no improvement
• Platelet count continued to remain ~2000• She was started on a 5 day cycle of Vidaza for
MDS on 1/19

• The patient remained profoundly symptomatic, refractory to blood product transfusion, and was stepped back up to the ICU for active acute blood loss