Embed Size (px)
Citation preview

Thrombocyte Adhesion and Release of Extracellular MicrovesiclesCorrelate with Surface Morphology of Adsorbent Polymers for LipidApheresisRene Weiss,† Andreas Spittler,‡ Gerd Schmitz,§ Michael B. Fischer,†,∥,⊥ and Viktoria Weber*,†,⊥
†Christian Doppler Laboratory for Innovative Therapy Approaches in Sepsis, Department for Health Sciences and Biomedicine,Danube University Krems, Austria‡Core Facility Flow Cytometry and Surgical Research Laboratories and ∥Department of Blood Group Serology and TransfusionMedicine, Medical University of Vienna, Austria§Institute for Clinical Chemistry and Laboratory Medicine, University of Regensburg, Germany
ABSTRACT: Whole blood lipid apheresis is clinically applied to reducelow density lipoprotein cholesterol in patients with homozygous familialhypercholesterolemia. Here, we studied the correlation betweenphysicochemical parameters, in particular, surface roughness and bloodcompatibility, of two polyacrylate-based and a dextran sulfate-basedpolymer for lipid apheresis. The adsorbent surface roughness was assessedby atomic force microscopy. Freshly isolated human thrombocytes werecirculated over adsorbent columns downscaled equivalent to clinical use tostudy thrombocyte adhesion and microvesicle generation. Quantification ofthrombocytes and microvesicles in the flow-through of the columnsrevealed that both thrombocyte adhesion and microvesicle generationincreased with increasing adsorbent surface roughness. Activation ofthrombocytes with thrombin receptor-activating peptide-6 favored theiradhesion to the adsorbents, as demonstrated by preferential depletion of CD62+ and PAC-1+ thrombocytes. Taken together,enhanced polymer surface roughness fostered cell adhesion and microvesicle release, underscoring the role of extracellularmicrovesicles as markers of cellular activation and of blood compatibility.
■ INTRODUCTION
The entry of low density lipoprotein (LDL) into the arterialwall and its retention through the binding of apolipoproteinB100 (apoB100) to proteoglycans of the extracellular matrix isregarded as a key initiator of atherogenesis.1−4 LDL undergoesenzymatic as well as nonenzymatic, free radical-mediatedoxidation in vivo, in particular, under conditions of hyper-lipidaemia.5−8 Oxidized LDL (oxLDL) acts as a damage-associated molecular pattern and is bound and internalized byscavenger receptors on macrophages, such as CD36 and SR-A.Unregulated uptake of oxLDL by macrophages stimulates thesecretion of pro-inflammatory cytokines and matrix degradingenzymes and leads to the formation of foam cells, a majorcomponent of atherosclerotic plaques.9,10 Thrombocytesactivated by oxidative stress and inflammation can adhere tothe endothelium, induce further leukocyte recruitment, andpromote the development of atherosclerotic lesions via P-selectin-dependent mechanisms, underscoring their contribu-tion to the maintenance and propagation of artheroscle-rosis.11−14
Patients suffering from homozygous familial hypercholester-olemia (FH) are unresponsive to diet and drug therapy andhave a markedly increased risk of developing atherosclerosisand its ischemic complications at an early age. Lowering of
LDL cholesterol levels in these patients can be achieved withLDL apheresis,15,16 This group of extracorporeal technologiescan selectively or specifically remove LDL and other apoB100containing lipoproteins, such as very low density lipoprotein,intermediate density lipoprotein, and lipoprotein (a), anindependent risk factor of coronary artery disease.17,18 SixLDL-apheresis systems are currently available for clinicalapplication. Four of these require the separation of plasmafrom blood cells prior to lipoprotein removal, while twosystems, DALI and Liposorber D, have been developed forlipoprotein adsorption directly from whole blood.19 DALI isbased on columns containing porous polyacrylamide beadsfunctionalized with anionic polyacrylate, and Liposorber Dconsists of cellulose beads functionalized with dextran sulfate.Both systems remove positively charged apoB100 containinglipoproteins by electrostatic interactions with the negativelycharged groups at the adsorbent surface. While these wholeblood adsorption systems are easy to handle and highly efficientsince they do not require plasma separation prior to adsorption,the direct contact of blood with artificial polymers demands a
Received: April 3, 2014Revised: May 17, 2014Published: May 20, 2014
Article
pubs.acs.org/Biomac
© 2014 American Chemical Society 2648 dx.doi.org/10.1021/bm500492r | Biomacromolecules 2014, 15, 2648−2655

great deal of blood compatibility to avoid or minimizeactivation of blood cells. Thrombocytes, in particular, undergoactivation and adhesion during contact with foreign surfaces,potentially leading to activation of coagulation and thrombo-cytopenia. Microvesicles released from activated platelets aremain culprits in the development of thrombotic events.20,21
They are intrinsically pro-coagulant due to their exposure ofphosphatidylserine, which interacts with vitamin K-dependentcoagulation factors and promotes coagulation. Microvesiclesmay also expose tissue factor, the primary initiator of thecoagulation cascade.The morphology and physicochemical parameters of
adsorbents used for whole blood lipid apheresis determinetheir adsorption characteristics, but also influence their bloodcompatibility. In this study, we assessed the impact of adsorbentmorphology, in particular, surface roughness, on thrombocyteadhesion and on the generation of microvesicles. Wedemonstrate that increased adsorbent surface roughnesscoincides with enhanced lipoprotein adsorption, but alsopromotes thrombocyte adhesion and microvesiculation.
■ EXPERIMENTAL SECTIONChemicals and Reagents. Phosphate buffered saline (PBS) was
purchased from Panreac, Barcelona, Spain. Priming solution (134 mMNa+, 4 mM K+, 1.75 mM Ca2+, 0.5 mM Mg2+, 106.5 mM Cl−, 36 mMHCO3−) and acid citrate dextrose solution A (ACD-A; 22.0 g/Ltrisodium citrate, 24.5 g/L glucose monohydrate, 7.3 g/L citric acid)were acquired from Fresenius Medical Care, Bad Homburg, Germany.Platelet storage medium SSP+ (3.18 g/L trisodium citrate dihydrate,4.42 g/L sodium acetate trihydrate, 1.05 g/L sodium dihydrogenphosphate dihydrate, 3.05 g/L disodium hydrogen phosphate, 0.37 g/L potassium chloride, 0.30 g/L magnesium chloride hexahydrate, 4.05g/L sodium chloride; pH 7.2) was purchased from Macopharma,Tourcoing, France. Unfractionated heparin was obtained fromGilvasan Pharma, Vienna, Austria. Thrombin receptor-activatingpeptide-6 (TRAP-6) was purchased from Bachem, Bubendorf,Switzerland.Plasma and Thrombocyte Concentrates. Freshly drawn human
plasma anticoagulated with heparin (2.5 IU/mL) was obtained from alocal plasma donation center after informed consent of the donors.The plasma was concentrated using an AlbuFlow filter (FreseniusMedical Care, Bad Homburg, Germany) to obtain a concentration oflow density lipoprotein (LDL) of 200−250 mg/dl.Thrombocyte concentrates (medical grade) were purchased from
the Clinic for Blood Group Serology and Transfusion Medicine,Medical University Vienna, Austria. The concentrates were producedusing a Trima Accel automated blood collection system (Version 5.0,Gambro BCT, Lund, Sweden) and stored for a maximum of 2 h at RTbefore use.Adsorbents. Two adsorbents which are approved for clinical
application in lipid apheresis from whole blood, DALI (FreseniusMedical Care, Bad Homburg, Germany) and Liposorber D (KanekaPharma Europe, Wiesbaden, Germany), were used in this study. DALIconsists of polyacrylamide beads functionalized with polyacrylate, andLiposorber D consists of cellulose beads functionalized with dextransulfate. Both adsorbents are negatively charged and bind toapolipoprotein B100 (apoB100) containing lipoproteins via electro-static interactions. A noncommercial polyacrylate-based resin function-alized with poly(acrylic acid) (ReliSorb) was tested in addition. Priorto use, adsorbent columns containing DALI and ReliSorb (6 × 1.8 cm;downscaled equivalent to clinical use) were rinsed with 2 × 20 mL ofpriming solution containing ACD-A (1:40), and 10 IU/mL of heparinwas supplemented during the first rinsing step. Liposorber D wasextensively washed with saline solution (0.9% w/v) prior to use.Characterization of Adsorbent Morphology, Surface Rough-
ness, and Porosity. Scanning electron microscopy was performed
using a JEOL T330 microscope (JEOL Ltd., Tokyo, Japan) aftersputtering the adsorbents with carbon.
The surface roughness of the adsorbents was characterized byamplitude modulation atomic force microscopy with a Dimension3100 Nanoscope IIIa (Veeco, Plainview, NY, U.S.A.) operated in thetapping mode. The following roughness parameters were determined:mean roughness, Ra, defined as arithmetic mean of the absolute valuesof the roughness profile ordinates; root-mean-square roughness, Rq,defined as the root-mean-square average of the roughness profileordinates; and the total height of the roughness profile, Rt, defined asthe distance between the highest peak and the lowest valley within thescanning length. Scanning length was 10 μm.
Specific surface area and pore size distribution of the adsorbentswere determined by recording nitrogen adsorption and desorptionisotherms at 77 K (liquid nitrogen) using an ASAP 2010 surface areaand porosimetry analyzer (Micromeritics Instrument Corporation,USA). Data analysis of the isotherms was performed using the BETmethod (Brunauer, Emmett, and Teller) for specific surface areadetermination. The average pore size diameter d(avg) was calculatedusing the total pore volume V(total) according to Gurwitsch’s rule[DIN 66134] and the specific surface area A as d(avg) = 4V(total)/A.
Adsorption of Lipoproteins. Human plasma was standardized toan LDL concentration of 200−250 mg/dl, as described above, andaliquots of the adsorbents (10% v/v) were incubated with plasma withgentle shaking at 37 °C. Samples were taken at 30, 60, and 90 min, theadsorbents were removed by centrifugation (3 min, 10.000g), and theconcentrations of LDL and HDL in the supernatant were determinedusing a Hitachi 902 Chemistry Analyzer and the reagent sets LDL-Cplus and HDL-C plus (all from Roche Diagnostics, Risch, Switzer-land). All experiments were carried out in triplicates.
Release of Microvesicles from Thrombocyte Concentratesupon Circulation over Adsorbents. To determine the generationof microvesicles from nonactivated thrombocytes upon contact withadsorbent polymers, freshly isolated thrombocytes (3 × 105/μL inSSP+ anticoagulated with ACD-A 1:12; total volume 50 mL) werecirculated over columns (3.5 × 1.8 cm, corresponding to a bed volumeof 19.7 mL; downscaled equivalent to clinical use) packed with therespective adsorbent materials at a constant flow rate of 1.2 mL permin for 2 h. An empty column served as negative control. Samples ofthe column-flow through were taken every 30 min, thrombocytes werequantified using a blood cell counter (Sysmex KX-21N, SysmexEurope, Neumunster, Germany), and microvesicles were determinedby flow cytometry as described below.
Flow Cytometric Characterization of Thrombocytes andMicrovesicles. Flow cytometric analysis was performed with a GalliosFlow Cytometer (Beckman Coulter, Brea, California, U.S.A.) afterstaining of thrombocytes and thrombocyte-derived microvesicles withan R-phycoerythrin-cyanine (PC7)-conjugated anti-CD61 monoclonalantibody (mAb; Becton Dickinson, Franklin Lakes, New Jersey,U.S.A.). Samples of the column flow through were diluted 1:83 in PBSprior to analysis. Calibration of the refractory index of microvesicleswas performed with fluorescent beads (Megamix, Biocytex, Marseille,France), as described in the manufacturer data sheet. The flowcytometer was adjusted to cover the microvesicle (0.5 and 0.9 μm) andthe thrombocyte size ranges (0.9 and 3 μm).
Activation of Thrombocytes. Thrombocytes (3 × 105/μL inSSP+ anticoagulated with ACD-A 1:12) were activated with increasingconcentrations of TRAP-6 (0; 2.5; 5; 10; 50; 100 μM) for 10 min atroom temperature in the dark and stained with a phycoerythrin (PE)-conjugated anti-CD-41 mAb as thrombocyte marker, with afluorescein isothiocyanate (FITC)-conjugated anti-CD62 mAb (Beck-man Coulter, Brea, California, U.S.A.) and a FITC-conjugated anti-PAC-1 mAb (Becton Dickinson, Franklin Lakes, New Jersey, U.S.A.)as thrombocyte activation markers, and with a FITC-conjugatedAnnexin V mAb (Becton Dickinson, Franklin Lakes, New Jersey,U.S.A.) as microvesicle marker. Samples were analyzed by flowcytometry as described above.
To assess the binding of activated thrombocytes to the adsorbentpolymers, freshly harvested thrombocytes (3 × 105/μL in SSP+anticoagulated with ACD-A 1:12; total volume 50 mL) were activated
Biomacromolecules Article
dx.doi.org/10.1021/bm500492r | Biomacromolecules 2014, 15, 2648−26552649

with TRAP-6 (50 μM) and circulated over a column packed with theDALI adsorbent at a flow rate of 1.2 mL per min for 2 h. A controlexperiment was performed under identical conditions using non-activated thrombocytes. Sampling, quantification of thrombocytes, andflow cytometric analysis were performed as described above.Statistical Analysis. Statistical analysis was performed using the
software package SPSS Statistics for Windows, version 18.0 (SPSS Inc.,Chicago, Illinois, U.S.A.). Data were analyzed using the Student’s ttest. Data are expressed as means ± standard error of the mean.Significance was accepted at P ≤ 0.05.
■ RESULTSMorphological Characterization of the Adsorbents.
The adsorbents for whole blood lipid apheresis used in this
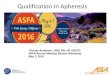
study were characterized morphologically by scanning electronmicroscopy and atomic force microscopy (Figure 1). The twopolyacrylate-based polymers had a specific surface area of 26m2/g for ReliSorb and 49 m2/g for DALI. The pore volume was1.4 and 1.7 mL per g dry adsorbent for ReliSorb and DALI,respectively, and their charge density was 300 and 530 μequivCOOH per g dry adsorbent. While the two adsorbentsexhibited a comparably structured inner surface, they showedclear differences with respect to their outer surface, whichappeared open and porous on scanning electron micrographsfor ReliSorb, while it had a closed and smooth appearance forDALI.
Figure 1. Scanning electron micrographs and surface roughness parameters of adsorbents for whole blood lipid apheresis. Representative scanningelectron micrographs of different adsorbent polymers (DALI, ReliSorb, Liposorber D) are shown (scale bars = 100, 30, and 3 μm). Surfaceroughness was determined by atomic force microscopy operated in the tapping mode. Ra, mean roughness (arithmetic mean of the absolute values ofthe roughness profile ordinates); Rq, root-mean-square roughness (root-mean-square average of the roughness profile ordinates); Rt, total height ofthe roughness profile (distance between the highest peak and the lowest valley within the scanning length). Scanning length was 10 μm.
Biomacromolecules Article
dx.doi.org/10.1021/bm500492r | Biomacromolecules 2014, 15, 2648−26552650

Amplitude modulation atomic force microscopy was used tocharacterize the surface roughness of the adsorbent polymers.In consistence with the morphological data obtained byscanning electron microscopy, surface roughness was lowerfor DALI as compared to ReliSorb and Liposorber D with amean roughness Ra of 84.8 versus 251 versus 148.9 nm,respectively, and a maximum height of the profile Rt of 777versus 1964 versus 1054 nm, respectively.Adsorption of LDL and HDL. The binding of low and high
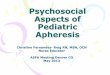
density lipoproteins was quantified in batch experiments usinghuman plasma which was standardized to initial LDLconcentrations of 200−250 mg/dl (Figure 2). DALI andLiposorber D bound comparable amounts of LDL over time(3.2 vs 3.5 mg LDL per mL adsorbent after 90 min), whileReliSorb showed significantly higher LDL binding (6.3 mg LDLper mL adsorbent after 90 min). Binding of HDL was negligiblefor all three adsorbents.Identification and Characterization of Microvesicles
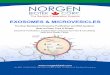
by Flow Cytometry. Microvesicles in the flow-through ofcolumns containing the different adsorbent polymers wereidentified and characterized by flow cytometry. Calibration wasperformed using a mix of fluorescent beads with diameters of0.5 and 0.9 μm to cover the microvesicle size range and 0.9 and3 μm to cover the thrombocyte size range (Figure 3). Themicrovesicle gate F was set around the cloud of the 0.9 μm
beads and microvesicles were quantified relative to the numberof total events.
Thrombocyte Adhesion and Release of Microvesicles.To study thrombocyte adhesion to the adsorbent polymers(Figure 4, upper panel), freshly isolated thrombocytes werecirculated over columns packed with DALI, ReliSorb, andLiposorber D, as described in the Experimental Section.Thrombocyte adhesion was significantly higher for ReliSorbas compared to DALI as calculated from the number ofthrombocytes remaining in the pool after 30, 60, 90, and 120min (195 ± 30 vs 246 ± 29 vs 300 ± 22 × 103/μL after 120min for ReliSorb vs DALI vs control without adsorbent). DALIand Liposorber D showed similar levels of thrombocyteadhesion (223 ± 41 vs 245 ± 46 vs 285 ± 42 × 103/μLafter 120 min for DALI vs Liposorber D vs control withoutadsorbent). Likewise, passage of thrombocytes over ReliSorbresulted in significantly higher levels of microvesicles (Figure 4,lower panel) as compared to DALI (5.7% vs 4.3% vs 4% of totalevents for ReliSorb vs DALI vs control without adsorbent after120 min). Again, Liposorber D and DALI showed comparablemicrovesicle release (4.4% vs 4.1% vs 3.8% for DALI vsLiposorber D vs control without adsorbent).
Activation of Thrombocytes with TRAP-6. Treatment ofthrombocytes with increasing amounts of TRAP-6 (0; 2.5; 5;10; 50; 100 μM) resulted in concentration-dependent
Figure 2. Adsorption of low density lipoprotein and high density lipoprotein by adsorbents for whole blood lipid apheresis. Adsorption was assessedin batch experiments in human plasma with an initial LDL concentration of 200−250 mg/dl using an adsorbent-to-plasma ratio of 1:9 (n = 3); *p <0.05.
Figure 3. Determination of microvesicles using flow cytometry. Fluorescent beads with diameters of 0.5, 0.9, and 3 μm, respectively, were used forcalibration according to the protocol of the supplier (Megamix, Biocytex, Marseille, France; left); the microvesicle gate (F) was set around the 0.9μm bead cloud (middle); example of microvesicles in a fresh thrombocyte concentrate (right); microvesicles were quantified in gate F relative to thenumber of total events.
Biomacromolecules Article
dx.doi.org/10.1021/bm500492r | Biomacromolecules 2014, 15, 2648−26552651

thrombocyte activation, as monitored by expression of theactivation marker CD62. The levels of CD62+CD41+
thrombocytes increased from 28% for untreated thrombocytesto 89% for thrombocytes treated with 50 and 100 μM TRAP-6(Figure 5a). A concentration of 50 μM TRAP-6 was used for allfurther experiments.Adhesion of Activated Thrombocytes to DALI.
Activated and nonactivated thrombocytes were circulated overDALI as described in Materials and Methods. Activatedthrombocytes adhered to DALI to a significantly higher extentthan nonactivated thrombocytes as calculated from the numberof thrombocytes remaining in the pool after 30, 60, 90, and 120min (126 ± 51 vs 232 ± 54 × 103/μL after 120 min foractivated vs nonactivated thrombocytes; Figure 5b). Activatedthrombocytes were preferentially bound by DALI, as reflectedby a decrease of CD41+ CD62+ thrombocytes from 96.2 to85.2% after 120 min (Figure 5c) and a decrease of CD41+
PAC-1+ thrombocytes from 42.4 to 17.7% after 120 min(Figure 5d). The number of CD41+ AnnexinV+ events in thethrombocyte region increased from 3.3% to 12.9% uponcirculation of activated thrombocytes over DALI, while no suchincrease was seen for nonactivated thrombocytes (Figure 5e,corresponding to region O in Figure 5f). We postulate that thetwo distinct populations in region O represent thrombocyte-microvesicle aggregates (T) and aggregates of thrombocyte-derived microvesicles (A), which are characterized by their highAnnexinV expression. Consequently, the relative amounts ofCD41+ AnnexinV+ microvesicles decreased during circulationof activated thrombocytes over DALI (Figure 5g) due to theiradhesion to either the adsorbent material, to thrombocytes, ordue to aggregation with other thrombocyte-derived micro-vesicles.
■ DISCUSSION
The morphology and physicochemical characteristics ofadsorbent polymers determine their blood compatibility nextto their adsorption capacity. Therefore, we studied thecorrelation between physicochemical parameters, in particular,surface roughness, and blood compatibility of three adsorbentsfor whole blood lipid apheresis. DALI and Liposorber D areclinically approved and applied to selectively remove theapoB100-containing lipoproteins LDL and Lp(a) from blood ofpatients suffering from familial hypercholesterolemia. Selectivebinding to their target substances is achieved by electrostaticinteractions between the negatively charged adsorbent surface(polyacrylate and dextran sulfate, respectively) and positivelycharged moieties of apoB100. As a third polymer, we includedReliSorb, a polyacrylate-based adsorbent, which is not yet inclinical application.The two polyacrylate-based polymers, DALI and ReliSorb,
exhibited clear differences in the structure of their outer surface,which appeared smooth and closed on scanning electronmicrographs for DALI, but open and porous for ReliSorb. Thisfinding correlated with atomic force microscopy, whereReliSorb exhibited higher surface roughness than DALI interms of all tested parameters. Due to its different chemicalcomposition, cellulose functionalized with dextran sulfate,Liposorber D is not directly comparable to DALI and ReliSorb,but in consistence with the appearance of its outer surface, itsroughness was higher than for DALI, but considerably lowerthan for ReliSorb.DALI and Liposorber D bound equal amounts of LDL,
which is in accordance with clinical data.22 Despite a lowercharge density, ReliSorb adsorbed significantly more LDL thanDALI and Liposorber D, reflecting a better accessibility of the
Figure 4. Generation of microvesicles and adhesion of thrombocytes upon circulation of thrombocyte concentrates over adsorbents for whole bloodlipid apheresis. Freshly isolated thrombocytes (3 × 105/μL in SSP+) were circulated over columns, as described in the Experimental Section. At theindicated time points, thrombocytes (upper panel) and microvesicles (lower panel) in the flow-through were quantified using a blood cell counterand flow cytometry, respectively (n = 5); *p < 0.05.
Biomacromolecules Article
dx.doi.org/10.1021/bm500492r | Biomacromolecules 2014, 15, 2648−26552652

Figure 5. Binding of activated thrombocytes to DALI. Thrombocytes were activated with TRAP-6, circulated over columns containing DALI, andsamples of the flow-through were analyzed by flow cytometry as described in the Experimental Section. CD41 was used as thrombocyte marker, andCD62 and PAC-1 served as markers of thrombocyte activation: (a) correlation between TRAP-6 concentration and thrombocyte activation; (b)adhesion of activated and nonactivated thrombocytes to DALI as assessed by blood cell counting; (c, d) binding of activated and nonactivatedthrombocytes to DALI as assessed by flow cytometry using CD62 or PAC-1 as activation markers; (e) binding of microvesicles to thrombocytesreflected by CD41+ AnnexinV+ events in the thrombocyte region, corresponding to region O (upper right quadrant) in (f). The two populations Tand A represent thrombocyte-microvesicle aggregates (T) and aggregates of thrombocyte-derived microvesicles (A). All experiments shown in (b−f)were performed with 50 μM TRAP-6. (g) Relative amounts of CD41+ AnnexinV+ events (thrombocyte-derived microvesicles), CD41+ AnnexinV−
events, CD41− AnnexinV+ events (microvesicles of nonthrombocyte origin, most likely, erythrocyte-derived), and CD41− AnnexinV− events (n = 5);*p < 0.05.
Biomacromolecules Article
dx.doi.org/10.1021/bm500492r | Biomacromolecules 2014, 15, 2648−26552653

inner adsorbent surface of ReliSorb for the large low densitylipoprotein complex. Binding of high density lipoprotein wasnegligible for all three adsorbents, since HDL does not containapoB100 and therefore lacks the positively charged moietiesthat mediate adsorption to anionic polymers. Under identicalexperimental conditions, cellulose beads functionalized withphenyl groups (Cellufine Phenyl, JNC Corporation, Japan)exhibited excellent LDL adsorption due to hydrophobicinteractions between LDL and the phenyl groups on thepolymer surface (data not shown). These resins, however,resulted in a reduction of HDL levels by almost 50%, whichprecludes their application in lipid apheresis, since HDLrepresents an important atheroprotective factor11 due to itsability to mediate reverse cholesterol transport23 and due to itsantioxidative as well as anti-inflammatory properties.24
Owing to their direct contact with blood during lipidapheresis, the blood compatibility of the adsorbents is of criticalimportance to minimize activation and adhesion of blood cellsand inflammatory response. We hypothesized that activationand adhesion of blood cells, in particular, thrombocytes, mightcorrelate with the polymer surface roughness. Affirming thisassumption, we observed significantly higher thrombocyteadhesion for ReliSorb as compared to DALI and LiposorberD during circulation of freshly isolated thrombocytes overcolumns containing the different adsorbent polymers. Ourhypothesis was further substantiated by flow cytometricdetection of thrombocyte-derived microvesicles in the flow-through of the adsorbent columns. Again, microvesicle releasecorrelated with surface roughness and was significantly higherfor ReliSorb as compared to DALI, adding evidence to therelevance of microvesicles as markers of cellular activation.There is emerging evidence for thrombocyte-derived micro-vesicles as players in thrombotic and inflammatory diseases25
apart from their participation in homeostatic multicellularprocesses such as hemostasis, maintenance of vascular health,and immunity, and our findings suggest that they can also serveas markers for blood compatibility of polymers.Treatment of thrombocytes with thrombin receptor-activat-
ing peptide-6 resulted in a dose dependent up-regulation ofthrombocyte activation markers CD62 (platelet surface P-selectin) and PAC-1 (activated GP IIb/IIIa). The activation ofthrombocytes correlated with their adhesion to DALI, and flowcytometric analysis revealed preferential adhesion of activatedvs nonactivated thrombocytes as suggested by the preferentialdepletion of CD62+ and PAC-1+ thrombocytes. The appear-ance of significantly increased numbers of AnnexinV+
thrombocytes in the flow through of the DALI column foractivated vs nonactivated thrombocytes provided a strongindication of microvesicle adhesion to thrombocytes. It is thusto be assumed that microvesicles do not only adhere to theadsorbent polymers, but also to activated platelets and to eachother, forming strongly AnnexinV-positive aggregates in thethrombocyte size range.Changes in thrombocyte shape may simply be held
responsible for their enhanced interaction with adsorbentpolymers and microvesicles, but it seems likely that there areother mechanisms fostering this interaction. Platelet factor 4(PF4), a platelet-specific chemokine, is released in largeamounts by activated platelets and expressed on the plateletsurface. Under physiological conditions, PF4 is positivelycharged, as reflected by its interaction with glycosaminoglycansof the endothelial layer. It is therefore tempting to assume thatthe expression of positively charged PF4 on the platelet surface
may boost the interaction of activated thrombocytes with both,negatively charged adsorbents and with microvesicles exposingnegatively charged phosphatidylserine residues on their surface.Consistently, LDL apheresis with Liposorber D and DALI hasbeen shown to reduce PF4 on the platelet surface,26 which wasexplained as a re-equilibration mechanism following depletionof plasma-derived PF4 by LDL adsorbent columns.Lipoprotein (a) may be another player in the setting of
platelet activation induced by LDL apheresis. Although itsphysiological function remains to be fully elucidated, there arestrong indications for its pro-thrombotic role. It has beenshown to promote platelet activation via thrombin-receptor-activated hexapeptide, and it induces production and surfaceexposure of tissue factor on monocytes.27,28 Taking these datatogether, Lp(a) attached to anionic adsorbents via its positivelycharged apoB100 moiety may promote tissue factor up-regulation on platelets, resulting in local thrombin generationand inducing a positive feedback loop toward furtherthrombocyte activation and adhesion.Our study was performed with thrombocyte concentrates,
while we are aware that proteins which rapidly coat a surfacefollowing its exposure to whole blood profoundly influence celladhesion. Among the numerous proteins, which may beadsorbed to a biomaterial surface, fibrinogen has been identifiedas a main inducer of platelet activation. Noteworthy, it has beendemonstrated that platelet adhesion is strongly correlated withthe degree of adsorption-induced protein unfolding.29,30
■ CONCLUSIONSThe physicochemical parameters and the morphology ofadsorbents for extracorporeal blood purification determinetheir binding of target factors and their blood compatibility.The results of this study indicate that the adhesion ofthrombocytes as well as the release of AnnexinV+ microvesiclescorrelate with morphology and surface roughness of adsorbentsfor whole blood lipid apheresis. Thrombocyte activationfostered their adhesion to adsorbent polymers, and theappearance of AnnexinV+ thrombocytes provided evidence forthe adhesion of microvesicles to activated thrombocytes.Binding of activated thrombocytes to adsorbents and micro-vesicles may be mediated by positively charged proteins, such asplatelet factor 4, which is released from activated thrombocytes.While the influence of adsorbent morphology on thrombo-
cyte adhesion and microvesicle release was a major topic of thisinvestigation, chemical parameters such as the effective chargedensity, the distribution, and the accessibility of functionalgroups on the adsorbent may have additional impact, which willbe elucidated in further studies using whole blood. This willalso allow to determine the cellular origin of the microvesiclesreleased during contact of blood with the adsorbents and tostudy the influence of deposited plasma proteins on theadhesion of blood cells.
■ AUTHOR INFORMATIONCorresponding Author*Phone: ++43 2732 893 2632. Fax: ++43 2732 893 4600. E-mail: [email protected] Contributions⊥Both authors contributed equally to this work (M.B.F. andV.W.).NotesThe authors declare no competing financial interest.
Biomacromolecules Article
dx.doi.org/10.1021/bm500492r | Biomacromolecules 2014, 15, 2648−26552654

■ ACKNOWLEDGMENTSThe excellent technical support by Ingrid Linsberger isgratefully acknowledged. The authors are grateful to TanjaEichhorn for support with preparation of figures. This work wasfunded by the Christian Doppler Society (Christian DopplerLaboratory for Innovative Therapy Approaches in Sepsis).
■ REFERENCES(1) Maiolino, G.; Rossitto, G.; Caielli, P.; Bisogni, V.; Rossi, G. P.;Calo, L. A. Mediators Inflammation 2013, 714653.(2) Tabas, I.; Williams, K. J.; Boren, J. Circulation 2007, 116, 1832−1844.(3) Skalen, K.; Gustafsson, M.; Rydberg, E. K.; Hulten, L. M.;Wiklund, O.; Innerarity, T. L.; Boren, J. Nature 2002, 417, 750−754.(4) Miller, Y. I.; Soo-Ho, C.; Wiesner, P.; Fang, L.; Harkewicz, R.;Hartvigsen, K.; Boullier, A.; Gonen, A.; Diehl, C. J.; Que, X.; Montano,E.; Shaw, P. X.; Tsimikas, S.; Binder, C.; Witztum, L. Circ. Res. 2011,108, 235−248.(5) Podrez, E. A.; Abu-Soud, H. M.; Hazen, S. L. Free Radic. Biol.Med. 2000, 28, 1717−1725.(6) Chisolm, G. M.; Steinberg, D. Free Radic. Biol. Med. 2000, 28,1815−1826.(7) Shao, B.; Heinecke, J. W. J. Lipid Res. 2009, 50, 599−601.(8) Miller, Y. I.; Choi, S.-H.; Fang, L.; Tsimikas, S. Subcell. Biochem.2010, 51, 229−251.(9) Steinberg, D.; Witztum, J. L. Arterioscler. Thromb. Vasc. Biol. 2010,30, 2311−2316.(10) Riches, K.; Porter, K. E. Cholesterol 2012, 923289.(11) Badrnya, S.; Assinger, A.; Volf, I. Int. J. Mol. Sci. 2013, 14,10107−10121.(12) Badrnya, S.; Butler, L. M.; Soderberg-Naucler, C.; Volf, I.;Assinger, A. Thromb. Haemost. 2012, 108, 719−729.(13) Badrnya, S.; Schrottmaier, W. C.; Kral, J. B.; Yaiw, K.-C.; Volf, I.;Schabbauer, G.; Soderberg-Naucler, C.; Assinger, A. Arterioscler.Thromb. Vasc. Biol. 2014, 34, 571−580.(14) Burger, P. C.; Wagner, D. D. Blood 2003, 101, 2661−2666.(15) Ueda, M. Mol. Genet. Metab. 2005, 86, 423−426.(16) Soutar, A. K.; Naoumova, R. P. Nat. Clin. Pract. Cardiovasc. Med.2007, 4, 214−225.(17) Bosch, T.; Lennertz, A.; Schmidt, B.; Fink, E.; Keller, C.;Toepfer, M.; Drager, J.; Samtleben, W. Artif. Organs 2000, 24, 81−90.(18) Stefanutti, C.; Morozzi, C.; Petta, A. Cytokine 2011, 56, 842−849.(19) Winters, J. L. J. Clin. Apher. 2011, 26, 269−275.(20) Del Conde, I.; Shrimpton, C. N.; Thiagarajan, P.; Lopez, J. A.Blood 2005, 106, 1604−1611.(21) Siljander, P. R. Thromb. Res. 2011, 127, S30−33.(22) Otto, C.; Berster, J.; Otto, B.; Parhofer, K. G. J. Clin. Apher.2007, 22, 301−305.(23) Fielding, C. J.; Fielding, P. E. J. Lipid Res. 1995, 36, 211−228.(24) Nofer, J. R.; Kehrel, B.; Fobker, M.; Levkau, B.; Assmann, G.;von Eckardstein, A. Atherosclerosis 2002, 161, 1−16.(25) Aatonen, M.; Gronholm, M.; Siljander, P. R. Semin. Thromb.Hemost. 2012, 38, 102−113.(26) Tanhehco, Y. C.; Rux, A. H.; Sachais, B. S. Transfusion 2011, 51,1022−1029.(27) Riches, K.; Porter, K. E. Cholesterol 2012, 923289.(28) Rand, M. L.; Sangrar, W.; Hancock, M. A.; Taylor, D. M.;Marcovina, S. M.; Packham, M. A.; Koschinsky, M. L. Arterioscler.Thromb. Vasc. Biol. 1998, 18, 1393−1399.(29) Sivaraman, B.; Latour, R. A. Biomaterials 2010, 31, 832−839.(30) Sivaraman, B.; Latour, R. A. Biomaterials 2011, 32, 5365−5370.
Biomacromolecules Article
dx.doi.org/10.1021/bm500492r | Biomacromolecules 2014, 15, 2648−26552655