Embed Size (px)
Citation preview

Journal of Applied Biomechanics, 2013, 29, 214-228 © 2013 Human Kinetics, Inc. An Official Journal of ISB
www.JAB-Journal.comTECHNICAL NOTE
214
Lennart Scheys is with the European Centre for Knee Research, Smith & Nephew, Leuven, Belgium. Alberto Leardini is with the Movement Analysis Laboratory, Istituto Ortopedico Rizzoli, Bologna, Italy. Pius D. Wong is with the European Centre for Knee Research, Smith & Nephew, Leuven, Belgium. Laurent Van Camp is with the Department of Medicine, Katholieke Universiteit Leuven, Leuven, Belgium. Barbara Callewaert is with the Clinical Motion Analysis Laboratory, University Hospital Pellenberg, Katholieke Universiteit Leuven, Leuven, Belgium. Johan Bellemans is with the Department of Medicine, Katholieke Universiteit Leuven, and with the Department of Orthopedics, University Hospital Pellenberg, Katholieke Universiteit Leuven, Leuven, Belgium. Kaat Desloovere (Cor-responding Author) is with the Clinical Motion Analysis Labo-ratory, University Hospital Pellenberg, Katholieke Universiteit Leuven, and with the Department of Rehabilitation Science, Katholieke Universiteit Leuven, Leuven, Belgium.
Three-Dimensional Knee Kinematics by Conventional Gait Analysis for Eleven Motor Tasks
of Daily Living: Typical Patterns and Repeatability
Lennart Scheys,1 Alberto Leardini,2 Pius D. Wong,1 Laurent Van Camp,3 Barbara Callewaert,3 Johan Bellemans,3 and Kaat Desloovere3
1Smith & Nephew, Inc., Leuven; 2Istituto Ortopedico Rizzoli; 3Katholieke Universiteit Leuven
The availability of detailed knee kinematic data during various activities can facilitate clinical studies of this joint. To describe in detail normal knee joint rotations in all three anatomical planes, 25 healthy subjects (aged 22–49 years) performed eleven motor tasks, including walking, step ascent and descent, each with and without sidestep or crossover turns, chair rise, mild and deep squats, and forward lunge. Kinematic data were obtained with a conventional lower-body gait analysis protocol over three trials per task. To assess the repeat-ability with standard indices, a representative subset of 10 subjects underwent three repetitions of the entire motion capture session. Extracted parameters with good repeatability included maximum and minimum axial rotation during turning, local extremes of the flexion curves during gait tasks, and stride times. These specific repeatable parameters can be used for task selection or power analysis when planning future clinical studies.
Keywords: motion analysis, 3D knee kinematics, repeatability, high-demand motor tasks
Numerous studies have demonstrated the beneficial role of gait analysis in the planning and evaluation of surgical treatments at the human knee joint. Most studies confine their research to flexion-extension during indi-vidual tasks, such as normal walking.1–3 This is mainly because motor tasks most frequently studied induce only small knee rotations out of the sagittal plane. These rotations are therefore difficult to measure accu-rately and reliably, given the sources of relatively large error involved in in vivo testing with external skin mark-ers.4 Despite limited availability of data documenting
three-dimensional knee kinematics,5–7 clinical interest in three-dimensional (3D) knee kinematics increased, especially during motor tasks inducing more out-of-sagittal plane motion.
Unfortunately, also repeatability data on 3D knee rotations during these tasks are not widely available. However, such data are crucial for the design of relevant clinical experiments, for example, for defining patient sample sizes. Consequently, it is difficult to involve complex motor tasks in clinical studies, since the quality of measurements from many of these tasks is unknown. The goal of the current study is to describe in detail the typical kinematics of knee joint rotation decomposed in the three anatomical planes for eleven motor tasks, as well as the repeatability within subjects of these knee joint rotation curves and specific parameters derived thereof.
Knowledge of joint motion and repeatability for each of these tasks can be used as a reference for the design of studies on pathological knees. The kinematics can be used as a guide for selecting the most suitable task to study, while the repeatability analysis of these tasks would serve as a crucial data source for power analyses when setting up clinical knee studies.
Methods
Sample CharacteristicsEthical approval was given by the University Hos-pital Pellenberg. Twenty-five healthy adult subjects

3-D Knee Kinematics for Motor Tasks of Daily Living 215
participated in this study after giving informed consent. They included 13 males and 12 females, with mean age of 32.9 (SD 9.8) years, range 22–49 years, mean weight 70.7 (SD 16.7) kg, mean height 1.74 (SD .09) m, and mean body mass index (BMI) 23.3 (SD 4.5).
Motion Capture
Kinematic data were obtained at 100 Hz using a motion capture system with eight to fourteen infrared cameras (Vicon, Oxford, UK), which determined the 3D trajec-tories of 23 passive retro-reflective spherical markers (14 mm diameter) fixed onto the skin over anatomical landmarks of the lower limbs and trunk (Full Body Plug-in-Gait marker set, Vicon, Oxford, UK) identified accord-ing to the guidelines by Van Sint Jan.8 Malalignment of the knee flexion axis is known to result in cross-talk between sagittal and coronal knee motion.9 Therefore, at least three knee alignment device (KAD)10 calibration trials were taken at the beginning of each session, and the trial that produced the minimum excursion of knee abduction-adduction during the swing phase of walking was selected for calibrating the remaining trials.
Motor Tasks
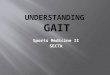
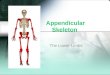
During each session, the subject was asked to perform eleven different motor tasks, with three repetitions each (Figure 1). Two subjects, with BMI over 30, declined to perform the deep squat because of its difficulty.
This specific set of motor tasks was selected because some of these induce greater motion at the knee joint.11
Data Analysis and Reduction
Thirteen right and 12 left lower limbs were randomly selected (one limb per subject) for further analysis. All walking and ascent/descent tasks were classified as “gait tasks” since these have both stance and swing phases, detected according to foot contact with the forceplates. Chair rise cycles were defined to start when the upper body began to lean forward until the time of maximal knee extension. Squat cycles were defined between times of maximal knee extension. The lunge cycle was defined between foot-strike and lift-off. All data were normalized to a 0 to 100% time cycle. Corresponding kinematics curves were grouped together according to subjects and tasks and averaged at each percentage cycle.
Repeatability Analysis
To detail within-subject measurement consistency of knee joint rotations, a subset of 10 subjects (sex: 9 male, 1 female; age: 29 ± 9 y; weight: 76 ± 20 kg; height: 178 ± 8 cm, BMI: 24 ± 5; these included the two high-BMI subjects who did not perform the deep squat) underwent two additional motion capture sessions, all conducted by the same well-trained physical therapist. The interval between these sessions ranged from 5 hours to 56 days (median = 7 days).
Based on the 9 trials collected for each motor task—equally spread over three motion analysis ses-sions—the following parameters of repeatability were calculated: within-subject coefficient of multiple correla-tion (CMC),12 average within-subject root-mean-squared error (RMS) against the average, and mean absolute variability.13
In addition, we analyzed the repeatability of a set of kinematic and temporal parameters commonly extracted from knee rotation curves14 (Tables 1–2) based on the mean within-subject standard deviation (SD) and coef-ficient of variation (CV)12 as well as the one-way random effects model intraclass correlation coefficient (ICC).15 Measurements were considered to have “good” repeat-ability if they showed a high ICC (0.8 to 1), low SD (<5°), low CV (<15%), or any combination of the three. These thresholds were chosen based on a recent relevant review.2
ResultsThe knee joint rotations measured in all 25 subjects resulted in a detailed description of knee kinematics during 11 different motor tasks in typical, healthy sub-jects (Figures 2–4). Furthermore, considerably different patterns were found among the tasks’ ensemble-averaged knee kinematics curves. Gait tasks (Figures 2 and 3) showed knee joint rotation curves with consistent patterns in all three anatomical planes, most clearly for flexion-extension. Crossover turns notably produced flatter flexion curves at terminal stance, corresponding to more knee flexion compared with the other walking and descent tasks. Knee abduction-adduction was larger in swing than in stance for all gait tasks. Axial rotation curves for walk-ing resembled those of the descent tasks; in both types of tasks, crossover and sidestep turns increased the range of axial rotation by factors of 1.5 and 2, respectively, com-pared with moving straight ahead. Stride times ranged from a mean of 1.049 s for straight walking to 1.458 s for ascent (Appendix Table 1). Nongait tasks (Figure 4) showed smoother patterns of the out-of-sagittal plane rotations. Furthermore, the patterns of the axial rota-tion were proportional to those of the corresponding flexion-extension curves, demonstrated also by highly significant correlations between the averages of these joint rotations in all motor tasks (Rchair rise = 0.988, Rlunge = 0.939, Rmild squat = 0.981, Rdeep squat = 0.993). Overall, the tasks showing the largest internal rotation were the crossover turns and the high-flexion tasks of ascent, chair rise, squat, and lunge (Figures 2–4). The tasks show-ing the largest external rotation were the sidestep turns (Figures 2–3). The crossover turns also showed smaller adduction peaks (Figures 2–3), compared with normal walking (Figure 2).
Further analysis in a subgroup of 10 subjects docu-mented, for each task, the repeatability within subjects of knee joint rotation curves (Figures 2–4). CMC values for all flexion-extension curves were greater than 0.92, whereas those for abduction-adduction and knee rotation curves were all less than 0.82 and 0.92, respectively. RMS

216
Figure 1 — Overview of the eleven motor tasks, defined as in Desloovere et al, 2010,11 that were performed in the displayed order—approximately according to increasing difficulty: walking at self-selected speed (A), walking followed by a 90° cross-over (B) and sidestep turn (C), ascent (D) and descent (E) on/from a step, descent followed by again crossover (F) and sidestep turn (G), chair rise (H), mild squat (I), deep squat (J) and lunge (K). When relevant, the analyzed leg is shown with a dark, gray overlay.

217
Tab
le 1
M
ean
wit
hin
-su
bje
ct S
D, m
ean
wit
hin
-su
bje
ct C
V, a
nd
ICC
val
ues
for
fou
rtee
n s
elec
ted
par
amet
ers
extr
acte
d f
rom
th
e kn
ee k
inem
atic
s cu
rves
of
seve
n g
ait
mo
tor
task
s
Kin
emat
ics
Para
met
ers
Tem
pora
l Par
amet
ers
12
34
56
78
910
1112
1314
Task
Mid
stan
ce
max
. fle
xion
(°
)
Term
inal
st
ance
min
. fle
x-ex
t. (°
)
Mid
swin
g m
ax.
flexi
on (°
)
Max
. ad
-duc
tion
(°)
Max
. in
tern
al
rota
tion
(°)
Max
. ex
tern
al
rota
tion
(°)
Str
ide
time
(s)
Sta
nce
time
(s)
%C
yc
at (1
)%
Cyc
at
(2)
%C
yc
at (3
)%
Cyc
at
(4)
%C
yc
at (5
)%
Cyc
at
(6)
Mea
n
W
alk
17.8
2.8
63.9
8.8
12.0
–4.4
1.04
60.
627
12.2
38.2
71.3
74.5
49.8
71.7
W
alk+
CO
18.8
*9.
264
.35.
918
.6–2
.41.
270
0.80
511
.8*
40.1
75.8
65.4
52.2
40.5
W
alk+
SS18
.90.
859
.28.
513
.6–1
0.3
1.26
10.
773
10.6
41.5
74.3
64.9
43.9
52.5
A
scen
t63
.426
.795
.510
.917
.3–0
.51.
507
1.04
74.
443
.777
.550
.967
.073
.6
D
esce
nt31
.36.
764
.68.
313
.0–3
.51.
124
0.68
313
.942
.772
.174
.437
.662
.6
D
esce
nt+
CO
30.6
10.7
64.1
6.4
17.1
–2.9
1.35
60.
883
13.5
44.1
77.1
66.0
47.7
47.6
D
esce
nt+
SS33
.33.
158
.38.
913
.5–1
2.0
1.35
30.
835
12.2
45.0
75.3
68.4
23.5
57.1
Stan
dard
dev
iati
on (
SD)
W
alk
3.2
1.7
2.5
1.9
3.8
3.2
0.03
50.
025
1.4
1.8
1.1
4.8
28.1
14.2
W
alk+
CO
4.4*
2.5
3.4
2.2
4.3
4.7
0.07
40.
059
2.1*
8.6
1.4
20.6
13.9
24.7
W
alk+
SS4.
02.
23.
12.
43.
43.
30.
072
0.05
91.
75.
01.
59.
529
.67.
3
A
scen
t6.
05.
03.
23.
43.
54.
40.
117
0.09
44.
12.
91.
618
.714
.523
.8
D
esce
nt4.
43.
32.
43.
43.
33.
20.
079
0.06
21.
43.
51.
48.
819
.415
.8
D
esce
nt+
CO
5.3
2.8
2.7
2.5
3.1
3.1
0.09
60.
083
1.4
6.2
1.7
10.4
12.4
19.5
D
esce
nt+
SS3.
82.
93.
02.
12.
93.
10.
069
0.05
71.
13.
21.
89.
021
.97.
4
(con
tinu
ed)

218
Coe
ffici
ent
of v
aria
tion
(C
V%
)
W
alk
20.3
65.9
4.0
23.5
31.7
423.
13.
34.
012
.65.
11.
56.
960
.121
.9
W
alk+
CO
26.2
*33
.75.
343
.921
.7–5
7.8
5.8
7.2
19.9
*22
.11.
839
.625
.574
.6
W
alk+
SS22
.966
.55.
229
.325
.2–4
9.5
5.7
7.5
15.8
12.1
2.0
15.6
74.8
13.1
A
scen
t9.
522
.43.
332
.319
.8–3
17.3
7.7
8.8
103.
86.
72.
163
.029
.944
.5
D
esce
nt14
.711
1.3
3.7
40.8
25.7
22.4
7.0
9.0
11.0
8.5
1.9
12.8
61.1
41.1
D
esce
nt+
CO
18.1
32.7
4.2
44.1
18.1
–33.
47.
09.
311
.014
.72.
122
.126
.093
.4
D
esce
nt+
SS11
.562
.75.
231
.222
.6–2
8.6
5.1
6.8
9.0
7.3
2.4
13.9
83.0
12.3
Intr
acla
ss c
orre
lati
on c
oeffi
cien
t (I
CC
)
W
alk
0.93
0.98
0.97
0.93
0.88
0.84
0.97
0.97
0.93
0.93
0.92
0.91
0.46
0.80
W
alk+
CO
0.92
*0.
940.
870.
910.
730.
760.
970.
960.
85*
0.64
0.92
0.74
0.84
0.88
W
alk+
SS0.
940.
970.
960.
910.
930.
860.
970.
970.
620.
750.
960.
630.
770.
90
A
scen
t0.
840.
970.
970.
860.
920.
740.
760.
820.
330.
950.
890.
950.
900.
81
D
esce
nt0.
960.
940.
770.
640.
910.
870.
760.
700.
950.
860.
860.
810.
880.
91
D
esce
nt+
CO
0.94
0.96
0.91
0.84
0.87
0.85
0.93
0.92
0.96
0.82
0.88
0.95
0.86
0.95
D
esce
nt+
SS0.
970.
940.
980.
940.
890.
890.
980.
980.
930.
900.
940.
720.
610.
86
Not
e. C
O =
cro
ssov
er tu
rn. S
S =
sid
este
p tu
rn. *
Out
lier
rem
oved
for
one
tria
l of
one
subj
ect’s
tim
ing
of th
e m
axim
al fl
exio
n du
ring
sta
nce
and
repl
aced
by
the
mea
n of
the
corr
espo
ndin
g va
lues
in a
ll 8
othe
r tr
ials
. Pea
k kn
ee fl
exio
n va
lue
was
cha
nged
to th
e co
rres
pond
ing
knee
flex
ion
valu
e at
that
spe
cific
pos
ition
.
Tab
le 1
(co
ntinued
)
Kin
emat
ics
Para
met
ers
Tem
pora
l Par
amet
ers
12
34
56
78
910
1112
1314
Task
Mid
stan
ce
max
. fle
xion
(°
)
Term
inal
st
ance
min
. fle
x-ex
t. (°
)
Mid
swin
g m
ax.
flexi
on (°
)
Max
. ad
-duc
tion
(°)
Max
. in
tern
al
rota
tion
(°)
Max
. ex
tern
al
rota
tion
(°)
Str
ide
time
(s)
Sta
nce
time
(s)
%C
yc
at (1
)%
Cyc
at
(2)
%C
yc
at (3
)%
Cyc
at
(4)
%C
yc
at (5
)%
Cyc
at
(6)

3-D Knee Kinematics for Motor Tasks of Daily Living 219
Table 2 Mean within-subject SD, mean within-subject CV and ICC values for seven selected parameters extracted from the knee kinematics curves of four nongait motor tasks
Parameter
1 2 3 4 5 6 7
TaskMax. flexion
(°)
Flexion at foot strike
(°)
Flexion excursion
(°)
Ab-/ adduction excursion
(°)
Max. internal
rotation (°)
In-/external rotation
excursion (°)
Cycle time (s)
Mean
Chair Rise 86.4 N/A 80.9 8.2 18.5 18.3 1.510
Squat, Mild 80.1 N/A 73.0 6.5 18.7 17.7 1.889
Squat, Deep 111.0 N/A 102.2 7.6 24.3 23.1 3.039
Lunge 101.7 28.1 80.2 8.4 16.3 15.5 1.457
Standard deviation (SD)
Chair Rise 3.5 N/A 4.9 2.2 3.2 4.1 0.256
Squat, Mild 6.6 N/A 7.7 2.0 3.4 3.7 0.298
Squat, Deep 5.9 N/A 7.6 1.7 4.7 5.8 0.489
Lunge 5.5 3.3 6.4 2.3 3.2 4.2 0.164
Coefficient of variation (CV%)
Chair Rise 4.1 N/A 6.2 29.8 18.4 21.9 16.6
Squat, Mild 8.3 N/A 10.6 31.9 19.8 21.2 15.8
Squat, Deep 5.4 N/A 7.7 22.7 21.0 25.7 15.6
Lunge 5.6 12.0 8.3 28.5 22.8 27.3 11.2
Intraclass correlation coefficient (ICC)
Chair Rise 0.95 N/A 0.94 0.83 0.96 0.89 0.82
Squat, Mild 0.98 N/A 0.98 0.93 0.93 0.90 0.91
Squat, Deep 0.99 N/A 0.98 0.94 0.92 0.90 0.96
Lunge 0.92 0.96 0.91 0.84 0.95 0.86 0.96
values for knee flexion-extension, abduction-adduction, and rotation curves had respective ranges of 2.8 to 10.7°, 1.4 to 3.7°, and 2.9 to 4.9°. MAV values had larger mag-nitudes than the RMS values but showed similar trends. Among the gait tasks, the increased ranges of axial rotation resulted in turning tasks having higher relative repeatability than straight walking for axial rotation. Sidestep turns in particular showed uniquely good CMC values for axial rotation of 0.90 and 0.91, whereas the corresponding values for straight movements were 0.79 and 0.63. The nongait tasks (Figure 4) showed worse repeatability compared with the gait tasks, particularly in abduction-adduction, as demonstrated by CMC, RMS, and MAV values. For completeness the knee kinematic patterns for the subgroup during all motor tasks are shown in Appendix Figures 1, 2, and 3. Furthermore, the close resemblance of these patterns with those of the full group of N = 25 subjects (Figures 2–4) indicates that the smaller
subject group for repeatability analysis is representative for the larger population in terms of knee joint kinematics.
The study also revealed that a large number of kinematic and temporal parameters have a good within-subject repeatability. These are reported in Tables 1 and 2, respectively for the gait and nongait motor tasks. Regard-ing relative repeatability, the most repeatable among the gait tasks were midswing maximum flexion and its corresponding %cycle, and stride and stance time (Table 1, parameters 3, 11, 7, 8). For each of these parameters, the CV was under 10%, with most tasks showing ICCs above 0.90. Regarding absolute repeatability, all gait tasks’ kinematic parameters (parameters 1–6) showed averaged within-subject SD values smaller than 5°, which was recommended as the highest threshold for the SD of clinical joint kinematics measurements,2 except for midstance maximum flexion during ascent and descent followed by crossover turn.

220 Scheys et al.
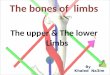
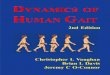
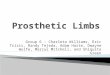
Figure 2 — Knee rotations for walking, walking with a crossover turn (CO), and walking with a sidestep turn (SS), averaged over all 25 healthy subjects. The mean curve (solid line) and single standard deviation band (shaded region) are depicted. Within-subject CMC, RMS, and MAV values based on data from the repeatability analysis subgroup of 10 subjects are also given for each curve. MAV values are based on 3 sessions per subject, and 3 trials per session. All measurements are in degrees.
DiscussionThis study investigated knee joint motion in the three anatomical planes during eleven motor tasks in healthy subjects. The goal of the current study was to describe typical kinematics and repeatability of normal knee joint rotations for eleven motor tasks. This information is crucial to identify the most reliable motor tasks and measurements that can potentially reveal patient-specific patterns during clinical motion analysis.
The presented knee rotation curves for straight walking resembled the curves found in other studies also reporting internal rotation coupled with flexion during stance phase.7–12 Additional studies confirmed specific measurements in the present data, except where experi-mental protocols differed (Table 3).2,13,16–19 For example, MAV values reported here are larger than those published previously,13 likely because of the analysis of a larger number of trials, sessions, and subjects in this study. This can probably also be attributed to differences in motion

221
Figure 3 — As in Figure 2, but for ascent, descent, descent with a crossover turn (CO), and descent with a sidestep turn (SS).

222
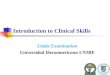
Figure 4 — As in Figure 2, but for chair rise, mild squat, deep squat, and forward lunge. Deep squat data are for 23 (8 for within-subject repeatability analysis) subjects only, whereas those of other tasks are for all 25 (10 for within-subject repeatability analysis) subjects. “Not applicable” (N/A) indicates undefined CMC values, due to variability across trials exceeding the variability of the mean trial across the cycle.

3-D Knee Kinematics for Motor Tasks of Daily Living 223
analysis protocols, as has been previously shown in a pop-ulation of normal children.20 Previously, standardized and constrained squats or lunges respectively showed higher absolute within-subject repeatability17 and ICCs,16 than in this study where squats and lunges were not constrained by any apparatus. It is also expected that skin motion artifacts4 affected the present measurements in addition to other artifacts such as marker placement, and kinematic cross-talk.9 Consequentially, these artifacts might have introduced small differences in shape with previously reported kinematics curves for abduction-adduction and axial rotation during walking.21 It has been shown22 that, in walking, a relevant 1 to 7 degree erroneous rotation at the single bone can occur in any of the three anatomical planes. This can result, with respect to the corresponding physiological skeletal motion, in 10, 50 and 100% error respectively in flexion-extension, abduction-adduction and axial rotation. These figures overcome within-subject
variability, but must be taken in careful consideration for any pathological-to-normal comparison in clinical stud-ies. This source of error is inevitable in any gait analysis system, and little has been reported to limit or to com-pensate for this.4 However, the large physiological axial rotation which occurs at the knee joint during turning tasks may increase the measurement-to-error ratio11 and consequentially limit this percentage error.
As in Zürcher et al,19 the current study demon-strated increased rotations of turning during walking and descent from a step, while additionally showing the good intrasubject repeatability of the turning measurements. Furthermore, turning steps have been proven to be very relevant during activities of daily living.23 These findings suggest the investigation of turning in future studies of knee axial rotation.
Results for the nongait motor tasks (chair rise, squat, and lunge) show consistent coupling between
Table 3 Comparison of results with previous studies on healthy adults
Study Motor Task Rotation Measurement Previous ResultsCurrent Results (Scheys et al)
McGinley et al, 20092 Walking Flexion/Extension CMC 0.96 to 0.99 a 0.99
Ab-/Adduction CMC 0.61 to 0.82 a 0.81
Int.-/External rotation CMC 0.49 to 0.87 a 0.79
Flexion/Extension RMS (or SD) 2 to 5° b 2.8°
Ab-/Adduction RMS (or SD) 1 to 4° b 1.4°
Int.-/External rotation RMS (or SD) 2 to 7° b 2.9°
Ferrari et al, 200813 Walking Flexion/Extension MAV 2.0 to 3.5° c 7.9°
Ab-/Adduction MAV 0.8 to 1.8° c 3.7°
Int.-/External rotation MAV 1.9 to 4.0° c 8.1°
Zurcher et al, 200819 Crossovers Int.-/External rotation Peak internal tibial rotation
14.2° d 17.1 to 18.6°
Sidesteps Int.-/External rotation Peak external tibial rotation
6.7° d 10.3 to 12.0°
Protopapadaki et al, 200718
Ascent Int.-/External rotation Peak flexion (SD) 93.9° (7.4°) e 95.5° (7.1°)
Lavoie et al, 200617 Squat Ab-/Adduction CMC, intra-subject 0.94 to 0.98 f 0.35 to 0.43
Int.-/External rotation CMC, intra-subject 0.82 to 0.94 f 0.65 to 0.77
Alkjaer et al, 200916 Lunge Flexion/Extension Peak flexion 91 to 93° g 101.7°
Flexion/Extension Peak flexion ICC 0.53 to 0.69 g 0.92
a Review, data from 4 studies on healthy adults, various protocols.b Review, data from 12 studies, including interassessor repeatability, various protocols.c Data from 3 subjects, 1 session/subject, 3 trials/session, 2 legs, 5 protocols.d 45° turn from chair rise, instead of 90°.e Ascent on stairs instead of on a step, overall between-subject standard deviation (SD).f Standardized squats, flexion range 0–60°, separate ascent/descent measurements.g Standardized lunge to 90° flexion.

224 Scheys et al.
flexion-extension and axial rotation curves, confirming previous studies.6,7,24,25
Notably, the average knee abduction-adduction curves for chair rise, squat, and lunge were relatively smooth and of small magnitude compared with the gait tasks. This was believed to be indicative of small cross-talk errors and caused by the higher knee loads stabilizing the knee during the entire cycle.
The many different motor tasks analyzed here revealed a large spectrum of repeatability and variability, and also very different patterns and ranges of knee joint motion, in flexion-extension but also in out-of-sagittal plane rotations. The least constrained motor tasks, such as lunge and squat, were also the least repeatable. Finally, larger joint rotations were more repeatable. All this knowledge is a good reference for e designing gait analysis studies in pathological conditions, in particular for selecting the most suitable tasks when validating, for example, the claims of prosthesis designers or surgical and clinical hypotheses.
Acknowledgments
This study was sponsored by and conducted at the European Centre for Knee Research, a part of Smith & Nephew, Inc, which employed the first and third author. The authors thank Liesbeth Swings for her help with data processing, Ellen Jaspers for providing consultation about repeatability indices, and staff and resources at Smith & Nephew.
References
1. McClelland JA, Webster KE, Feller JA. Gait analysis of patients following total knee replacement: A systematic review. Knee. 2007;14(4):253–263. PubMed doi:10.1016/j.knee.2007.04.003
2. McGinley JL, Baker R, Wolfe R, Morris ME. The reli-ability of three-dimensional kinematic gait measurements: a systematic review. Gait Posture. 2009;29(3):360–369. PubMed doi:10.1016/j.gaitpost.2008.09.003
3. Minns RJ. The role of gait analysis in the manage-ment of the knee. Knee. 2005;12(3):157–162. PubMed doi:10.1016/j.knee.2004.12.009
4. Leardini A, Chiari L, Della Croce U, Cappozzo A. Human movement analysis using stereophotogrammetry Part 3. Soft tissue artifact assessment and compensation. Gait Posture. 2005;21(2):212–225. PubMed doi:10.1016/j.gaitpost.2004.05.002
5. Houck J, Yack HJ. Associations of knee angles, moments and function among subjects that are healthy and ante-rior cruciate ligament deficient (ACLD) during straight ahead and crossover cutting activities. Gait Posture. 2003;18(1):126–138. PubMed doi:10.1016/S0966-6362(02)00188-1
6. Moro-oka TA, Hamai S, Miura H, et al. Dynamic activity dependence of in vivo normal knee kinematics. J Orthop Res. 2008;26(4):428–434. PubMed doi:10.1002/jor.20488
7. Komistek RD, Dennis DA, Mahfouz M. In vivo fluoro-scopic analysis of the normal human knee. Clin Orthop Relat Res. 2003;410:69–81. PubMed doi:10.1097/01.blo.0000062384.79828.3b
8. Van Sint Jan S. Color atlas of skeletal landmark definitions. Guidelines for reproducible manual and virtual palpations. 1st ed. London, England: Churchill- Livingston Elsevier; 2007.
9. Kadaba MP, Ramakrishnan HK, Wootten ME. Measure-ment of lower extremity kinematics during level walking. J Orthop Res. 1990;8(3):383–392. PubMed doi:10.1002/jor.1100080310
10. Schache AG, Baker R, Lamoreux LW. Defining the knee joint flexion-extension axis for purposes of quan-titative gait analysis: an evaluation of methods. Gait Posture. 2006;24(1):100–109. PubMed doi:10.1016/j.gaitpost.2005.08.002
11. Desloovere K, Wong P, Swings L, Callewaert B, Vanden-neucker H, Leardini A. Range of motion and repeatability of knee kinematics for 11 clinically relevant motor tasks. Gait Posture. 2010;32(4):597–602. PubMed doi:10.1016/j.gaitpost.2010.08.010
12. Kadaba MP, Ramakrishnan HK, Wootten ME, Gainey J, Gorton G, Cochran GV. Repeatability of kinematic, kinetic, and electromyographic data in normal adult gait. J Orthop Res. 1989;7(6):849–860. PubMed doi:10.1002/jor.1100070611
13. Ferrari A, Benedetti MG, Pavan E, et al. Quantitative comparison of five current protocols in gait analysis. Gait Posture. 2008;28(2):207–216. PubMed doi:10.1016/j.gaitpost.2007.11.009
14. Benedetti MG, Catani F, Leardini A, Pignotti E, Giannini S. Data Management in gait analysis for clinical applica-tions. Clin Biomech (Bristol, Avon). 1998;13(3):204–215. PubMed doi:10.1016/S0268-0033(97)00041-7
15. McGraw KO, Wong SP. Forming inferences about some intraclass correlation coefficients. Psychol Methods. 1996;1(1):30–46. doi:10.1037/1082-989X.1.1.30
16. Alkjaer T, Henriksen M, Dyhre-Poulsen P, Simon-sen EB. Forward lunge as a functional performance test in ACL deficient subjects: test-retest reliability. Knee. 2009;16(3):176–182. PubMed doi:10.1016/j.knee.2008.11.011
17. Lavoie F, Laplante M, Parent G, Duval N, Dore S, De Guise JA. Gesture standardization increases the reproducibility of 3D kinematic measurements of the knee joint. Clin Biomech (Bristol, Avon). 2006;21(5):502–507. PubMed doi:10.1016/j.clinbiomech.2005.12.007
18. Protopapadaki A, Drechsler WI, Cramp MC, Coutts FJ, Scott OM. Hip, knee, ankle kinematics and kinetics during stair ascent and descent in healthy young individuals. Clin Biomech (Bristol, Avon). 2007;22(2):203–210. PubMed doi:10.1016/j.clinbiomech.2006.09.010
19. Zurcher AW, Wolterbeek N, Harlaar J, Poll RG. Knee rota-tion during a weightbearing activity: Influence of turning. Gait Posture. 2008;28(3):472–477. PubMed doi:10.1016/j.gaitpost.2008.03.008
20. Leardini A, Sawacha Z, Paolini G, Ingrosso S, Nativo R, Benedetti MG. A new anatomically based protocol for gait analysis in children. Gait Posture. 2007;26(4):560–571. PubMed doi:10.1016/j.gaitpost.2006.12.018
21. Georgoulis AD, Papadonikolakis A, Papageorgiou CD, Mitsou A, Stergiou N. Three-dimensional tibiofemoral kinematics of the anterior cruciate ligament-deficient and reconstructed knee during walking. Am J Sports Med. 2003;31(1):75–79. PubMed
22. Cappozzo A, Catani F, Leardini A, Benedetti MG, Della Croce U. Position and orientation in space of bones during movement: experimental artefacts. Clin Biomech (Bristol,

3-D Knee Kinematics for Motor Tasks of Daily Living 225
Avon). 1996;11(2):90–100. PubMed doi:10.1016/0268-0033(95)00046-1
23. Glaister BC, Bernatz GC, Klute GK, Orendurff MS. Video task analysis of turning during activities of daily living. Gait Posture. 2007;25(2):289–294. PubMed doi:10.1016/j.gaitpost.2006.04.003
24. Dennis DA, Komistek RD, Mahfouz MR, Walker SA, Tucker A. A multicenter analysis of axial femorotibial
rotation after total knee arthroplasty. Clin Orthop Relat Res. 2004; (428):180–189. PubMed doi:10.1097/01.blo.0000148777.98244.84
25. Dennis DA, Mahfouz MR, Komistek RD, Hoff W. In vivo determination of normal and anterior cru-ciate ligament-deficient knee kinematics. J Bio-mech. 2005;38(2):241–253. PubMed doi:10.1016/j. jbiomech.2004.02.042

226
Appendix Table 1: Average stride time for gait-related motor tasks in 25 healthy subjects
Task Stride Time (s)
Mean
Walk 1.049 Walk+SS 1.294 Ascent 1.458 Descent 1.121 Descent+CO 1.434 Descent+SS 1.373
Appendix Figure 1 — Knee rotations for walking, walking with a crossover turn (CO), and walking with a sidestep turn (SS), averaged over the repeatability analysis subgroup of 10 subjects. The mean curve (solid line) and single standard deviation band (shaded region) are depicted.

227
Appendix Figure 2 — Knee rotations for ascent, descent, descent with a crossover turn (CO), and descent with a sidestep turn (SS), averaged over the repeatability analysis subgroup of 10 subjects. The mean curve (solid line) and single standard deviation band (shaded region) are depicted.

228
Appendix Figure 3 — Knee rotations for chair rise, mild squat, deep squat, and forward lunge. Deep squat data are averaged over 8 subjects only, whereas those of other tasks are averaged over the full repeatability analysis subgroup of 10 subjects. The mean curve (solid line) and single standard deviation band (shaded region) are depicted.