Embed Size (px)
DESCRIPTION
KEDOKTERAN
Citation preview

ORIGINAL ARTICLE
Downregulation of the serum response factor/miR-1axis in the quadriceps of patients with COPD
Amy Lewis,1 Joanna Riddoch-Contreras,1 Samantha A Natanek,2 Anna Donaldson,1,2
William D-C Man,2 John Moxham,3 Nicholas S Hopkinson,2
Michael I Polkey,2 Paul R Kemp1
ABSTRACTRationale Muscle atrophy confers a poor prognosis inpatients with chronic obstructive pulmonary disease(COPD), yet the molecular pathways responsible arepoorly characterised. Muscle-specific microRNAs andserum response factor (SRF) are important regulators ofmuscle phenotype that contribute to a feedback systemto regulate muscle gene expression. The role of thesefactors in the skeletal muscle dysfunction thataccompanies COPD is unknown.Methods 31 patients with COPD and 14 healthyage-matched controls underwent lung and quadricepsfunction assessments, measurement of daily activity anda percutaneous quadriceps muscle biopsy. Theexpression of muscle-specific microRNAs, myosin heavychains and components of the serum response factorsignalling pathway were determined by qPCR.Results A reduction in expression of miR-1 (2.5-fold,p¼0.01) and the myocardin-related transcription factors(MRTFs) A and B was observed in patients comparedwith controls (MRTF-A mRNA: twofold, p¼0.028;MRTF-B mRNA: fourfold, p¼0.011). miR-1 expressionwas associated with smoking history, lung function,fat-free mass index, 6 min walk distance and percentageof type 1 fibres. miR-133 and miR-206 were negativelycorrelated with daily physical activity. Insulin-like growthfactor 1 mRNA was increased in the patients and miR-1was negatively correlated with phosphorylation of thekinase Akt. Furthermore, the protein levels of histonedeacetylase 4, another miR-1 target, were increased inthe patients.Conclusions Downregulation of the activity of theMRTF-SRF axis and the expression of muscle-specificmicroRNAs, particularly miR-1, may contribute toCOPD-associated skeletal muscle dysfunction.
INTRODUCTIONSkeletal muscle dysfunction in the locomotormuscles is an important systemic complication ofchronic obstructive pulmonary disease (COPD).Quadriceps weakness and wasting predict mortalityamong patients with moderate to severe COPDindependently of lung function1 2 and are commoncomplications.3 Characteristically, the vastus later-alis of patients with COPD exhibits a shift towardsa predominance of type IIA fibres and an increase inthe proportion of type IIX fibres associated witha marked reduction in exercise capacity.4 5 In addi-tion to these changes, fibre atrophy occurs and isparticularly marked in type IIX fibres. However, the
mechanisms that control these phenotypic changeshave not been fully defined.Recent data have implicated microRNAs
(miRNAs, small non-coding RNAs that reducemRNA half-life and translation) in the regulation ofthe skeletal muscle phenotype.6 Several miRNAsare highly expressed in skeletal muscle and regulatemuscle phenotype. miR-1 and miR-206 promotemyotube formation7 and miR-206 is associatedwith regeneration after nerve injury.8 Geneticknockout of miR-499 or miR208-b reduces theproportion of type I fibres whereas overexpressionof miR-499 increases type I fibres and endurance inmice.9 10 Conversely, miR-133 expression inhibitsmyotube formation and promotes proliferation.11
Analysis of miRNA expression in primary skel-etal myopathies identified changes in miRNAs thattarget conserved pathways, but the expression ofindividual miRNAs varied.12 Similarly, the profile ofmiRNAs is altered in the skeletal muscle of patientswith insulin resistance.13 miRNA profiles are alsomarkedly affected by activity, and studies inhumans have shown altered miRNA profiles asso-ciated with endurance exercise training.14 As inac-tivity may be a major contributor to skeletalmuscle dysfunction in COPD, changes in miRNAexpression associated with inactivity maycontribute to the phenotype. Studies of inactivityresulting from denervation,15 nerve entrapment16
or space flight17 all show initial reductions in
Key messages
What is the question?< How are changes in microRNA expression and
serum response factor (SRF) activity associatedwith changes in skeletal muscle phenotype inpatients with chronic obstructive pulmonarydisease (COPD)?
What is the key point?< The expression of the myocardin-related tran-
scription factors (activators of SRF) and of miR-1 (an SRF target) is reduced in the quadriceps ofpatients with COPD.
Why read on?< The study identifies the SRF/miR-1 axis as an
important contributor to muscle phenotype inpatients with COPD.
< Additional materials arepublished online only. To viewthese files please visit thejournal online (http://thorax.bmj.com/content/67/1.toc).1Section of Molecular Medicine,National Heart and LungInstitute, Imperial CollegeLondon, London, UK2NIHR Respiratory BiomedicalResearch Unit at the RoyalBrompton, Harefield FoundationNHS Trust, Imperial College,London, UK3Department of Asthma, Allergyand Lung Biology, King’s CollegeLondon School of Medicine,Kings Health Partners, London,UK
Correspondence toDr Paul R Kemp, Section ofMolecular Medicine, NationalHeart and Lung Institute,Imperial College London, SAFBuilding South KensingtonCampus, London SW7 2AZ, UK;[email protected]
MIP and PRK contributedequally to the study.
Received 6 April 2011Accepted 15 September 2011Published Online First13 October 2011
This paper is freely availableonline under the BMJ Journalsunlocked scheme, see http://thorax.bmj.com/site/about/unlocked.xhtml
26 Thorax 2012;67:26e34. doi:10.1136/thoraxjnl-2011-200309
Chronic obstructive pulmonary disease
group.bmj.com on January 29, 2014 - Published by thorax.bmj.comDownloaded from

miR-1, but whether miR-1 levels remain suppressed varies.Interestingly, miR-1 did not change in response to resistancetraining in humans but there was altered expression of miRsassociated with the mTOR pathway.18
The myocardin-related transcription factor (MRTF)-serumresponse factor (SRF) axis regulates the expression of miR-119
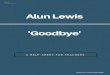
and other muscle-specific miRNAs.20 Changes in the expressionand localisation of SRF and the SRF co-activators, MRTF-A andMRTF-B, in response to physical activity and ageing have allbeen reported.21e23 In addition to miRNA expression, MRTF/SRF activity is important in regulating MHC expression. SRFactivity is more important in activating expression of MHCIthan MHCIIa and MHCIIx, implying a role for SRF in fibre-typecontrol.24 The miRNAs feed back to regulate MRTF/SRF andother factors that control muscle cell phenotype such asmyocyte enhancer factor-2 (MEF-2), and proliferation includinginsulin-like growth factor 1 (IGF-1)25 and the myostatinsignalling pathway.26 27 Together these MRTF/SRF-miRNAinteractions provide the system shown in figure 1.
We hypothesised that reduced physical activity commonlyobserved in patients with COPD would suppress SRF activityand reduce expression of miR-1 and other SRF-dependentmiRNAs along with altered expression of miRNA targets incomparison with healthy controls. We therefore analysedmuscle-specific miRNA expression, the expression of miR-145(an miRNA associated with SRF activity in smooth muscle) andmiR-181 (an miRNA altered by activity but not known to beSRF-dependent28) along with the expression of components ofthe SRF pathway in quadriceps biopsies from patients withCOPD and age-matched controls. Some of the results presentedhere have been reported in abstract form.29
METHODSSubjectsThirty-one patients with COPD according to the GlobalInitiative in Obstructive Lung Disease guidelines 200430 wereenrolled from clinics at the Royal Brompton Hospital. Fourteenhealthy age-matched controls were recruited by advertisement.
Patient exclusion criteria and ethical approval are detailed in theonline supplement.
Physiological measurementsGeneral assessmentLung volume, carbon monoxide transfer, blood gas tension andfat-free mass index (FFMI) were measured as described in theonline supplement.
Muscle assessmentsQuadriceps strength was determined by measuring maximalvoluntary contraction (MVC) and unpotentiated twitchquadriceps force (TwQ). Exercise performance was measuredusing a 6 min walk (6MW) test and daily physical activitywas measured using a tri-axial accelerometer. Detaileddescriptions of the physiological methods are given in theonline supplement.
Assessment of mRNA, miRNA and protein levelsMessenger RNA was extracted and quantified as describedpreviously31 and detailed in the online supplement. MicroRNAexpression was analysed in trizol extracted RNA using theNcode SYBR green miRNA-qRT-PCR kit (Invitrogen, Paisley,UK) as detailed in the online supplement. Protein was analysedby luminex or western blotting as described in the onlinesupplement. The amount of material available did not allow usto measure all values in all subjects.
Assessment of MRTF activityThe activity of MRTFs on the miR-1 promoters was determinedas described in the online supplement.
Immunofluorescence analysisFibre size, fibre proportion and SRF localisation were determinedby immunofluorescence as described in the online supplement.
Statistical analysisUnsupervised principal components analysis (PCA) and unsu-pervised hierarchical clustering were performed in Aabel(Gigawiz). The variables for hierarchical clustering were scaledto unit variance and distances calculated based on correlationcoefficient similarity. Groups were defined based on centroidlinkage. Log transformation of the miRNA data produceda normal distribution for all the miRNAs. Correlation analysiswas performed using the Pearson correlation coefficient. Tointerpret the correlation data, p<0.05 was taken as an indicatorof association to allow us to investigate likely relationshipswithin the data, but none of the relationships were significant ifapplying a Bonferroni correction.Differences between patients and controls were calculated by
the Student t test for normally distributed data and by theManneWhitney U test for data that did not fit a normaldistribution. The test used for each analysis is denoted by T(t-test) and MW (ManneWhitney U) in parentheses. Thestatistical significance of differences was taken at p<0.05.
RESULTSPatient characteristics and muscle phenotypeAs expected, the patients had significant lung function impair-ment and reduced arterial blood oxygen tensions, consistentwith a diagnosis of COPD. However, there was no significantdifference in age, weight, body mass index (BMI) or arterialblood carbon dioxide tensions between groups and the groups
Hypertrophy signalling
miR-499/208 miR-133/145miR-1/ 206
HDAC4 IGF-1
Myostatin
Atrophy signalling
SRF
MRTF-A MRTF-B
Follistatin
Act IIB
receptor
Akt/PI3K
Figure 1 Relationships between miRNAs and selected target genes inmuscle. The relationship between miRNAs and the RNAs that encodeproteins is shown. miRNA targets are either predicted using targetscan(http://www.targetscan.org/) or verified by experiment. HDAC4, histonedeacetylase 4; IGF-1, insulin-like growth factor 1; MRTF, myocardin-related transcription factor; SRF, serum response factor; Act IIBreceptor, activin type IIB receptor.
Thorax 2012;67:26e34. doi:10.1136/thoraxjnl-2011-200309 27
Chronic obstructive pulmonary disease
group.bmj.com on January 29, 2014 - Published by thorax.bmj.comDownloaded from

were matched for gender (p¼0.74, Fisher exact test). Patientshad a significantly reduced FFMI, quadriceps force and loco-motion time compared with controls (table 1).
The patients had a marked difference in the size and propor-tion of muscle fibres compared with the controls (see figure S1 inonline supplement). The proportion of type I fibres in thepatients was reduced (from a median of 52 (IQR 39e62) to 25(IQR 17e30)) and the proportion of type II fibres was increased(from mean6SD 47614 to 69615, table 1). The proportion ofhybrid type I/type II fibres was also increased in patients (froma median of 1.5 (IQR 0e3) to 3 (IQR 0e11), table 1). The fibresof the patients were smaller than those of the controls witha significant reduction in the size of the type I and type IIXfibres (table 1).
Patients had reduced MHCI mRNA compared with controls(table 1 and figure S2 in online supplement). MHCI mRNA wasdirectly correlated with forced expiratory volume in 1 s (FEV1)
percentage predicted and inversely correlated with smokinghistory across both patients and controls (see figure S2 in onlinesupplement). MHCIIa expression was not correlated withsmoking history or FEV1 (not shown). MHCI mRNA waspositively correlated with exercise performance (6MW, figure S3in online supplement) but was not associated with strength.MHCIIa was inversely correlated with 6MW (figure S3 in onlinesupplement) across all data as well as within the patient groupalone, but also showed no association with strength. There wasno significant difference in a-actin expression between thegroups (data not shown).
miRNA expression in quadriceps of patients with COPDMultivariate statistical analyses (eg, hierarchical clustering andPCA) offer a powerful unsupervised approach for the identifi-cation of structure and relationships between samples, allowingfor the visualisation of natural groupings in data. Hierarchical
Table 1 Clinical characteristics of study subjects
Controls (n[14) COPD (n[31)Significance(p value)
Sex (F:M) 6:8 11:21
Age 6868 6567 0.192 (T)
Height (cm) 17168 16969 >0.5 (T)
Weight (kg) 79.8618.4 70.9616.5 0.114 (T)
BMI (kg/m2) 26.964.5 24.564.7 0.109 (T)
FFMI (kg/m2) 17.862.3 15.762.2 0.006 (T)
Pack-years* 4.1 (0e10) 45 (34e69) <0.001 (MW)
FEV1 (% pred)* 110 (103.6e112.6) 32 (25.1e47.1) <0.001 (MW)
RV/TLC (%) 37.164.7 58.669.9 <0.001 (T)
TLCO (% pred)* 86 (82.5e91.8) 33 (26.2e52.2) <0.001 (MW)
PaCO2 (kPa)* 5.33 (4.80e5.42) 5.18 (4.96e5.74) >0.5 (MW)
PaO2 (kPa) 10.3761.55 9.2561.34 0.017 (T)
6MW (m) 623689 3786134 <0.001 (T)
6MW (% pred) 125615 72624 <0.001 (T)
Locomotiontime (min/12 h)*
86 (61e122) 45.5 (23e81) 0.006 (MW)
Mt (%)* 20.667.2 15.766.2 0.03 (T)
MI (m/s2)* 2.1 (1.7e2.4) 1.6 (1.4e2.0) 0.017 (MW)
SGRQ* 5 (1e8) 52 (41e61) <0.001 (MW)
Best MVC 36.8467.78 29.2169.11 0.009 (T)
Best TwQ 9.5863.04 7.8962.41 0.077 (T)
MVC/BMI 1.460.3 1.260.3 0.075 (T)
Quadricepsendurance T80(s)*
110 (70e160) 80 (60e105) 0.121 (MW)
MHCI mRNA (AU)* 28.0 (19.2e39.9) 7.0 (4.8e14.0) <0.001 (MW)
MHCIIA mRNA (AU)* 1.5 (0.8e2.2) 2.6 (1.3e3.6) 0.105 (MW
Type I CSA (mm2) 578661371 490961327 0.048 (T)
Type IIA CSA (mm2)* 4593.5 (2946�6105) 3784 (2964�4615) 0.141 (MW)
Type IIX CSA (mm2) 618761868 323161403 <0.001 (T)
% Type I fibres* 52 (39e62) 25 (17e30) <0.001 (MW)
% Type I/II fibres* 1.5 (0e3) 3 (0e11) 0.088 (MW)
% Type II fibres 47614 69615 <0.001 (T)
% Type IIA fibres 44613 60615 0.002 (T)
% Type IIX fibres* 2.6 (0e4.0) 8.9 (3.0e13.0) 0.006 (MW)
Values are mean6SEM for normally distributed data or median (IQR) for non-normallydistributed data.p values were calculated by t test (normally distributed data), indicated by (T), or theManneWhitney test (non-normally distributed data), indicated by (MW), and are shown inbold when p<0.05.MHC RNAs were determined by qPCR and normalised to the expression of RPLPO in thesame samples as described in the online supplement.*Not normally distributed.BMI, body mass index; CSA, cross-sectional area; FFMI, fat-free mass index; FEV1, forcedexpiratory volume in 1 s; MVC, maximal voluntary contraction; MI, movement intensity; Mt,movement time; PaO2, arterial oxygen tension; PaCO2, arterial carbon dioxide tension; pred,predicted; RV, residual volume; TLC, total lung capacity; TLCO, transfer factor of the lung forcarbon monoxide; TwQ, twitch force in the quadriceps.
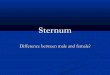
Figure 2 miRNA expression is markedly different in patients withchronic obstructive pulmonary disease (COPD) compared with matchedcontrols. The expression of miRNAs was determined by qPCR andnormalised to the expression of 5S RNA in the same sample, asdescribed in the Methods section. The heat map shows the expressionof miRNAs in each sample organised by hierarchical clustering in whichthe expression of each miRNA was given equal weighting. This analysisshows clear separation of the majority of patients (closed circles) fromthe control group (open circles).
28 Thorax 2012;67:26e34. doi:10.1136/thoraxjnl-2011-200309
Chronic obstructive pulmonary disease
group.bmj.com on January 29, 2014 - Published by thorax.bmj.comDownloaded from

clustering (figure 2) and PCA of miRNA expression identifieda distinct profile for the patients compared with the controls(PCA, p<0.0001, figure 3B), primarily associated with anapproximate 2.5-fold reduction in the expression of miR-1(p¼0.01(T), figure 3D and figure 4) in patients compared withcontrols, but there was no change in the expression of miR-133(figure 4). Differences in the expression of miR-208 and miR-499contributed to the observed difference in the miRNA expressionpattern (figure 3D), although taken alone these did not reachstatistical significance (miR-208, p¼0.099, miR-499, p¼0.142(T),figure 4). Hierarchical clustering of the expression patterns ofindividual miRNAs within the samples showed that miR-1,miR-133 and miR-206 formed a cluster consistent with theirexpression as bicistronic RNAs from the miR-1/miR-133and miR-206/miR-133 genes, providing validation of ourmethodology.
Comparison of the expression of the miRNAs with thephysiological data showed that miR-1 was negatively correlatedwith smoking history (r¼�0.39, p¼0.007) but positively asso-ciated with FEV1 (r¼0.34, p¼0.022), FFMI (r¼0.33, p¼0.025),6MW (r¼0.33, p¼0.026) and MVC/BMI (r¼0.29, p¼0.049). LikemiR-1, miR-499 was positively associated with FFMI (r¼0.37,p¼0.012) and negatively with smoking history (r¼�0.33,p¼0.027). miR-133 and miR-206 were negatively associatedwith physical activity (movement intensity; miR-133: r¼�0.30,p¼0.057; miR-206: r¼�0.35, p¼0.023 and locomotion time;miR-133: r¼�0.35, p¼0.027; miR-206: r¼�0.34, p¼0.029).The association of the miRNAs with different physiologicalcharacteristics is shown in figure 5A. Associations with p<0.05
were only present if both the control and patient groups werecombined; this feature may result from a lack of power but alsoraises the possibility that disease is an important component ofthe difference.Comparison of miRNA expression with the muscle charac-
teristics showed that miR-1 was positively correlated with thepercentage of type I fibres (r¼0.33, p¼0.029) and miR-499showed a trend towards association with percentage of type Ifibres (r¼0.28, p¼0.063). None of the other miRNAs wasassociated with muscle fibre characteristics (figure 5B).
Expression of SRF, MRTF-A, MRTF-BTo investigate the SRF system we analysed the expression ofSRF and two SRF co-activators (MRTF-A and MRTF-B) byqPCR. Mean SRF mRNAwas not significantly different betweenthe groups (COPD 3.42 (IQR 2.49e3.63) AU, n¼19; controls3.31 (IQR 3.22e3.89) AU, n¼16, p¼0.185 (MW), figure 6A).MRTF-A and MRTF-B mRNA levels were significantly lower inpatients (3.73 (IQR 3.48e3.87) AU and 3.9460.394 AU respec-tively, n¼25) than in controls (3.85 (IQR 372e4.22) AU,p¼0.028 (MW), figure 6B and 4.4260.634 AU, p¼0.011 (T)respectively, n¼15, figure 6C). MRTF-A expression was corre-lated with FEV1 (% predicted, r¼ 0.46, p¼0.027) and MRTF-Bwas correlated with smoking history (r¼�0.576, p¼0.006, notshown). Again these associations were not present in individualgroups. To tie this reduction in MRTF expression to miR-1, weshowed that MRTFs could activate the miR-1 promoters(figure 6D and supplementary results).
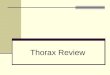
Figure 3 Principal componentanalysis of the miRNA expressionpattern in patients with chronicobstructive disease (COPD) andcontrols. (A) Scatter plot comparingPC1 and PC2 for each sample. (B)Principal component analysis of miRNAexpression in patients and controlsshows a significant difference in thepattern of miRNA expression betweenthe two groups as a difference in PC2(p<0.0001). (C) Loading plots for PC1showing equal contribution of themiRNAs to this component. (D) Loadingplots for principal component analysisidentifies miR-1, miR-208 and miR-499as the major contributors to theseparation of the two groups. Patientsare shown as closed circles andcontrols are shown as open circles.
Thorax 2012;67:26e34. doi:10.1136/thoraxjnl-2011-200309 29
Chronic obstructive pulmonary disease
group.bmj.com on January 29, 2014 - Published by thorax.bmj.comDownloaded from

SRF activity is also regulated by the localisation of the protein.We therefore determined the localisation of SRF in musclesections from a subset of patients with COPD and controls. Inthe controls, SRF was readily detectable in the nuclei of all of thesamples analysed. However, in the patients there was a reduc-tion in nuclear staining and the appearance of nuclei withperinuclear SRF staining (figure 7).
Reduced expression of targets of miR-1 in patients with COPDmiR-1 targets include IGF-1 and the IGF-1 receptor,25 indicatingthat it should modify the activity of the IGF-1 pathway, and wehave found that phosphorylation of the kinase Akt (also knownas protein kinase B) is inversely proportional to activity in ourpatient group.32 We therefore analysed the expression of IGF-1and the activity of the IGF-1 pathway by examining the phos-phorylation of Akt in patients and controls. IGF-1 mRNA wasincreased in patients (figure 8A) and miR-1 expressionwas inversely proportional to the phospho-Akt/total Akt ratio(figure 8B, r¼�0.43, p¼0.022). A trend towards this associationwas present in the patients alone (r¼�0.46, p¼0.053). Therewere no other associations of the phospho-Akt/total Akt ratiowith any of the other miRNAs.
We also determined the expression of histone deacetylase 4(HDAC4) mRNA and protein in an additional set of patientswith COPD and controls. This analysis showed that, whilethere was no difference in the expression of HDAC4 mRNAbetween patients and controls (figure 8C), HDAC4 protein washigher in patients with COPD than in controls (figure 8D).
DISCUSSIONThis study shows that the profile of miRNAs in the quadricepsof patients with COPD differs from that in controls. The dataalso suggest that MRTF/SRF activity is downregulated in
patients. Together with previous animal data showing a role forSRF and the miRNAs in the control of muscle phenotype, thesedata support the hypothesis that altered miRNA expression andreduced SRF activity contribute to COPD-associated muscledysfunction.
Significance of the findingsThe most striking finding is the reduction in the expression ofmiR-1 in patients compared with controls. miR-1 expression isincreased by SRF,19 and we show that it is increased in an SRF-dependent manner by the MRTFs. The reduced expression ofMRTFs, as well as altered SRF localization, suggest that reducedactivity of the MRTF/SRF axis contributes to the reduction inMHCI and miR-1 expression. Our data also indicate functionalconsequences of reduced miR-1 with increased expression ofIGF-1, an inverse correlation of miR-1 with Akt phosphorylationand increased HDAC4 protein in the patients. Whether theobserved increase in IGF-1 mRNA is a direct response to reducedmiR-1 is not clear, as miRNAs are suggested to inhibit trans-lation in muscle rather than increase RNA degradation.13
Consistent with this suggestion, we found that patients hadnormal HDAC4 mRNA levels but increased HDAC4 protein.The interaction of miR-1 with IGF-1 signalling and HDAC4have been documented previously.25 33e35 These observationsraise two points regarding the role of the SRF/miR-1 axis inmuscle, which are discussed separately.
miR-1 in muscle biologymiR-1 has an accepted role in skeletal muscle differentiation.One likely effect of the reduced miR-1 observed is the increase inHDAC4 protein. HDAC4 inhibits the activity of MEF-2 and SRF,both of which are important regulators of MHCI expression,providing a mechanism by which the reduction in miR-1 may
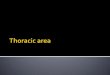
Figure 4 Expression of microRNAs inpatients with chronic obstructivepulmonary disease (COPD) andcontrols. Expression of miRNAs wasdetermined by qPCR and normalised tothe expression of the 5S RNA in thesame sample as described in theMethods section. The expression ofmiR-1 (A) was lower in patients thancontrols but there was no significantdifference in the expression of miR-499(B) or the other miRNAs (C) analysed.Data are presented as log normalisedexpression with the box showingmedian and IQR, error bars to maximumand minimum points. Patients areshown as closed circles and controlsare shown as open circles. Statisticalsignificance was calculated by t test.
30 Thorax 2012;67:26e34. doi:10.1136/thoraxjnl-2011-200309
Chronic obstructive pulmonary disease
group.bmj.com on January 29, 2014 - Published by thorax.bmj.comDownloaded from

Figure 5 Pearson correlation matricesfor miRNAs with physiologicalcharacteristics and muscle fibreparameters in the cohort. MicroRNAexpression was correlated with non-muscle physiological characteristics forall the samples (A) or with the muscle-specific physiological and histochemicalparameters (B). The direction andintensity of the correlation is colour-coded according to the bar. ThemiRNAs are organised in the order oftheir contribution to PC2 as determinedby principal components analysis.Correlations reaching a statisticalsignificance where p<0.05 areindicated by * and the p values aregiven in table S1 in the onlinesupplement. Characteristics wereordered by hierarchical clustering(figure S4 in online supplement). BMI,body mass index; CSA, cross-sectionalarea; FFMI, fat-free mass index; FEV1,forced expiratory volume in 1 s; Lo,locomotion; MVC, maximal voluntarycontraction; MI, movement intensity;Mt, movement time; 6MW, 6 min walktest; SGRQ, St George RespiratoryQuestionnaire; TwQ, twitch force in thequadriceps; Ty, type.
Figure 6 Effect of myocardin-relatedtranscription factors (MRTFs) on miR-1promoter activity and the expression ofMRTF and serum response factor (SRF) inthe quadriceps muscle of patients withchronic obstructive pulmonary disease(COPD). Expression of MRTF-A (A),MRTF-B (B) and SRF (C) mRNA in thequadriceps of patients and healthy age-matched controls was quantified by real-time PCR and normalised to theexpression of RPLPO. Data are presentedas log normalised expressionwith the boxshowing median and IQR, error bars tomaximum and minimum points. Theexpression of MRTF-A and MRTF-B wassuppressed in the patients comparedwithcontrols but SRF expression did not differsignificantly between groups (AU,arbitrary units). (D) C2C12 cells weretransfected with miR-1-1, miR-1-2promoter reporter vectors as described inthe online supplement in the presence orabsence of expression vectors for MRTF-A and MRTF-B. Luciferase activity wasdetermined 24 h later. MRTF-A andMRTF-B increased the activity of the miR-1-1 andmiR-1-2 promoters (p<0.001) butdid not increase the activity of the deltaenhancer promoter. Data are presented asmean6SEM. Patients are shown asclosed circles and controls are shown asopen circles. Statistical significance forthe mRNA expression was calculated by theManneWhitney U test.
Thorax 2012;67:26e34. doi:10.1136/thoraxjnl-2011-200309 31
Chronic obstructive pulmonary disease
group.bmj.com on January 29, 2014 - Published by thorax.bmj.comDownloaded from

contribute to reduced MHCI and fibre shift. The fact that miR-1is an SRF target provides a positive feedback loop that maycontribute to the downward spiral in muscle phenotype.HDAC4 also suppresses the expression of follistatin: reducedmiR-1 would therefore increase the activity of the myostatinpathway and promote muscle wasting.36 These effects of miR-1suggest a role in the maintenance of muscle phenotype and,consistent with these suggestions, miR-1 expression wasinversely proportional to the percentage of type I muscle fibres.The reduction in miR-1 in patients, who have a lower level ofactivity than controls, is different from the response to endur-ance training in young adults.18 miR-1 has also been suggestedto inhibit the calcineurin pathway, thereby suppressing activity-dependent MEF-2 activation.37 The activity of miRNAs istherefore likely to be cell and context dependent.
miR-1 also inhibits the expression of IGF-1 and, consistentwith previous reports,25 we found an inverse correlationbetween miR-1 and IGF-1 signalling. A similar increase in IGF-1mRNA has previously been observed by mRNA profiling inCOPD.38 The increase in IGF-1 mRNA in patients likely to showmuscle wasting seems paradoxical. However, other studies havealso shown increased activity of the hypertrophy signallingpathway in patients with COPD, which they hypothesised to bepart of a compensation pathway39 but could also result fromsynthetic resistance.
MRTF/SRF and muscle gene expressionMRTF/SRF activity is widely recognised as important in thecontrol of muscle-specific gene expression. However, there islimited information on changes in the MRTFs in response to
changing activity or disease. Human studies have found thatMRTF expression increases in response to physical training anddeclines following a period of detraining.21 22 Previous in vitroand animal studies are consistent with a role for these proteinsin the regulation of MHCI expression. For example, expressionof a dominant negative MRTF-B in differentiating C2C12 cells40
reduces SRF activity and MHCI expression. Similarly,reduced SRF activity is associated with the reduction in MHCIand increased MHCIIa and MHCIIx following hind limbsuspension in rats.41
miRNA in muscle diseaseIn addition to the reduction in miR-1 expression, the pattern ofmiRNA expression was also different between patients andcontrols, suggesting a more general change in miRNA expres-sion. The expression of miR-133 and miR-206 were inverselyassociated with daily physical activity. This change is consistentwith the observations of Nielsen et al42 and Keller et al14 whoshowed that endurance training suppresses the expression ofthese and other myo-miRs. The fact that we observed noassociation of miR-1 and miR-499 with physical activitysuggests that factors other than daily physical activity are moreimportant in determining their levels in patients with COPD.Similarly, there was a trend towards reduced miR-499 and miR-208, miRNAs that target myostatin, expression of which isincreased in weak COPD patients.43
Limitations of the studyThe conclusions drawn from this study are limited by the cross-sectional design that only enables us to detect associations
Figure 7 Serum response factor (SRF)localisation is altered in patients withchronic obstructive pulmonary disease(COPD). The localisation of SRF wasdetermined in sections of quadricepsmuscle from patients with COPD andcontrols by immunofluorescence asdescribed in the online supplement.Arrowheads show the localisation ofnuclei and the inset shows perinuclearstaining for SRF.
32 Thorax 2012;67:26e34. doi:10.1136/thoraxjnl-2011-200309
Chronic obstructive pulmonary disease
group.bmj.com on January 29, 2014 - Published by thorax.bmj.comDownloaded from

between the gene expression and physiological characteristics.Furthermore, the data are correlative and, although they high-light potential mechanisms, they do not prove causality. Itshould be noted, however, that the highlighted associations havebeen demonstrated mechanistically through in vitro and in vivostudies.
We have also proposed that patients have reduced SRF activitybut could not make direct measurements of SRF activity in ourmuscle samples. However, from the reduced MRTF andincreased MHCI and miR-1 expression, together with alteredSRF localization, it seems reasonable to conclude that SRFactivity is reduced.
CONCLUSIONSIn this study we show that the expression of miRNAs isdifferent in the quadriceps of patients with COPD than incontrol subjects. In particular, the expression of miR-1 is reducedand is associated with changes in fibre proportion, probablyleading to the observed association with muscle mass andexercise performance. Furthermore, the expression of the MRTFsis also suppressed in the patients and again the expression of oneof these genes is associated with disease severity. Together withdata from studies identifying the MRTFs and SRF as criticalregulators of skeletal muscle phenotype, these findings suggestthat reduced activity of the SRF pathway contributes to COPDskeletal muscle dysfunction, in part by downregulating miR-1expression.
Acknowledgements We are grateful to Dr Jake Bundy for help with the principalcomponents analysis and statistical analysis.
Funding This work was funded by the BBSRC, Wellcome Trust and the NationalInstitute for Health Research (NIHR) Respiratory Biomedical Unit at the RoyalBrompton Hospital and Imperial College. AL is a BBSRC PhD student, SAN receiveda Wellcome Trust Fellowship, AD received a NIHR Respiratory Biomedical Unitfellowship and WM is a NIHR Clinician Scientist. NSH is a HEFCE Clinical SeniorLecturer. MIP’s salary is part funded by the NIHR Respiratory Biomedical Unit at theRoyal Brompton Hospital and National Heart & Lung Institute.
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by Royal Brompton and Harefield NHSTrust research ethics committee.
Contributors AL, JR-C, SAN, PRK, AD, MIP: experimental design, data collection andanalysis. AL, SAN, PRK, MIP: analysis and interpretation of data. All authors made animportant intellectual contribution to the manuscript drafting and editing.
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES1. Swallow EB, Reyes D, Hopkinson NS, et al. Quadriceps strength predicts mortality
in patients with moderate to severe chronic obstructive pulmonary disease. Thorax2007;62:115e20.
2. Marquis K, Debigare R, Lacasse Y, et al. Midthigh muscle cross-sectional area isa better predictor of mortality than body mass index in patients with chronicobstructive pulmonary disease. Am J Respir Crit Care Med 2002;166:809e13.
3. Seymour JM, Spruit MA, Hopkinson NS, et al. The prevalence of quadricepsweakness in COPD and the relationship with disease severity. Eur Respir J2010;36:81e8.
4. Allaire J, Maltais F, Doyon JF, et al. Peripheral muscle endurance and theoxidative profile of the quadriceps in patients with COPD. Thorax2004;59:673e8.
5. Gosker HR, Zeegers MP, Wouters EF, et al. Muscle fibre type shifting in the vastuslateralis of patients with COPD is associated with disease severity: a systematicreview and meta-analysis. Thorax 2007;62:944e9.
6. Williams AH, Liu N, van Rooij E, et al. MicroRNA control of muscle developmentand disease. Curr Opin Cell Biol 2009;21:461e9.
Figure 8 Altered insulin-like growthfactor 1 (IGF-1) and histone deacetylase4 (HDAC4) in patients with chronicobstructive pulmonary disease (COPD).IGF-1 (A) and HDAC4 (C) mRNA werequantified by real-time PCR asdescribed in the online supplement. IGF-1 mRNA was increased whereasHDAC4 mRNA was unchanged inpatients relative to controls. Data arepresented as log normalised expressionwith the box showing median and IQR,error bars to maximum and minimumpoints. Akt levels and phospho-Aktlevels were determined by lunminexassay in muscle homogenates preparedas described in the online supplement.miRNA expression was quantified byqPCR and normalised to the expressionof 5S RNA. Pearson correlationcoefficients showed that miR-1 (B) wascorrelated with the ratio of phospho-Aktto total Akt. Patients are shown as opencircles and controls are shown asclosed circles. (D) HDAC4 protein levelswere detected by western blotting(inset) quantified by densitometry andnormalised to total protein loaded ontothe blot determined by Ponceau Redstaining. HDAC4 protein levels wereincreased in patients compared withcontrols. Data are presented asnormalised protein levels with the boxshowing median and IQR, error bars to maximum and minimum points. Statistical significance for mRNA and protein levels was determined by theManneWhitney U test. Due to limitations on specimen size, we were unable to measure HDAC4 protein and miRNA in the same sample set.
Thorax 2012;67:26e34. doi:10.1136/thoraxjnl-2011-200309 33
Chronic obstructive pulmonary disease
group.bmj.com on January 29, 2014 - Published by thorax.bmj.comDownloaded from

7. Nakajima N, Takahashi T, Kitamura R, et al. MicroRNA-1 facilitates skeletalmyogenic differentiation without affecting osteoblastic and adipogenic differentiation.Biochem Biophys Res Commun 2006;350:1006e12.
8. Williams AH, Valdez G, Moresi V, et al. MicroRNA-206 delays ALS progression andpromotes regeneration of neuromuscular synapses in mice. Science2009;326:1549e54.
9. van Rooij E, Quiat D, Johnson BA, et al. A family of microRNAs encoded by myosingenes governs myosin expression and muscle performance. Dev Cell2009;17:662e73.
10. McCarthy JJ, Esser KA, Peterson CA, et al. Evidence of MyomiR network regulationof beta-myosin heavy chain gene expression during skeletal muscle atrophy. PhysiolGenomics 2009;39:219e26.
11. Chen JF, Mandel EM, Thomson JM, et al. The role of microRNA-1 and microRNA-133 in skeletal muscle proliferation and differentiation. Nat Genet 2006;38:228e33.
12. Eisenberg I, Eran A, Nishino I, et al. Distinctive patterns of microRNA expression inprimary muscular disorders. Proc Natl Acad Sci U S A 2007;104:17016e21.
13. Gallagher IJ, Scheele C, Keller P, et al. Integration of microRNA changes in vivoidentifies novel molecular features of muscle insulin resistance in type 2 diabetes.Genome Med 2010;2:9.
14. Keller P, Vollaard NB, Gustafsson T, et al. A transcriptional map of the impact ofendurance exercise training on skeletal muscle phenotype. J Appl Physiol2011;110:46e59.
15. Jeng SF, Rau CS, Liliang PC, et al. Profiling muscle-specific microRNA expressionafter peripheral denervation and reinnervation in a rat model. J Neurotrauma2009;26:2345e53.
16. Rau CS, Jeng JC, Jeng SF, et al. Entrapment neuropathy results in differentmicroRNA expression patterns from denervation injury in rats. BMC MusculoskeletDisord 2010;11:181.
17. Allen DL, Bandstra ER, Harrison BC, et al. Effects of spaceflight on murine skeletalmuscle gene expression. J Appl Physiol 2009;106:582e95.
18. Davidsen PK, Gallagher IJ, Hartman JW, et al. High responders to resistanceexercise training demonstrate differential regulation of skeletal muscle microRNAexpression. J Appl Physiol 2011;110:309e17.
19. Zhao Y, Samal E, Srivastava D. Serum response factor regulates a muscle-specificmicroRNA that targets Hand2 during cardiogenesis. Nature 2005;436:214e20.
20. Niu Z, Iyer D, Conway SJ, et al. Serum response factor orchestrates nascentsarcomerogenesis and silences the biomineralization gene program in the heart. ProcNatl Acad Sci U S A 2008;105:17824e9.
21. Lamon S, Wallace MA, Leger B, et al. Regulation of STARS and its downstreamtargets suggest a novel pathway involved in human skeletal muscle hypertrophy andatrophy. J Physiol 2009;587:1795e803.
22. Wallace MA, Hock MB, Hazen BC, et al. Striated muscle activator of Rho signalling(STARS) is a PGC-1alpha/oestrogen-related receptor-alpha target gene and isupregulated in human skeletal muscle after endurance exercise. J Physiol2011;589:2027e39.
23. Sakuma K, Akiho M, Nakashima H, et al. Age-related reductions in expression ofserum response factor and myocardin-related transcription factor A in mouse skeletalmuscles. Biochim Biophys Acta 2008;1782:453e61.
24. Allen DL, Weber JN, Sycuro LK, et al. Myocyte enhancer factor-2 and serumresponse factor binding elements regulate fast Myosin heavy chain transcription invivo. J Biol Chem 2005;280:17126e34.
25. Elia L, Contu R, Quintavalle M, et al. Reciprocal regulation of microRNA-1 and insulin-like growth factor-1 signal transduction cascade in cardiac and skeletal muscle inphysiological and pathological conditions. Circulation 2009;120:2377e85.
26. Rosenberg MI, Georges SA, Asawachaicharn A, et al. MyoD inhibits Fstl1 and Utrnexpression by inducing transcription of miR-206. J Cell Biol 2006;175:77e85.
27. Drummond MJ, Glynn EL, Fry CS, et al. Essential amino acids increase microRNA-499, -208b, and -23a and downregulate myostatin and myocyte enhancer factor 2CmRNA expression in human skeletal muscle. J Nutr 2009;139:2279e84.
28. Safdar A, Abadi A, Akhtar M, et al. miRNA in the regulation of skeletal muscleadaptation to acute endurance exercise in C57Bl/6J male mice. PLoS One 2009;4:e5610.
29. Lewis A, Riddoch-Contreras J, Natanek SA, et al. Alterations in MRTF and FHL1activity contribute to fibre type shift in the quadriceps of patients with COPD. Am JRespir Crit Care Med 2010;181:A6611.
30. Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management,and prevention of chronic obstructive pulmonary disease: GOLD executive summary.Am J Respir Crit Care Med 2007;176:532e55.
31. Ellis PD, Smith CW, Kemp P. Regulated tissue-specific alternative splicing ofenhanced green fluorescent protein transgenes conferred by alpha-tropomyosinregulatory elements in transgenic mice. J Biol Chem 2004;279:36660e9.
32. Riddoch Contreras J, Sathyapala SA, Marsh GS, et al. Four and a half LIM protein1 expression and akt phosphorylation in quadriceps muscle in chronic obstructivepulmonary disease patients and its relation to muscle strength and physical activity.Thorax 2008;63:A24.
33. Yu XY, Song YH, Geng YJ, et al. Glucose induces apoptosis of cardiomyocytes viamicroRNA-1 and IGF-1. Biochem Biophys Res Commun 2008;376:548e52.
34. Hua Y, Zhang Y, Ren J. IGF-1 deficiency resists cardiac hypertrophy and myocardialcontractile dysfunction: role of microRNA-1 and microRNA-133a. J Cell Mol Med.Published Online First: 21 March 2011. doi:10.1111/j.1582-4934.2011.01307.x.
35. Shan ZX, Lin QX, Fu YH, et al. Upregulated expression of miR-1/miR-206 in a ratmodel of myocardial infarction. Biochem Biophys Res Commun 2009;381:597e601.
36. Sun Y, Ge Y, Drnevich J, et al. Mammalian target of rapamycin regulates miRNA-1and follistatin in skeletal myogenesis. J Cell Biol 2010;189:1157e69.
37. Ikeda S, He A, Kong SW, et al. MicroRNA-1 negatively regulates expression of thehypertrophy-associated calmodulin and Mef2a genes. Mol Cell Biol2009;29:2193e204.
38. Debigare R, Maltais F, Cote CH, et al. Profiling of mRNA expression in quadriceps ofpatients with COPD and muscle wasting. COPD 2008;5:75e84.
39. Doucet M, Russell AP, Leger B, et al. Muscle atrophy and hypertrophy signaling inpatients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med2007;176:261e9.
40. Selvaraj A, Prywes R. Megakaryoblastic leukemia-1/2, a transcriptional co-activatorof serum response factor, is required for skeletal myogenic differentiation. J BiolChem 2003;278:41977e87.
41. Giger JM, Bodell PW, Zeng M, et al. Rapid muscle atrophy response to unloading:pretranslational processes involving MHC and actin. J Appl Physiol2009;107:1204e12.
42. Nielsen S, Scheele C, Yfanti C, et al. Muscle specific microRNAs are regulated byendurance exercise in human skeletal muscle. J Physiol 2010;588:4029e37.
43. Man WDC, Natanek SA, Riddoch-Contreras J, et al. Quadriceps myostatinexpresssion in COPD. Eur Respir J 2010;36:686e9.
Thorax online
Visit Thorax online and listen to the latest podcast, post comments and download any you mighthave missed. Keep informed and up to date by visiting thorax.bmj.com.
34 Thorax 2012;67:26e34. doi:10.1136/thoraxjnl-2011-200309
Chronic obstructive pulmonary disease
group.bmj.com on January 29, 2014 - Published by thorax.bmj.comDownloaded from

doi: 10.1136/thoraxjnl-2011-200309 2012 67: 26-34 originally published online October 13, 2011Thorax
Amy Lewis, Joanna Riddoch-Contreras, Samantha A Natanek, et al. patients with COPDfactor/miR-1 axis in the quadriceps of Downregulation of the serum response
http://thorax.bmj.com/content/67/1/26.full.htmlUpdated information and services can be found at:
These include:
Data Supplement http://thorax.bmj.com/content/suppl/2011/10/13/thoraxjnl-2011-200309.DC1.html
"Supplementary Data"
References
http://thorax.bmj.com/content/67/1/26.full.html#related-urlsArticle cited in:
http://thorax.bmj.com/content/67/1/26.full.html#ref-list-1This article cites 42 articles, 24 of which can be accessed free at:
Open Access
http://creativecommons.org/licenses/by-nc/2.0/legalcode.http://creativecommons.org/licenses/by-nc/2.0/ and compliance with the license. See:work is properly cited, the use is non commercial and is otherwise in use, distribution, and reproduction in any medium, provided the originalCreative Commons Attribution Non-commercial License, which permits This is an open-access article distributed under the terms of the
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
CollectionsTopic
(835 articles)Tobacco use � (834 articles)Smoking �
(979 articles)Health education � (93 articles)Open access �
Articles on similar topics can be found in the following collections
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on January 29, 2014 - Published by thorax.bmj.comDownloaded from

Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on January 29, 2014 - Published by thorax.bmj.comDownloaded from