Embed Size (px)
Citation preview

AustralAs .I Cardiac Thorac Surg 1993:2(2)
Thoracic Surgeons Are Different
Peter Clarke, FRACS
Thoracic Surgical Unit, Austin Hospital, Victoria, Australia
A lthough George Stirling was a pioneer in open heart surgery in Australia, and made his name in cardiac
surgery, he had the advantage of training in a unit where the cardiothoracic surgeons had considerable thoracic surgical experience. He has always been equally at home with the lungs and oesophagus as with the heart. Unfortunately, this happy state of affairs has not con- tinued. Many modern trainees are graduating with only a superficial knowledge of thoracic surgery, and no real depth of experience in its performance.
Until recently, there has been an exponential growth in coronary artery surgery. This has meant that the trainees are often left opening and closing the chest in cardiac patients, while the thoracic surgery is done by one of the consultants in the next-door theatre. The heavy surgical workload has prevented the trainee from having time to attend hospital meetings where the thoracic patients are discussed with the oncologists and radiother- apists.
There is too little time to learn fibre-optic bron- choscopy and oesophagoscopy with the result that these investigations often fall by default into the hands of the physicians. In some centres practically all oesophageal surgery is done by the general surgeons to the detriment of the training program and the operative results.
This lack of adequate thoracic training becomes a significant problem particularly when the young cardio- thoracic trainee, after training in an overseas cardiac unit, returns to Australia only to find that the demand for coronary artery surgery has plateaued and that although the senior surgeons are overworked, few new patients come in his or her direction. All too often the result is that he or she sets up peripheral rooms and purports to the local practitioners that a fully trained cardiothoracic surgeon has arrived and can deal with all their problems.
Of course many patients have thoracic problems which are then dealt with badly. Our young surgeon may be equally deficient in paediatric cardiac surgical expe- rience, but there is little danger of getting such patients unless the surgeon has an attachment to a major pae- diatric cardiac surgical unit.
In an ideal world a thoracic surgeon would initially obtain a fellowship in general surgery so that he or she is truly competent in upper abdominal problems and also is seen to be properly licensed. The training rotation would then cover the outline shown in Table 1 with a heavy emphasis on attending interdisciplinary meetings with the respiratory physicians, oncologists and radiotherapists.
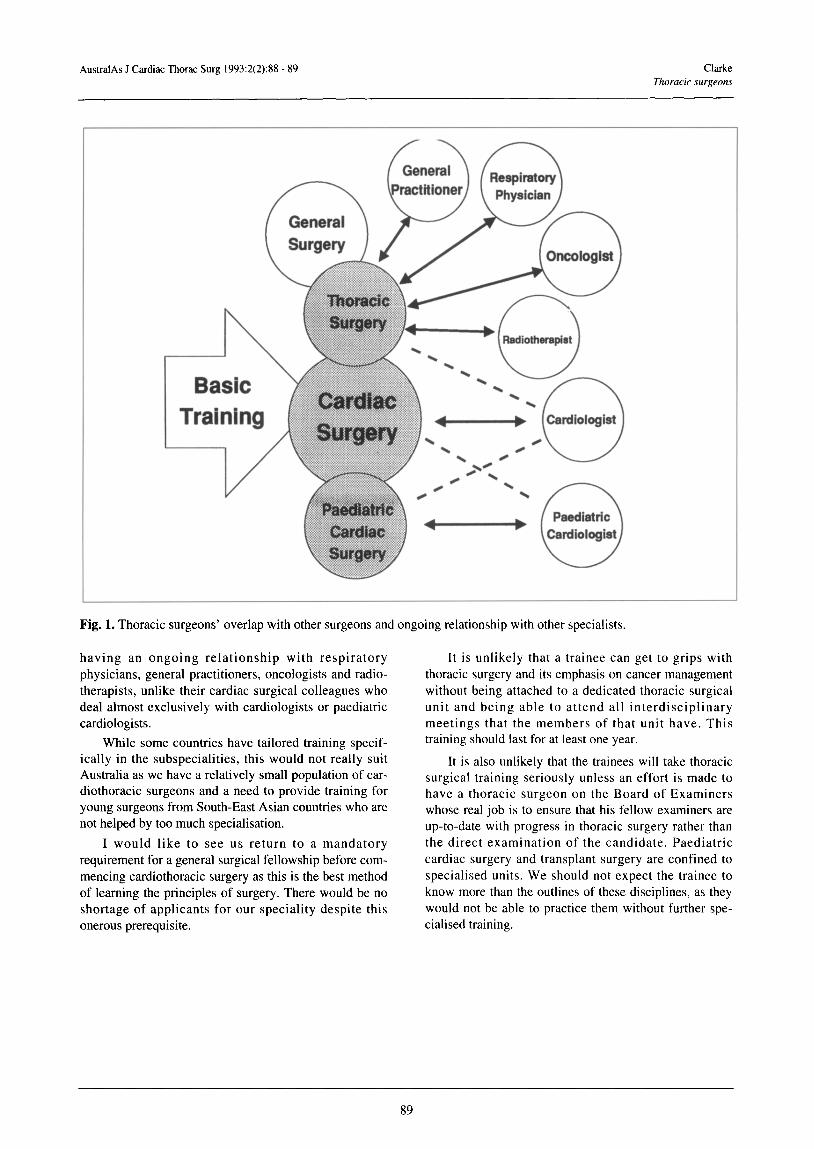
They might then end up as shown in Fig. 1, over- lapping to some extent with the general surgeons and
Table 1: Ideal training for tboracic surgery. A. Full training in general surgery
B. Thoracic training 1. Understanding of:
l respiratory physiology l pulmonary function testing particularly in
relation to operability l oesophageal physiology including pressure
monitoring and pH testing l principles of oncology l principles of radiotherapy including brachytherapy
2. Competence in performance of l flexible bronchoscopy
l rigid bronchoscopy l flexible gastroscopy l rigid oesophagoscopy
3. Exposure to and performance under supervision of full range of:
l oesophageal operations l pulmonary operations l operations on mediastinum l operations for chest wall deformities l operations for tracheal problems
4. Exposure to and performance of video-assisted thoraco- scopic procedures
5. Experience of management of: l pulmonary problems in the intensive care unit l chest trauma l pulmonary complications of AIDS l pulmonary complications of tuberculosis
6. Understanding and exposure to the management of endobronchial and endo-oesophageal lesions with lasers or stents
7. Understanding and exposure to management of lung transplantation
8. Exposure to research program and Journal Club
88
AustralAs J Cardiac Thorac Surg 1993:2(2):88 - 89 Clarke Thoracic .surgeons
r Cardiologist \ /
Fig. 1. Thoracic surgeons’ overlap with other surgeons and ongoing relationship with other specialists.
having an ongoing relationship with respiratory physicians, general practitioners, oncologists and radio- therapists, unlike their cardiac surgical colleagues who deal almost exclusively with cardiologists or paediatric cardiologists.
While some countries have tailored training specif- ically in the subspecialities, this would not really suit Australia as we have a relatively small population of car- diothoracic surgeons and a need to provide training for young surgeons from South-East Asian countries who are not helped by too much specialisation.
I would like to see us return to a mandatory requirement for a general surgical fellowship before com- mencing cardiothoracic surgery as this is the best method of learning the principles of surgery. There would be no shortage of applicants for our speciality despite this onerous prerequisite.
It is unlikely that a trainee can get to grips with thoracic surgery and its emphasis on cancer management without being attached to a dedicated thoracic surgical unit and being able to attend all interdisciplinary meetings that the members of that unit have. This training should last for at least one year.
It is also unlikely that the trainees will take thoracic surgical training seriously unless an effort is made to have a thoracic surgeon on the Board of Examiners whose real job is to ensure that his fellow examiners are up-to-date with progress in thoracic surgery rather than the direct examination of the candidate. Paediatric cardiac surgery and transplant surgery are confined to specialised units. We should not expect the trainee to know rnore than the outlines of these disciplines, as they would not be able to practice them without further spe- cialised training.
89





























