Embed Size (px)
Citation preview
Supplemental Material
This supplement has been provided by the authors to give readers additional
information about their work.
1
Supplemental Methods
Polysomnography and CPAP Therapy
Nocturnal polysomnography was performed using an Embla signal recording
system with Somnologica Window NT Software (Flaga hf. Medical Devices
Broomfield, CO) as previously described.1 Piezoelectric bands and both oronasal
thermistor and nasal pressure were used for apneas/hypopneas detection.2
Continuous positive airway pressure (CPAP) was titrated to a level that
eliminated apneas, hypopneas, oxyhemoglobin desaturation, and sleep
fragmentation.3 The titration protocol was performed by registered
polysomnographic technician and reviewed by a board certified sleep medicine
physician. The titration protocol for split-night titration studies was identical to that
of full-night titration studies. All patients had respiratory disturbance index (RDI) <
5 and a minimum SaO2 above 90% at the prescribed CPAP pressure.3 Sleep
stages were scored in 30-second epochs according to standard criteria.4 An
obstructive apnea was defined as a cessation of upper airway flow in association
with continued respiratory effort of at least 10 seconds. An obstructive hypopnea
was defined as a discrete reduction in airflow for at least 10 seconds associated
with a decrease in oxygen saturation of >3 percent or an arousal in the presence
of thoracoabdominal ventilatory efforts.5 Apnea plus hypopnea index (AHI) was
defined as the number of obstructive apnea plus hypopnea episodes per hour of
sleep. Among study participants recruited from community (n=40), 10 had OSA
and 30 did not. Among study participants recruited from the Sleep Disorders
Center (n=31), 28 had OSA and 3 did not.
2
Study participants recruited form the Sleep Disorders Center had been referred
to the Center. Among subjects recruited from the Sleep Disorders Center, 67%
had BMI≥30 kg/m2, 23% had BMI 25-29.9 kg/m2, and 10% had BMI<25 kg/m2.
Among subjects recruited from community, 42% had BMI≥30 kg/m2, 40% had
BMI 25-29.9 kg/m2, and 18% had BMI<25 kg/m2.
Patients with OSA who had AHI≥20 events/hour (n=19) during at least 2 hours of
baseline sleep recording underwent split-night polysomnography. In OSA
patients who underwent split-night polysomnography, experimental procedures
were performed 48 hours later to avoid any CPAP interference. The duration of
possible CPAP effects on endothelial protein expression in patients is unknown.
We allowed at least 48 hours period after CPAP titration study based on in vitro
studies of the effects of hypoxia on endothelial cells. Expression of eNOS mRNA
and protein in cultured endothelial cells returns to baseline within 24 hours of
cessation of exposure to hypoxia.6,7 Repetitive hypoxia and arousals occur
immediately after discontinuation of CPAP therapy in patients with OSA.8 The
selected interval of 48 hours after a short-term alleviation of obstructive events
(i.e. CPAP titration) is twice as long as that required for alteration in eNOS
expression in vitro.
Patients who underwent split-night study had mostly severe OSA (median
AHI=51, Q1-to-Q3 37 to 87). The duration of the baseline recording was 187±47
min (mean±SD) in the split-night study. The duration of the baseline recording
3
was 388±68 min for the full-night study (n=19, median AHI=10, Q1-to-Q3 8 to
13). CPAP therapy was recommended for all patients with OSA. The adherence
with CPAP therapy did not differ between all patients who underwent split-night
and full-night diagnostic polysomnography (3.6±3.0 vs. 3.0±3.0 hours, p=0.48).
When patients who did not adhere with CPAP were excluded, the adherence with
CPAP therapy remained similar in patients who underwent split-night and full-
night diagnostic polysomnography (4.9±2.4 vs. 5.1±2.0 hours, p=0.86).
Adherence with treatment was assessed by using CPAP device with compliance
software that recorded usage time only when prescribed pressure was received
by the patient. The time when suboptimal pressure was received was not
counted as usage time.
Brachial Artery Flow-Mediated Dilation
Vascular response in the brachial artery was assessed by flow-mediated dilation
(FMD) according to the guidelines of the International Brachial Artery Reactivity
Task Force.9 Brachial artery diameter was measured in the contralateral arm to
the endothelial harvesting site. Subjects were evaluated in a quiet, temperature-
controlled room. After a 30-minute rest in a supine position, the brachial artery
diameter was measured 6 cm proximal to the antecubital fossa using a 7–
15 MHz linear array transducer (Philips 5500, Andover, MA). Occlusion blood
pressure cuff was placed over the proximal forearm just below the antecubital
fossa. FMD was measured as the dilator response to reactive hyperemia induced
by a 5-minute blood pressure cuff occlusion of the upper arm. The cuff was
4
inflated to 50 mmHg above systolic blood pressure if the systolic blood pressure
was greater than 150 mmHg, or to 200 mmHg if the systolic blood pressure was
less than 150 mmHg. Systolic blood pressure was lower than 150 mmHg in all
study participants. Brachial artery diameter (expressed in millimeters up to one
decimal place) was measured at rest and during peak hyperemia for 1 minute
after a 5-minute occlusion of arterial flow. A blinded reader analyzed brachial
artery diameters off-line using analysis software. The percent diameter change
for FMD was calculated as follows:
FMD (%) = [(brachial artery diameter at peak hyperemia − diameter at
rest)/diameter at rest] × 100.
Endothelium-independent smooth muscle dependent brachial vasodilation was
not assessed in our study. Endothelium-independent vasodilation was previously
shown to be unaltered in patients with OSA.10 Endothelial cell harvesting and
FMD were performed the same morning within 2 hours in all participants. We did
not administer nitrates during FMD to avoid possible effects on measured
endothelial protein expression in our study participants.
5
Supplemental References:
1. Jelic S, Bartels MN, Mateika JH, Ngai P, DeMeersman RM, Basner RC.
Arterial stiffness increases during obstructive sleep apneas. Sleep. 2002;
25:850–855.
2. Iber C, Ancoli-Israel S, Chesson A, and Quan SF for the American
Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep
and Associated Events: Rules, Terminology and Technical Specifications,
1st ed.: Westchester, Illinois: American Academy of Sleep Medicine, 2007.
3. Kushida CA, Chediak A, Berry RB, Brown LK, Gozal D, Iber C,
Parthasarathy S, Quan SF, Rowley JA; Positive Airway Pressure Titration
Task Force; American Academy of Sleep Medicine. Clinical guidelines for
the manual titration of positive airway pressure in patients with obstructive
sleep apnea. J Clin Sleep Med. 2008; 4:157-171.
4. Rechtschaffen A, Kales A. A manual of standardized terminology,
techniques and scoring system for sleep stages of human subjects.
Bethesda, MD: National Institutes of Health; 1968:1–12. National Institutes
of Health publication 204.
5. Sleep-related breathing disorders in adults: recommendations for
syndrome definition and measurement techniques in clinical research: the
report of the American Academy of Sleep Medicine Task Force. Sleep.
1999; 22:667–689.
6
6. McQuillan LP, Leung GK, Marsden PA, Kostyk SK, Kourembanas S.
Hypoxia inhibits expression of eNOS via transcriptional and
posttranscriptional mechanisms. Am J Physiol. 1994; 267:H1921-1927.
7. Liao JK, Zulueta JJ, Yu FS, Peng HB, Cote CG, Hassoun PM. Regulation
of bovine endothelial constitutive nitric oxide synthase by oxygen. J Clin
Invest. 1995; 96:2661-2666.
8. Kribbs NB, Pack AI, Kline LR, Getsy JE, Schuett JS, Henry JN, Maislin G,
Dinges DF. Effects of one night without nasal CPAP treatment on sleep
and sleepiness in patients with obstructive sleep apnea. Am Rev Respir
Dis. 1993; 147:1162-1168.
9. Corretti MC, Anderson TJ, Benjamin EJ, Celermajer D, Charbonneau F,
Creager MA, Deanfield J, Drexler H, Gerhard-Herman M, Herrington D,
Vallance P, Vita J, Vogel R, International Brachial Artery Reactivity Task
Force. Guidelines for the ultrasound assessment of endothelial-dependent
flow-mediated vasodilation of the brachial artery: a report of the
International Brachial Artery Reactivity Task Force. J Am Coll Cardiol.
2002; 39:257–265.
10. Kato M, Roberts-Thomson P, Phillips BG, Haynes WG, Winnicki M,
Accurso V, Somers VK. Impairment of endothelium-dependent
vasodilation of resistance vessels in patients with obstructive sleep apnea.
Circulation. 2000; 102:2607-2610.
7
8
Supplemental Figure Legends:
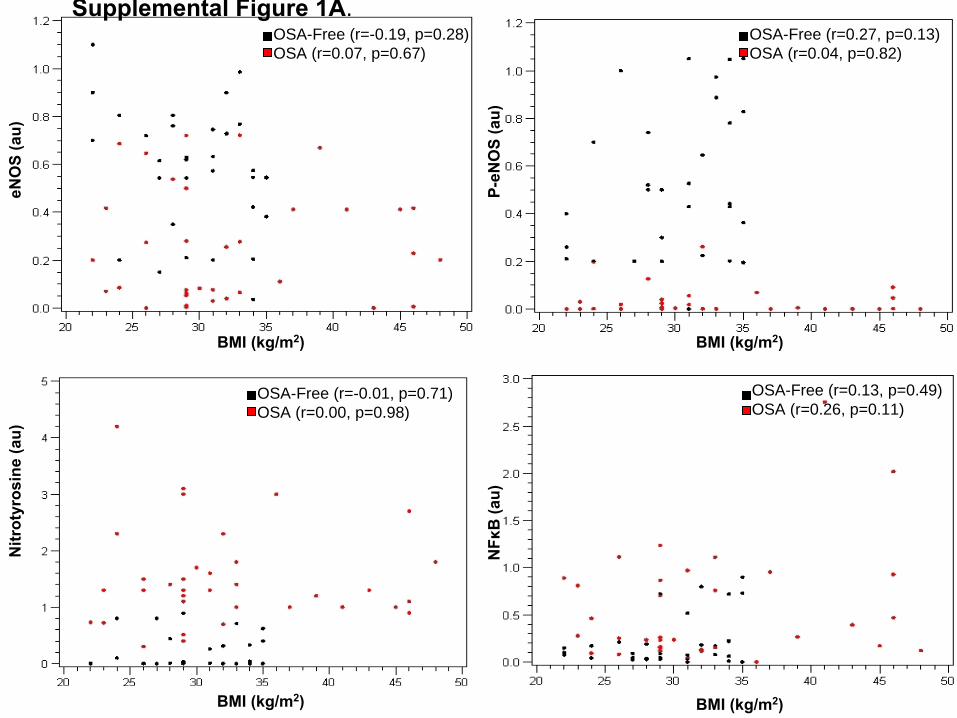
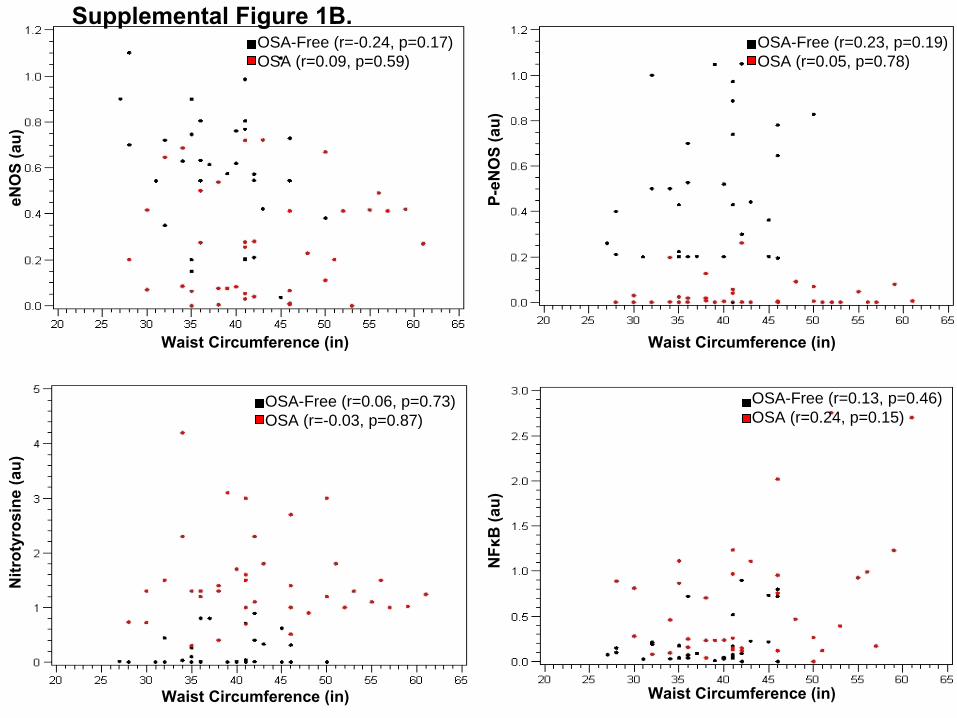
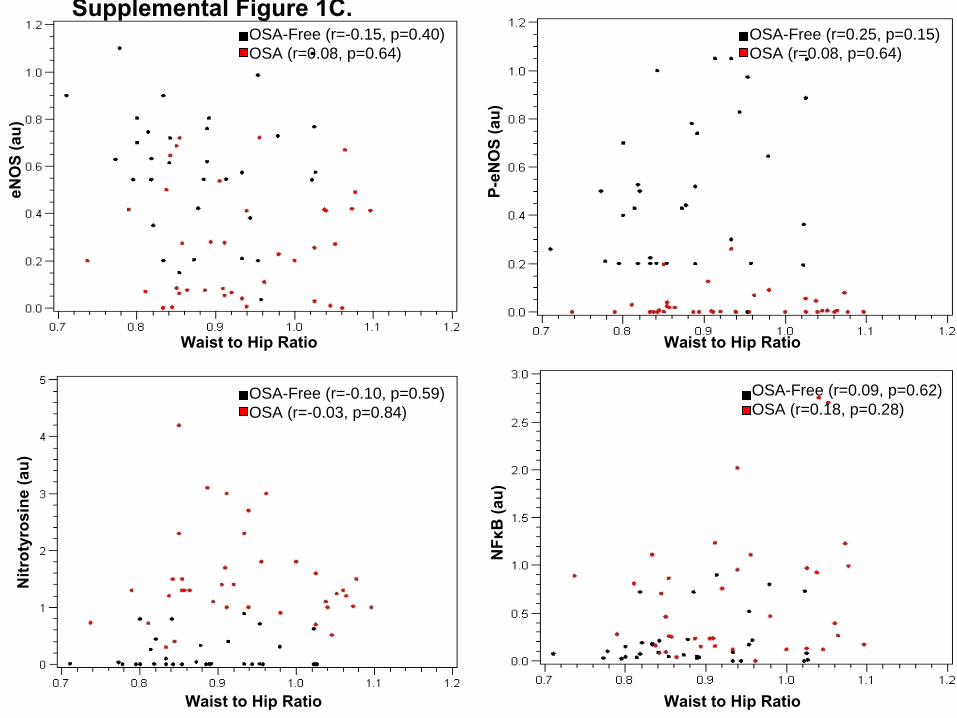
Supplemental Figure 1.
Relationship between expression of endothelial nitric oxide synthase (eNOS),
phosphorylated eNOS (P-eNOS), nitrotyrosine and nuclear factor kappa B
(NFκB) in harvested venous endothelial cells and body mass index (BMI), waist
circumference and waist to hip ratio. Endothelial protein expression did not
significantly correlate with BMI (A), waist circumference (B) or waist to hip ratio
(C) in patients with OSA (red circles) and OSA-free subjects (black circles) (r
values are Spearman correlation coefficients).
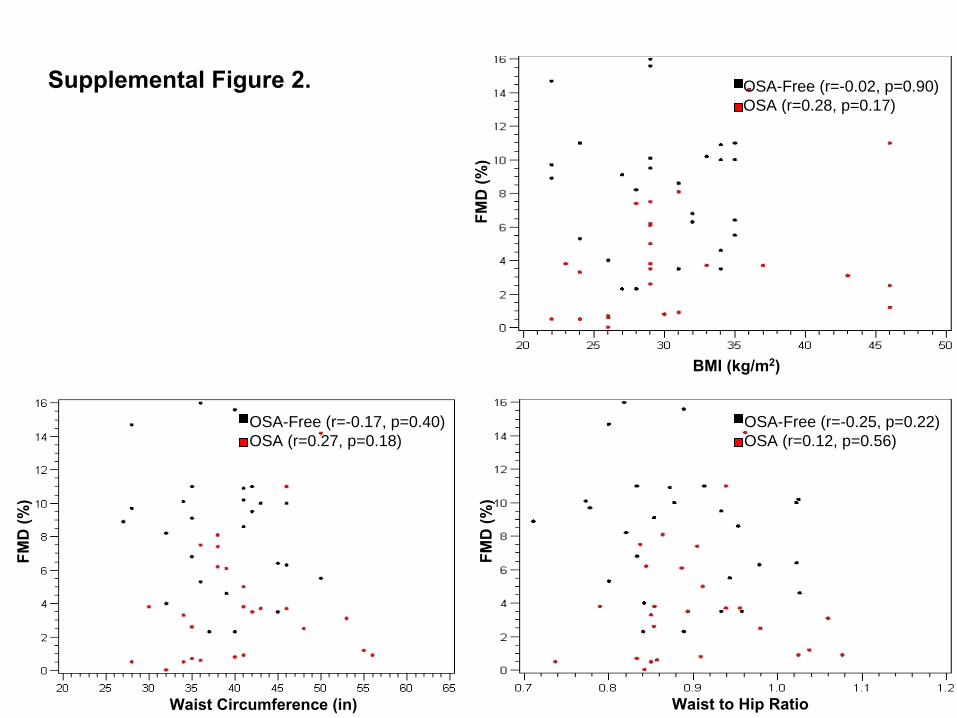
Supplemental Figure 2. Brachial artery flow-mediated dilation (FMD) did not correlate significantly with
body mass index (BMI), waist circumference or waist to hip ratio in patients with
OSA (red circles) and OSA-free subjects (black circles) (r values are Spearman
correlation coefficients).
BMI (kg/m2)
OSA-Free (r=-0.19, p=0.28)OSA (r=0.07, p=0.67)
eNO
S(a
u)
BMI (kg/m2)
OSA-Free (r=-0.01, p=0.71)OSA (r=0.00, p=0.98)
Nitr
otyr
osin
e(a
u)
BMI (kg/m2)
OSA-Free (r=0.27, p=0.13)OSA (r=0.04, p=0.82)
P-eN
OS
(au)
BMI (kg/m2)
NFκ
B(a
u)
OSA-Free (r=0.13, p=0.49)OSA (r=0.26, p=0.11)
Supplemental Figure 1A.
Waist Circumference (in)
OSA-Free (r=-0.24, p=0.17)OSA (r=0.09, p=0.59)
eNO
S(a
u)
Waist Circumference (in)
OSA-Free (r=0.23, p=0.19)OSA (r=0.05, p=0.78)
P-eN
OS
(au)
Waist Circumference (in)
NFκ
B(a
u)
OSA-Free (r=0.13, p=0.46)OSA (r=0.24, p=0.15)
Supplemental Figure 1B.
Waist Circumference (in)
Nitr
otyr
osin
e(a
u)
OSA-Free (r=0.06, p=0.73)OSA (r=-0.03, p=0.87)
Waist to Hip Ratio
OSA-Free (r=-0.15, p=0.40)OSA (r=0.08, p=0.64)
eNO
S(a
u)
Waist to Hip Ratio
OSA-Free (r=-0.10, p=0.59)OSA (r=-0.03, p=0.84)
Nitr
otyr
osin
e(a
u)
Waist to Hip Ratio
OSA-Free (r=0.25, p=0.15)OSA (r=0.08, p=0.64)
P-eN
OS
(au)
Waist to Hip Ratio
NFκ
B(a
u)
OSA-Free (r=0.09, p=0.62)OSA (r=0.18, p=0.28)
Supplemental Figure 1C.
BMI (kg/m2)
FMD
(%)
OSA-Free (r=-0.02, p=0.90)OSA (r=0.28, p=0.17)
Waist Circumference (in)
FMD
(%)
OSA-Free (r=-0.17, p=0.40)OSA (r=0.27, p=0.18)
Waist to Hip Ratio
FMD
(%)
OSA-Free (r=-0.25, p=0.22)OSA (r=0.12, p=0.56)
Supplemental Figure 2.





























