Embed Size (px)
Citation preview

WELCOME
April 14, 2016
OPTIMIZINGCOSTS AND OUTCOMESIN HEALTHCARE
From theory to real life
ROB TEN HOEDT
EXECUTIVE VICE PRESIDENT & PRESIDENT, EMEA
OPTIMIZING COSTS AND OUTCOMES IN HEALTHCARE
AGENDA
TIME TOPIC PRESENTER
11:00 – 11:15 WelcomeThe Role of Medical Technology in Value-Based Healthcare, Medtronic Value Work Underway
ROB TEN HOEDT, Executive Vice President and President,Medtronic EMEA
11:15 – 11:25 HBR ‘s Focus on and Definition of Value-Based Healthcare
JOSH MACHT, Executive Vice President & Group Publisher,Harvard Business Review
11:25 – 11:40 Measuring Outcomes: ICHOM perspective CHRISTINA AKERMAN, MD, PHD, President of International Consortium for Health Outcomes Measurement (ICHOM)
11:40 – 11:55 Measuring Outcomes: ERAS Society perspective PROF. OLLE LJUNGQVIST, Chairman and Founding Member , The Enhanced Recovery After Surgery (ERAS) Society
11:55 – 12:15 Panel DiscussionModerator: JOSH MACHT
12:15 – 12:30 Open Floor Q&A
12:30 Close

CORE SET OF UNIVERSAL HEALTHCARE NEEDSHAS EXPANDED BEYOND CLINICAL OUTCOMES ALONE
Optimize costs and efficiencies
Expand access
Improve clinical outcomes
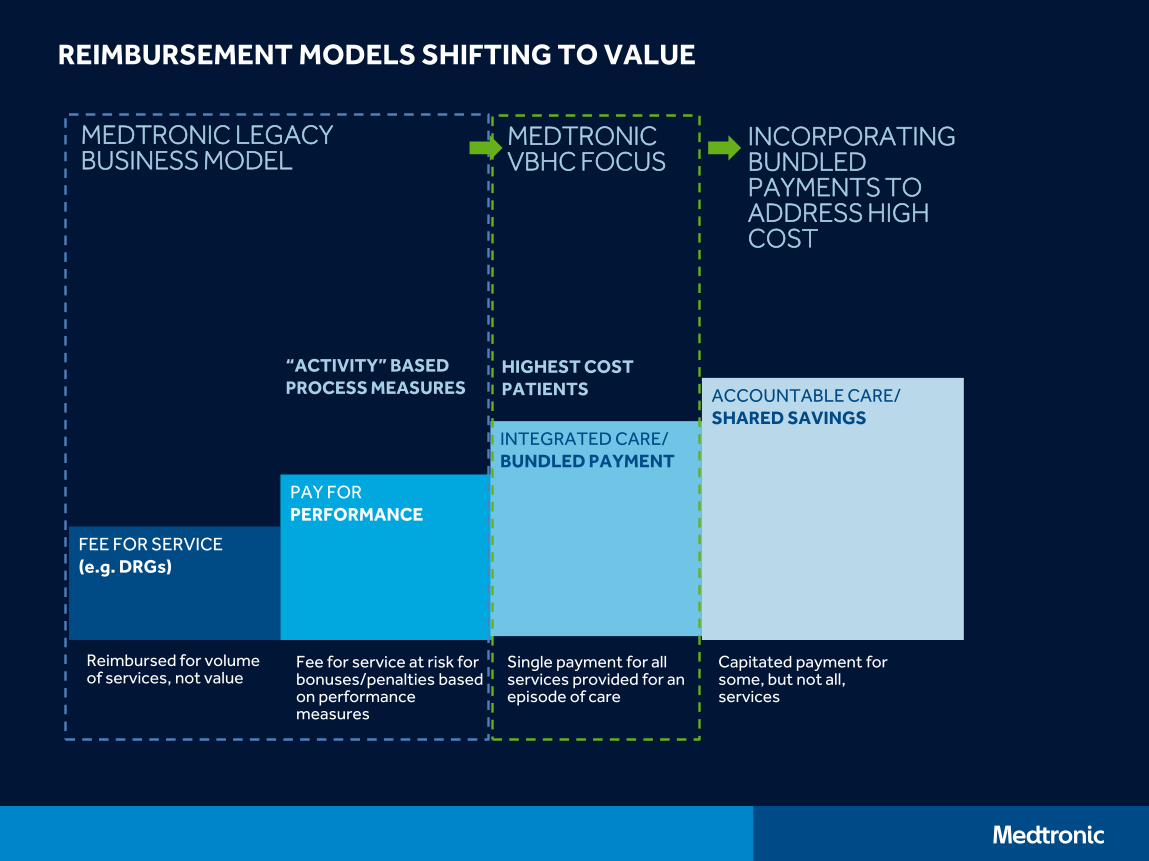
REIMBURSEMENT MODELS SHIFTING TO VALUE
FEE FOR SERVICE(e.g. DRGs)
PAY FORPERFORMANCE
Reimbursed for volume of services, not value
Fee for service at risk for bonuses/penalties based on performance measures
“ACTIVITY” BASED PROCESS MEASURES
MEDTRONIC LEGACY BUSINESS MODEL
INTEGRATED CARE/ BUNDLED PAYMENT
Single payment for all services provided for an episode of care
HIGHEST COST PATIENTS
MEDTRONIC VBHC FOCUS
ACCOUNTABLE CARE/SHARED SAVINGS
Capitated payment for some, but not all, services
INCORPORATING BUNDLED PAYMENTS TO ADDRESS HIGH COST
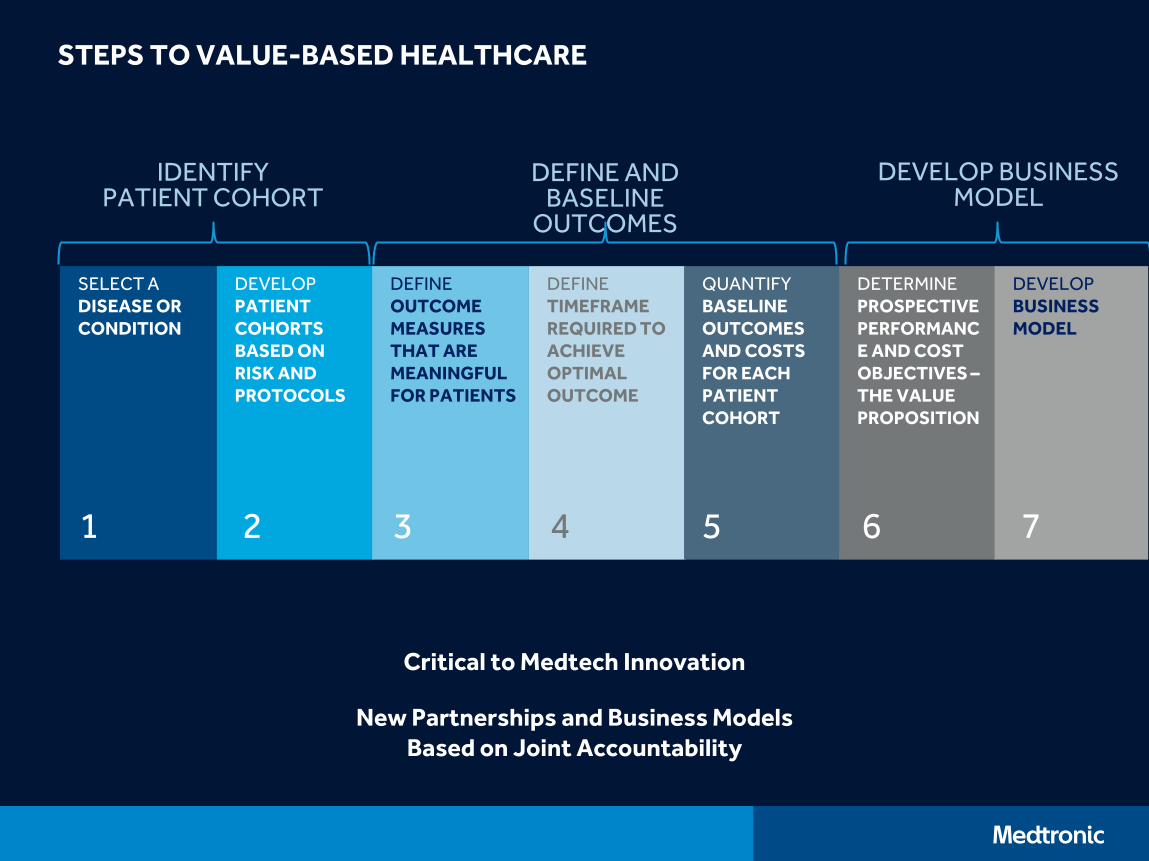
STEPS TO VALUE-BASED HEALTHCARE
SELECT ADISEASE OR CONDITION
DEVELOPPATIENT COHORTS BASED ON RISK AND PROTOCOLS
DEFINEOUTCOME MEASURESTHAT AREMEANINGFULFOR PATIENTS
DEFINETIMEFRAMEREQUIRED TO ACHIEVE OPTIMAL OUTCOME
QUANTIFYBASELINE OUTCOMES AND COSTS FOR EACH PATIENT COHORT
DETERMINEPROSPECTIVE PERFORMANCE AND COST OBJECTIVES –THE VALUE PROPOSITION
DEVELOPBUSINESS MODEL
1 2 3 4 5 6 7
Critical to Medtech Innovation
New Partnerships and Business Models Based on Joint Accountability
IDENTIFY PATIENT COHORT
DEFINE AND BASELINE
OUTCOMES
DEVELOP BUSINESS MODEL
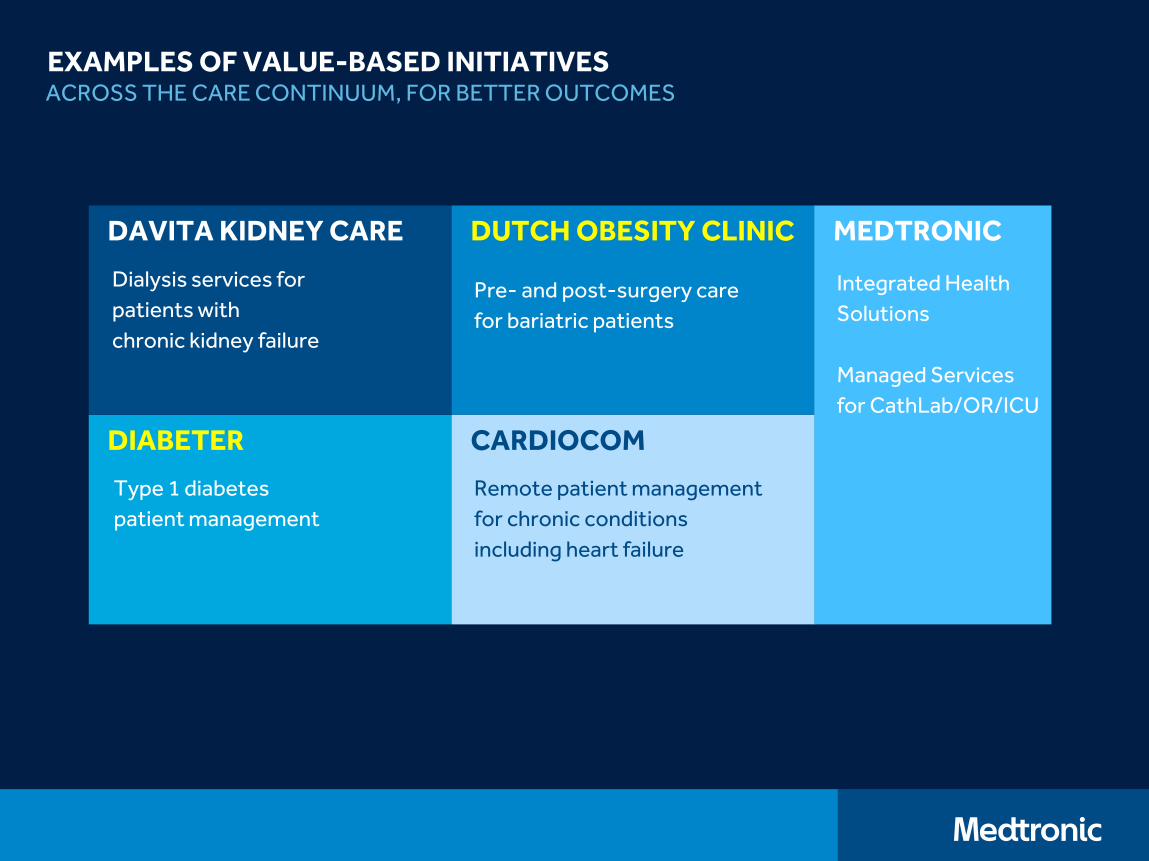
EXAMPLES OF VALUE-BASED INITIATIVES
DIABETER
Type 1 diabetes
patient management
DAVITA KIDNEY CARE
Dialysis services for
patients with
chronic kidney failure
DUTCH OBESITY CLINIC
Pre- and post-surgery care
for bariatric patients
CARDIOCOM
Remote patient management
for chronic conditions
including heart failure
MEDTRONIC
Integrated Health
Solutions
Managed Services
for CathLab/OR/ICU
ACROSS THE CARE CONTINUUM, FOR BETTER OUTCOMES
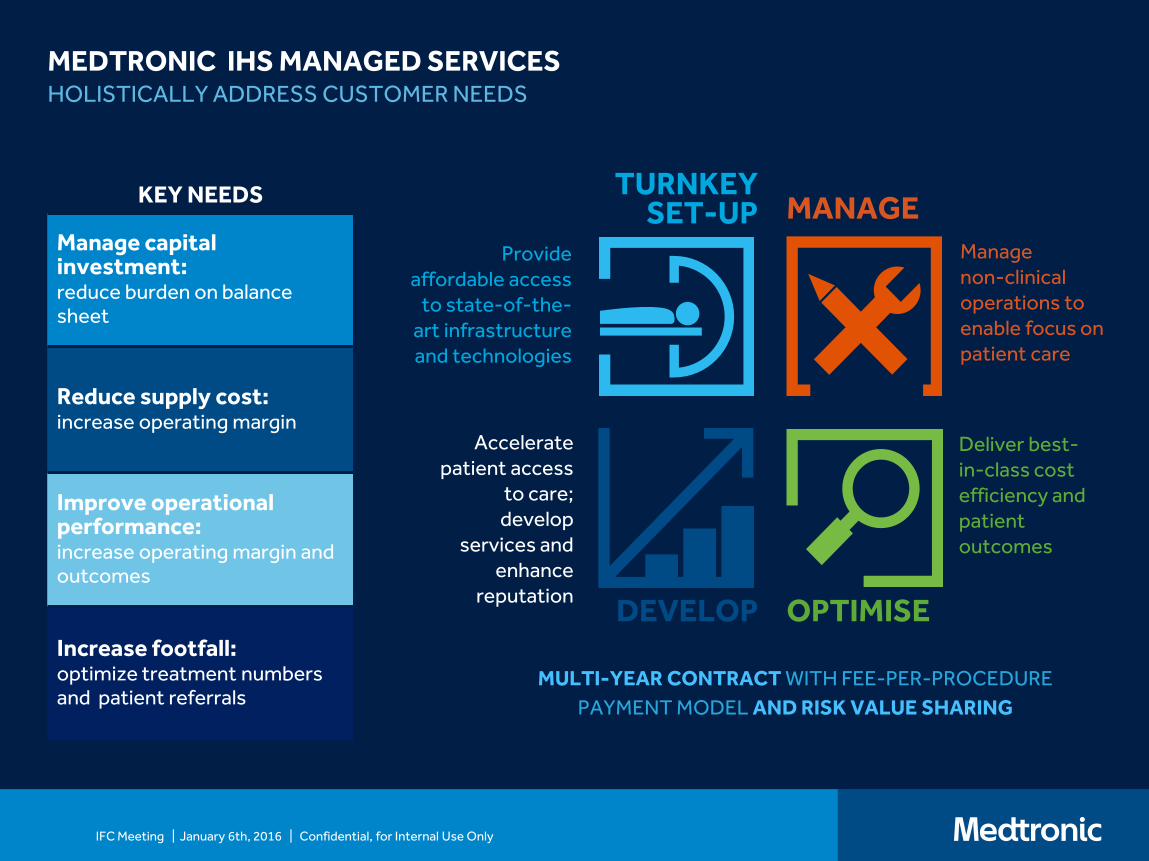
MEDTRONIC IHS MANAGED SERVICESHOLISTICALLY ADDRESS CUSTOMER NEEDS
KEY NEEDS
Manage capital investment: reduce burden on balance sheet
Reduce supply cost: increase operating margin
Improve operational performance: increase operating margin and outcomes
Increase footfall: optimize treatment numbers and patient referrals
Provide affordable access
to state-of-the-art infrastructure and technologies
Manage non-clinical operations to enable focus on patient care
Deliver best-in-class cost efficiency and patient outcomes
Accelerate patient access
to care; develop
services and enhance
reputation
TURNKEY SET-UP MANAGE
OPTIMISEDEVELOP
MULTI-YEAR CONTRACT WITH FEE-PER-PROCEDURE
PAYMENT MODEL AND RISK VALUE SHARING
IFC Meeting | January 6th, 2016 | Confidential, for Internal Use Only
JOSH MACHTExecutive Vice President & Group PublisherHarvard Business Review
The International Consortium for Health Outcomes Measurement (ICHOM)
14th April 2016
Standard Presentation.pptx 16Copyright © 2013 by the International Consortium for Health Outcomes Measurement. All rights reserved.
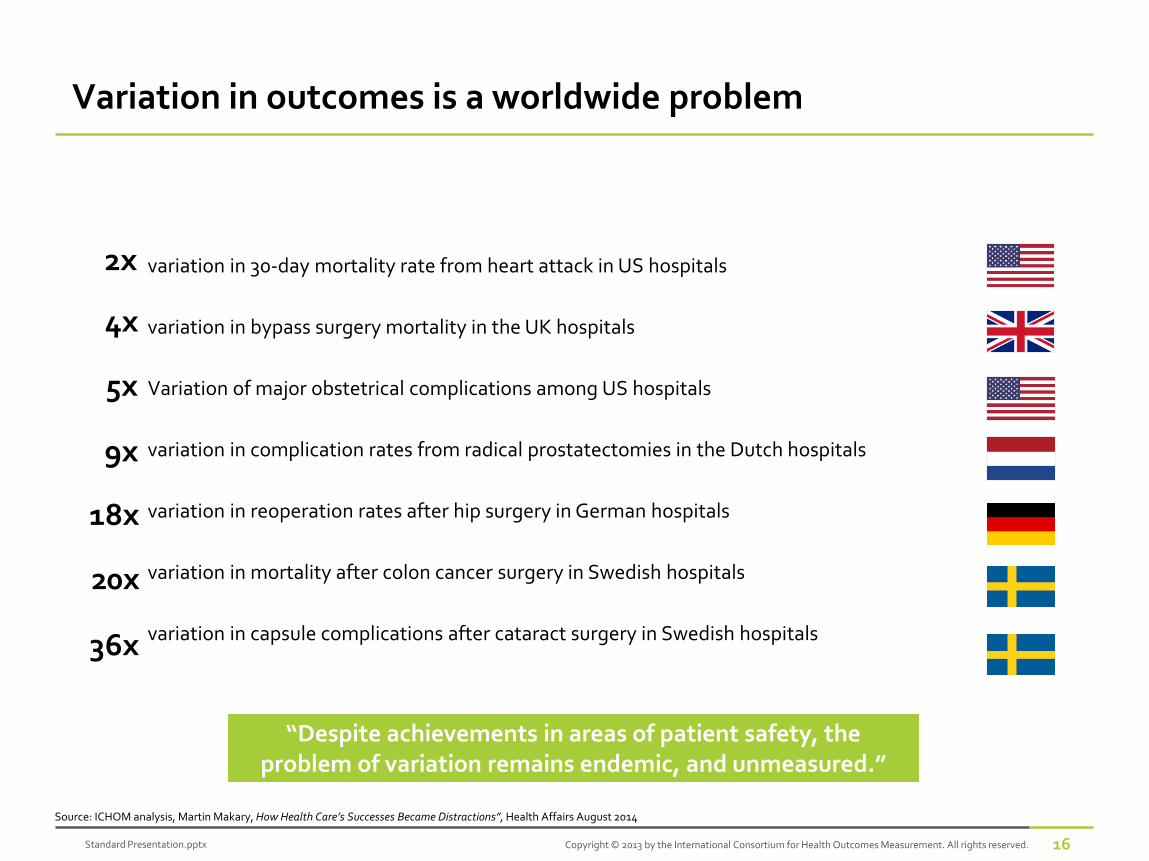
variation in 30-day mortality rate from heart attack in US hospitals
variation in bypass surgery mortality in the UK hospitals
Variation of major obstetrical complications among US hospitals
variation in complication rates from radical prostatectomies in the Dutch hospitals
variation in reoperation rates after hip surgery in German hospitals
variation in mortality after colon cancer surgery in Swedish hospitals
variation in capsule complications after cataract surgery in Swedish hospitals
Variation in outcomes is a worldwide problem
4x
9x
18x
20x
36x
2x
Source: ICHOM analysis, Martin Makary, How Health Care’s Successes Became Distractions”, Health Affairs August 2014
5x
“Despite achievements in areas of patient safety, the problem of variation remains endemic, and unmeasured.”
Standard Presentation.pptx 17Copyright © 2013 by the International Consortium for Health Outcomes Measurement. All rights reserved.
75.5
43.3
94.0
80.0
50.0
94.0
34.7
6.5
95.0
0
10
20
30
40
50
60
70
80
90
100
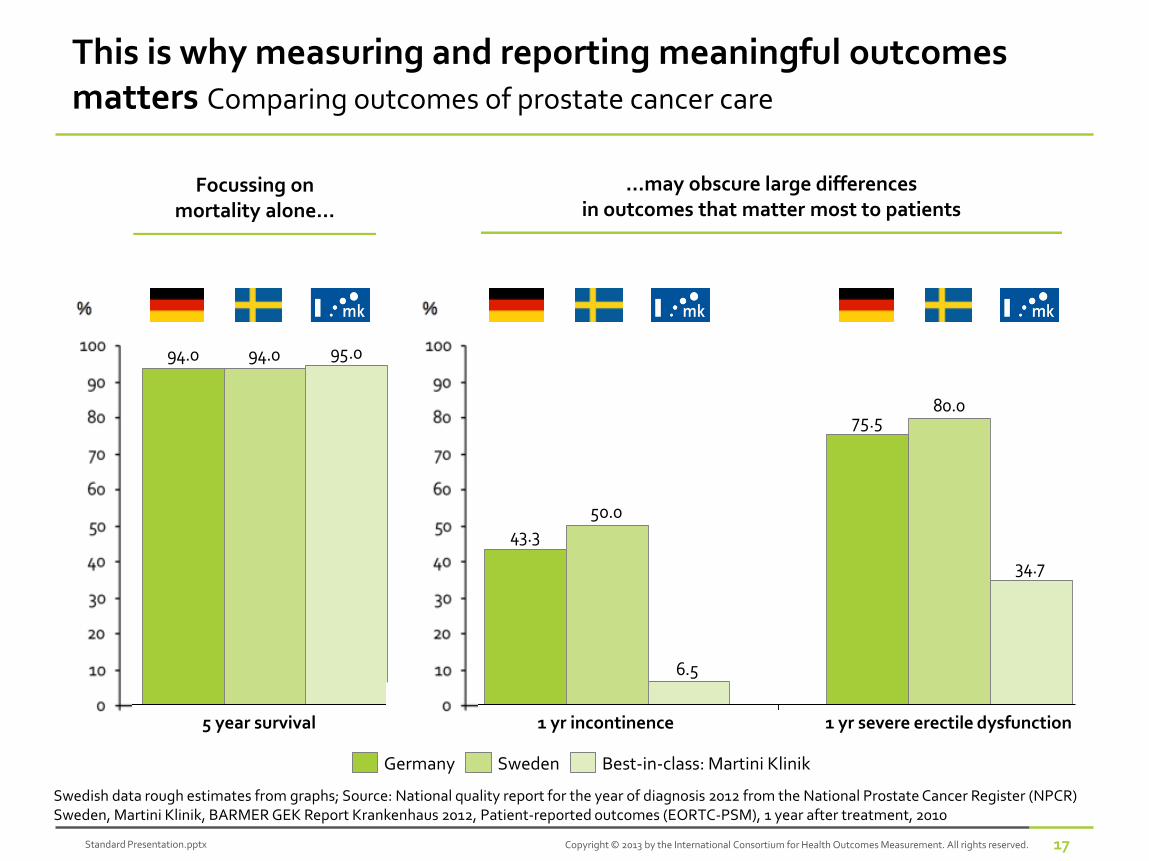
This is why measuring and reporting meaningful outcomes matters Comparing outcomes of prostate cancer care
Swedish data rough estimates from graphs; Source: National quality report for the year of diagnosis 2012 from the National Prostate Cancer Register (NPCR) Sweden, Martini Klinik, BARMER GEK Report Krankenhaus 2012, Patient-reported outcomes (EORTC-PSM), 1 year after treatment, 2010
1 yr severe erectile dysfunction
%
1 yr incontinence5 year survival
Best-in-class: Martini KlinikGermany Sweden
Focussing on mortality alone…
…may obscure large differences in outcomes that matter most to patients
Standard Presentation.pptx 18Copyright © 2013 by the International Consortium for Health Outcomes Measurement. All rights reserved.
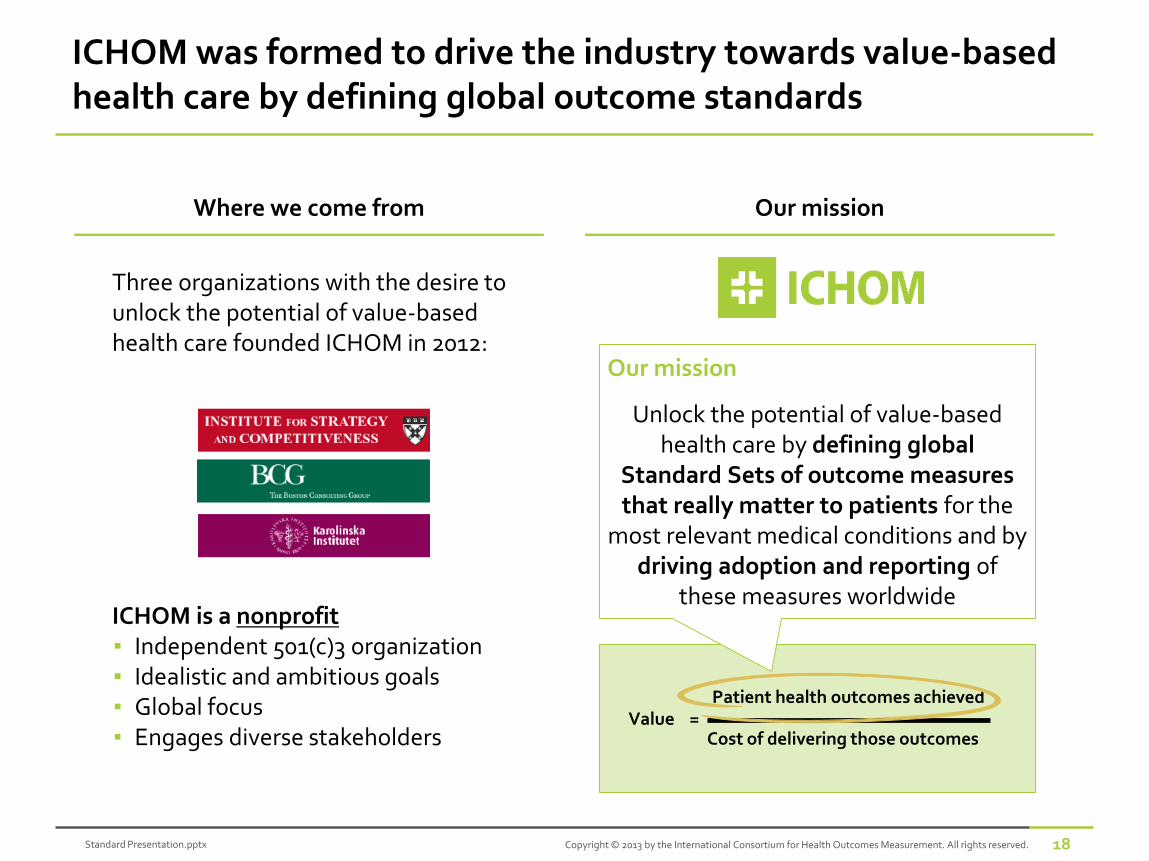
ICHOM was formed to drive the industry towards value-based health care by defining global outcome standards
Our missionWhere we come from
Three organizations with the desire to unlock the potential of value-based health care founded ICHOM in 2012:
ICHOM is a nonprofit▪ Independent 501(c)3 organization▪ Idealistic and ambitious goals▪ Global focus▪ Engages diverse stakeholders
Value =
Our mission
Unlock the potential of value-based health care by defining global
Standard Sets of outcome measures that really matter to patients for the
most relevant medical conditions and by driving adoption and reporting of
these measures worldwide
Cost of delivering those outcomes
Patient health outcomes achieved
Standard Presentation.pptx 19Copyright © 2013 by the International Consortium for Health Outcomes Measurement. All rights reserved.
The starting point for value-based health care reform is to measure meaningful outcomes
5 reasons why outcome measurement is essential:
Outcomes define the goal of the organization and its accountability to patients
Outcomes inform the composition of integrated care teams
Outcomes motivate clinicians to collaborate and improve together
Outcomes highlight value-enhancing cost reduction
Outcomes enable payment to shift from volume to results
1
2
3
4
5
See full article in Harvard Business Review: https://hbr.org/2015/09/better-value-in-health-care-requires-focusing-on-outcomes
Standard Presentation.pptx 20Copyright © 2013 by the International Consortium for Health Outcomes Measurement. All rights reserved.
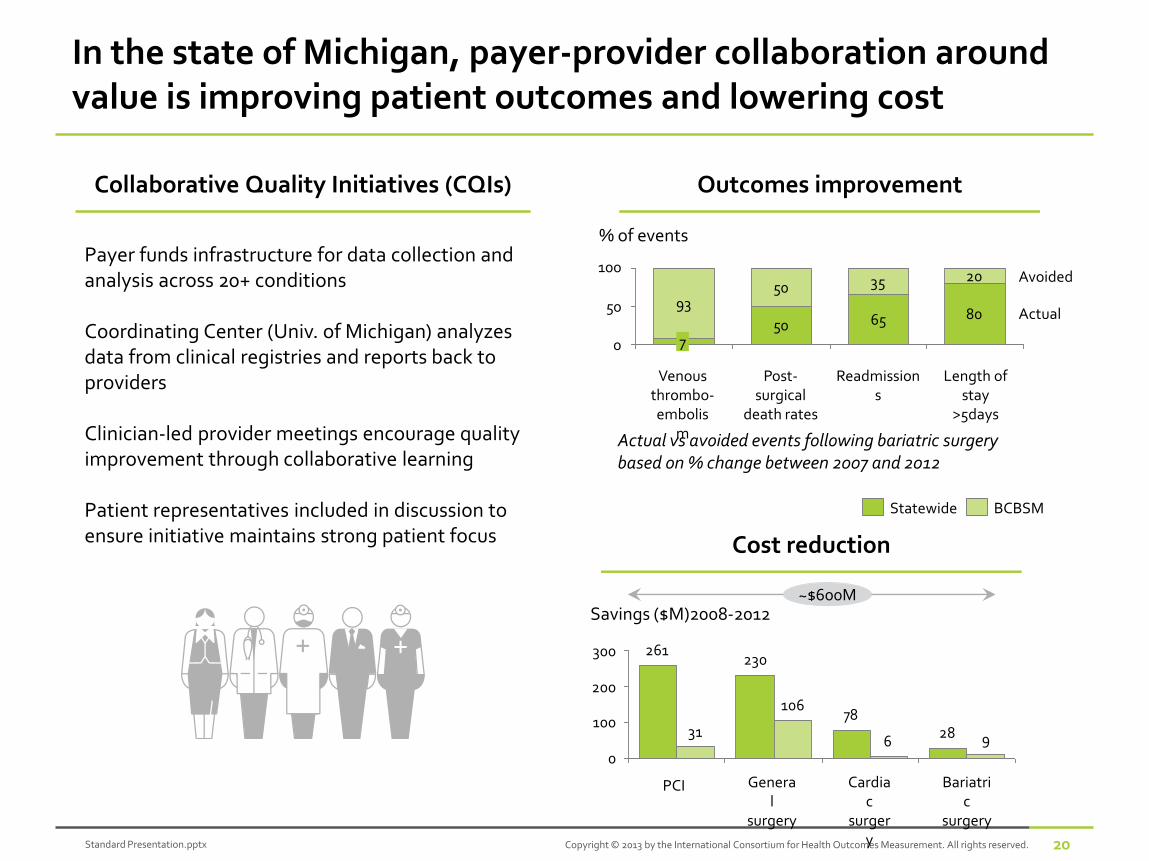
In the state of Michigan, payer-provider collaboration around value is improving patient outcomes and lowering cost
Collaborative Quality Initiatives (CQIs)
Payer funds infrastructure for data collection and analysis across 20+ conditions
Coordinating Center (Univ. of Michigan) analyzes data from clinical registries and reports back to providers
Clinician-led provider meetings encourage quality improvement through collaborative learning
Patient representatives included in discussion to ensure initiative maintains strong patient focus Cost reduction
2878
230261
96
106
31
0
100
200
300
PCI Cardiac
surgery
General
surgery
Savings ($M)2008-2012
Bariatric
surgery
~$600M
50 65 8093
50 35 20
50
100
0
% of events
Avoided
Readmissions
Length of stay
>5days
Venous thrombo-embolis
m
Post-surgical
death rates
7
Actual
Outcomes improvement
Actual vs avoided events following bariatric surgery based on % change between 2007 and 2012
Statewide BCBSM
Standard Presentation.pptx 21Copyright © 2013 by the International Consortium for Health Outcomes Measurement. All rights reserved.
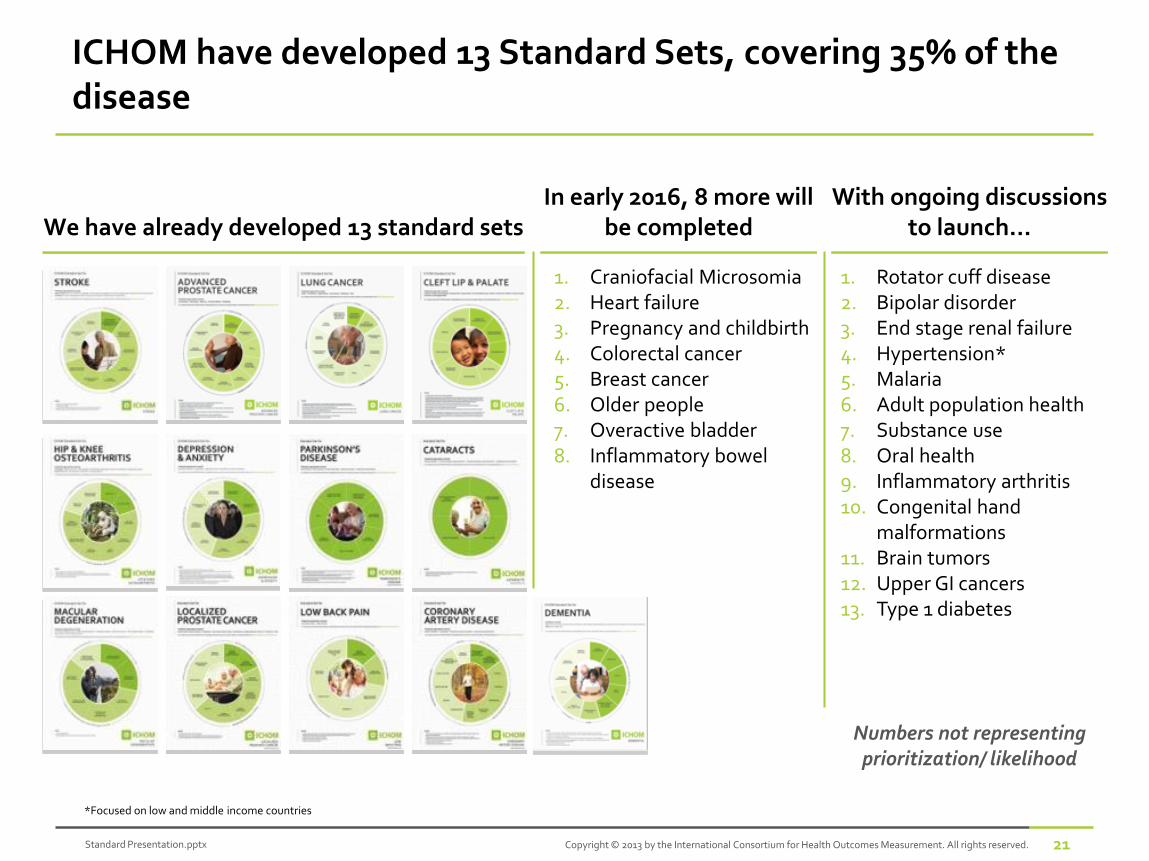
ICHOM have developed 13 Standard Sets, covering 35% of the disease
We have already developed 13 standard setsIn early 2016, 8 more will
be completedWith ongoing discussions
to launch...
1. Craniofacial Microsomia2. Heart failure3. Pregnancy and childbirth4. Colorectal cancer5. Breast cancer6. Older people7. Overactive bladder8. Inflammatory bowel
disease
1. Rotator cuff disease2. Bipolar disorder3. End stage renal failure4. Hypertension* 5. Malaria6. Adult population health7. Substance use8. Oral health9. Inflammatory arthritis10. Congenital hand
malformations11. Brain tumors12. Upper GI cancers13. Type 1 diabetes
Numbers not representing prioritization/ likelihood
*Focused on low and middle income countries
Standard Presentation.pptx 22Copyright © 2013 by the International Consortium for Health Outcomes Measurement. All rights reserved.
Strong global demand to measure and compare outcomes
Standard Presentation.pptx 23Copyright © 2013 by the International Consortium for Health Outcomes Measurement. All rights reserved.
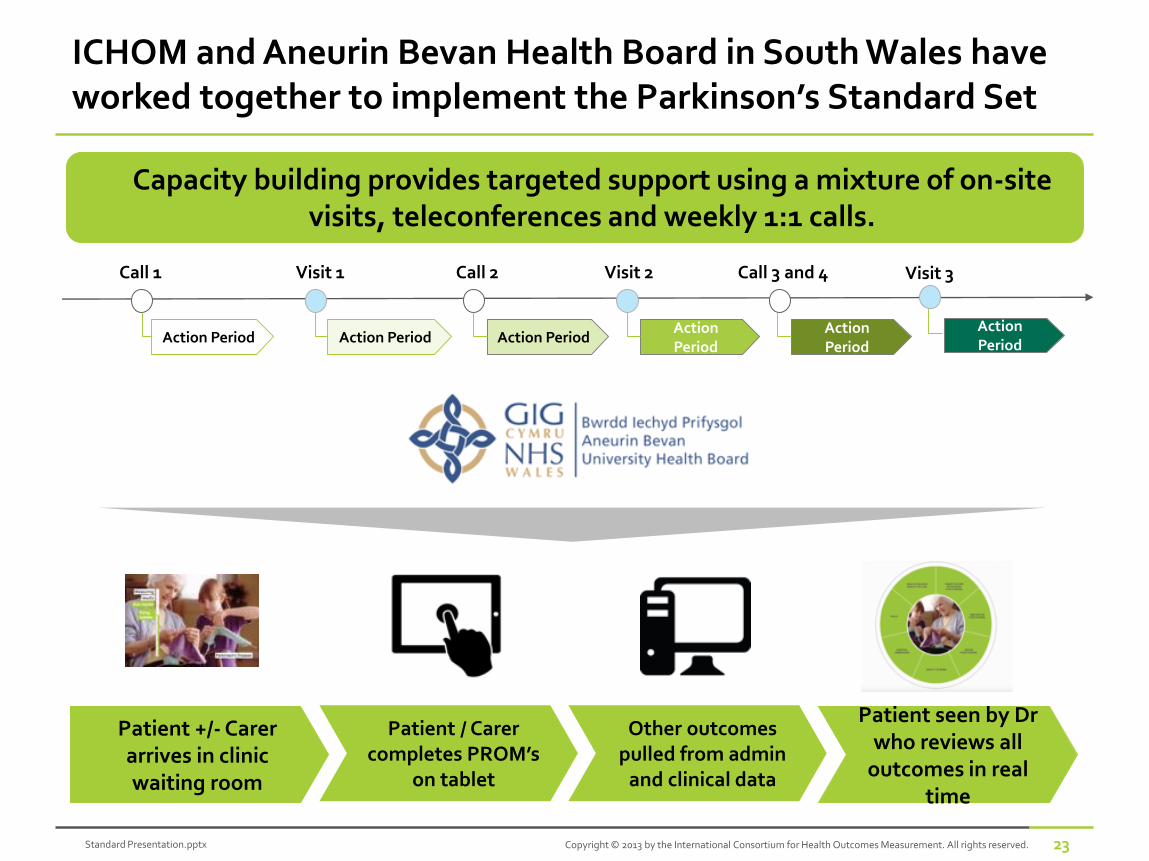
ICHOM and Aneurin Bevan Health Board in South Wales have worked together to implement the Parkinson’s Standard Set
Capacity building provides targeted support using a mixture of on-site visits, teleconferences and weekly 1:1 calls.
Action Period
Call 1 Visit 1 Call 2 Visit 2
Action Period Action PeriodAction Period
Call 3 and 4
Action Period
Action Period
Visit 3
Patient +/- Carer arrives in clinic waiting room
Patient / Carer completes PROM’s
on tablet
Patient seen by Dr who reviews all
outcomes in real time
Other outcomes pulled from admin
and clinical data
Standard Presentation.pptx 24Copyright © 2013 by the International Consortium for Health Outcomes Measurement. All rights reserved.
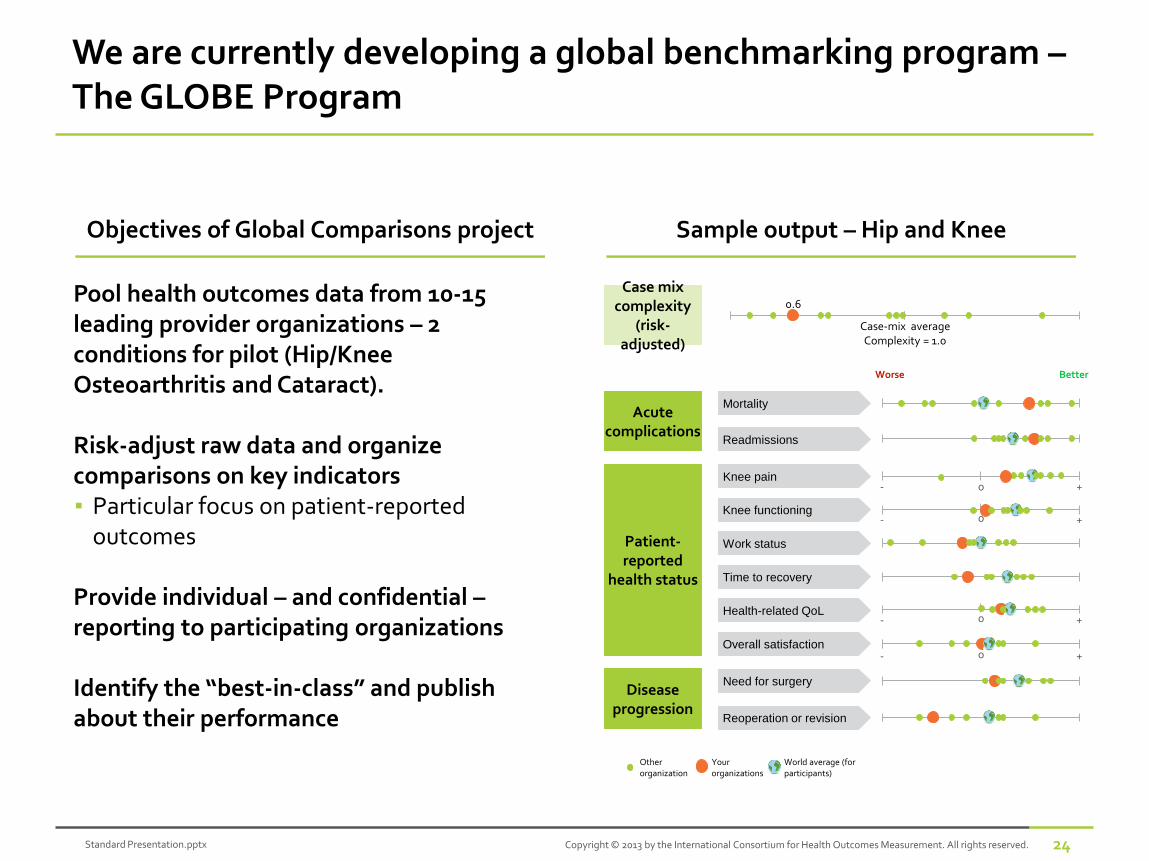
We are currently developing a global benchmarking program –The GLOBE Program
Objectives of Global Comparisons project
Pool health outcomes data from 10-15 leading provider organizations – 2 conditions for pilot (Hip/Knee Osteoarthritis and Cataract).
Risk-adjust raw data and organize comparisons on key indicators▪ Particular focus on patient-reported
outcomes
Provide individual – and confidential –reporting to participating organizations
Identify the “best-in-class” and publish about their performance
Sample output – Hip and Knee
Worse Better
Mortality
Readmissions
Acute complications
Patient-reported
health status
Disease progression
Knee pain
Knee functioning
Work status
Time to recovery
Health-related QoL
Overall satisfaction
Need for surgery
Reoperation or revision
Case mix complexity
(risk-adjusted)
Other organization
Your organizations
World average (for participants)
0.6
Case-mix averageComplexity = 1.0
- +
- +
0
0
- +0
- +0
Standard Presentation.pptx 25Copyright © 2013 by the International Consortium for Health Outcomes Measurement. All rights reserved.
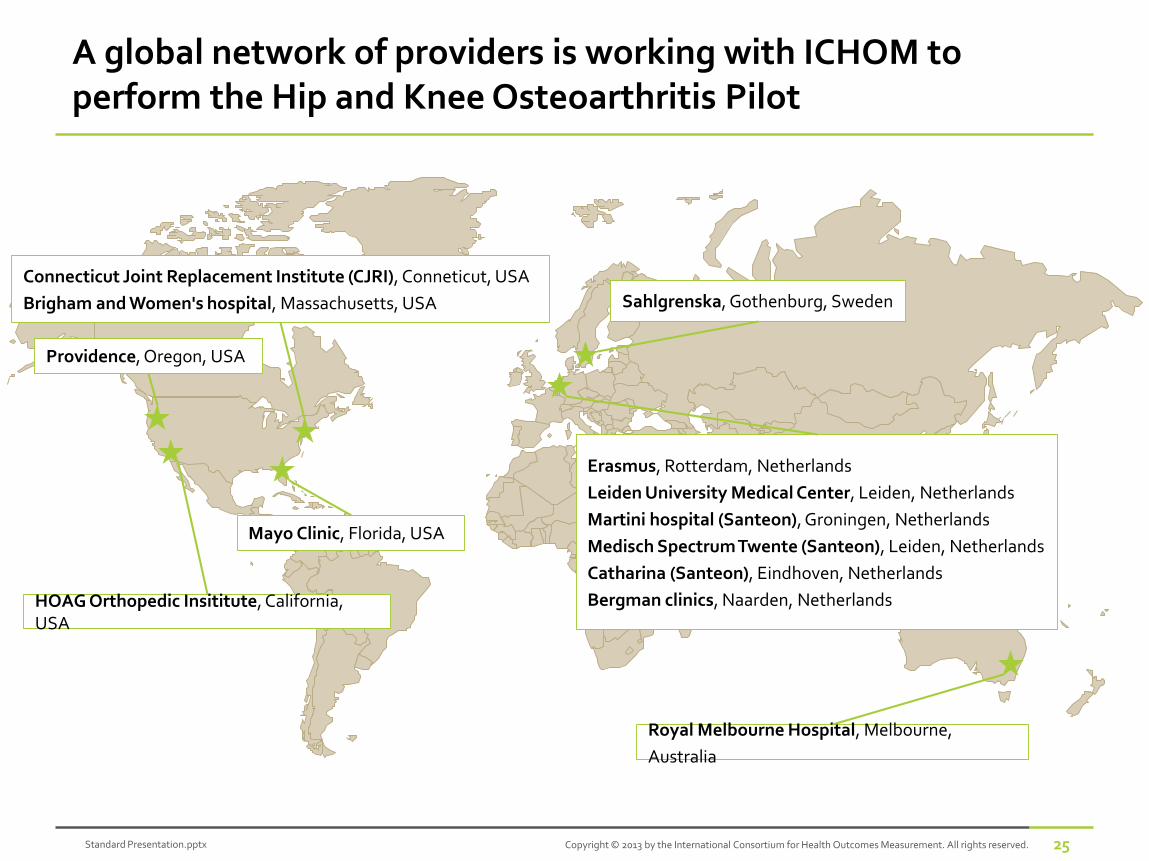
Royal Melbourne Hospital, Melbourne,
Australia
Erasmus, Rotterdam, Netherlands
Leiden University Medical Center, Leiden, Netherlands
Martini hospital (Santeon), Groningen, Netherlands
Medisch Spectrum Twente (Santeon), Leiden, Netherlands
Catharina (Santeon), Eindhoven, Netherlands
Bergman clinics, Naarden, Netherlands
Sahlgrenska, Gothenburg, Sweden
Connecticut Joint Replacement Institute (CJRI), Conneticut, USA
Brigham and Women's hospital, Massachusetts, USA
Mayo Clinic, Florida, USA
HOAG Orthopedic Insititute, California, USA
Providence, Oregon, USA
A global network of providers is working with ICHOM to perform the Hip and Knee Osteoarthritis Pilot
Standard Presentation.pptx 26Copyright © 2013 by the International Consortium for Health Outcomes Measurement. All rights reserved.
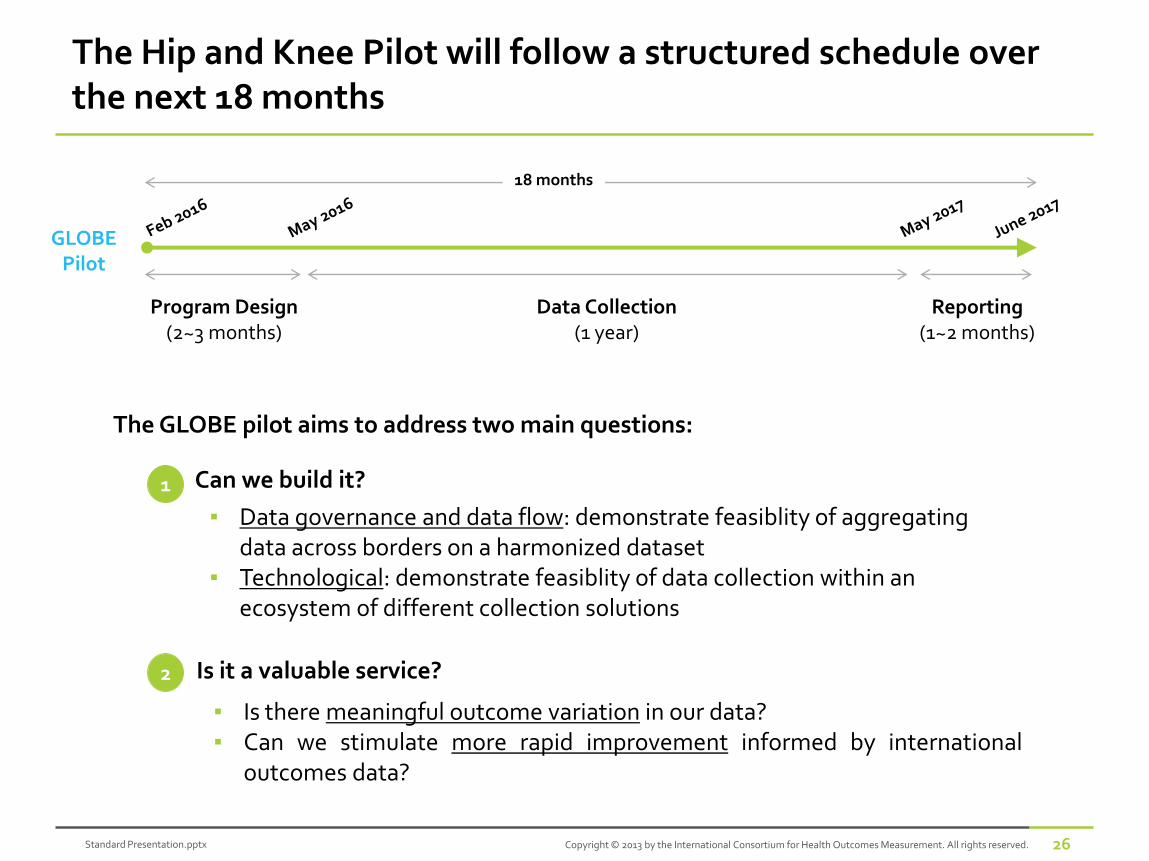
The Hip and Knee Pilot will follow a structured schedule over the next 18 months
▪ Data governance and data flow: demonstrate feasiblity of aggregating data across borders on a harmonized dataset
▪ Technological: demonstrate feasiblity of data collection within an ecosystem of different collection solutions
1
2
Can we build it?
Is it a valuable service?
▪ Is there meaningful outcome variation in our data?▪ Can we stimulate more rapid improvement informed by international
outcomes data?
The GLOBE pilot aims to address two main questions:
GLOBEPilot
18 months
Program Design(2~3 months)
Data Collection(1 year)
Reporting(1~2 months)
Standard Presentation.pptx 27Copyright © 2013 by the International Consortium for Health Outcomes Measurement. All rights reserved.
Join us in London for the Fourth ICHOM Conference!
In May 2016, the ICHOM team will hold our largest conference to date. We would be delighted if you would join us.
▪ When and where: May 16-17, University College London
▪ Content: The theme of the 2016 conference will be implementation and impact: how to implement the Standard Sets—and the positive results that can come from outcomes measurement.
▪ Format:Attendees will participate in two days of plenary sessions, small-group discussions, and networking, with opportunities to hear from members of the ICHOM team, distinguished guest speakers, and from one another.
▪ Register here:http://www.ichom.org/2016-ichom-conference/
Measuring Outcomes:ERAS Society perspective
Olle Ljungqvist MD, PhDChairman ERAS Society
Professor of Surgery
Örebro University & Karolinska Insitutet
HBR-Medtronic Optimizing Costs and Outcomes in Healthcare
Gothenburgh Quality Forum
April 14, 2016
Improving Perioperative Care Worldwide
Health Care Challenges
• Growing and ageing population
• Pressure for better results
• Diminishing funding
• Better care for less cost – Fast
Obstacles
>15 years ago……

Last year: March 31, 2015
Understanding the playground

Hospital organization
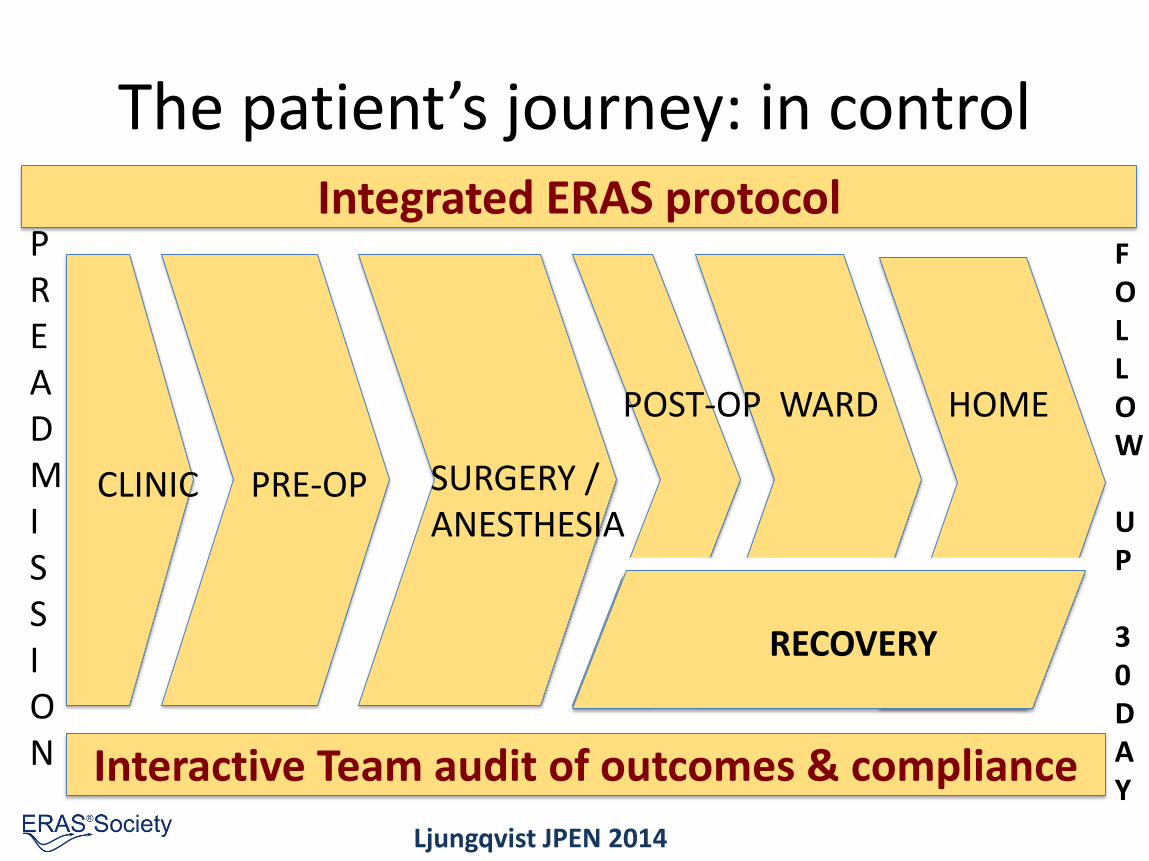
The patient’s journey: in control
CLINIC PRE-OP
POST-OP WARD HOME
RECOVERY
SURGERY /ANESTHESIA
Interactive Team audit of outcomes & compliance
PREADMISSION
FOLLOW
UP
30DAY
Integrated ERAS protocol
Ljungqvist JPEN 2014
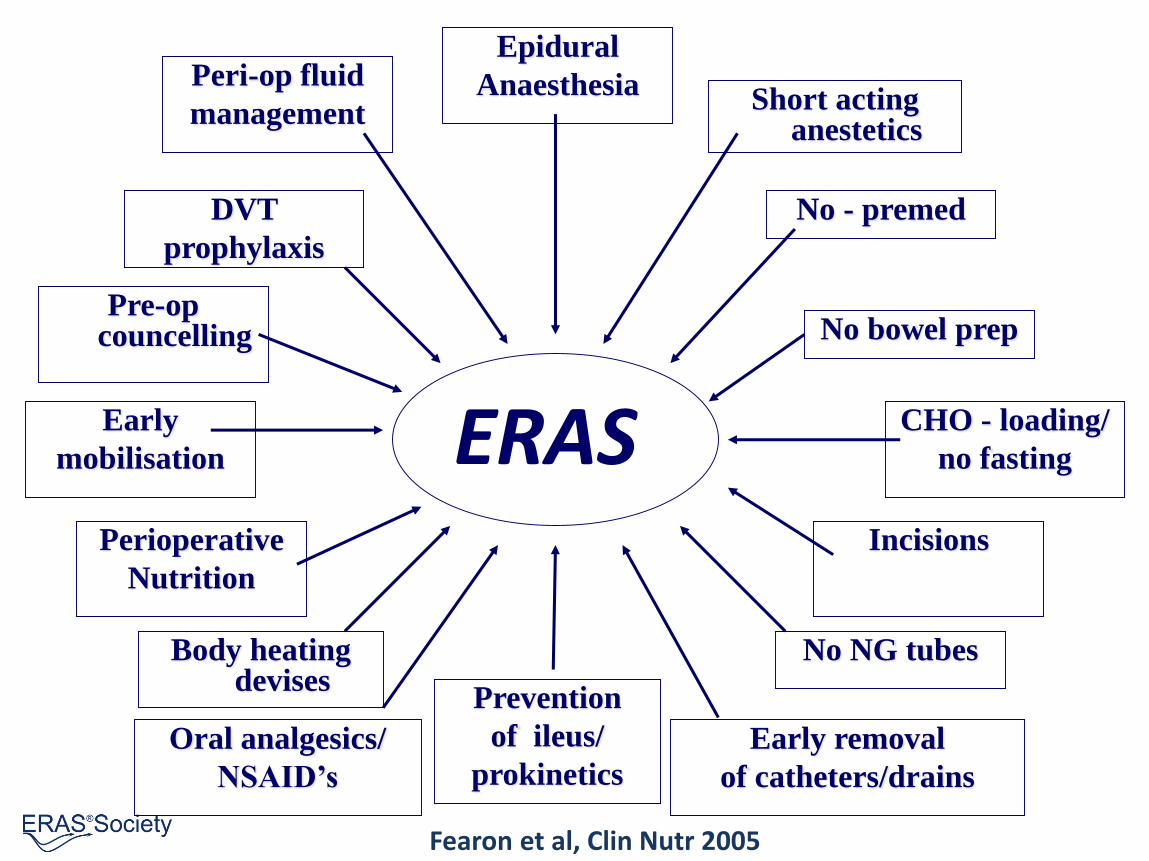
ERAS
Epidural
Anaesthesia
Prevention
of ileus/
prokinetics
CHO - loading/
no fasting
Early
mobilisation
Peri-op fluid
management
DVT
prophylaxis
Pre-op councelling
Short acting anestetics
No - premed
No bowel prep
Perioperative
Nutrition
Body heating devises
Oral analgesics/
NSAID’s
Incisions
No NG tubes
Early removal
of catheters/drains
Fearon et al, Clin Nutr 2005
Nice idea!
But…does it work?
Relevant outcomes
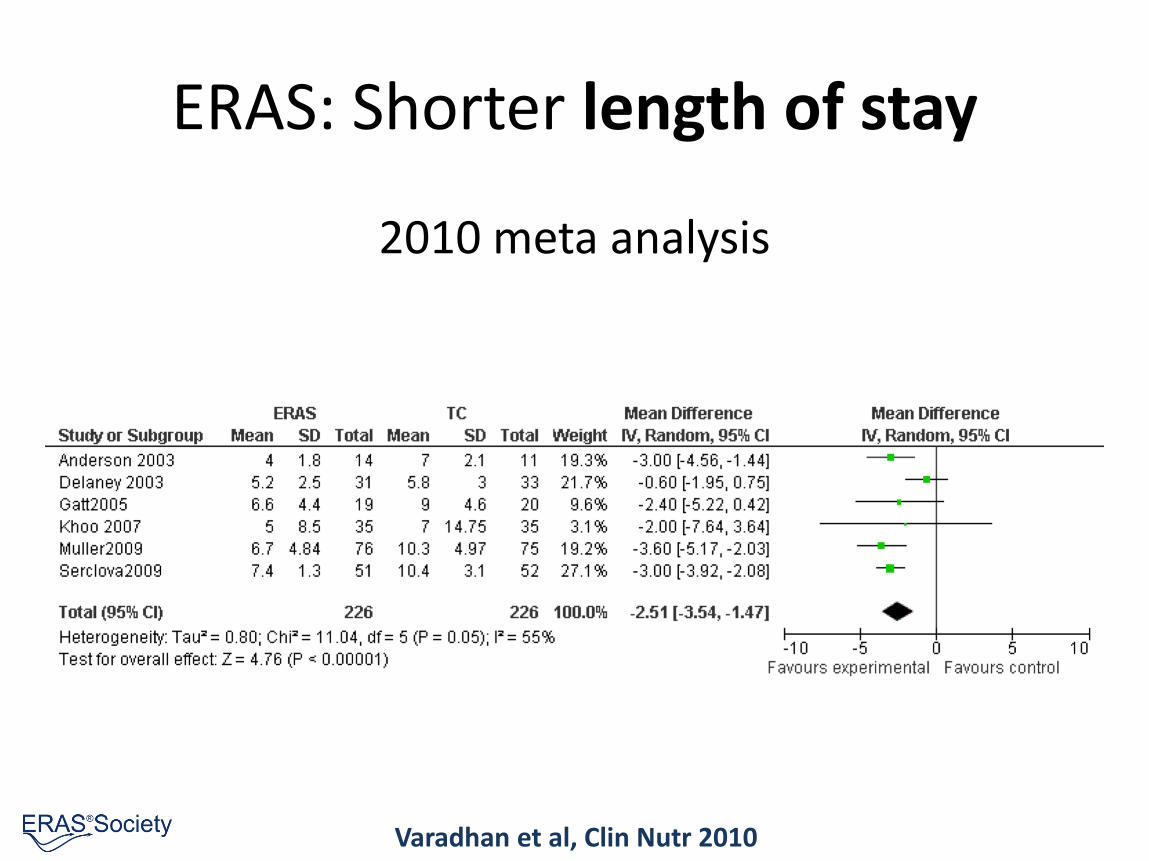
ERAS: Shorter length of stay
2010 meta analysis
Varadhan et al, Clin Nutr 2010
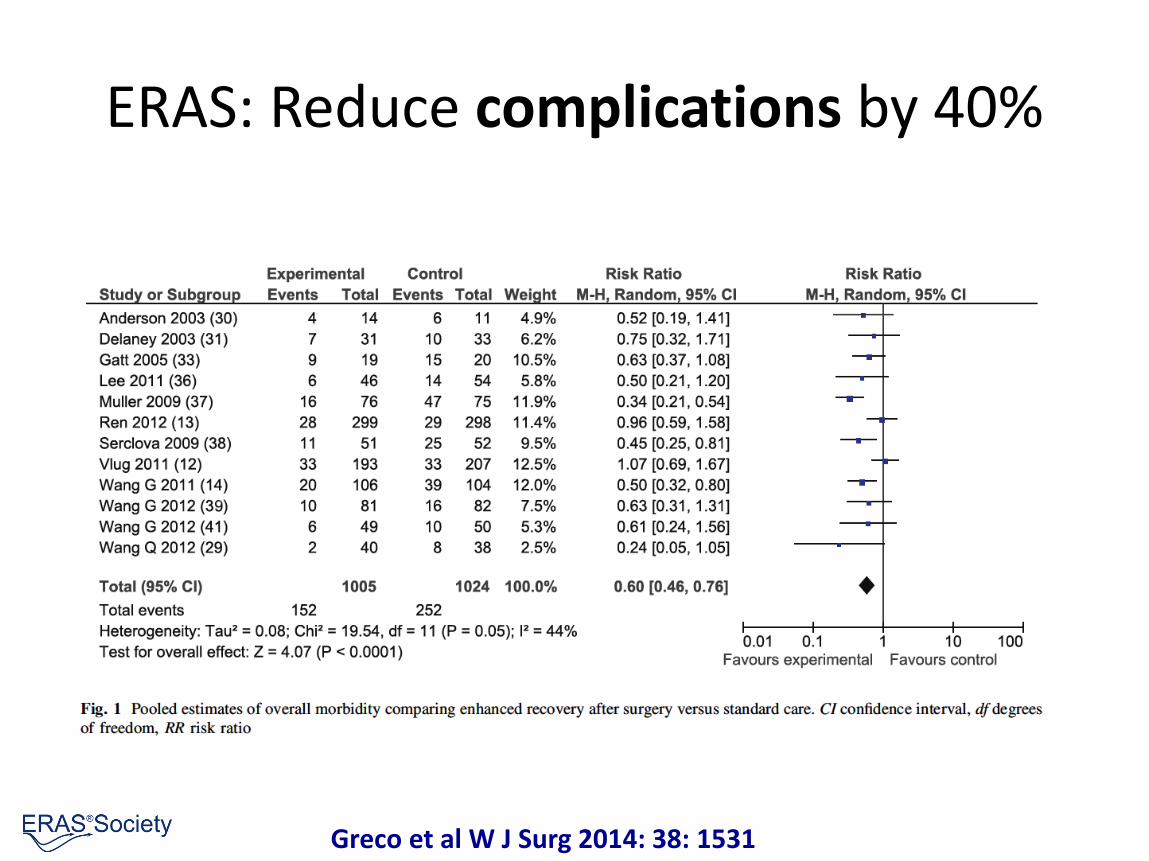
ERAS: Reduce complications by 40%
Greco et al W J Surg 2014: 38: 1531
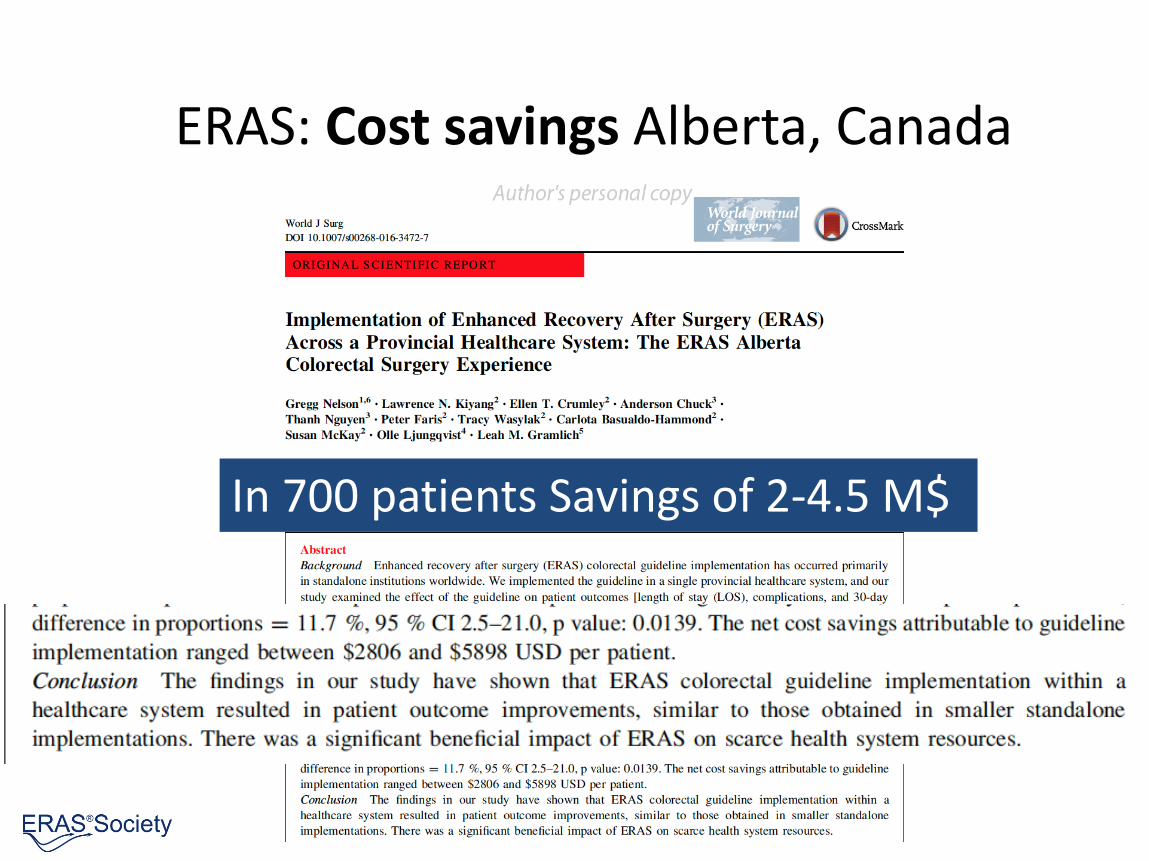
ERAS: Cost savings Alberta, Canada
In 700 patients Savings of 2-4.5 M$
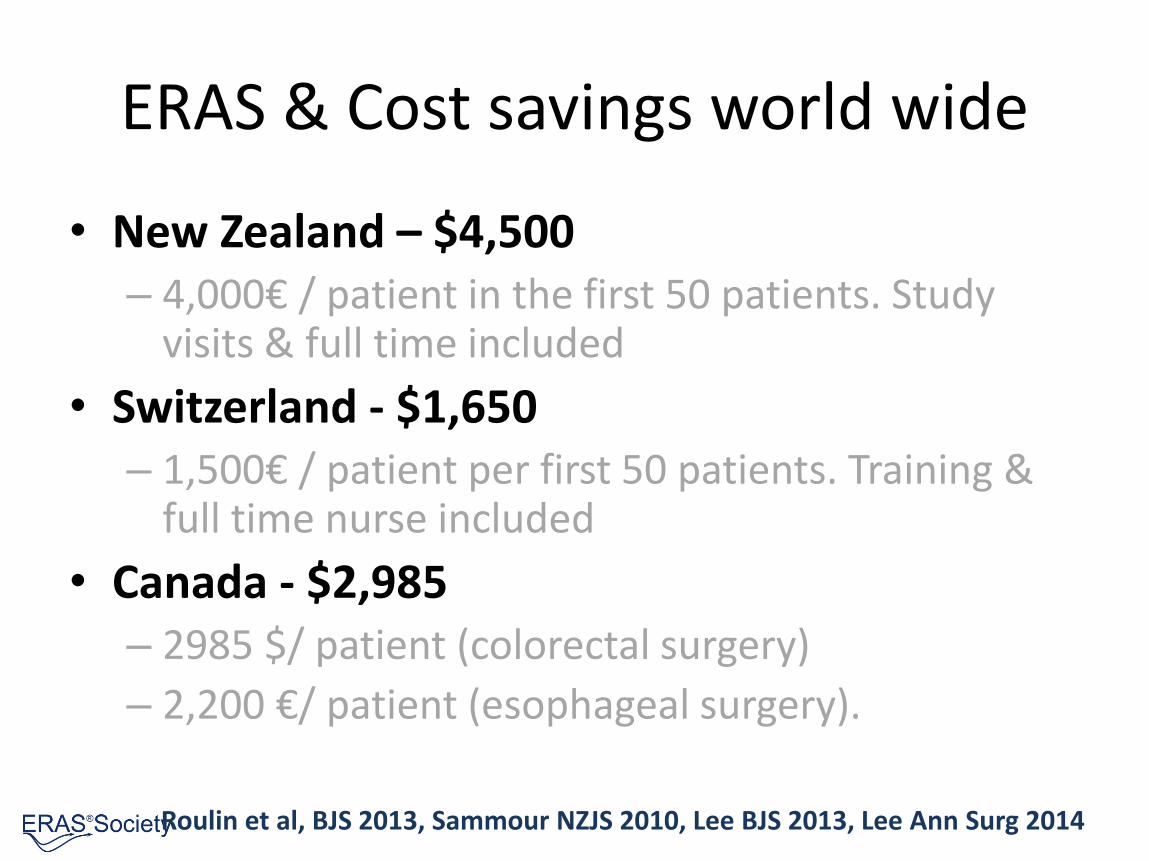
ERAS & Cost savings world wide
• New Zealand – $4,500– 4,000€ / patient in the first 50 patients. Study
visits & full time included
• Switzerland - $1,650– 1,500€ / patient per first 50 patients. Training &
full time nurse included
• Canada - $2,985– 2985 $/ patient (colorectal surgery)
– 2,200 €/ patient (esophageal surgery).
Roulin et al, BJS 2013, Sammour NZJS 2010, Lee BJS 2013, Lee Ann Surg 2014
ERAS Society approach
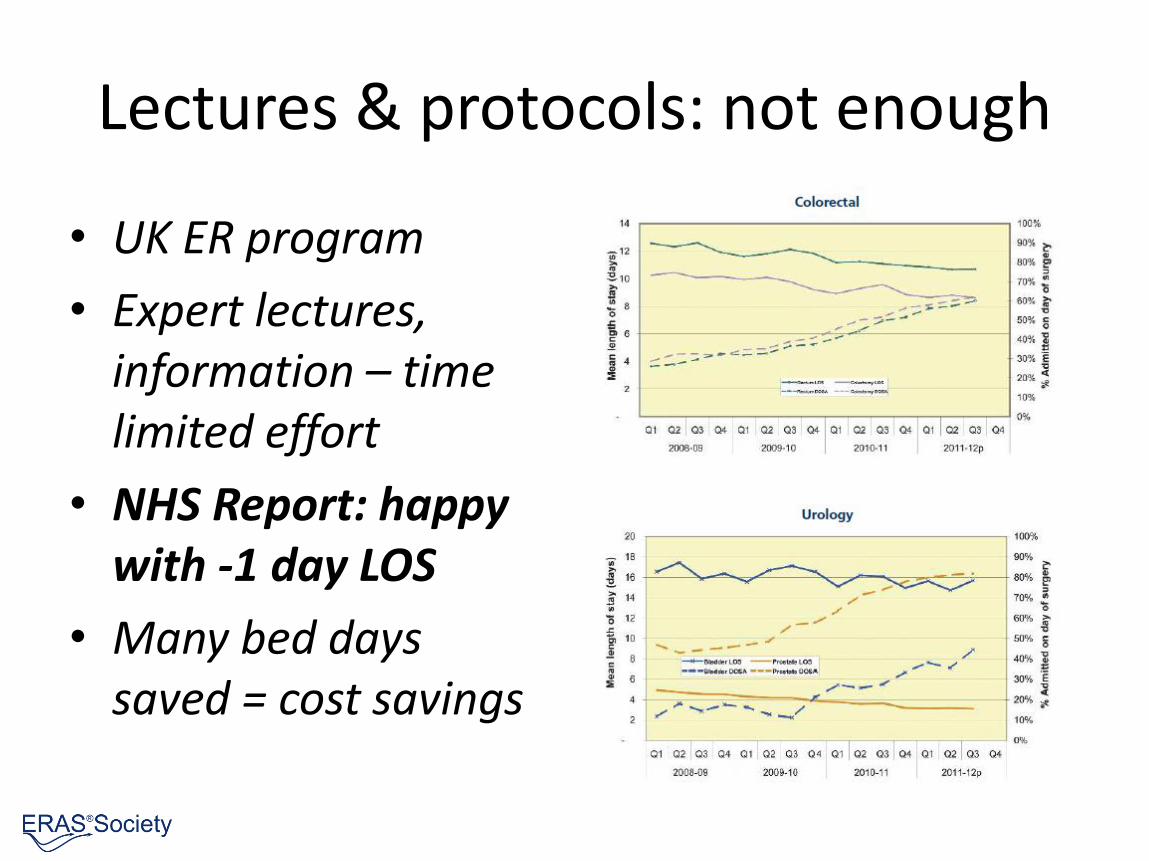
Lectures & protocols: not enough
• UK ER program
• Expert lectures, information – timelimited effort
• NHS Report: happy with -1 day LOS
• Many bed dayssaved = cost savings

ERAS® Implementation ProgramBuilding Blocks
• World Experts
– Guidelines
– Centers of Excellence (teaching)
• Structured Training
– Breakthrough tailored for ERAS
– Qulturum (IHI Sweden) and others
• IT support – ERAS Interactive Audit System
– Encare & Partners
Colorectal
Pancreatic resection
Cystectomy
Gastrectomy
2015: Anaesthesia
2015/16: Gynecology
Bariatric
Breast reconstruction
H & N cancer
Nephrectomy
Hip replacement
Knee replacement
Liver resection
Thoracic
Esophageal resection
ERAS® Society Guidelines

Do the guidelines work?A test of Compliance
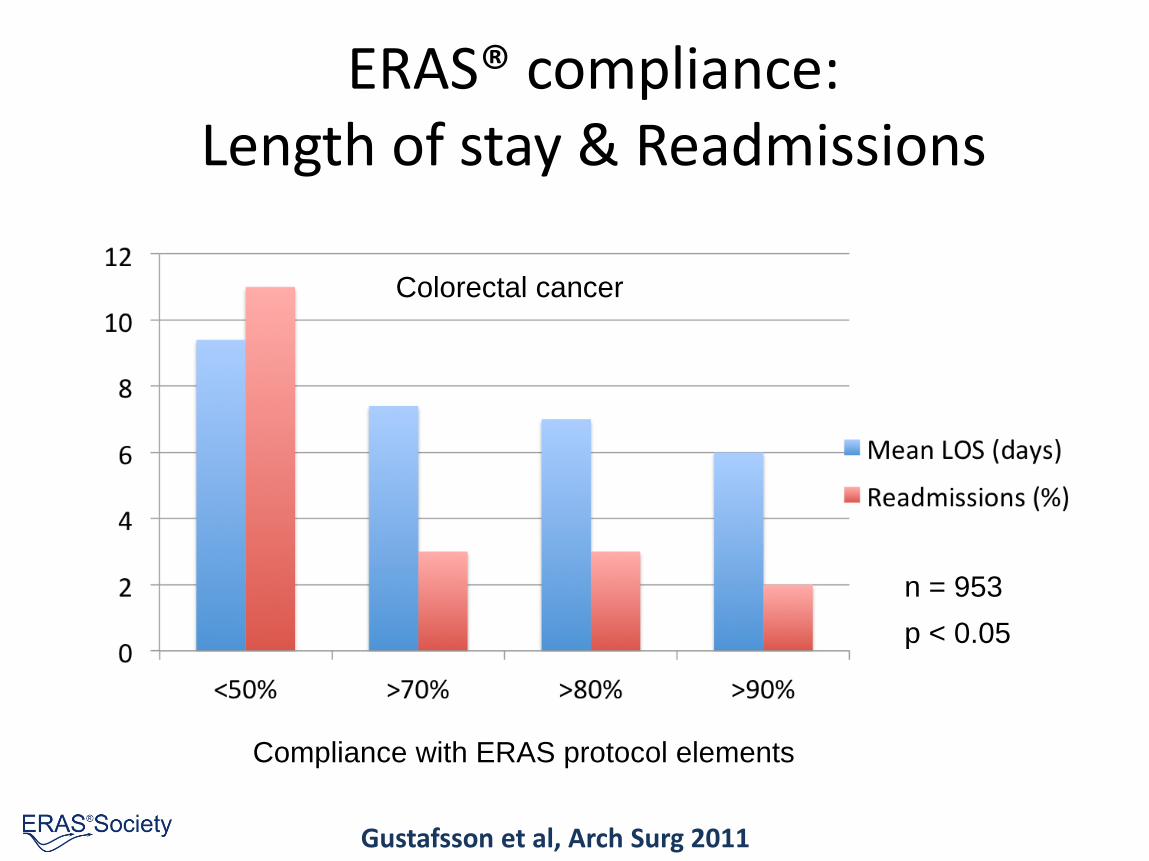
ERAS® compliance:Length of stay & Readmissions
Gustafsson et al, Arch Surg 2011
n = 953
p < 0.05
Compliance with ERAS protocol elements
Colorectal cancer
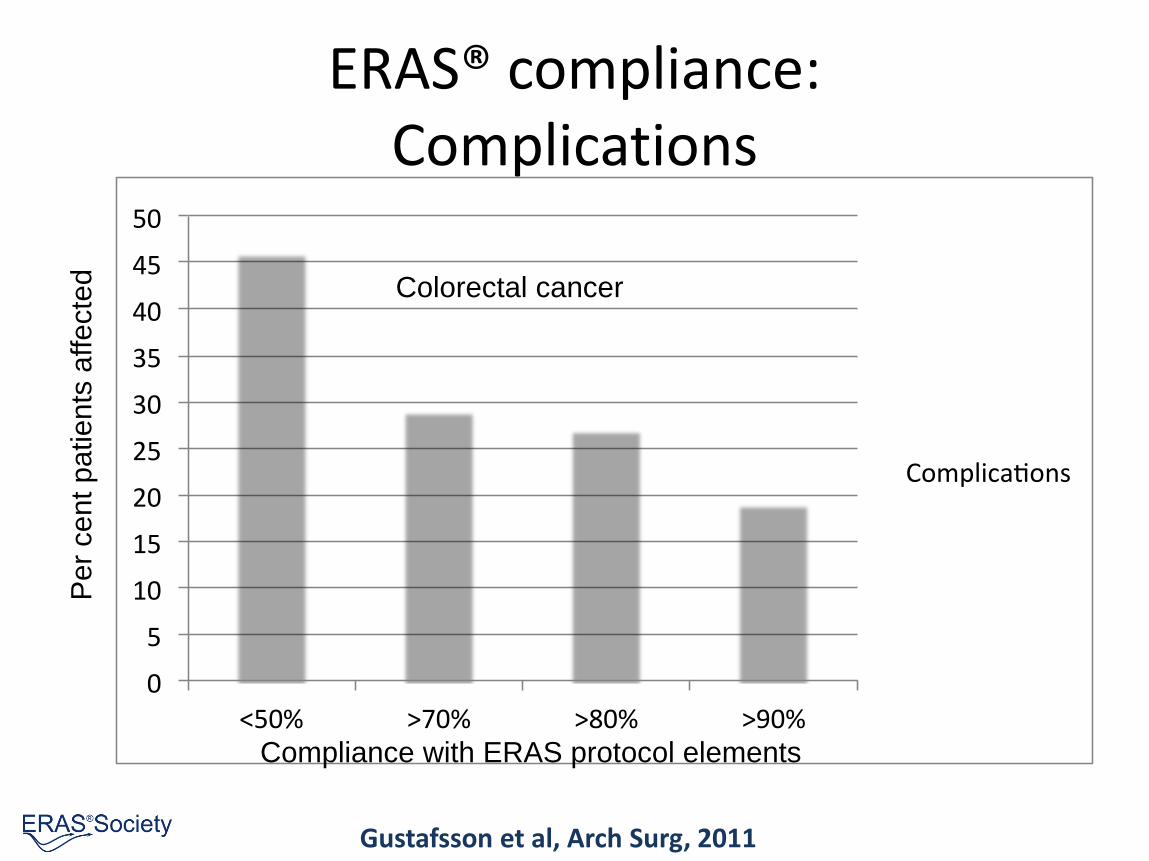
ERAS® compliance:Complications
Gustafsson et al, Arch Surg, 2011
n = 953
p < 0.05
0
5
10
15
20
25
30
35
40
45
50
<50% >70% >80% >90%
Complica ons
Compliance with ERAS protocol elements
Pe
r ce
nt
pa
tie
nts
affe
cte
d Colorectal cancer
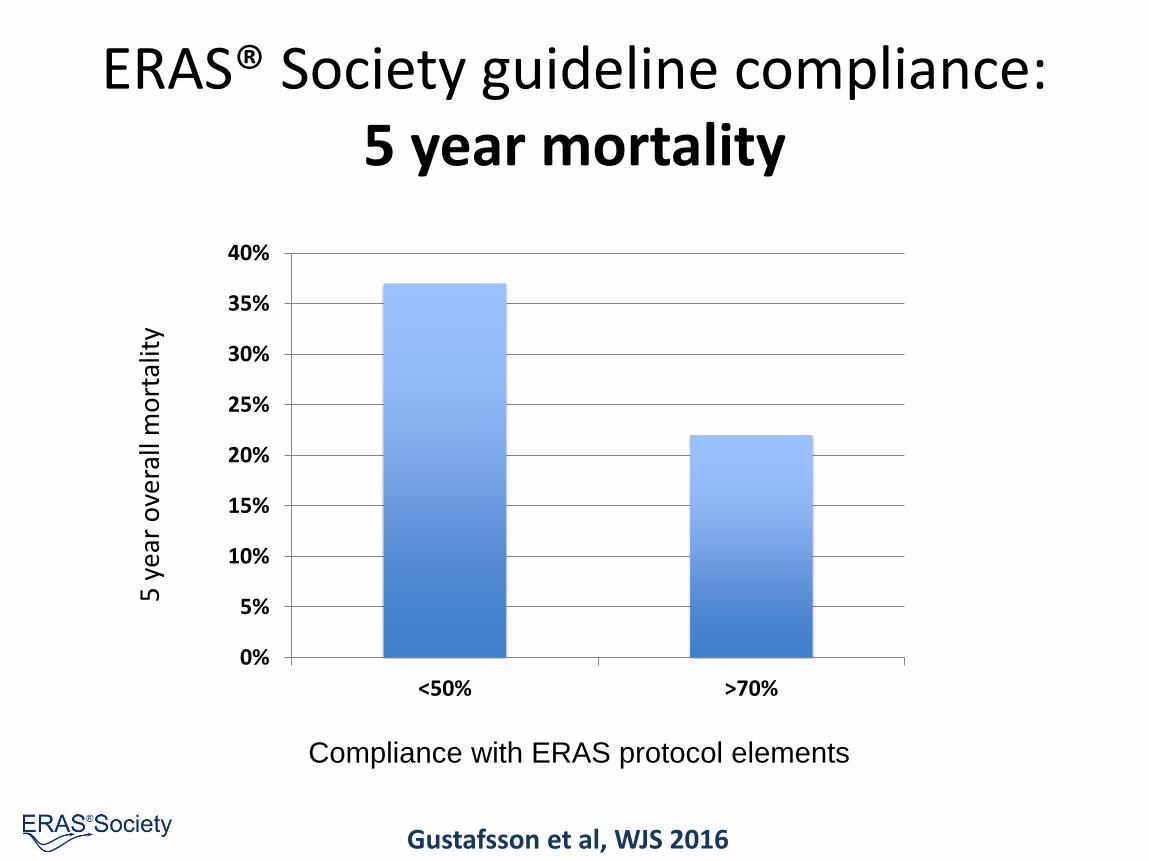
ERAS® Society guideline compliance:5 year mortality
Compliance with ERAS protocol elements
5 y
ear
ove
rall
mo
rtal
ity
0%
5%
10%
15%
20%
25%
30%
35%
40%
<50% >70%
Gustafsson et al, WJS 2016
ERAS® Society basics
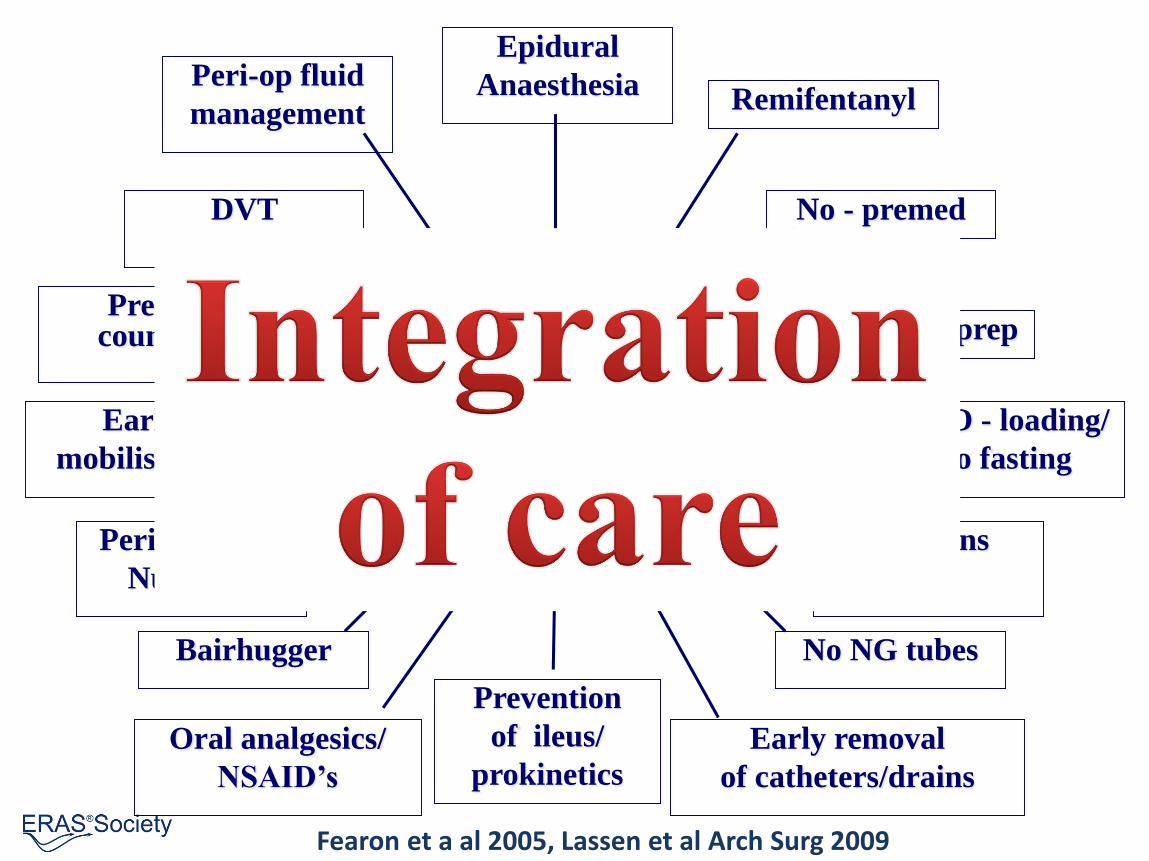
ERAS
Epidural
Anaesthesia
Prevention
of ileus/
prokinetics
CHO - loading/
no fasting
Early
mobilisation
Peri-op fluid
management
DVT
prophylaxis
Pre-op councelling
Remifentanyl
No - premed
No bowel prep
Perioperative
Nutrition
Bairhugger
Oral analgesics/
NSAID’s
Incisions
No NG tubes
Early removal
of catheters/drains
Fearon et a al 2005, Lassen et al Arch Surg 2009

Local Leadership Team
Anaesthesiologist Surgeon ERAS Coordinating Nurse
ERAS team approach
• Surgeon
• Anesthestist
• HDU specialist
• Ward nurses
• Anesthesia nurses
• Physiotherapist
• Dietitian
• Management
Team work:
• Training
• Implementing
• Planning
• Auditing
• Updating
• Reporting
• Research
ERAS® Society network
700,000,000 users
ERAS® Interactive Audit System
• Implementation tool
– Help units implement ERAS and get full control
• Quality registry
– Continuous results updated, benchmarking
• Research tool
– Tailored for Audit research and PRCTs
• Updating tool
– New treatments – all users get it via the system
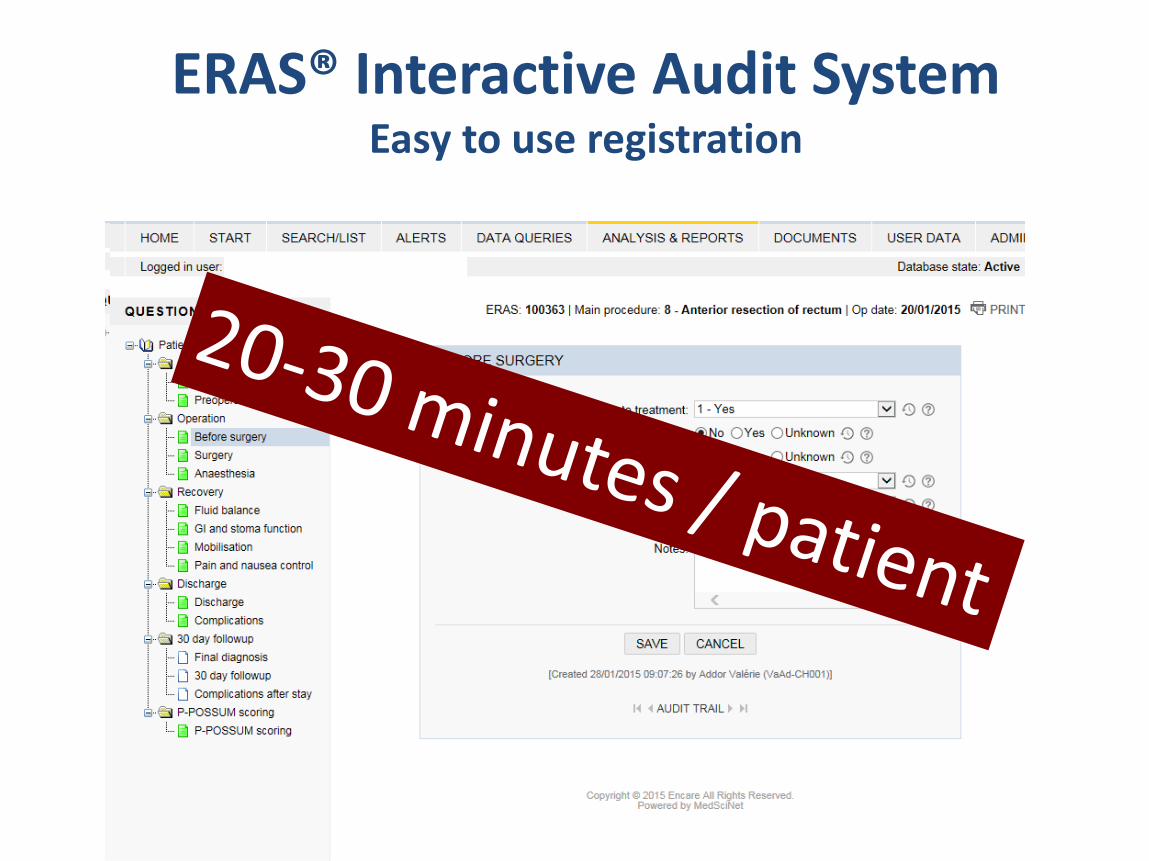
ERAS® Interactive Audit System Easy to use registration
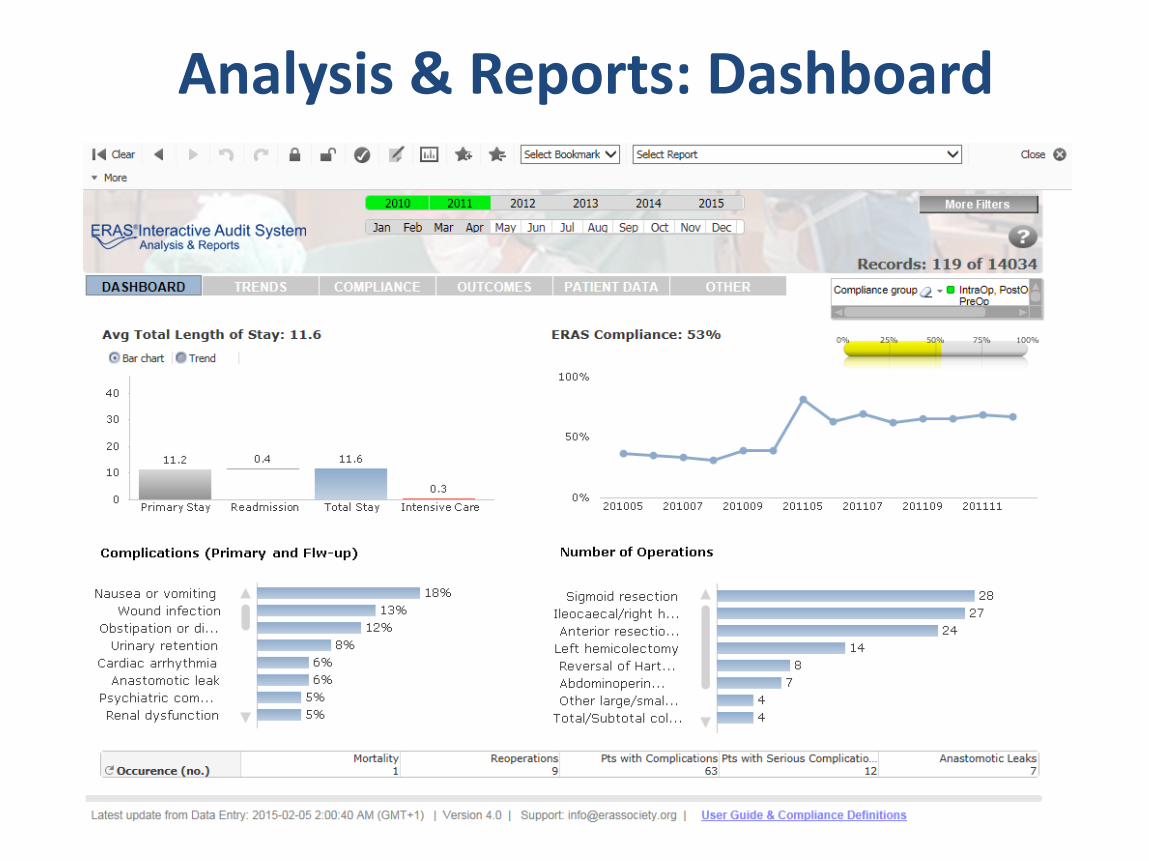
Analysis & Reports: Dashboard
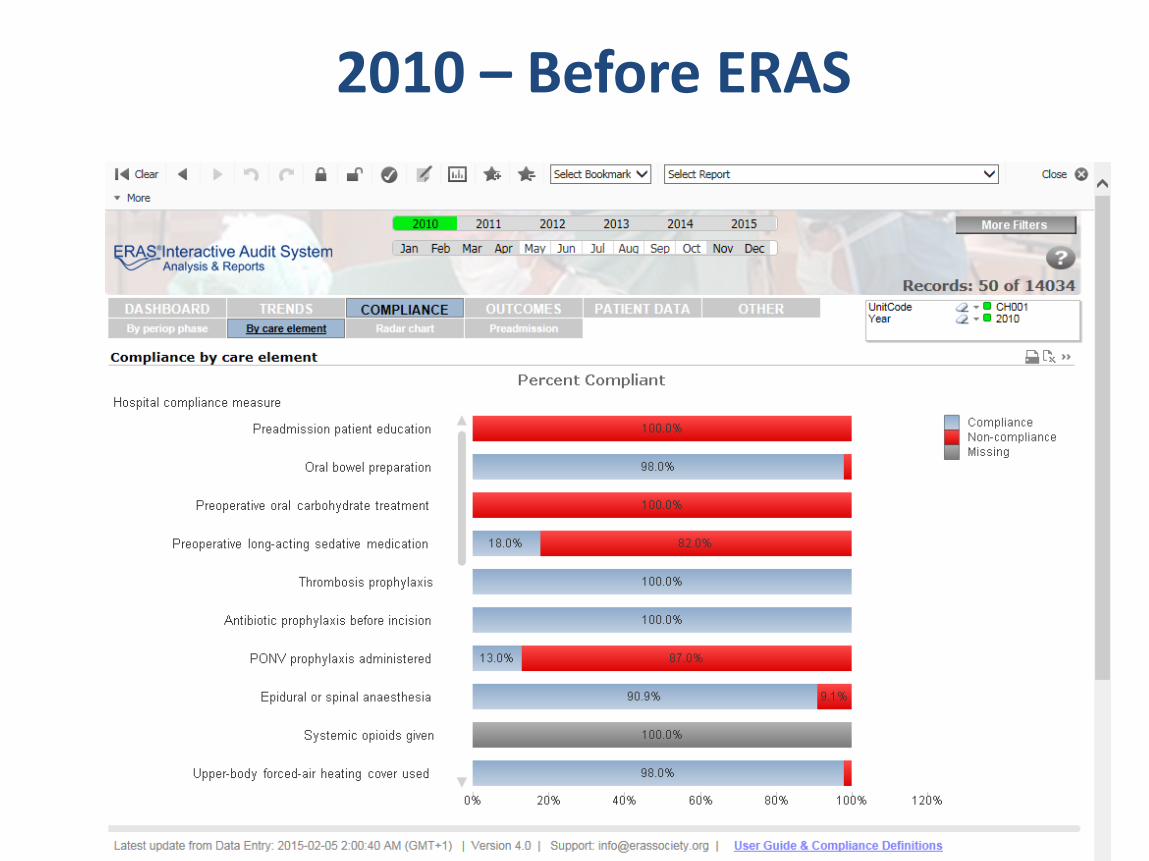
2010 – Before ERAS
62
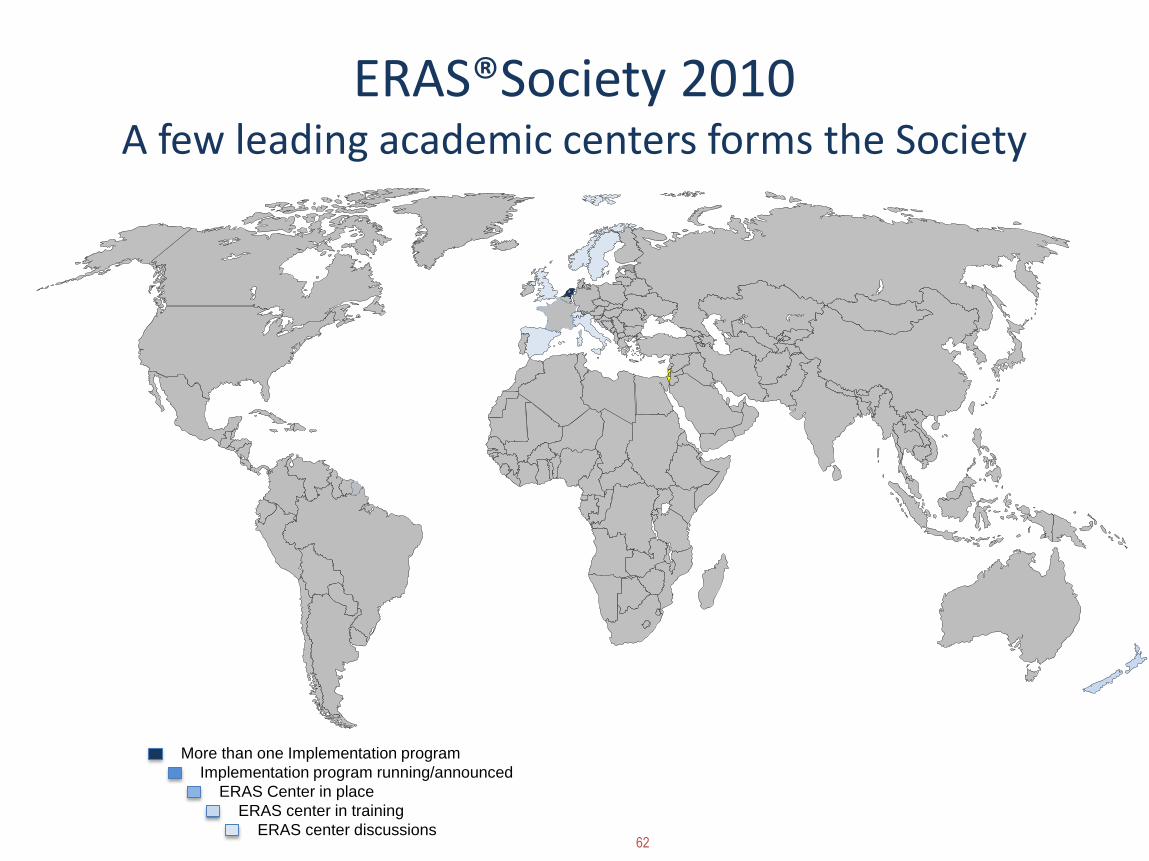
ERAS®Society 2010A few leading academic centers forms the Society
More than one Implementation program
ERAS Center in place
ERAS center discussions
Implementation program running/announced
ERAS center in training
63
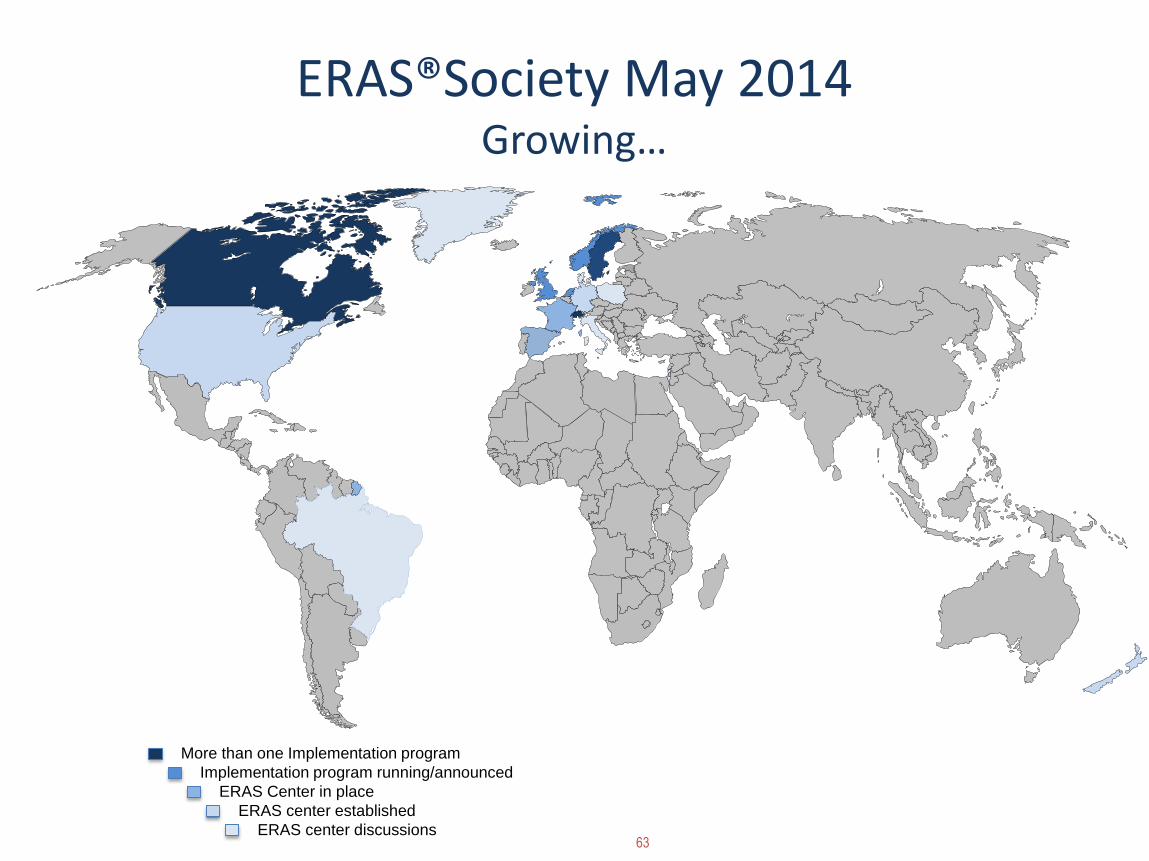
ERAS®Society May 2014Growing…
More than one Implementation program
Implementation program running/announced
ERAS Center in place
ERAS center established
ERAS center discussions
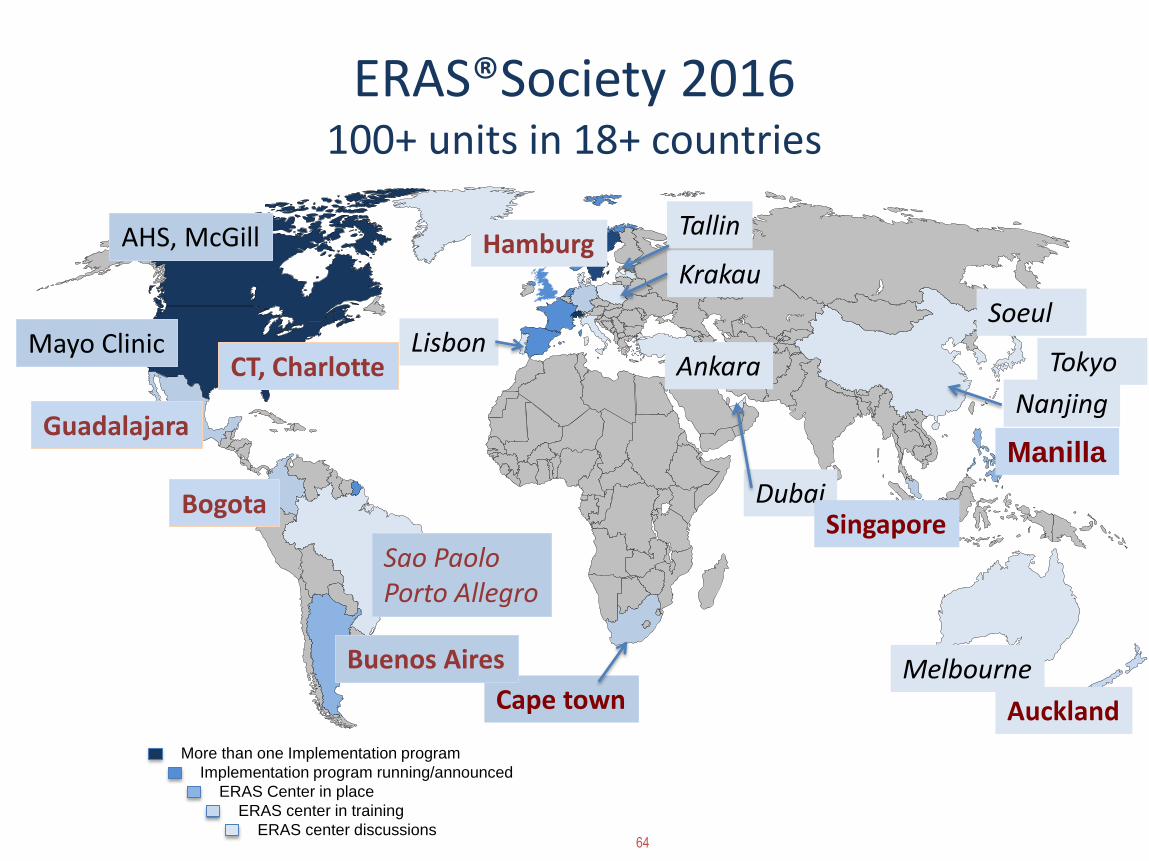
64
ERAS®Society 2016100+ units in 18+ countries
More than one Implementation program
Implementation program running/announced
ERAS Center in place
ERAS center in training
ERAS center discussions
Manilla
DubaiSingapore
Guadalajara
Bogota
LisbonTokyo
Nanjing
Melbourne
Krakau
Cape town
Buenos Aires
Auckland
Mayo Clinic
AHS, McGill Hamburg
CT, Charlotte
Soeul
Sao PaoloPorto Allegro
Ankara
Tallin
Health Care Challenges
• Growing and ageing population
• Pressure for better results
• Diminishing funding
• Better care for less cost – Fast
Health Care Challenges & ERAS
• Growing and ageing population
• Pressure for better results
• Diminishing funding
• Better care for less cost – Fast
• Better care
• Saves costs
• Implement in 8-10 mo
Summary
• Best practice is not in use
• Multi professional & Multi disciplinary
• Systematic implementation
• Teams
• Interactive Audit
ERAS improves outcomes
Winners: Patients, staff, payers
Summary
Best practice is not in use
Perioperative care is complex and important
Multi professional & Multi disciplinary apporach necessary
Systematic implementation in teams
Interactive Audit is a useful tool
ERAS improves outcomes
Winners: Patients, staff, payers


MODERATEDPANEL Q&A

OPEN FLOOR Q&A

THANK YOU FOR JOINING US!
MODERATOR QUESTIONS FOR PANEL Q&A**(THIS SLIDE WILL NOT BE PROJECTED FOR AUDIENCE)**
We have a number of healthcare provider executives in the audience with us today. What advice do you have for them as they navigate the shift from traditional fee-for-service models to value-based models, and have to show results in each area? (for all)
Integrated practice units sound lovely, but I don’t see many where I can get my care. Is this an idealistic notion, or are they really developing? (for Olle)
Who really uses outcomes data – patients who want to function like consumers, or providers? (for Christina)
What does a transformation from vendor to partner in outcomes measurement and accountability look like/require from medical technology company? How does Medtronic concretely contribute to VBHC going forward? (for Rob)
Our ability to access and use data effectively is key to improving outcomes. Can we solve our data challenges through registries? What other solutions would help? (for Christina)
Should outcomes – and our expectations for outcomes – change across different cultures and countries? (for Christina, then all)
A lot of the work to optimize for improving outcomes involves new models and processes for efficiency. Where does innovation come from in this environment, and is there room for breakthrough innovation? ( for Rob, then all)
What’s your impression about the availability of audits in general today? Are there organizations out there auditing effectively? (for Olle)
What are the key success factors for implementing VBHC in a hospital today (for All)
With respect to improving outcomes, our panelists have shared some examples of success. What are some other pockets of success in other parts of the world that we might replicate here in Europe? (for All)





























