Embed Size (px)
Citation preview

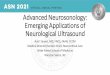
analysis. This calculation can be explained by the followingexample: An observer is asked to analyze the male voicesof a choir. At timepoints 1, 2, and 3 seconds, he is asked tomark on a diagram how loud he can hear the tenor, ba-ritone, and bass. At time points 1 and 2, the tenor is theloudest, the baritone is moderately loud, and the bass isthe quietest. At time point 3, the tenor is silent while thebass is loudest (Fig. A1.9). Applying this to Doppler fre-quencies, a large Doppler shift translates into high flowvelocity and a small Doppler shift translates into a low flowvelocity, while the volume depends on the number ofreflectors, moving with a given flow velocity. In our exam-ple (Fig. A1.10), most erythrocytes are flowing fast, amod-erate number are slower, and a small number are veryslow, which is usually the case in regions with a laminarflow pattern.Extension of frequency step numbers of timepoints per
second leads to a typical Doppler spectrum (Fig. A1.11).The exact number of frequency steps varies from64 to 256depending on the Doppler or duplex ultrasound systembeing used.
Doppler Shift and Flow Velocity
To transfer the Doppler shift (= a frequency in kHz) intoflow velocities (cm/s or m/s) the Doppler formula needs tobe applied (Equation A1.1). As the formula includes thecosine of the insonation angle, exact flow velocity can onlybe calculated if the ultrasound beam is directly in linewiththe direction of blood flow in the vessel segment beinganalyzed (cosine of 0° insonation angle = 1). Therefore,
1 Flow and Ultrasound Basics4
440 Hz
447 Hz?
440 Hz
330 m/s
330 m/s
5 m/s
Fig. A1.6 Example of the Doppler effect occurring within the rangeof the audible sound. An observer evaluates the sound emitted by atuning fork. Top: The observer stands still. The emitted frequency isidentical to the received frequency. Bottom: The observer is movingtoward the acoustic source, therefore passing more quickly throughthe sound waves resulting in a subjectively higher received fre-quency.
Movingacousticsource
Tympanicmembrane
Inner ear and centralnervous system
Middle ear
Acoustic Doppler shift analysis
Fig. A1.7 Schematic drawing of the human auditory apparatus andits ability to detect a frequency shift of a moving acoustic source.
Demodulator(f*– f)
Discriminatorof flow direction
Frequency analysisFourier analysis Speaker
AmplifierEmitter (f)
Receiver (f*)
Ultrasound Doppler shift analysis
Fig. A1.8 Schematic drawing demonstrating the analogy of a diag-nostic ultrasound machine to the human auditory system.
Tenor
(Frequency)
Baritone
Bass
1
Loud Medium Low
2 3 (Time)
Fig. A1.9 Explanation of Fourier analysis with the example of a choir.A frequency analysis is performed over time. At defined timepointsthe song is analyzed and documented in colored boxes according tothe active singers (= frequencies) and to the strength at which theysing, i. e., point 1 depicts the moment when the tenor is loudest, thebaritone sings at moderate volume and the bass has the weakestsound.
aus: Valdueza u.a., Neurosonology and Neuroimaging of Stroke (ISBN 9783131418715) © 2008 Georg Thieme Verlag KG

whenever the angle is greater than 0° the calculated ve-locitywill be “false low.”As blood vessels hardly ever pointdirectly toward the ultrasound transducer, an acceptableflow velocity can only be calculated if the insonation angleis less than 30° (error from real Doppler shift is ≥13%) orthe insonation angle is known and corrected for(Fig. A1.12).
The reflected ultrasound waves contain a spectrum offrequencies. From these, several diagnostically relevanthemodynamic parameters are generally automaticallycalculated by modern ultrasound machines, providedthat a correct envelope curve has been fitted (Fig. A1.13)(for further details about hemodynamic parameters, seealso Chapter 3, “Parameters of Cerebral Hemodynamics,”p. 60).
Ultrasound Principles 5
Fast
(Velocity = frequency)
Medium
Slow
1
many
Number of reflectors:
medium few
2 3 (Time)
Fig. A1.10 Fourier analysis of ultrasound-generated Doppler sig-nals: Transferring the example of the choir to blood flow analysis.The detected frequencies now resemble the detected Doppler shift,the loudness results from the number of reflectors generating anequal Doppler shift.
Fig. A1.11 The Doppler spectrum of a transcranial (TCD) ultrasoundsystem. Note the “systolic window,” i. e., in laminar flow most eryth-rocytes are fast flowing, therefore the highest intensities (orangecolored) are close to the highest flow velocities. Intensity near thezero line is low as only few erythrocytes are slow.
Angle
0
10
20
30
45
90
Doppler shift(%)
100
98
94
87
71
0
Error(%)
0
2
6
13
29
100
Fig. A1.12 Relation of insonation angle and error in Doppler shiftdetermination.
v = Flow velocityc = Velocity of sound within the tissuef = Emitted frequencyf* = Received frequencyf – f* = Doppler shiftα = Insonation anglecos = Cosine
( )-=
ac f* f
v2f cos
α < 20°
( )-=
c f* fv
2f
Equation A1.1
aus: Valdueza u.a., Neurosonology and Neuroimaging of Stroke (ISBN 9783131418715) © 2008 Georg Thieme Verlag KG

Flow Profile Alterations—Spectral BroadeningDoppler spectrumanalysis of normal blood flow classicallyreveals a laminar flow characterized by a systolic window,whichmeans that its highest velocity is in the center of thevessel and the lowest at its wall. In case of medium- tohigh-grade stenosis the laminar flow changes to turbu-lent—in that only few erythrocytes flow very fast, themajority are slow and nonlinear, resulting in raised Dopp-ler spectrum intensities near the zero line (Fig. A5.19). Invery high-grade stenosis a harmonic phenomenon, the so-called musical murmur, can be observed. Acoustically itresembles a bird cry and is therefore also frequently calledthe “sea gull cry” or “goose cry.” In the Doppler spectrum,mirror-image parallel strings or bands can be observed(see Fig. A5.20 and video). The phenomenon presumablyresults fromharmonic frequencies, generated fromregularvibrations of the vessel walls caused by the increasedblood flow velocities. Musical murmurs may be found inextra- and intracranial stenosis. A recent study that re-ported on 66 musical murmurs found 94% of murmursoccurred in intracranial and 6% in extracranial vessels (Linet al. 2006). In 88% of cases a severe, high-grade stenosiswas detected. In the remaining cases, the musical murmurwas found mainly in the communicating intracranial ar-teries. Hereby the musical murmur indicates a “functionalstenosis,” when blood flow is too high for the size of theACoA or PCoA. As a rule of thumb it can be postulated thatwhenever a musical murmur is detected intracranially,and even if the maximal flow velocities are not clearlyraised, a high-grade stenosis or proximal stenoocclusiveprocess has to be present.Both of the above criteria, spectral broadening and mu-
sical murmurs, however, are additional and not exclusivecriteria for stenosis. They depend on the grade as well asthe configuration of the stenosis and are not mandatory.
Indirect Hemodynamic Assessment
In any case of a suspected or known stenosis not only theintrastenotic flow profile but also the flow profiles fromvessel segments proximal and distal to a stenosis (preste-notic and poststenotic flow signal) have to be analyzed.This allows distinguishing between stenoses with or with-out a relevant hemodynamic effect. Proximal or distal flowalterations are only seen in hemodynamically relevantstenoses (Fig. A5.21). Stenoses are hemodynamically rele-vant if they cause a reduced blood volume flow and post-stenotic pressure drop. According to a mathematicalmodel calculation applied to the ICA by Spencer and Reid(1979) this occurs if the diameter is decreased by morethan 80% or the cross-sectional area is reduced by 90–95%(Fig. A5.17). Archie and Feldtman (1981) found similarresults, suggesting a beginning of relevant blood flowreduction of 40% from 75% diameter stenosis or 94%area stenosis onward. The Spencer curve (Fig. A5.17) canbe considered as a guide to study hemodynamic conse-quences in stenoses. As it refers to a circumscribed and
5 Vascular Pathology84
Fig. A5.18 Doppler spectra, obtained from follow-up transcranialinsonation of the MCA in a patient with severe hypoxia. A Normalblood flow. B Hyperemia. Note the increased flow velocities as wellas the reduced pulsatility. C Reduced blood flow (hypoemia). Notethe reduced flow velocity as well as the increased pulsatility.
Fig. A5.19 Top: Schematic drawing of flow pattern in a normal and astenosed blood vessel. Bottom: Corresponding Doppler spectra.Note the preserved systolic window in the unaffected vessel andthe turbulent flow with spectral broadening and increased velocitywithin the stenosis.
Fig. A5.20 TCD Doppler spectrum of a high-grade stenosis (systolicflow velocity > 300 cm/s). Note the mirror-image parallel strings asthe visual correlate of a musical murmur.
aus: Valdueza u.a., Neurosonology and Neuroimaging of Stroke (ISBN 9783131418715) © 2008 Georg Thieme Verlag KG

symmetric stenosis without sinus dilatation however, themodel can only be transferred with caution to real ICAstenoses which are frequently axis-asymmetric, of varia-ble length, and of different distal resistance depending onthe presence of collaterals. Considering waveform appear-ance together with flow velocities will therefore help torecognize a hemodynamically relevant stenosis.Unfortunately, the terminology of the pre- and postste-
notic flow signals is notwell standardized. In this book, weuse the terms pre- and poststenotic flow pattern for de-tectable proximal or distal flow signal alterations.The prestenotic flow pattern comprises amostly normal
systolic flow velocity and always a normal rise in systolicflow. However, the distal flow obstruction leads to raisedperipheral resistance, reduced prestenotic diastolic flow,and subsequently raised pulsatility. In cases with unclearcause of the distal flow obstruction (occlusion or stenosis)but highly pulsatile flow signals, the term high-resistanceflowwith increased pulsatilitymight bemore appropriate.A poststenotic flow pattern requires a relevant proximal
obstruction, which then leads to the phenomenon of adelayed systolic rise. For exact assessment of a postste-notic flow pattern, clearly the insonation has to be per-formed outside of the stenosis. The compromised bloodflow results in a compensatory dilatation of the resistancevessels to avoid downstream hypoperfusion. This resultsin a rising total arterial cross-sectional area with subse-quent reduction of the peripheral resistance causing araised diastolic flow component and reduced pulsatility.For these flow patterns, terms such as “blunted flow,” “lowresistance flow,” or, in case of distinct alterations, “venous-like flow” have been used. A delayed systolic flow rise andreduced velocity may coexist. However, one or the othermay also be the dominating feature of the Doppler spec-trum alteration. The term poststenotic flow pattern can begenerally used in proximal stenosis and occlusion as theremaining distal flow is never postocclusive but always aresult of an upstream functional stenosis, i. e., in a collat-eral. The only relevant differential diagnoses of a postste-notic flow pattern are low-resistance flow patterns inAVMs (which, however, are usually associated with raisedand not reduced flow velocities) and general low-resis-tance flow patterns in all brain-supplying arteries, forexample, in those caused by severe aortic valve stenosis.To reach the greatest diagnostic certainty during every-
day clinical practice, we recommend that signals should beobtained from all three vessel segments (i. e., prestenotic,intrastenotic, and poststenotic) when possible. The abovecriteria are of special help when performing serial mea-surements over long periods to detect disease progression.For instance, if initially absent indirect hemodynamic cri-teria develop over time, an increase of the stenosis to arange of at least 80% is likely. Follow-up assessment of anextracranial low-grade progressive stenosis <50% is moredifficult.We recommend considering a lumen reduction ofat least 10% as sign of progression. In stenoses >50% untilindirect hemodynamic signs are present, an increase of
peak systolic velocity > 50 cm/s should be considered asprogress, only if good insonation conditions are presentand angle correction can performed without difficulties.
Ultrasound Criteria of Occlusions
Direct Morphologic Assessment
Extracranial B-mode duplex ultrasound may reveal com-plete filling of the vessel lumen with thrombotic materialof varying echogenicity. In chronic occlusion, precise ves-sel identification and differentiation of the vessel lumenmight be difficult, a fresh thrombotic occlusion usuallypresents with hypoechogenic thrombotic material. B-mode insonation alone however is not sufficient for diag-nosis of occlusion. It should always be combined withcolor-mode and Doppler spectrum analysis.
Direct Hemodynamic Assessment
Occlusions result in a complete absence of color-flow sig-nal, even after adjustment for very low flow signals (low-est pulse repetition frequency and increased color-gainsettings). Doppler spectrum analysis reveals a small stumpsignal near the zero line but no flow signals. In caseswith aproximal vessel stump, a distinctly reduced, alternatingflow pattern with a short systolic peak and a small retro-grade flow component (“to-and-fro signal”) can be found.Diagnostic certainty may be increased by using intrave-nously applied ultrasound contrast agents. On transcranialinsonation, a missing flow signal does not necessarily im-ply occlusion. For example, P1-PCA segment might beabsent due to P1 hypo- or aplasia in case of a fetal-typePCA. Also, the A1-ACA segment might be missing in dis-
Stenoses and Occlusions 85
Fig. A5.21 Left: Schematic drawing of severe extracranial ICAstenosis. Right: Extracranial duplex, longitudinal view. Doppler spec-trum analysis proximal, within and distal to a hemodynamicallyrelevant high-grade 90 % ICA stenosis. CCA flow velocity: 38/12 cm/s. ICA flow velocity within the stenosis was 360/105 cm/sand distal from the stenosis was 36/10 cm/s. Note the reducedpulsatility in the prestenotic CCA and the distinctly delayed systolicflow rise in the poststenotic ICA.
aus: Valdueza u.a., Neurosonology and Neuroimaging of Stroke (ISBN 9783131418715) © 2008 Georg Thieme Verlag KG

VA—Occlusion
The analysis of VA occlusions requires specific knowledgeto avoid diagnostic errors. As in the diagnosis of ICA oc-clusion, an occluded vessel might be depicted by color-mode sonography with an absent color signal (Fig. A5.34).Within the V2-VA segment the usually preserved bloodflow of the concomitant vertebral vein might be of diag-nostic aid (Fig. A5.35).In contrast with the extracranial ICA which does not
show secondary filling from extracranial collaterals, theVA has numerous extracranial anastomoses at all levels ofits extracranial course which can potentially serve as col-
laterals and prevent occlusion over its entire length. Theseare anastomoses from the thyrocervical trunk andbranches of the ECA, especially from the occipital artery.In case of a proximal VA occlusion, they may lead to asecondary VA filling, resulting in a “postocclusional” VAflow, which might then be detected within the distal VAsegments (Figs A5.36, A5.37). Because of the bilateral VAcomposition, the above collateral pathways are rarely ofimportance as the contralateral VA will provide the bloodsupply to the posterior circulation and also retrogradely tothe affected VA in most cases. However, in case of con-tralateral VA hypoplasia or when the contralateral VA ter-minates as the PICA, the extracranial anastomoses are in-deed of relevance and the distal VA flow profile may thenbe orthograde with a typical poststenotic flow pattern.Although the term “poststenotic” seems slightly inaccu-rate in a vessel segment distal to an occlusion, we wouldsuggest its use nevertheless, as it clearly illustrates thecommon problem of hemodynamic impairment in steno-ses and occlusions. A distal extracranial VA occlusion maycause a stump signal or a high pulsatile flow signal withalmost absent end-diastolic flow component (Fig. A5.38).In a recently published study including 10 VA occlusionsproximal to the origin of the PICA, all subjects presented adiastolic zero flow (Saito et al. 2004). Because of the highvariability of distal collateral filling, it has to be empha-sized that the term “VA occlusion” alone is not sufficientbut has to be complemented by the exact location of theocclusion and the information about possible secondaryVA filling by collaterals distal to the occlusion. For furtherdetails, see Case 19 (p. 245).
5 Vascular Pathology92
Fig. A5.34 Extracranial duplex, longitudinal plane: V0/V1-occlusion.A absent color filling and absent Doppler spectrum in the V0-VAsegment. B Normal color signal and Doppler spectrum of the SA.
Fig. A5.35 A DSA, selective SA filling, posteroanterior view: Prox-imal VA-occlusion (arrow). B–D Extracranial duplex, V2-VA seg-ment. B B-mode image: Typical image constellation with the bilat-eral acoustic shadowing from the transverse processus and thehypoechogenic transverse signal of the VA in between. Dashedline: Estimated VA diameter. C Color-mode image demonstrates amissing flow signal within the occluded VA but a preserved flowsignal in the vertebral vein. Long and short dashed lines: Estimatedand real diameter of the VA, respectively.D Doppler spectrum of thevertebral vein.
Fig. A5.36 Left: DSA, selective thyrocervical trunk filling, LAO view.Proximal VA occlusion. Secondary, segmental collateral filling of theV2- and V3-VA segments from numerous muscle anastomoses. 1–3Extracranial duplex, longitudinal plane. 1 V2-VA with minimal flow;2Muscle branch anastomosis (flow velocity: 25/10 cm/s); 3 Postste-notic flow pattern with reduced flow in the postocclusive V3-VA(flow velocity: 16/5 cm/s).
aus: Valdueza u.a., Neurosonology and Neuroimaging of Stroke (ISBN 9783131418715) © 2008 Georg Thieme Verlag KG

SA—Proximal Stenosis and Occlusion
Direct signs of a hemodynamically relevant SA stenosis>50% are, as in all other arteries raised flow velocitiesand a turbulent flow, which is often difficult to directlyassess. In stenoses > 70–80% and in proximal SA occlusionindirect hemodynamic signsmight be observedwithin thedependent axillary, brachial, and radial arteries. Thesevessels then show a poststenotic flow profile, i. e., a de-
layed systolic flow rise, reduced flow velocities as well as achange of the typical triphasic flow profile to a bi- ormonophasic flow signal. A characteristic and pathogno-monic sign of proximal high-grade SA stenosis or occlusionis a flow alteration within the ipsilateral VA, which mayserve as a collateral for the blood supply of the arm—whichis then called subclavian steal phenomenon (Figs A5.39,A5.40). Depending on the grade of SA stenosis a reduced
Extracranial Pathology 93
Fig. A5.37 Left: DSA, selective right VA filling, posteroanterior view.Occlusion of the left proximal VA and the right VA ending as theposterior inferior cerebellar artery. Secondary segmental collateralfilling of the left VA via numerous segmental spinal anastomosesfrom the right VA. 1–3 Extracranial duplex, longitudinal plane. 1Proximal left V2-VA (flow velocity: 18/9 cm/s); 2Mid left V2-VA (flowvelocity: 22/10 cm/s); 3Distal left V2-VA (flow velocity: 27/10 cm/s).Note the improving flow in distal segments with increasing numberof collaterals.
Fig. A5.38 Left: DSA, selective VA-filling, lateral view: V3-VA occlu-sion (arrow). Note the only outflow pathway via a small musclesupplying arterial branch. Right: Extracranial duplex of V2-VA withnormal diameter, longitudinal view: preserved color signal but highlypulsatile flow on Doppler spectrum analysis with small retrogradeflow component (flow velocity: 58/0 cm/s) indicating that this vesseldoes not participate in brain perfusion and strongly suggestive of VAocclusion distal of the PICA origin.
Fig. A5.39 Schematic drawing of the two main variants of collateralflow in case of a subclavian steal phenomenon. A Vertebrovertebraloverflow (regular type), B ICA-VA overflow (in cases with additionalcontralateral VA pathology). Furthermore, a few rare collateral var-iants have been described with conventional angiography which are,however, all difficult to assess with ultrasound.
Fig. A5.40 Subclavian steal syndrome in left proximal SA occlusion.Left: DSA, selective right VA filling, posteroanterior view. Vertebro-vertebral contrast overflow. Right: Doppler spectrum analysis. SA-R:Right SA with normal triphasic flow signal. V2-VA-R: Strong ortho-grade VA signal. V2-VA-L: Retrograde vertebral flow, which corre-sponds to a complete subclavian steal effect. SA-L: Monophasicpoststenotic distal SA signal.
aus: Valdueza u.a., Neurosonology and Neuroimaging of Stroke (ISBN 9783131418715) © 2008 Georg Thieme Verlag KG

Case 1Extracranial Internal Carotid Artery Stenosis
Clinical Presentation
A 60-year-old woman presented with three transient epi-sodes of right-sided loss of vision, each lasting a few mi-nutes, in the 2 days preceding her admission. There wereno further episodes of transient focal neurologic deficits.She had no vascular risk factors and was not on anti-platelet therapy. On admission, neurologic examinationincluding visual field and visual acuity was normal.
Initial Neuroradiologic Findings
There were no signs of ischemia on the initial computedtomography (CT) scan.
Suspected Diagnosis
Recurring right-sided amaurosis fugax.
Questions to Answer by UltrasoundTechniques
• Was there evidence of high-grade stenosis in the rightinternal carotid artery (ICA)?
• If so, what was the grade of stenosis?
Initial Neurosonologic Findings
Extracranial Duplex Sonography
B-mode sonography revealed no structural abnormality.The color-flow image of the right ICA demonstrated areduction in the lumen distal to the carotid bifurcationcaused by nonechogenicmaterial. Doppler spectrum anal-ysis in this area revealed a stenotic flow signal (flow veloc-ity: 288/116 cm/s). Cross-sectional insonation confirmedthe marked reduction of the vessel diameter. Distal ofthe stenosis the ICA Doppler spectrum demonstrated amild delayed systolic rise compared with the left side(flow velocity: 65/17 cm/s). Flow in the common carotidartery (CCA)was regular (flow velocity: 75/34 cm/s). Therewere no pathologic findings in the left ICA (Figs. B1.1–B1.6).
Transcranial Duplex Sonography
All detectable intracranial vessels including the OAs re-vealed normal and symmetric flow signals.
Conclusion
Right ICA stenosis of 70–80%, directly above the carotidbifurcation. The nonechogenic character of the stenoticmaterial was thought to be caused by either a smooth-surfaced “soft plaque” or a fresh, nonorganized intravas-cular thrombus.
Conventional Angiography
Digital subtraction angiography (DSA) demonstrated seg-mental narrowing of the superior aspect of the ICAwith anulcerated surface, directly above the bifurcation. The ex-tension of the stenotic segment was approximately 3 cm(Fig. B1.7). The degree of stenosis (local measurement)was estimated to be 80%. There were no pathologic find-ings in the distal ICA or the middle cerebral artery (MCA)on the affected side.
Clinical Course
Considering the three recurring transient retinal ischemicattacks and the ultrasound finding of a nonechogenicplaque, suggestive of a recent thrombus, the patient wasinitially treated with partial thromboplastin time (PTT)-guided heparinization instead of the usual treatment withantiplatelet drugs. A cardiac embolic source was consid-ered unlikely after transesophageal echocardiography and24-hour electrocardiogram (ECG) demonstrated normalfindings. Seven days after admission the patient under-went carotid endarterectomy (CEA). Intraoperatively, asoft plaque was removed, and there was no evidence of afresh thrombus. The operation and postoperative clinicalcourse were uneventful. No further ischemic attacks oc-curred, and the patient was prescribed clopidogrel forlong-term secondary stroke prevention.
128
aus: Valdueza u.a., Neurosonology and Neuroimaging of Stroke (ISBN 9783131418715) © 2008 Georg Thieme Verlag KG

Clinical Course
DegreeofNeurosonologicDifficulty:Low
129
Fig. B1.1 Extracranial duplex, longitudinal plane. Normal flow signalin the right CCA (flow velocity: 75/34 cm/s).
Fig. B1.2 Extracranial duplex, longitudinal plane. B-mode imagingof the right-sided carotid bifurcation including the right ICA appearsto be normal.
Fig. B1.3 Extracranial duplex, longitudinal plane. Color imaging ofthe same region as in Figure B1.2 demonstrates a marked segmen-tal narrowing.
Fig. B1.4 Extracranial duplex, transversal plane. Cross-sectionalimaging of the right ICA reveals the true diameter of the artery.
Fig. B1.5 Extracranial duplex, longitudinal plane. Right ICA withintrastenotic flow signal (flow velocity 288/116 cm/s).
Fig. B1.6 Extracranial duplex, longitudinal plane. Distal segment ofthe right ICA revealing a mild poststenotic flow pattern (flow veloc-ity: 65/17 cm/s).
aus: Valdueza u.a., Neurosonology and Neuroimaging of Stroke (ISBN 9783131418715) © 2008 Georg Thieme Verlag KG

Case 26Extracranial Vertebral Artery Dissecting Aneurysmfollowing Basilar Artery Stenting
Clinical Presentation
A 58-year-old man was admitted to an external hospitalwith right-sided sensorimotor hemisyndrome and dys-arthria. Several weeks earlier he had complained of tran-sient vertigo and a gait disorder. The patient had knownvascular risk factors of arterial hypertension, hypercholes-terolemia, and diabetes mellitus. On admission he pre-sented fluctuating symptoms with a moderate propor-tional hemiparesis, hemihypesthesia on the right side,and dysarthria (National Institute of Health Stroke Scale[NIHSS] score 7).
Initial Neuroradiologic Findings
The initial cerebral computed tomography (CT) scanshowed hypodensities in both cerebellar hemispheresand a small hypodense area in the right pons consistentwith subacute infarction (Fig. B26.1). Diffusion magneticresonance imaging (MRI) revealed moderate acute leftparamedian pontine ischemia (Fig. B26.2).
Suspected Diagnosis
Recurrent ischemia in the vertebrobasilar artery territorysuspicious of basilar artery (BA) stenosis or thrombosis.
Conventional Angiography
Digital subtraction angiography (DSA) demonstrated ahigh-grade stenosis in the middle segment of the BA. Thevertebral and carotid arteries were normal (Fig. B26.3).
Clinical Course (1)
In view of the remitting clinical symptoms, and the lesionson MRI, interventional percutaneous transluminal angio-plasty of the BA followed by stent implantation was per-formed via the left vertebral artery (VA). The procedurewas technically and clinically successful and a follow-upCT scan showed a patent BA without evidence of bleeding
or new ischemic lesions (Fig. B26.4). Secondary strokeprevention was commenced with aspirin and clopidogreland the patient was referred to a rehabilitation center. Bythis stage there had still not been any neurosonologicexamination.
Two weeks following the stenting, the patient had atransient ischemic attack (TIA) with double vision and aleft-sided hemiparesis that lasted a few hours. Further-more, the residual right-sided hemiparesis and the dys-arthriamildlyworsened. The patientwas then admitted toour department for the first time.
Questions to Answer by UltrasoundTechniques
• Was there restenosis or occlusion of the stented BA?• Was there evidence of an embolic source in the verte-
brobasilar system?
Initial Neurosonologic Findings (Day 1)
Extracranial Duplex Sonography
B-mode imaging of the carotid arteries showed moderateatherosclerotic vascular changes, more pronounced in thecarotid bifurcation. Doppler spectrum analysis demon-strated normal findings. The left VA showed a markedincrease in caliber in the V2-VA segment at the vertebrallevel between C5 and C6 with a maximal diameter of10.5mm in B-mode and color-mode imaging. The diame-ter of the V1-VA segmentwas 5.5mm. A constant diameterranging from4.3mmto 4.5mmwas seen in all segments ofthe right VA. The Doppler spectrumanalysis demonstratednormal flow signals in the left middle and distal V2-VAsegment as well as in the right V2-VA segment (Figs.B26.5–B26.10).
Transcranial Duplex Sonography
Transtemporal insonation yielded normal findings in theanterior (ACA),middle (MCA), and posterior (PCA) cerebralarteries on both sides. Transforaminal insonation demon-strated normal flow signals in the BA and the intracranialsegment of both VAs (not shown).
306
aus: Valdueza u.a., Neurosonology and Neuroimaging of Stroke (ISBN 9783131418715) © 2008 Georg Thieme Verlag KG

Conclusion
Suspected left VA dissectionwith formation of a dissectinganeurysm in the proximal V2-VA segment at the C5/C6level. There were no signs of detectable restenosis in thestented BA.
Cranial CT and CTA (Day 1)
Cranial CT confirmed the known cerebellar and pontineinfarctions. In addition, a new paramedian pontine infarctof moderate size was seen on the right side adjoining theBA stent (Fig. B26.11). Computed tomographic angiog-raphy (CTA) confirmed the widening of the left V2-VAsegment between C5 and C6 in terms of a VA dissectinganeurysm (Figs. B26.12, B26.13).
Clinical Course
The VA dissection was thought to be of iatrogenic origingenerated during the initial DSA with BA stent implanta-tion. The recent pontine infarction was attributed to astent-related secondary occlusion of a perforating artery.An embolic event, potentially originating from the aneu-rysm could not be excluded. Therefore, oral anticoagula-tionwith phenprocoumonwas started and the patientwasreferred again to a rehabilitation center. He was then lostto follow-up.
Final Diagnosis
Primary left-sided pontine infarction and old right-sidedpontine and cerebellar infarctions caused by BA stenosis ofunknown origin. Secondary right-sided pontine infarctionafter successful BA stenting either induced by secondaryocclusion of a pontine perforator artery within the stentedregion or by artery-to-artery embolism from V2-VA seg-ment dissecting aneurysm.
Final Diagnosis
Deg
ree
ofNeu
roso
nolo
gic
Difficu
lty:
Hig
h
307
Fig. B26.1 Unenhanced cranial CT, axial plane. Hypodensities in theright cerebellar hemisphere and a small right-sided hypodense areawithin the pons suggestive of subacute stroke (arrows). Note theenlarged and slightly hyperdense BA (arrowhead).
Fig. B26.2 MRI, apparent diffusion coefficient (ADC) map, axialplane. Acute left-sided paramedian pontine ischemic lesion (arrow).
aus: Valdueza u.a., Neurosonology and Neuroimaging of Stroke (ISBN 9783131418715) © 2008 Georg Thieme Verlag KG

Case 26 Extracranial Vertebral Artery Dissecting Aneurysm following Basilar Artery StentingDegreeof
NeurosonologicDifficulty:High
308
Fig. B26.3 DSA, left VA-injection, posteroanterior view. High-gradestenosis in the middle segment of the BA (arrow).
Fig. B26.4 Intracranial CTA, 3D-reconstruction. Patent BA afterstenting (arrows).
Fig. B26.5 Extracranial duplex, longitudinal plane (B-mode). LeftV1-VA diameter: 5.5 mm.
Fig. B26.6 Extracranial duplex, longitudinal plane (B-mode): LeftV2-VA dilatation between the transverse processes of C5 and C6with a diameter of 10.5 mm (encircled by arrows) suggestive ofdissecting aneurysm.
aus: Valdueza u.a., Neurosonology and Neuroimaging of Stroke (ISBN 9783131418715) © 2008 Georg Thieme Verlag KG

Final Diagnosis
Deg
ree
ofNeu
roso
nolo
gic
Difficu
lty:
Hig
h
309
Fig. B26.7 Extracranial duplex, longitudinal plane. Color-coded im-age of the dilated left V2-VA between C5 and C6 with a diameter of10.8mm.
Fig. B26.8 Extracranial duplex, longitudinal plane. Normal flow inthe distal left V2-VA between C3 and C4 (flow velocity: 49/17 cm/s).
Fig. B26.9 Extracranial duplex, longitudinal plane. Normal diameterof the right V2-VA segment (4.4mm).
Fig. B26.10 Extracranial duplex, longitudinal plane. Normal flow inthe right V2-VA (flow velocity: 43/13 cm/s).
Fig. B26.11 Unenhanced cranial CT, axial plane. New right-sidedhypodense area within the pons adjacent to the BA stent (arrow).Note the hyperdensity within the BA caused by the stent itself(arrowhead).
Fig. B26.12 CTA, curviplanar reformatted image, coronal view.Widening of the left V2-VA between C5 and C6 consistent withdissecting aneurysm (arrow).
aus: Valdueza u.a., Neurosonology and Neuroimaging of Stroke (ISBN 9783131418715) © 2008 Georg Thieme Verlag KG