Embed Size (px)
Citation preview

They aren’t the same thing
Daniel Dunham

Capnometry Displays the value (as a number) of the partial pressure
of CO2

Capnography Waveform capnography shows (as a wave) the change in
CO2 over time
Both are valuable, and both measure CO2, but they should be used for different things.

Why are we measuring end-tidal CO2? CO2 is a byproduct of aerobic metabolism CO2 is carried by the blood to be excreted by the lungs
Respiratory rate controls the amount of CO2 in the blood
End tidal CO2 can non-invasively reveal cardiac output, patient response to ventilation, and ETT placement confirmation and monitoring.
Capnometry In capnometry, the resultant value is directly
correlated to the blood CO2, HOWEVER, values may not match EtCO2 is closest to PaCO2 in healthy patients, when
cardiac function is not reduced In patients with reduced cardiac output, EtCO2 and
PaCO2 can be very different – For example, a patient in cardiac arrest (without chest compressions), EtCO2 will be very low or zero, but PaCO2 will be very high. This is because without cardiac output, blood will not be
flowing to bring CO2 to the lungs to allow them to exhale the CO2.
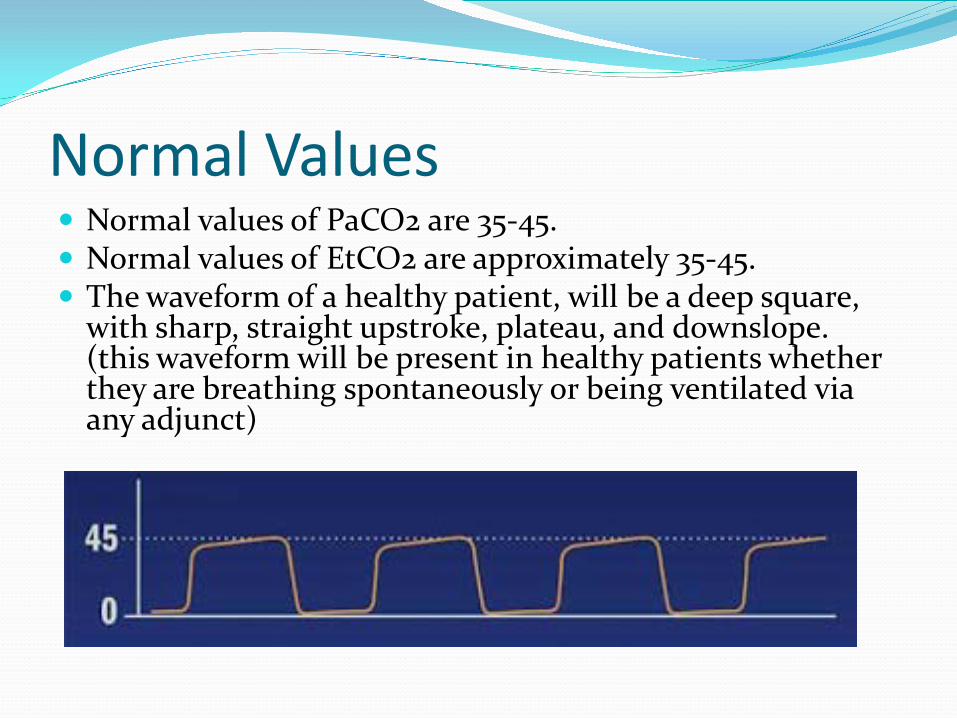
Normal Values Normal values of PaCO2 are 35-45. Normal values of EtCO2 are approximately 35-45. The waveform of a healthy patient, will be a deep square,
with sharp, straight upstroke, plateau, and downslope. (this waveform will be present in healthy patients whether they are breathing spontaneously or being ventilated via any adjunct)


Exhalation begins
CO2 does not increase immediately: the first air exhaled does not contain CO2 because of airway dead space.
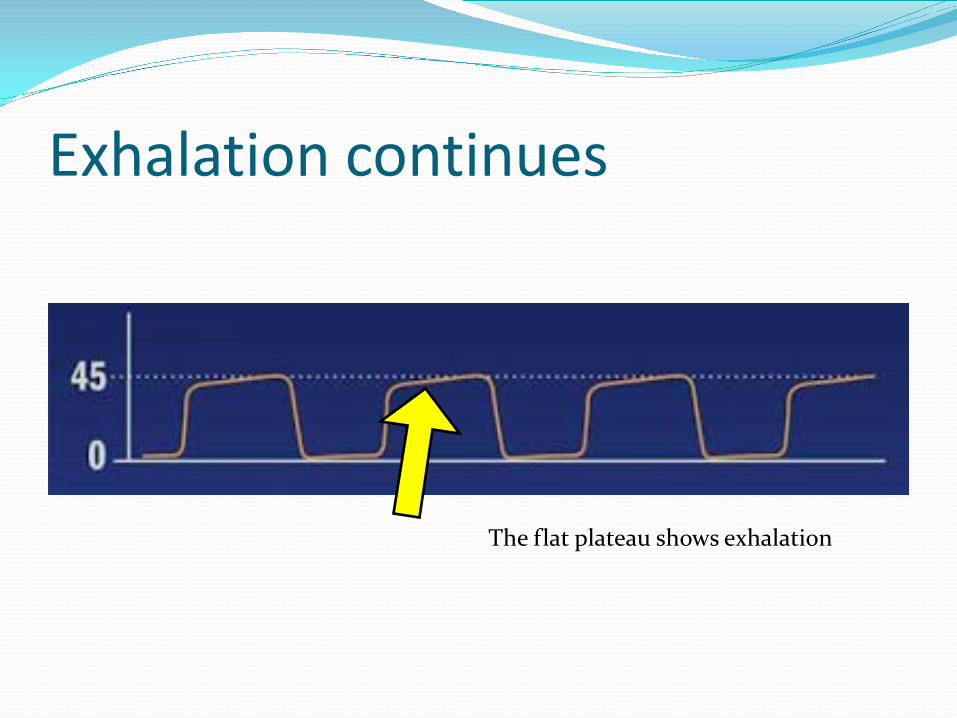
Exhalation continues
The flat plateau shows exhalation

Exhalation ends
Exhalation ends

No air movement, or inspiration
A value of zero indicates inspiration or no air movement

During Intubation Following intubation, waveform capnography is much
more valuable than numerical capnometry. A square waveform does not occur unless air exchange is
occurring in the lungs

Esophageal Intubation
This is what you can expect from an esophageal intubation. CO2 may be returned initially (due to CO2 that is already in the stomach), but it will rapidly taper off. A LOW CO2 READING IS CAUSE FOR CONCERN
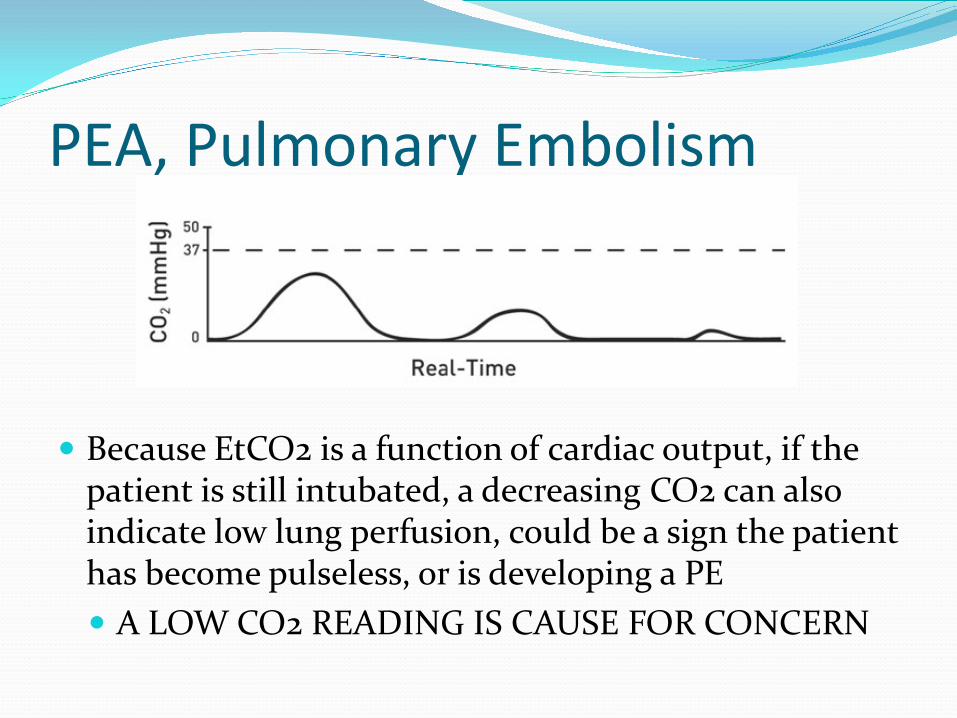
PEA, Pulmonary Embolism
Because EtCO2 is a function of cardiac output, if the patient is still intubated, a decreasing CO2 can also indicate low lung perfusion, could be a sign the patient has become pulseless, or is developing a PE A LOW CO2 READING IS CAUSE FOR CONCERN
Shark Fin
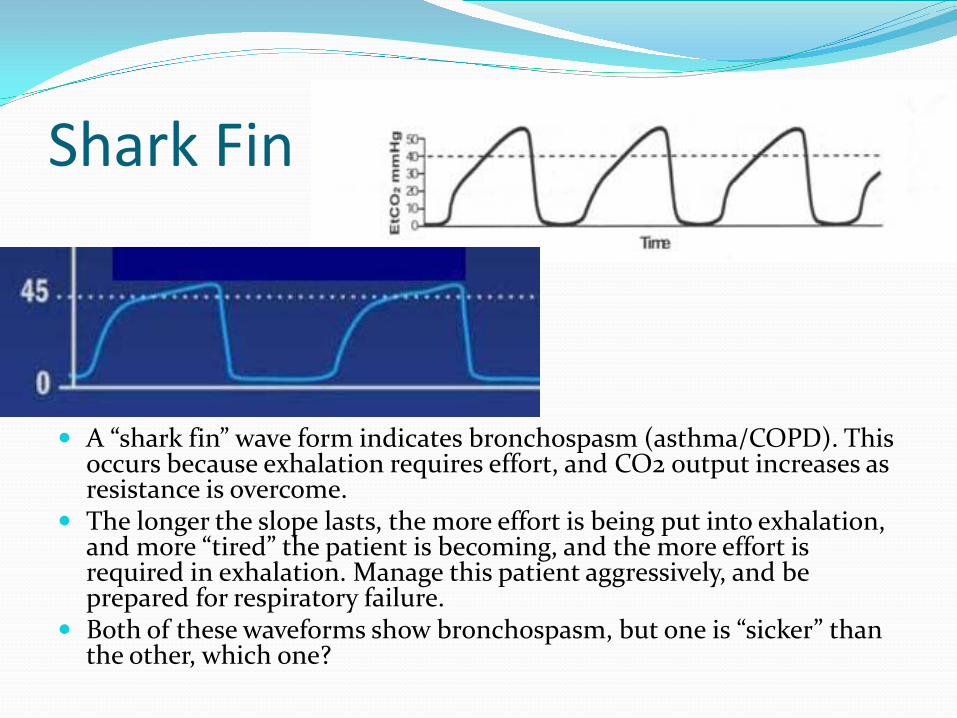
A “shark fin” wave form indicates bronchospasm (asthma/COPD). This occurs because exhalation requires effort, and CO2 output increases as resistance is overcome.
The longer the slope lasts, the more effort is being put into exhalation, and more “tired” the patient is becoming, and the more effort is required in exhalation. Manage this patient aggressively, and be prepared for respiratory failure.
Both of these waveforms show bronchospasm, but one is “sicker” than the other, which one?

Curare Cleft
A Curare Cleft is a notch that can be found anywhere in a waveform, with varying depths.
It is the result of spontaneous respiration from the patient This can be due to inadequate sedation, neuromuscular
blockade wearing off, due to the patient resisting ventilations (usually on a mechanical vent)
Fix this by more sedation or neuromuscular blockade. BVM ventilations (instead of ventilation by mechanical vent) can also improve this.


Normal Values Normal values for capnometry are 35-45. Remember that capnometry is dependent on cardiac output and
the ability of CO2 to cross from blood to inspired air for exhalation. Pulselessness, low metabolic rate (like hypothermia), or interrupted metaboilc process (like occurs with cyanide poisoning – when aerobic metabolism doesn’t occur, CO2 is not being created) can also effect EtCO2.
It’s also important to remember that while there is a direct correlation between EtCO2 and PaCO2, they are not necessarily the same (however, if you obtain a PaCO2 and EtCO2 at the same time, it is ok to assume that the difference will remain the same for a reasonable amount of time; e.g., EtCO2 is 32 and PaCO2 is 36, add 4 to your changing EtCO2 to approximate PaCO2 if you make changes to how you are ventilating)

During CPR EtCO2 > 20 indicate chest compressions are being
performed well Values any higher than 20 indicate the patient may
have a spontaneous pulse (this will help you differentiate PEA and hypotension, and help you decide on continuing CPR or started a fluid bolus and dopamine)
Values less than 10 mean chest compressions are not being performed well, ETT is displaced, or the metabolic processes are no longer occurring (i.e., the patient is dead)

For ventilation It is not uncommon to see values over 110 after intubating
patients that had inadequate respirations for an extended period of time.
Increasing ventilation rate results in a lower EtCO2 Goal is to maintain EtCO2 of 35-45 (hyperventilation to
maintain EtCO2 of 30 in head injuries is no longer recommended)
It is rarely warranted to ventilate >24 or <8/minute regardless of EtCO2; possible exceptions include DKA and hypothermia
The biggest clinical benefit in EMS is to avoid hyperventilation of intubated patients
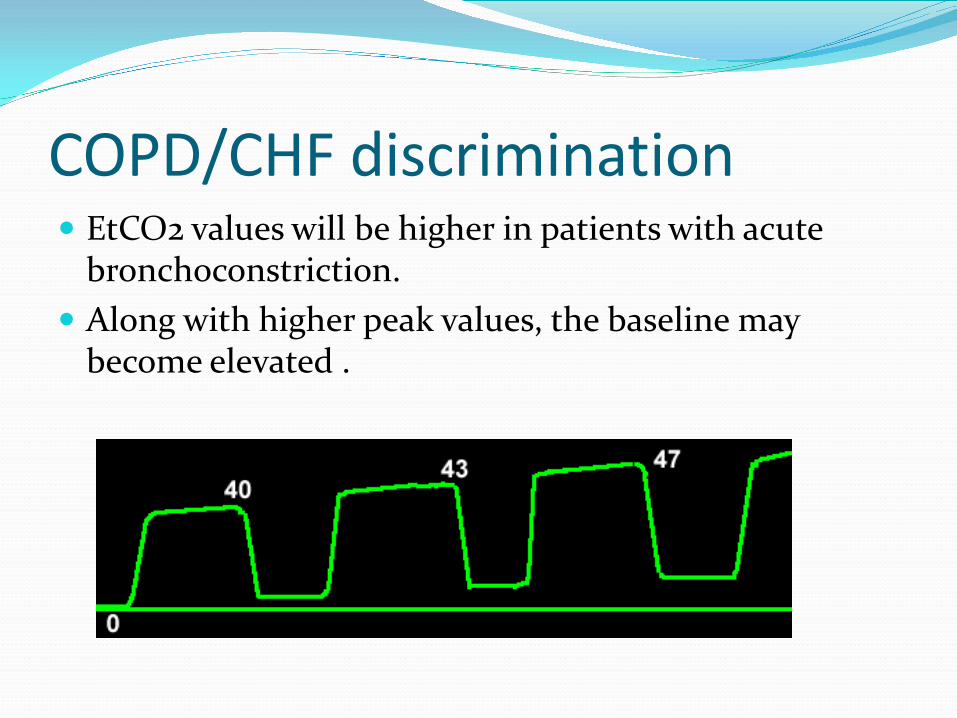
EtCO2 values will be higher in patients with acute bronchoconstriction.
Along with higher peak values, the baseline may become elevated .
COPD/CHF discrimination
EtCO2 can be used to determine whether bronchoconstriction is present, even in patients with inaudible lung sounds. A high EtCO2 in indicative of bronchoconstriction. A normal EtCO2 is non-diagnostic (it does not rule out
bronchoconstriction, or confirm pulmonary edema). If you’ve determined that a patient is either having a
exacerbation of COPD or CHF, but you’re not sure which, EtCO2 can answer this question for you.
COPD/CHF discrimination

EtCO2 is non-invasive and can be performed on any patient with any symptoms, but is strongly encouraged for all patients with respiratory distress.
Continuous EtCO2 monitoring is now expected (mandatory) for all patients in which nebulized medication is administered (be sure to document this in your report) When you administer nebulized medications, you are treating
bronchoconstriction, if you’re going to treat bronchoconstriction, you should assess for bronchoconstriction (of course, this can be done with lung sounds, but in a loud ambulance environment and many people will less than perfect hearing, EtCO2 can be easier to assess – so do both!)
EtCO2 changes are an excellent indicator of the effectiveness of bronchodilators. As nebulizer is more effective, you will see EtCO2 return to normal levels, and
baseline return to zero. An elevated, unchanging EtCO2 indicates that bronchoconstriction is not
improving
Continuous EtCO2 Monitoring
Capnography and capnometry can be very valuable tools if you understand how they work and their limitations.
In conjunction with SpO2, a normal EtCO2 range indicate a patient is being ventilated very well.
A square waveform on a capnograph is nearly irrefutable and objective evidence that intubation was successful, and that ventilations are being performed properly.
EtCO2 can be used on spontaneously breathing patients, ETT, King Tube, or LMA intubation, Trach or cric patients, or any other adjunct that you attach a BVM to, and the reference values do not change.