Direct questions or constructive criticism to:
Dr. Lawrence Cheung 2E4.34 [email protected]
Script: a 58 year old female presents to the emergency
department with gradually worsening dyspnea and a dry cough over
the past 8 months. Her exercise tolerance is now about 2 blocks.
She denies any chest pain, hemoptysis, orthopnea, or pnd. She is a
nonsmoker, is not on any medications, and has no past history of
medical problems, either in himself or his family. She works in an
office doing clerical work and denies exposure to any fumes or
gases. No one else in her workplace is ill. Functional inquiry is
negative for nasal symptoms, joint pains, skin rashes, weight loss,
fever or chills.
On physical exam, her vital signs are stable but his oxygen
saturation is only 85% on room air. It goes up to 90% with 5 lpm of
oxygen. Cardiac exam is unremarkable. Respiratory exam is
remarkable for bilateral crackles at both bases and mild clubbing.
The rest of the physical exam is unremarkable.
Bloodwork including a CBC, lytes, BUN, Cr, liver enzymes,
calcium, EKG, are all unremarkable.
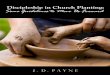
A CXR is performed and shown on the next slide.So, question
number 1 how would you interpret the CXR?
This CXR shows bilateral reticular opacities with a bibasilar
and peripheral predominance. There are no obvious pleural
effusions. The cardiac sillohouette is just within normal limits.
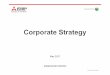
The reticular pattern is better appreciated on the CT chest that
was done on this patient which is shown on the next slide.
The CT chest on this patient demonstrates thickening of the
septa, resulting in a honeycomb appearance, especially seen in the
right lung periphery, as shown by the single long arrow. As well,
there is some scarring in the dorsal areas on this cut, as shown by
the short arrows.
Sometimes it is hard to tell the difference between a reticular
pattern and airspace disease on the plain CXR, especially when the
reticular disease is severe. An example of airspace disease is
shown on the next slide. This is an example of a patient with
airspace disease who turned out to have organizing pneumonia on
lung biopsy. Note how the radiographic appearance of airspace
disease differs from the appearance of reticular opacities seen in
the patient in our case.This patient went on to have PFTs. She was
able to do some spirometry but could not tolerate further
post-bronchodilator testing. We were able to measure her lung
volumes but she could not come off of oxygen long enough for us to
measure diffusing capacity.
Q number x how would you interpret her PFTs?
Answer with the measurements that were obtained, we can tell
that she does not seem to have an obstructive defect because here
FEV1 / FEVC ratio is 97% predicted. However, she does have a
restrictive defect because here TLC is low. Thus, the PFTs are
compatible with a restrictive defect.Question number 3, given the
clinical features, radiographs, and PFTs, what is your most likely
clinical diagnosis?
Answer At this point, our most likely diagnosis is pulmonary
fibrosis. Other diseases that can give rise to similar radiographs
are fibrosis due to certain medications, connective tissue disease,
pneumoconiosis, and less commonly, chronic hypersensitivity
pneumonitis, but she had nothing to suggest these diseases on
history or physical. Sarcoidosis is less likely because the
fibrosis seen in this disease is usually distributed in the upper
lobes. Chronic infections such as TB usually do not give rise to
this radiographic appearance.
Question number 4 Amongst the options listed below, what would
you do next?
At the very least, bronchoscopy with a bronchoalveolar lavage
should be performed to look for infection (even though it is
clinically unlikely) as well as malignancy.
Unfortunately, what to do in addition to this is somewhat
controversial but, thats life.
Some respirologists would do a transbronchial biopsy keep in
mind, however, that this is only useful if the biopsy shows
granulomas (to suggest a granulomatous disease like sarcoid),
infection, or malignancy. If the biopsy just shows non-specific
fibrosis, this is not very useful because, due to the small amount
of tissue obtained, it is hard to come up with a specific diagnosis
like organizing pneumonia, UIP, etc, as a cause of the
fibrosis.
An open lung biopsy would be ideal, but not every patient can
tolerate this due to severe cardiopulmonary disease, medical
comorbidities or physical frailty.
Some people would advocate empiric treatment with steroids.
However, steroids have side effects, and there are many forms of
fibrosis which are not responsive to steroids.
For this patient, we performed a bronchoscopy with BAL which did
not reveal malignancy or infection. She then underwent an open lung
biopsy which showed UIP pattern. Note that I used the term UIP
pattern because, as mentioned in the Pulmonary Medicine Primer, we
use this terminology because the final diagnosis should ideally
incorporate the clinical features, the pathology, and the
radiology. In other words, you, the clinician, now take the biopsy
result of UIP-pattern and decide if the UIP-pattern is due to any
cause discernible on history, such as a medication, connective
tissue disease, a pneumoconiosis, or chronic hypersensitivity
pneumonitis. If no obvious clinical cause is found, you would call
it Idiopathic pulmonary fibrosis. If a cause is apparent on
history, such as a medication like amiodarone, you would call it
UIP-pattern due to amiodarone, and so on.
In this particular case, we did not find any evidence of any
medication, connective tissue disease, pneumoconiosis, or chronic
hypersensitivity pneumonitis to cause her UIP-pattern. Thus, we
made a diagnosis of idiopathic pulmonary fibrosis.The patient is
worked up for a lung transplant and eventually put on the list for
this. She is sent home on 5 lpm of oxygen to maintain saturations
of > 90%. Over the next 6 months, she notices a gradual decline
in her exercise capacity, such that she can now barely walk outside
of her house. As well, her oxygen requirements have increased to 5
lpm.
She presents again to hospital with acute worsening of her
dyspnea over a few days. She has an associated dry cough which she
thinks is a bit worse than before. She denies fever or chills,
chest pain, or orthopnea. She has had bilateral pedal edema also
developing over the past few days.
In the emergency department, her HR is 110, with a stable BP.
She is using some accessory muscles of respiration and has a RR of
28. She can speak 8 to 10 word sentences. Her CXR shows more
reticular fibrosis compared with the previous CXR.
Question number x what is your explanation of why this patient
has deteriorated?The differential diagnosis is quite wide, but the
commonest causes would include heart failure, pulmonary embolism,
or LRTI. If the patient had co-existing COPD, then an exacerbation
of COPD could also be the cause.
One entity that is sometimes overlooked is an exacerbation of
the IPF. An example of this is nicely illustrated in the NEJM
article from 2002. Patients with IPF can experience an acute
worsening of their underlying disease, which can often come as a
surprise to the patient and clinician who believe that IPF is a
disease that can only progress slowly.
Our patient underwent a CT angio which did not demonstrate PE.
Left Heart failure with pulmonary edema was felt to be clinically
unlikely we felt the pedal edema was due to worsening right heart
function due to hypoxemia and pulmonary artery hypertension. We
placed the patient empirically on antibiotics and steroids, but she
continued to deteriorate and ultimately died of severe hypoxemia
despite high flow oxygen.