Embed Size (px)
Citation preview

DOI 10121201wnl0000275537716238e2007691293-1297 Neurology
Eduardo E BenarrochThermoregulation Recent concepts and remaining questions
This information is current as of September 17 2007
httpwwwneurologyorgcontent69121293fullhtmllocated on the World Wide Web at
The online version of this article along with updated information and services is
0028-3878 Online ISSN 1526-632Xsince 1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN
reg is the official journal of the American Academy of Neurology Published continuouslyNeurology
ThermoregulationRecent concepts and remaining questions
Eduardo E BenarrochMD
Maintenance of body core temperature withinnarrow limits is a major homeostatic functioncritical for survival Thermoregulation is a typicalexample of the integrative role of the hypothala-mus in generating patterns of autonomic endo-crine motor and behavioral responses to adaptto environmental challenges Experimental stud-ies have provided new information on mecha-nisms of thermal sensation hypothalamicintegration and central effect or pathways in-volved in thermoregulation1-5 Disorders of ther-moregulation are frequently puzzling to theneurologist Whereas some of these disorders maybe attributable to focal hypothalamic brainstemor spinal lesions or autonomic failure in manycases no clear cause is found Although there arestill many questions that remain unanswered re-cent insights into mechanisms of thermoregula-tion provide a framework to begin understandingthese challenging clinical problems and suggestpotential targets for dug therapy
FUNCTIONAL ANATOMY OF THERMOREGU-LATION Experimental evidence indicates that themedial preopticanterior hypothalamic area(POA) dorsomedial nucleus of the hypothalamus(DMH) periaqueductal gray matter of the mid-brain (PAG) and the nucleus raphe pallidus(RPa) in the medulla have a critical role inthermoregulation1-8 (figure)
The POA is the primary thermosensitive areaof the CNS12 In vitro studies indicate that thePOA contains warm-sensitive (WS) cold-sensitive and temperature-insensitive neurons2
The WS neurons act as the central integrators ofthermal information as their activity is deter-mined both by their own temperature and by af-ferent information from skin and visceralthermoreceptors These WS neurons are sponta-neously active and their rate of spontaneous de-polarization is controlled by a transienthyperpolarizing potassium (K) current (IA) In-
crease in hypothalamic temperature promotes in-activation of IA resulting in increased WS firing2
The dendrites of WS neurons are oriented perpen-dicular to the third ventricle and receive informa-tion from all ascending thermoreceptivepathways and from endogenous signals in theCSF2 This allows WS neurons to integrate infor-mation from skin thermosensors with that of vis-ceral and vascular thermosensor detectingchanges in core temperature Peripheral ther-mosensors including skin cold and warm sensorsexpress a subclass of transient receptor potential(TRP) channels called thermoTRP channels19
ThermoTRP channels include several subtypeseach is activated within a narrow physiologictemperature range9 Activation of these channelsresults in cation influx and depolarization of dor-sal root ganglion neurons that project totemperature-sensitive neurons of lamina I of thedorsal horn The dorsal horn conveys these pe-ripheral thermosensory signals to the POA bothdirectly via spinohypothalamic projections or in-directly via relay in brainstem nuclei includingthe parabrachial nucleus1
The level of activity of WS neurons triggers ei-ther heat-loss or heat-gain responses12 IncreasedWS neuron activity triggers sympathetically me-diated responses for heat loss including skin va-sodilation and sweating3 As WS neuronstonically inhibit cold-responsive hypothalamicand brainstem neurons decreased activity of WSneurons in response to inputs from peripheralcold receptors triggers cold-defense responses12
These include sympathetically mediated skin va-soconstriction shivering and in small mammalsnonshivering thermogenesis in the brown adiposetissue3
The mechanisms of hypothalamic thermoreg-ulation are still incompletely understood124
Studies in vitro indicate that the majority of POAneurons are temperature insensitive and partici-pate in reciprocal inhibitory interactions with WS
Address correspondence andreprint requests to Dr EBenarroch Department ofNeurology Mayo Clinic 200First Street SW West 8A MayoBldg or 811 Guggenheim BldgRochester MN 55905benarrocheduardomayoedu
From the Department of Neurology Mayo Clinic Rochester MN
Disclosure The author reports no conflicts of interest
CLINICALIMPLICATIONS OFNEUROSCIENCERESEARCH
Section EditorEduardo E Benarroch MD
Copyright copy 2007 by AAN Enterprises Inc 1293
neurons2 According to the ldquoset-pointrdquo modelWS neurons activate heat-loss effector neuronsand inhibit heat-gain effector neurons whereastemperature-insensitive neurons inhibit heat-lossand activate heat-gain effector neurons Thesetwo opposing influences would counterbalance ata core temperature ldquoset pointrdquo of 37 degC At highertemperatures the increased firing of WS neuronswould elicit a net excitation of heat-loss effectorneurons whereas at temperatures below 37 degCthe inhibitory influence of WS neurons on heat-production neurons would progressively decreasetriggering cold-defense responses2 However theldquoset-pointrdquomechanism of hypothalamic thermosen-sitivity continues to be disputed14 Core tempera-ture may fluctuate slightly but is maintained withina relatively narrow zone (within 02 to 05 degC) byadjustments of skin vasomotor responses onlylarger fluctuations of core temperature above or be-low certain threshold zones activate sweating orshivering responses respectively4
Recent experimental studies provide informa-tion on the central pathways that mediate the in-fluences of the POA on thermoregulatoryeffectors3 So far the pathways involved in cold-defense responses have been better characterized
than those mediating heat-loss responses (figure)Several parallel pathways involving the DMH6
PAG7 and RPa58 have been found to be involvedin the responses to cold exposure The RPa is apivotal component of these pathways as it sendsdescending projections that activate sympatheticpreganglionic neurons that control skin vasocon-striction and nonshivering thermogenesis and to-gether with adjacent portions of the reticularformation activates motor neurons that elicitshivering358 According to a current model thehypothalamic WS neurons tonically inhibit cold-responsive neurons of the DMH and RPa TheDMH both directly and via the caudal PAG acti-vates the RPa neurons initiating cold-defense re-sponses357 The pathways involved in heat lossare much less well understood Some studies indi-cate that the caudal portion of the RPa may acti-vate skin vasodilation and sweating10 Effects oflesions in humans suggest that the insular cortexhypothalamus or both may provide a descendingpathway that exerts an inhibitory influence onsympathetic neurons that activate sweating on thecontralateral body Unilateral hyperhidrosis canoccur following strokes involving the contralat-eral insula hypothalamus or brainstem11-14
POSSIBLE MECHANISMS OF THERMOREGU-LATORY DYSFUNCTION IN NEUROLOGIC DIS-ORDERS Recent insights into the mechanismsand pathways involved in thermoregulation mayhelp to understand some clinical thermoregula-tory disorders such as paroxysmal hypothermiawith hyperhydrosis and hypothermia in multiplesclerosis (MS)
PAROXYSMAL HYPOTHERMIA WITH HYPER-HIDROSIS Hypothermia is defined as a core (rec-tal) temperature lower than 35 degC Spontaneousepisodic hypothermia may occur in several condi-tions15 Paroxysmal hypothermia with hyperhi-drosis (PHH) is characterized by episodes ofhypothermia associated with excessive sweatingthat is commonly generalized15-17 but may also beunilateral18 Associated manifestations includepallor or flushing sensation of being cold or hotbradycardia generalized weakness ataxia andconfusional state Shivering may or may not oc-cur despite the profound hypothermia Theremay be wide fluctuations of core temperatureduring the day The effector mechanisms of heatgain and heat loss may respond normally but areactivated at lower core temperature suggestingthat there is a low core temperature set point andincreased gain of sweat response This may ex-plain the failure of external warming to improve
Figure Central thermoregulatory pathways involved in responses triggered bywarm-sensitive (WS) neurons of the medial preopticanteriorhypothalamic region
The WS neurons are activated by increased in core temperature and inhibited by inputs fromcold receptors in the skin possibly via temperature-insensitive preoptic hypothalamic neu-rons (not shown) The WS neurons trigger responses for heat loss (skin vasodilation andsweating) via still poorly defined pathways that may involve the caudal portion of the nucleusraphe pallidus (RPa) In contrast WS neurons tonically inhibit cold-responsive neurons of thedorsomedial nucleus of the hypothalamus (DMH) periaqueductal gray (PAG) and RPa Therostral PAG mediates some of the inhibitory effects of WS on the RPa whereas the caudalPAG mediates excitatory effects of DMH neurons on these raphe neurons Cold exposureresults in decrease in WS activity and disinhibition of DMH PAG and RPa neurons thatinitiate responses for heat conservation (skin vasoconstriction) or production (shivering ornonshivering thermogenesis)
1294 Neurology 69 September 18 2007
hypothermia in many of these cases The episodesmay last variably between 30 minutes and 2hours recur several times daily without a clearprecipitating factor continue daily for severalweeks or months and then subside spontaneouslyor may be separated by long asymptomatic peri-ods lasting several months The causes and mech-anisms underlying PHH are heterogeneous andwith few exceptions largely unknown15 (table 1)This syndrome may rarely occur in associationwith agenesis of the corpus callosum (Shapirosyndrome)16 but callosal agenesis cannot explainthe syndrome as paroxysmal hyperthermia (re-verse Shapiro syndrome) may also occur in thiscondition19 In one autopsy case of Shapiro syn-drome there was neuronal loss in the infundib-
ular and premammillary nuclei of thehypothalamus20 but hypothalamic lesions havenot been documented in other cases PHH hasalso been described with basal forebrain le-sions17 acute hydrocephalus21 subarachnoidhemorrhage22 traumatic brain injury23 limbicencephalitis24 and in association with HIVinfections25However most cases of PHH arenot associated with detectable structural ab-normality or underlying disease
Paroxysmal hypothermia may occur in chil-dren some of them with history ofmigraine sug-gesting that PHH may be an example ofchildhood periodic syndrome associated with mi-graine26 It is conceivable that at least in somecases PHH may be a manifestation of a chan-nelopathy As discussed above there is in vitroevidence that voltage-gated K channels limit thefiring frequency of WS neurons Thus impairedactivity of these channels may result in an inap-propriate increase in WS firing and sweatingleading to hypothermia This possibility is sup-ported by a report of a patient who developed se-vere hypothermia and diaphoresis as aconsequence of accidental overdose of4-aminopyridine a drug that blocks voltage-gated K channels27 Hyperhidrosis in patientswith Morvan syndrome which may be associatedwith K channel antibodies could reflect similarmechanisms The importance of exaggeratedsweating as the cause of hypothermia in thesecases is supported by the beneficial effect of drugsthat block muscarinic cholinergic receptors ofsweat glands such as oxybutynin or glycopyrro-
Table 2 Neurochemical influences that affect activity of thermoregulatory preoptic hypothalamic neurons
Influence Effect Clinical implications (examples)
Serotonin (5-HT2receptor)
Hyperthermia Serotonin syndrome IL-1 induced feverantipsychotic-induced hypothermia
Serotonin (5-HT1receptor)
Hypothermia SSRI-induced sweatingdagger postoperative hypothermiahypoxia-induced hypothermia
Dopamine (D2 receptor) Hypothermia Bromocriptine-induced hypothermia neurolepticmalignant syndromeDagger
Norepinephrine ( 1receptor)
Hypothermia Isoflurane-induced hypothermia
Opioids
receptor Hyperthermia Fentanyl reduces shivering threshold during epiduralanesthesia
and receptors Hypothermia Hypothermia during opioid overdose
Acidosis Hyperthermia Heat shock
Prostaglandin E2 Hyperthermia Fever
Risperidone and other antipsychotic agents block 5-HT2 receptors and this could lead to hypothermiadaggerCyproheptadine may reduce SSRI-induced sweating presumably by blocking 5-HT1 receptorsDaggerThis disorder may reflect blockade of D2 receptors in the hypothalamusIL-1 interleukin 1 SSRI selective serotonin reuptake inhibitors
Table 1 Conditions associated with paroxysmalhypothermia
Congenital lesions
Agenesis of corpus callosum (Shapiro syndrome)
Basal forebrain malformation
Acquired disorders
Hemispheric stroke
Hypothalamic lesions
Traumatic brain injury
Multiple sclerosis
Acute hydrocephalus
Subarachnoid hemorrhage
Leigh syndrome
Limbic encephalitis
HIV infection
Neurology 69 September 18 2007 1295
late in ameliorating hypothermia in these pa-tients17 Other treatments that have been reportedto be effective in isolated cases include cyprohep-tadine (a nonselective serotonin receptorblocker) clonidine (an 2-receptor agonist)chlorpromazine (a D2 dopamine receptorblocker) and rarely antiepileptic drugs such asphenobarbital or phenytoin15 The lack of consis-tent response to these centrally acting drugs likelyreflect the multiplicity of neurochemical influ-ences that may affect thermoregulation at thelevel of the POA and manifest clinically with hy-pothermia or hyperthermia (table 2)
HYPOTHERMIA IN MS There are several reportsof hypothermia as a manifestation of MS bothduring acute relapses or chronically2829 Althoughhypothermia may reflect posterior hypothalamicinvolvement in MS in many cases no hypotha-lamic lesion is found The PAG is frequently af-fected in MS and involvement of this importantrelay of cold-response pathways may explain atleast some of the cases of hypothermia in this dis-order This is supported that the fact the PAG isalso typically affected in Wernicke encephalopa-thy a condition may also manifest withhypothermia
PERSPECTIVE There have been important ad-vances in basic science research on mechanisms ofthermoregulation but many questions regardingthe pathophysiology of human thermoregulatorydisorders still remain unanswered Neverthelessthese experimental studies provide insights andtestable hypotheses that may eventually lead tobetter therapeutic approaches to these challeng-ing disorders For example it could be hypothe-sized that acetazolamide which is effective in K
channelopathies such as episodic ataxia type 1 ortopiramate which is effective for migraine pro-phylaxis and also reduces sweat productioncould be considered as therapeutic options in pa-tients with PHH that do not respond to othertreatments Unfortunately the infrequent occur-rence of these groups of disorders makes it diffi-cult to design controlled therapeutic trials
REFERENCES1 Romanovsky AA Thermoregulation some concepts
have changed Functional architecture of the thermo-regulatory system Am J Physiol Regul Integr CompPhysiol 2007292R37ndashR46
2 Boulant JA Neuronal basis of Hammelrsquos model forset-point thermoregulation J Appl Physiol 20061001347ndash1354
3 Nagashima K Nakai S TanakaM Kanosue K Neuro-nal circuitries involved in thermoregulation AutonNeurosci 20008518ndash25
4 Mekjavic IB Eiken O Contribution of thermal andnonthermal factors to the regulation of body tempera-ture in humans J Appl Physiol 20061002065ndash2072
5 McAllen RM The cold path to BAT Am J PhysiolRegul Integr Comp Physiol 2007292R124ndashR126
6 Dimicco JA Zaretsky DV The dorsomedial hypothal-amus a new player in thermoregulation Am J PhysiolRegul Integr Comp Physiol 2007292R47ndashR63
7 Yoshida K Konishi M Nagashima K Saper CB Kano-sue K Fos activation in hypothalamic neurons duringcold or warm exposure projections to periaqueductalgray matter Neuroscience 20051331039ndash1046
8 Nakamura K Morrison SF Central efferent pathwaysmediating skin cooling-evoked sympathetic thermo-genesis in brown adipose tissue Am J Physiol RegulIntegr Comp Physiol 2007292R127ndashR136
9 CaterinaMJ Transient receptor potential ion channelsas participants in thermosensation and thermoregula-tion Am J Physiol Regul Integr Comp Physiol 2007292R64ndashR76
10 Asahina M Sakakibara R Liu Z Ito T Yamanaka Yet al The raphe magnuspallidus regulates sweat secre-tion and skin vasodilation of the cat forepaw pad apreliminary electrical stimulation study Neurosci Lett2007
11 Labar DR Mohr JP Nichols FT3rd Tatemichi TKUnilateral hyperhidrosis after cerebral infarction Neu-rology 1988381679ndash1682
12 Korpelainen JT Sotaniemi KA Myllyla VV Asym-metric sweating in stroke a prospective quantitativestudy of patients with hemispheral brain infarctionNeurology 1993431211ndash1214
13 Kim BS Kim YI Lee KS Contralateral hyperhidrosisafter cerebral infarction Clinicoanatomic correlationsin five cases Stroke 199526896ndash899
14 Smith CD A hypothalamic stroke producing recurrenthemihyperhidrosis Neurology 2001561394ndash1396
15 Kloos RT Spontaneous periodic hypothermia Medi-cine (Baltimore) 199574268ndash280
16 LeWitt PA Newman RP Greenberg HS Rocher LLCalne DB Ehrenkranz JR Episodic hyperhidrosis hy-pothermia and agenesis of corpus callosum Neurol-ogy 1983331122ndash1129
17 Klein CJ Silber MH Halliwill JR Schreiner SASuarez GA Low PA Basal forebrain malformationwith hyperhidrosis and hypothermia variant of Shapi-rorsquos syndrome Neurology 200156254ndash256
18 Magnifico F Pierangeli G Barletta G et al Paroxys-mal episodic central thermoregulatory failure Neurol-ogy 2002581300ndash1302
19 Hirayama K Hoshino Y Kumashiro H Yamamoto TReverse Shapirorsquos syndrome A case of agenesis of cor-pus callosum associated with periodic hyperthermiaArch Neurol 199451494ndash496
20 Noel P Hubert JP Ectors M Franken L Flament-Durand J Agenesis of the corpus callosum associatedwith relapsing hypothermia A clinico-pathological re-port Brain 197396359ndash368
21 Darnell RB Arbit E Reversible diencephalic dysfunc-tion episodic hyperhidrosis due to a trapped third ven-tricle Neurology 199343579ndash582
1296 Neurology 69 September 18 2007
22 Tuettenberg J Woitzik J Siegel L Thome C Episodichypothermia and hyperhidrosis after subarachnoid hem-orrhage Case illustration J Neurosurg 200399610
23 De Tanti A Gasperini G Rossini M Paroxysmal epi-sodic hypothalamic instability with hypothermia aftertraumatic brain injury Brain Inj 2005191277ndash1283
24 Fukushima K Yasaki M Kaneko K et al Nonpara-neoplastic nonherpetic limbic encephalitis with severeepisodic hypothermia a case report Eur Neurol 200554170ndash174
25 Moulignier A Guiard-Schmid JB Gbadoe AH Rozen-baum W HIV-1-related spontaneous episodic hypo-thermia Neurology 200361418ndash419
26 Ruiz C Gener B Garaizar C Prats JM Episodic spon-taneous hypothermia a periodic childhood syndromePediatr Neurol 200328304ndash306
27 Johnson NC Morgan MW An unusual case of4-aminopyridine toxicity J Emerg Med 200630175ndash177
28 White KD Scoones DJ Newman PK Hypothermia inmultiple sclerosis J Neurol Neurosurg Psychiatry199661369ndash375
29 Edwards S Lennox G Robson K Whiteley A Hypo-thermia due to hypothalamic involvement in multiplesclerosis J Neurol Neurosurg Psychiatry 199661419ndash420
Neurology 69 September 18 2007 1297
DOI 10121201wnl0000275537716238e2007691293-1297 Neurology
Eduardo E BenarrochThermoregulation Recent concepts and remaining questions
This information is current as of September 17 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent69121293fullhtmlincluding high resolution figures can be found at
References
1httpwwwneurologyorgcontent69121293fullhtmlref-list-at This article cites 28 articles 19 of which you can access for free
Citations
icleshttpwwwneurologyorgcontent69121293fullhtmlotherartThis article has been cited by 4 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

ThermoregulationRecent concepts and remaining questions
Eduardo E BenarrochMD
Maintenance of body core temperature withinnarrow limits is a major homeostatic functioncritical for survival Thermoregulation is a typicalexample of the integrative role of the hypothala-mus in generating patterns of autonomic endo-crine motor and behavioral responses to adaptto environmental challenges Experimental stud-ies have provided new information on mecha-nisms of thermal sensation hypothalamicintegration and central effect or pathways in-volved in thermoregulation1-5 Disorders of ther-moregulation are frequently puzzling to theneurologist Whereas some of these disorders maybe attributable to focal hypothalamic brainstemor spinal lesions or autonomic failure in manycases no clear cause is found Although there arestill many questions that remain unanswered re-cent insights into mechanisms of thermoregula-tion provide a framework to begin understandingthese challenging clinical problems and suggestpotential targets for dug therapy
FUNCTIONAL ANATOMY OF THERMOREGU-LATION Experimental evidence indicates that themedial preopticanterior hypothalamic area(POA) dorsomedial nucleus of the hypothalamus(DMH) periaqueductal gray matter of the mid-brain (PAG) and the nucleus raphe pallidus(RPa) in the medulla have a critical role inthermoregulation1-8 (figure)
The POA is the primary thermosensitive areaof the CNS12 In vitro studies indicate that thePOA contains warm-sensitive (WS) cold-sensitive and temperature-insensitive neurons2
The WS neurons act as the central integrators ofthermal information as their activity is deter-mined both by their own temperature and by af-ferent information from skin and visceralthermoreceptors These WS neurons are sponta-neously active and their rate of spontaneous de-polarization is controlled by a transienthyperpolarizing potassium (K) current (IA) In-
crease in hypothalamic temperature promotes in-activation of IA resulting in increased WS firing2
The dendrites of WS neurons are oriented perpen-dicular to the third ventricle and receive informa-tion from all ascending thermoreceptivepathways and from endogenous signals in theCSF2 This allows WS neurons to integrate infor-mation from skin thermosensors with that of vis-ceral and vascular thermosensor detectingchanges in core temperature Peripheral ther-mosensors including skin cold and warm sensorsexpress a subclass of transient receptor potential(TRP) channels called thermoTRP channels19
ThermoTRP channels include several subtypeseach is activated within a narrow physiologictemperature range9 Activation of these channelsresults in cation influx and depolarization of dor-sal root ganglion neurons that project totemperature-sensitive neurons of lamina I of thedorsal horn The dorsal horn conveys these pe-ripheral thermosensory signals to the POA bothdirectly via spinohypothalamic projections or in-directly via relay in brainstem nuclei includingthe parabrachial nucleus1
The level of activity of WS neurons triggers ei-ther heat-loss or heat-gain responses12 IncreasedWS neuron activity triggers sympathetically me-diated responses for heat loss including skin va-sodilation and sweating3 As WS neuronstonically inhibit cold-responsive hypothalamicand brainstem neurons decreased activity of WSneurons in response to inputs from peripheralcold receptors triggers cold-defense responses12
These include sympathetically mediated skin va-soconstriction shivering and in small mammalsnonshivering thermogenesis in the brown adiposetissue3
The mechanisms of hypothalamic thermoreg-ulation are still incompletely understood124
Studies in vitro indicate that the majority of POAneurons are temperature insensitive and partici-pate in reciprocal inhibitory interactions with WS
Address correspondence andreprint requests to Dr EBenarroch Department ofNeurology Mayo Clinic 200First Street SW West 8A MayoBldg or 811 Guggenheim BldgRochester MN 55905benarrocheduardomayoedu
From the Department of Neurology Mayo Clinic Rochester MN
Disclosure The author reports no conflicts of interest
CLINICALIMPLICATIONS OFNEUROSCIENCERESEARCH
Section EditorEduardo E Benarroch MD
Copyright copy 2007 by AAN Enterprises Inc 1293
neurons2 According to the ldquoset-pointrdquo modelWS neurons activate heat-loss effector neuronsand inhibit heat-gain effector neurons whereastemperature-insensitive neurons inhibit heat-lossand activate heat-gain effector neurons Thesetwo opposing influences would counterbalance ata core temperature ldquoset pointrdquo of 37 degC At highertemperatures the increased firing of WS neuronswould elicit a net excitation of heat-loss effectorneurons whereas at temperatures below 37 degCthe inhibitory influence of WS neurons on heat-production neurons would progressively decreasetriggering cold-defense responses2 However theldquoset-pointrdquomechanism of hypothalamic thermosen-sitivity continues to be disputed14 Core tempera-ture may fluctuate slightly but is maintained withina relatively narrow zone (within 02 to 05 degC) byadjustments of skin vasomotor responses onlylarger fluctuations of core temperature above or be-low certain threshold zones activate sweating orshivering responses respectively4
Recent experimental studies provide informa-tion on the central pathways that mediate the in-fluences of the POA on thermoregulatoryeffectors3 So far the pathways involved in cold-defense responses have been better characterized
than those mediating heat-loss responses (figure)Several parallel pathways involving the DMH6
PAG7 and RPa58 have been found to be involvedin the responses to cold exposure The RPa is apivotal component of these pathways as it sendsdescending projections that activate sympatheticpreganglionic neurons that control skin vasocon-striction and nonshivering thermogenesis and to-gether with adjacent portions of the reticularformation activates motor neurons that elicitshivering358 According to a current model thehypothalamic WS neurons tonically inhibit cold-responsive neurons of the DMH and RPa TheDMH both directly and via the caudal PAG acti-vates the RPa neurons initiating cold-defense re-sponses357 The pathways involved in heat lossare much less well understood Some studies indi-cate that the caudal portion of the RPa may acti-vate skin vasodilation and sweating10 Effects oflesions in humans suggest that the insular cortexhypothalamus or both may provide a descendingpathway that exerts an inhibitory influence onsympathetic neurons that activate sweating on thecontralateral body Unilateral hyperhidrosis canoccur following strokes involving the contralat-eral insula hypothalamus or brainstem11-14
POSSIBLE MECHANISMS OF THERMOREGU-LATORY DYSFUNCTION IN NEUROLOGIC DIS-ORDERS Recent insights into the mechanismsand pathways involved in thermoregulation mayhelp to understand some clinical thermoregula-tory disorders such as paroxysmal hypothermiawith hyperhydrosis and hypothermia in multiplesclerosis (MS)
PAROXYSMAL HYPOTHERMIA WITH HYPER-HIDROSIS Hypothermia is defined as a core (rec-tal) temperature lower than 35 degC Spontaneousepisodic hypothermia may occur in several condi-tions15 Paroxysmal hypothermia with hyperhi-drosis (PHH) is characterized by episodes ofhypothermia associated with excessive sweatingthat is commonly generalized15-17 but may also beunilateral18 Associated manifestations includepallor or flushing sensation of being cold or hotbradycardia generalized weakness ataxia andconfusional state Shivering may or may not oc-cur despite the profound hypothermia Theremay be wide fluctuations of core temperatureduring the day The effector mechanisms of heatgain and heat loss may respond normally but areactivated at lower core temperature suggestingthat there is a low core temperature set point andincreased gain of sweat response This may ex-plain the failure of external warming to improve
Figure Central thermoregulatory pathways involved in responses triggered bywarm-sensitive (WS) neurons of the medial preopticanteriorhypothalamic region
The WS neurons are activated by increased in core temperature and inhibited by inputs fromcold receptors in the skin possibly via temperature-insensitive preoptic hypothalamic neu-rons (not shown) The WS neurons trigger responses for heat loss (skin vasodilation andsweating) via still poorly defined pathways that may involve the caudal portion of the nucleusraphe pallidus (RPa) In contrast WS neurons tonically inhibit cold-responsive neurons of thedorsomedial nucleus of the hypothalamus (DMH) periaqueductal gray (PAG) and RPa Therostral PAG mediates some of the inhibitory effects of WS on the RPa whereas the caudalPAG mediates excitatory effects of DMH neurons on these raphe neurons Cold exposureresults in decrease in WS activity and disinhibition of DMH PAG and RPa neurons thatinitiate responses for heat conservation (skin vasoconstriction) or production (shivering ornonshivering thermogenesis)
1294 Neurology 69 September 18 2007
hypothermia in many of these cases The episodesmay last variably between 30 minutes and 2hours recur several times daily without a clearprecipitating factor continue daily for severalweeks or months and then subside spontaneouslyor may be separated by long asymptomatic peri-ods lasting several months The causes and mech-anisms underlying PHH are heterogeneous andwith few exceptions largely unknown15 (table 1)This syndrome may rarely occur in associationwith agenesis of the corpus callosum (Shapirosyndrome)16 but callosal agenesis cannot explainthe syndrome as paroxysmal hyperthermia (re-verse Shapiro syndrome) may also occur in thiscondition19 In one autopsy case of Shapiro syn-drome there was neuronal loss in the infundib-
ular and premammillary nuclei of thehypothalamus20 but hypothalamic lesions havenot been documented in other cases PHH hasalso been described with basal forebrain le-sions17 acute hydrocephalus21 subarachnoidhemorrhage22 traumatic brain injury23 limbicencephalitis24 and in association with HIVinfections25However most cases of PHH arenot associated with detectable structural ab-normality or underlying disease
Paroxysmal hypothermia may occur in chil-dren some of them with history ofmigraine sug-gesting that PHH may be an example ofchildhood periodic syndrome associated with mi-graine26 It is conceivable that at least in somecases PHH may be a manifestation of a chan-nelopathy As discussed above there is in vitroevidence that voltage-gated K channels limit thefiring frequency of WS neurons Thus impairedactivity of these channels may result in an inap-propriate increase in WS firing and sweatingleading to hypothermia This possibility is sup-ported by a report of a patient who developed se-vere hypothermia and diaphoresis as aconsequence of accidental overdose of4-aminopyridine a drug that blocks voltage-gated K channels27 Hyperhidrosis in patientswith Morvan syndrome which may be associatedwith K channel antibodies could reflect similarmechanisms The importance of exaggeratedsweating as the cause of hypothermia in thesecases is supported by the beneficial effect of drugsthat block muscarinic cholinergic receptors ofsweat glands such as oxybutynin or glycopyrro-
Table 2 Neurochemical influences that affect activity of thermoregulatory preoptic hypothalamic neurons
Influence Effect Clinical implications (examples)
Serotonin (5-HT2receptor)
Hyperthermia Serotonin syndrome IL-1 induced feverantipsychotic-induced hypothermia
Serotonin (5-HT1receptor)
Hypothermia SSRI-induced sweatingdagger postoperative hypothermiahypoxia-induced hypothermia
Dopamine (D2 receptor) Hypothermia Bromocriptine-induced hypothermia neurolepticmalignant syndromeDagger
Norepinephrine ( 1receptor)
Hypothermia Isoflurane-induced hypothermia
Opioids
receptor Hyperthermia Fentanyl reduces shivering threshold during epiduralanesthesia
and receptors Hypothermia Hypothermia during opioid overdose
Acidosis Hyperthermia Heat shock
Prostaglandin E2 Hyperthermia Fever
Risperidone and other antipsychotic agents block 5-HT2 receptors and this could lead to hypothermiadaggerCyproheptadine may reduce SSRI-induced sweating presumably by blocking 5-HT1 receptorsDaggerThis disorder may reflect blockade of D2 receptors in the hypothalamusIL-1 interleukin 1 SSRI selective serotonin reuptake inhibitors
Table 1 Conditions associated with paroxysmalhypothermia
Congenital lesions
Agenesis of corpus callosum (Shapiro syndrome)
Basal forebrain malformation
Acquired disorders
Hemispheric stroke
Hypothalamic lesions
Traumatic brain injury
Multiple sclerosis
Acute hydrocephalus
Subarachnoid hemorrhage
Leigh syndrome
Limbic encephalitis
HIV infection
Neurology 69 September 18 2007 1295
late in ameliorating hypothermia in these pa-tients17 Other treatments that have been reportedto be effective in isolated cases include cyprohep-tadine (a nonselective serotonin receptorblocker) clonidine (an 2-receptor agonist)chlorpromazine (a D2 dopamine receptorblocker) and rarely antiepileptic drugs such asphenobarbital or phenytoin15 The lack of consis-tent response to these centrally acting drugs likelyreflect the multiplicity of neurochemical influ-ences that may affect thermoregulation at thelevel of the POA and manifest clinically with hy-pothermia or hyperthermia (table 2)
HYPOTHERMIA IN MS There are several reportsof hypothermia as a manifestation of MS bothduring acute relapses or chronically2829 Althoughhypothermia may reflect posterior hypothalamicinvolvement in MS in many cases no hypotha-lamic lesion is found The PAG is frequently af-fected in MS and involvement of this importantrelay of cold-response pathways may explain atleast some of the cases of hypothermia in this dis-order This is supported that the fact the PAG isalso typically affected in Wernicke encephalopa-thy a condition may also manifest withhypothermia
PERSPECTIVE There have been important ad-vances in basic science research on mechanisms ofthermoregulation but many questions regardingthe pathophysiology of human thermoregulatorydisorders still remain unanswered Neverthelessthese experimental studies provide insights andtestable hypotheses that may eventually lead tobetter therapeutic approaches to these challeng-ing disorders For example it could be hypothe-sized that acetazolamide which is effective in K
channelopathies such as episodic ataxia type 1 ortopiramate which is effective for migraine pro-phylaxis and also reduces sweat productioncould be considered as therapeutic options in pa-tients with PHH that do not respond to othertreatments Unfortunately the infrequent occur-rence of these groups of disorders makes it diffi-cult to design controlled therapeutic trials
REFERENCES1 Romanovsky AA Thermoregulation some concepts
have changed Functional architecture of the thermo-regulatory system Am J Physiol Regul Integr CompPhysiol 2007292R37ndashR46
2 Boulant JA Neuronal basis of Hammelrsquos model forset-point thermoregulation J Appl Physiol 20061001347ndash1354
3 Nagashima K Nakai S TanakaM Kanosue K Neuro-nal circuitries involved in thermoregulation AutonNeurosci 20008518ndash25
4 Mekjavic IB Eiken O Contribution of thermal andnonthermal factors to the regulation of body tempera-ture in humans J Appl Physiol 20061002065ndash2072
5 McAllen RM The cold path to BAT Am J PhysiolRegul Integr Comp Physiol 2007292R124ndashR126
6 Dimicco JA Zaretsky DV The dorsomedial hypothal-amus a new player in thermoregulation Am J PhysiolRegul Integr Comp Physiol 2007292R47ndashR63
7 Yoshida K Konishi M Nagashima K Saper CB Kano-sue K Fos activation in hypothalamic neurons duringcold or warm exposure projections to periaqueductalgray matter Neuroscience 20051331039ndash1046
8 Nakamura K Morrison SF Central efferent pathwaysmediating skin cooling-evoked sympathetic thermo-genesis in brown adipose tissue Am J Physiol RegulIntegr Comp Physiol 2007292R127ndashR136
9 CaterinaMJ Transient receptor potential ion channelsas participants in thermosensation and thermoregula-tion Am J Physiol Regul Integr Comp Physiol 2007292R64ndashR76
10 Asahina M Sakakibara R Liu Z Ito T Yamanaka Yet al The raphe magnuspallidus regulates sweat secre-tion and skin vasodilation of the cat forepaw pad apreliminary electrical stimulation study Neurosci Lett2007
11 Labar DR Mohr JP Nichols FT3rd Tatemichi TKUnilateral hyperhidrosis after cerebral infarction Neu-rology 1988381679ndash1682
12 Korpelainen JT Sotaniemi KA Myllyla VV Asym-metric sweating in stroke a prospective quantitativestudy of patients with hemispheral brain infarctionNeurology 1993431211ndash1214
13 Kim BS Kim YI Lee KS Contralateral hyperhidrosisafter cerebral infarction Clinicoanatomic correlationsin five cases Stroke 199526896ndash899
14 Smith CD A hypothalamic stroke producing recurrenthemihyperhidrosis Neurology 2001561394ndash1396
15 Kloos RT Spontaneous periodic hypothermia Medi-cine (Baltimore) 199574268ndash280
16 LeWitt PA Newman RP Greenberg HS Rocher LLCalne DB Ehrenkranz JR Episodic hyperhidrosis hy-pothermia and agenesis of corpus callosum Neurol-ogy 1983331122ndash1129
17 Klein CJ Silber MH Halliwill JR Schreiner SASuarez GA Low PA Basal forebrain malformationwith hyperhidrosis and hypothermia variant of Shapi-rorsquos syndrome Neurology 200156254ndash256
18 Magnifico F Pierangeli G Barletta G et al Paroxys-mal episodic central thermoregulatory failure Neurol-ogy 2002581300ndash1302
19 Hirayama K Hoshino Y Kumashiro H Yamamoto TReverse Shapirorsquos syndrome A case of agenesis of cor-pus callosum associated with periodic hyperthermiaArch Neurol 199451494ndash496
20 Noel P Hubert JP Ectors M Franken L Flament-Durand J Agenesis of the corpus callosum associatedwith relapsing hypothermia A clinico-pathological re-port Brain 197396359ndash368
21 Darnell RB Arbit E Reversible diencephalic dysfunc-tion episodic hyperhidrosis due to a trapped third ven-tricle Neurology 199343579ndash582
1296 Neurology 69 September 18 2007
22 Tuettenberg J Woitzik J Siegel L Thome C Episodichypothermia and hyperhidrosis after subarachnoid hem-orrhage Case illustration J Neurosurg 200399610
23 De Tanti A Gasperini G Rossini M Paroxysmal epi-sodic hypothalamic instability with hypothermia aftertraumatic brain injury Brain Inj 2005191277ndash1283
24 Fukushima K Yasaki M Kaneko K et al Nonpara-neoplastic nonherpetic limbic encephalitis with severeepisodic hypothermia a case report Eur Neurol 200554170ndash174
25 Moulignier A Guiard-Schmid JB Gbadoe AH Rozen-baum W HIV-1-related spontaneous episodic hypo-thermia Neurology 200361418ndash419
26 Ruiz C Gener B Garaizar C Prats JM Episodic spon-taneous hypothermia a periodic childhood syndromePediatr Neurol 200328304ndash306
27 Johnson NC Morgan MW An unusual case of4-aminopyridine toxicity J Emerg Med 200630175ndash177
28 White KD Scoones DJ Newman PK Hypothermia inmultiple sclerosis J Neurol Neurosurg Psychiatry199661369ndash375
29 Edwards S Lennox G Robson K Whiteley A Hypo-thermia due to hypothalamic involvement in multiplesclerosis J Neurol Neurosurg Psychiatry 199661419ndash420
Neurology 69 September 18 2007 1297
DOI 10121201wnl0000275537716238e2007691293-1297 Neurology
Eduardo E BenarrochThermoregulation Recent concepts and remaining questions
This information is current as of September 17 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent69121293fullhtmlincluding high resolution figures can be found at
References
1httpwwwneurologyorgcontent69121293fullhtmlref-list-at This article cites 28 articles 19 of which you can access for free
Citations
icleshttpwwwneurologyorgcontent69121293fullhtmlotherartThis article has been cited by 4 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

neurons2 According to the ldquoset-pointrdquo modelWS neurons activate heat-loss effector neuronsand inhibit heat-gain effector neurons whereastemperature-insensitive neurons inhibit heat-lossand activate heat-gain effector neurons Thesetwo opposing influences would counterbalance ata core temperature ldquoset pointrdquo of 37 degC At highertemperatures the increased firing of WS neuronswould elicit a net excitation of heat-loss effectorneurons whereas at temperatures below 37 degCthe inhibitory influence of WS neurons on heat-production neurons would progressively decreasetriggering cold-defense responses2 However theldquoset-pointrdquomechanism of hypothalamic thermosen-sitivity continues to be disputed14 Core tempera-ture may fluctuate slightly but is maintained withina relatively narrow zone (within 02 to 05 degC) byadjustments of skin vasomotor responses onlylarger fluctuations of core temperature above or be-low certain threshold zones activate sweating orshivering responses respectively4
Recent experimental studies provide informa-tion on the central pathways that mediate the in-fluences of the POA on thermoregulatoryeffectors3 So far the pathways involved in cold-defense responses have been better characterized
than those mediating heat-loss responses (figure)Several parallel pathways involving the DMH6
PAG7 and RPa58 have been found to be involvedin the responses to cold exposure The RPa is apivotal component of these pathways as it sendsdescending projections that activate sympatheticpreganglionic neurons that control skin vasocon-striction and nonshivering thermogenesis and to-gether with adjacent portions of the reticularformation activates motor neurons that elicitshivering358 According to a current model thehypothalamic WS neurons tonically inhibit cold-responsive neurons of the DMH and RPa TheDMH both directly and via the caudal PAG acti-vates the RPa neurons initiating cold-defense re-sponses357 The pathways involved in heat lossare much less well understood Some studies indi-cate that the caudal portion of the RPa may acti-vate skin vasodilation and sweating10 Effects oflesions in humans suggest that the insular cortexhypothalamus or both may provide a descendingpathway that exerts an inhibitory influence onsympathetic neurons that activate sweating on thecontralateral body Unilateral hyperhidrosis canoccur following strokes involving the contralat-eral insula hypothalamus or brainstem11-14
POSSIBLE MECHANISMS OF THERMOREGU-LATORY DYSFUNCTION IN NEUROLOGIC DIS-ORDERS Recent insights into the mechanismsand pathways involved in thermoregulation mayhelp to understand some clinical thermoregula-tory disorders such as paroxysmal hypothermiawith hyperhydrosis and hypothermia in multiplesclerosis (MS)
PAROXYSMAL HYPOTHERMIA WITH HYPER-HIDROSIS Hypothermia is defined as a core (rec-tal) temperature lower than 35 degC Spontaneousepisodic hypothermia may occur in several condi-tions15 Paroxysmal hypothermia with hyperhi-drosis (PHH) is characterized by episodes ofhypothermia associated with excessive sweatingthat is commonly generalized15-17 but may also beunilateral18 Associated manifestations includepallor or flushing sensation of being cold or hotbradycardia generalized weakness ataxia andconfusional state Shivering may or may not oc-cur despite the profound hypothermia Theremay be wide fluctuations of core temperatureduring the day The effector mechanisms of heatgain and heat loss may respond normally but areactivated at lower core temperature suggestingthat there is a low core temperature set point andincreased gain of sweat response This may ex-plain the failure of external warming to improve
Figure Central thermoregulatory pathways involved in responses triggered bywarm-sensitive (WS) neurons of the medial preopticanteriorhypothalamic region
The WS neurons are activated by increased in core temperature and inhibited by inputs fromcold receptors in the skin possibly via temperature-insensitive preoptic hypothalamic neu-rons (not shown) The WS neurons trigger responses for heat loss (skin vasodilation andsweating) via still poorly defined pathways that may involve the caudal portion of the nucleusraphe pallidus (RPa) In contrast WS neurons tonically inhibit cold-responsive neurons of thedorsomedial nucleus of the hypothalamus (DMH) periaqueductal gray (PAG) and RPa Therostral PAG mediates some of the inhibitory effects of WS on the RPa whereas the caudalPAG mediates excitatory effects of DMH neurons on these raphe neurons Cold exposureresults in decrease in WS activity and disinhibition of DMH PAG and RPa neurons thatinitiate responses for heat conservation (skin vasoconstriction) or production (shivering ornonshivering thermogenesis)
1294 Neurology 69 September 18 2007
hypothermia in many of these cases The episodesmay last variably between 30 minutes and 2hours recur several times daily without a clearprecipitating factor continue daily for severalweeks or months and then subside spontaneouslyor may be separated by long asymptomatic peri-ods lasting several months The causes and mech-anisms underlying PHH are heterogeneous andwith few exceptions largely unknown15 (table 1)This syndrome may rarely occur in associationwith agenesis of the corpus callosum (Shapirosyndrome)16 but callosal agenesis cannot explainthe syndrome as paroxysmal hyperthermia (re-verse Shapiro syndrome) may also occur in thiscondition19 In one autopsy case of Shapiro syn-drome there was neuronal loss in the infundib-
ular and premammillary nuclei of thehypothalamus20 but hypothalamic lesions havenot been documented in other cases PHH hasalso been described with basal forebrain le-sions17 acute hydrocephalus21 subarachnoidhemorrhage22 traumatic brain injury23 limbicencephalitis24 and in association with HIVinfections25However most cases of PHH arenot associated with detectable structural ab-normality or underlying disease
Paroxysmal hypothermia may occur in chil-dren some of them with history ofmigraine sug-gesting that PHH may be an example ofchildhood periodic syndrome associated with mi-graine26 It is conceivable that at least in somecases PHH may be a manifestation of a chan-nelopathy As discussed above there is in vitroevidence that voltage-gated K channels limit thefiring frequency of WS neurons Thus impairedactivity of these channels may result in an inap-propriate increase in WS firing and sweatingleading to hypothermia This possibility is sup-ported by a report of a patient who developed se-vere hypothermia and diaphoresis as aconsequence of accidental overdose of4-aminopyridine a drug that blocks voltage-gated K channels27 Hyperhidrosis in patientswith Morvan syndrome which may be associatedwith K channel antibodies could reflect similarmechanisms The importance of exaggeratedsweating as the cause of hypothermia in thesecases is supported by the beneficial effect of drugsthat block muscarinic cholinergic receptors ofsweat glands such as oxybutynin or glycopyrro-
Table 2 Neurochemical influences that affect activity of thermoregulatory preoptic hypothalamic neurons
Influence Effect Clinical implications (examples)
Serotonin (5-HT2receptor)
Hyperthermia Serotonin syndrome IL-1 induced feverantipsychotic-induced hypothermia
Serotonin (5-HT1receptor)
Hypothermia SSRI-induced sweatingdagger postoperative hypothermiahypoxia-induced hypothermia
Dopamine (D2 receptor) Hypothermia Bromocriptine-induced hypothermia neurolepticmalignant syndromeDagger
Norepinephrine ( 1receptor)
Hypothermia Isoflurane-induced hypothermia
Opioids
receptor Hyperthermia Fentanyl reduces shivering threshold during epiduralanesthesia
and receptors Hypothermia Hypothermia during opioid overdose
Acidosis Hyperthermia Heat shock
Prostaglandin E2 Hyperthermia Fever
Risperidone and other antipsychotic agents block 5-HT2 receptors and this could lead to hypothermiadaggerCyproheptadine may reduce SSRI-induced sweating presumably by blocking 5-HT1 receptorsDaggerThis disorder may reflect blockade of D2 receptors in the hypothalamusIL-1 interleukin 1 SSRI selective serotonin reuptake inhibitors
Table 1 Conditions associated with paroxysmalhypothermia
Congenital lesions
Agenesis of corpus callosum (Shapiro syndrome)
Basal forebrain malformation
Acquired disorders
Hemispheric stroke
Hypothalamic lesions
Traumatic brain injury
Multiple sclerosis
Acute hydrocephalus
Subarachnoid hemorrhage
Leigh syndrome
Limbic encephalitis
HIV infection
Neurology 69 September 18 2007 1295
late in ameliorating hypothermia in these pa-tients17 Other treatments that have been reportedto be effective in isolated cases include cyprohep-tadine (a nonselective serotonin receptorblocker) clonidine (an 2-receptor agonist)chlorpromazine (a D2 dopamine receptorblocker) and rarely antiepileptic drugs such asphenobarbital or phenytoin15 The lack of consis-tent response to these centrally acting drugs likelyreflect the multiplicity of neurochemical influ-ences that may affect thermoregulation at thelevel of the POA and manifest clinically with hy-pothermia or hyperthermia (table 2)
HYPOTHERMIA IN MS There are several reportsof hypothermia as a manifestation of MS bothduring acute relapses or chronically2829 Althoughhypothermia may reflect posterior hypothalamicinvolvement in MS in many cases no hypotha-lamic lesion is found The PAG is frequently af-fected in MS and involvement of this importantrelay of cold-response pathways may explain atleast some of the cases of hypothermia in this dis-order This is supported that the fact the PAG isalso typically affected in Wernicke encephalopa-thy a condition may also manifest withhypothermia
PERSPECTIVE There have been important ad-vances in basic science research on mechanisms ofthermoregulation but many questions regardingthe pathophysiology of human thermoregulatorydisorders still remain unanswered Neverthelessthese experimental studies provide insights andtestable hypotheses that may eventually lead tobetter therapeutic approaches to these challeng-ing disorders For example it could be hypothe-sized that acetazolamide which is effective in K
channelopathies such as episodic ataxia type 1 ortopiramate which is effective for migraine pro-phylaxis and also reduces sweat productioncould be considered as therapeutic options in pa-tients with PHH that do not respond to othertreatments Unfortunately the infrequent occur-rence of these groups of disorders makes it diffi-cult to design controlled therapeutic trials
REFERENCES1 Romanovsky AA Thermoregulation some concepts
have changed Functional architecture of the thermo-regulatory system Am J Physiol Regul Integr CompPhysiol 2007292R37ndashR46
2 Boulant JA Neuronal basis of Hammelrsquos model forset-point thermoregulation J Appl Physiol 20061001347ndash1354
3 Nagashima K Nakai S TanakaM Kanosue K Neuro-nal circuitries involved in thermoregulation AutonNeurosci 20008518ndash25
4 Mekjavic IB Eiken O Contribution of thermal andnonthermal factors to the regulation of body tempera-ture in humans J Appl Physiol 20061002065ndash2072
5 McAllen RM The cold path to BAT Am J PhysiolRegul Integr Comp Physiol 2007292R124ndashR126
6 Dimicco JA Zaretsky DV The dorsomedial hypothal-amus a new player in thermoregulation Am J PhysiolRegul Integr Comp Physiol 2007292R47ndashR63
7 Yoshida K Konishi M Nagashima K Saper CB Kano-sue K Fos activation in hypothalamic neurons duringcold or warm exposure projections to periaqueductalgray matter Neuroscience 20051331039ndash1046
8 Nakamura K Morrison SF Central efferent pathwaysmediating skin cooling-evoked sympathetic thermo-genesis in brown adipose tissue Am J Physiol RegulIntegr Comp Physiol 2007292R127ndashR136
9 CaterinaMJ Transient receptor potential ion channelsas participants in thermosensation and thermoregula-tion Am J Physiol Regul Integr Comp Physiol 2007292R64ndashR76
10 Asahina M Sakakibara R Liu Z Ito T Yamanaka Yet al The raphe magnuspallidus regulates sweat secre-tion and skin vasodilation of the cat forepaw pad apreliminary electrical stimulation study Neurosci Lett2007
11 Labar DR Mohr JP Nichols FT3rd Tatemichi TKUnilateral hyperhidrosis after cerebral infarction Neu-rology 1988381679ndash1682
12 Korpelainen JT Sotaniemi KA Myllyla VV Asym-metric sweating in stroke a prospective quantitativestudy of patients with hemispheral brain infarctionNeurology 1993431211ndash1214
13 Kim BS Kim YI Lee KS Contralateral hyperhidrosisafter cerebral infarction Clinicoanatomic correlationsin five cases Stroke 199526896ndash899
14 Smith CD A hypothalamic stroke producing recurrenthemihyperhidrosis Neurology 2001561394ndash1396
15 Kloos RT Spontaneous periodic hypothermia Medi-cine (Baltimore) 199574268ndash280
16 LeWitt PA Newman RP Greenberg HS Rocher LLCalne DB Ehrenkranz JR Episodic hyperhidrosis hy-pothermia and agenesis of corpus callosum Neurol-ogy 1983331122ndash1129
17 Klein CJ Silber MH Halliwill JR Schreiner SASuarez GA Low PA Basal forebrain malformationwith hyperhidrosis and hypothermia variant of Shapi-rorsquos syndrome Neurology 200156254ndash256
18 Magnifico F Pierangeli G Barletta G et al Paroxys-mal episodic central thermoregulatory failure Neurol-ogy 2002581300ndash1302
19 Hirayama K Hoshino Y Kumashiro H Yamamoto TReverse Shapirorsquos syndrome A case of agenesis of cor-pus callosum associated with periodic hyperthermiaArch Neurol 199451494ndash496
20 Noel P Hubert JP Ectors M Franken L Flament-Durand J Agenesis of the corpus callosum associatedwith relapsing hypothermia A clinico-pathological re-port Brain 197396359ndash368
21 Darnell RB Arbit E Reversible diencephalic dysfunc-tion episodic hyperhidrosis due to a trapped third ven-tricle Neurology 199343579ndash582
1296 Neurology 69 September 18 2007
22 Tuettenberg J Woitzik J Siegel L Thome C Episodichypothermia and hyperhidrosis after subarachnoid hem-orrhage Case illustration J Neurosurg 200399610
23 De Tanti A Gasperini G Rossini M Paroxysmal epi-sodic hypothalamic instability with hypothermia aftertraumatic brain injury Brain Inj 2005191277ndash1283
24 Fukushima K Yasaki M Kaneko K et al Nonpara-neoplastic nonherpetic limbic encephalitis with severeepisodic hypothermia a case report Eur Neurol 200554170ndash174
25 Moulignier A Guiard-Schmid JB Gbadoe AH Rozen-baum W HIV-1-related spontaneous episodic hypo-thermia Neurology 200361418ndash419
26 Ruiz C Gener B Garaizar C Prats JM Episodic spon-taneous hypothermia a periodic childhood syndromePediatr Neurol 200328304ndash306
27 Johnson NC Morgan MW An unusual case of4-aminopyridine toxicity J Emerg Med 200630175ndash177
28 White KD Scoones DJ Newman PK Hypothermia inmultiple sclerosis J Neurol Neurosurg Psychiatry199661369ndash375
29 Edwards S Lennox G Robson K Whiteley A Hypo-thermia due to hypothalamic involvement in multiplesclerosis J Neurol Neurosurg Psychiatry 199661419ndash420
Neurology 69 September 18 2007 1297
DOI 10121201wnl0000275537716238e2007691293-1297 Neurology
Eduardo E BenarrochThermoregulation Recent concepts and remaining questions
This information is current as of September 17 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent69121293fullhtmlincluding high resolution figures can be found at
References
1httpwwwneurologyorgcontent69121293fullhtmlref-list-at This article cites 28 articles 19 of which you can access for free
Citations
icleshttpwwwneurologyorgcontent69121293fullhtmlotherartThis article has been cited by 4 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

hypothermia in many of these cases The episodesmay last variably between 30 minutes and 2hours recur several times daily without a clearprecipitating factor continue daily for severalweeks or months and then subside spontaneouslyor may be separated by long asymptomatic peri-ods lasting several months The causes and mech-anisms underlying PHH are heterogeneous andwith few exceptions largely unknown15 (table 1)This syndrome may rarely occur in associationwith agenesis of the corpus callosum (Shapirosyndrome)16 but callosal agenesis cannot explainthe syndrome as paroxysmal hyperthermia (re-verse Shapiro syndrome) may also occur in thiscondition19 In one autopsy case of Shapiro syn-drome there was neuronal loss in the infundib-
ular and premammillary nuclei of thehypothalamus20 but hypothalamic lesions havenot been documented in other cases PHH hasalso been described with basal forebrain le-sions17 acute hydrocephalus21 subarachnoidhemorrhage22 traumatic brain injury23 limbicencephalitis24 and in association with HIVinfections25However most cases of PHH arenot associated with detectable structural ab-normality or underlying disease
Paroxysmal hypothermia may occur in chil-dren some of them with history ofmigraine sug-gesting that PHH may be an example ofchildhood periodic syndrome associated with mi-graine26 It is conceivable that at least in somecases PHH may be a manifestation of a chan-nelopathy As discussed above there is in vitroevidence that voltage-gated K channels limit thefiring frequency of WS neurons Thus impairedactivity of these channels may result in an inap-propriate increase in WS firing and sweatingleading to hypothermia This possibility is sup-ported by a report of a patient who developed se-vere hypothermia and diaphoresis as aconsequence of accidental overdose of4-aminopyridine a drug that blocks voltage-gated K channels27 Hyperhidrosis in patientswith Morvan syndrome which may be associatedwith K channel antibodies could reflect similarmechanisms The importance of exaggeratedsweating as the cause of hypothermia in thesecases is supported by the beneficial effect of drugsthat block muscarinic cholinergic receptors ofsweat glands such as oxybutynin or glycopyrro-
Table 2 Neurochemical influences that affect activity of thermoregulatory preoptic hypothalamic neurons
Influence Effect Clinical implications (examples)
Serotonin (5-HT2receptor)
Hyperthermia Serotonin syndrome IL-1 induced feverantipsychotic-induced hypothermia
Serotonin (5-HT1receptor)
Hypothermia SSRI-induced sweatingdagger postoperative hypothermiahypoxia-induced hypothermia
Dopamine (D2 receptor) Hypothermia Bromocriptine-induced hypothermia neurolepticmalignant syndromeDagger
Norepinephrine ( 1receptor)
Hypothermia Isoflurane-induced hypothermia
Opioids
receptor Hyperthermia Fentanyl reduces shivering threshold during epiduralanesthesia
and receptors Hypothermia Hypothermia during opioid overdose
Acidosis Hyperthermia Heat shock
Prostaglandin E2 Hyperthermia Fever
Risperidone and other antipsychotic agents block 5-HT2 receptors and this could lead to hypothermiadaggerCyproheptadine may reduce SSRI-induced sweating presumably by blocking 5-HT1 receptorsDaggerThis disorder may reflect blockade of D2 receptors in the hypothalamusIL-1 interleukin 1 SSRI selective serotonin reuptake inhibitors
Table 1 Conditions associated with paroxysmalhypothermia
Congenital lesions
Agenesis of corpus callosum (Shapiro syndrome)
Basal forebrain malformation
Acquired disorders
Hemispheric stroke
Hypothalamic lesions
Traumatic brain injury
Multiple sclerosis
Acute hydrocephalus
Subarachnoid hemorrhage
Leigh syndrome
Limbic encephalitis
HIV infection
Neurology 69 September 18 2007 1295
late in ameliorating hypothermia in these pa-tients17 Other treatments that have been reportedto be effective in isolated cases include cyprohep-tadine (a nonselective serotonin receptorblocker) clonidine (an 2-receptor agonist)chlorpromazine (a D2 dopamine receptorblocker) and rarely antiepileptic drugs such asphenobarbital or phenytoin15 The lack of consis-tent response to these centrally acting drugs likelyreflect the multiplicity of neurochemical influ-ences that may affect thermoregulation at thelevel of the POA and manifest clinically with hy-pothermia or hyperthermia (table 2)
HYPOTHERMIA IN MS There are several reportsof hypothermia as a manifestation of MS bothduring acute relapses or chronically2829 Althoughhypothermia may reflect posterior hypothalamicinvolvement in MS in many cases no hypotha-lamic lesion is found The PAG is frequently af-fected in MS and involvement of this importantrelay of cold-response pathways may explain atleast some of the cases of hypothermia in this dis-order This is supported that the fact the PAG isalso typically affected in Wernicke encephalopa-thy a condition may also manifest withhypothermia
PERSPECTIVE There have been important ad-vances in basic science research on mechanisms ofthermoregulation but many questions regardingthe pathophysiology of human thermoregulatorydisorders still remain unanswered Neverthelessthese experimental studies provide insights andtestable hypotheses that may eventually lead tobetter therapeutic approaches to these challeng-ing disorders For example it could be hypothe-sized that acetazolamide which is effective in K
channelopathies such as episodic ataxia type 1 ortopiramate which is effective for migraine pro-phylaxis and also reduces sweat productioncould be considered as therapeutic options in pa-tients with PHH that do not respond to othertreatments Unfortunately the infrequent occur-rence of these groups of disorders makes it diffi-cult to design controlled therapeutic trials
REFERENCES1 Romanovsky AA Thermoregulation some concepts
have changed Functional architecture of the thermo-regulatory system Am J Physiol Regul Integr CompPhysiol 2007292R37ndashR46
2 Boulant JA Neuronal basis of Hammelrsquos model forset-point thermoregulation J Appl Physiol 20061001347ndash1354
3 Nagashima K Nakai S TanakaM Kanosue K Neuro-nal circuitries involved in thermoregulation AutonNeurosci 20008518ndash25
4 Mekjavic IB Eiken O Contribution of thermal andnonthermal factors to the regulation of body tempera-ture in humans J Appl Physiol 20061002065ndash2072
5 McAllen RM The cold path to BAT Am J PhysiolRegul Integr Comp Physiol 2007292R124ndashR126
6 Dimicco JA Zaretsky DV The dorsomedial hypothal-amus a new player in thermoregulation Am J PhysiolRegul Integr Comp Physiol 2007292R47ndashR63
7 Yoshida K Konishi M Nagashima K Saper CB Kano-sue K Fos activation in hypothalamic neurons duringcold or warm exposure projections to periaqueductalgray matter Neuroscience 20051331039ndash1046
8 Nakamura K Morrison SF Central efferent pathwaysmediating skin cooling-evoked sympathetic thermo-genesis in brown adipose tissue Am J Physiol RegulIntegr Comp Physiol 2007292R127ndashR136
9 CaterinaMJ Transient receptor potential ion channelsas participants in thermosensation and thermoregula-tion Am J Physiol Regul Integr Comp Physiol 2007292R64ndashR76
10 Asahina M Sakakibara R Liu Z Ito T Yamanaka Yet al The raphe magnuspallidus regulates sweat secre-tion and skin vasodilation of the cat forepaw pad apreliminary electrical stimulation study Neurosci Lett2007
11 Labar DR Mohr JP Nichols FT3rd Tatemichi TKUnilateral hyperhidrosis after cerebral infarction Neu-rology 1988381679ndash1682
12 Korpelainen JT Sotaniemi KA Myllyla VV Asym-metric sweating in stroke a prospective quantitativestudy of patients with hemispheral brain infarctionNeurology 1993431211ndash1214
13 Kim BS Kim YI Lee KS Contralateral hyperhidrosisafter cerebral infarction Clinicoanatomic correlationsin five cases Stroke 199526896ndash899
14 Smith CD A hypothalamic stroke producing recurrenthemihyperhidrosis Neurology 2001561394ndash1396
15 Kloos RT Spontaneous periodic hypothermia Medi-cine (Baltimore) 199574268ndash280
16 LeWitt PA Newman RP Greenberg HS Rocher LLCalne DB Ehrenkranz JR Episodic hyperhidrosis hy-pothermia and agenesis of corpus callosum Neurol-ogy 1983331122ndash1129
17 Klein CJ Silber MH Halliwill JR Schreiner SASuarez GA Low PA Basal forebrain malformationwith hyperhidrosis and hypothermia variant of Shapi-rorsquos syndrome Neurology 200156254ndash256
18 Magnifico F Pierangeli G Barletta G et al Paroxys-mal episodic central thermoregulatory failure Neurol-ogy 2002581300ndash1302
19 Hirayama K Hoshino Y Kumashiro H Yamamoto TReverse Shapirorsquos syndrome A case of agenesis of cor-pus callosum associated with periodic hyperthermiaArch Neurol 199451494ndash496
20 Noel P Hubert JP Ectors M Franken L Flament-Durand J Agenesis of the corpus callosum associatedwith relapsing hypothermia A clinico-pathological re-port Brain 197396359ndash368
21 Darnell RB Arbit E Reversible diencephalic dysfunc-tion episodic hyperhidrosis due to a trapped third ven-tricle Neurology 199343579ndash582
1296 Neurology 69 September 18 2007
22 Tuettenberg J Woitzik J Siegel L Thome C Episodichypothermia and hyperhidrosis after subarachnoid hem-orrhage Case illustration J Neurosurg 200399610
23 De Tanti A Gasperini G Rossini M Paroxysmal epi-sodic hypothalamic instability with hypothermia aftertraumatic brain injury Brain Inj 2005191277ndash1283
24 Fukushima K Yasaki M Kaneko K et al Nonpara-neoplastic nonherpetic limbic encephalitis with severeepisodic hypothermia a case report Eur Neurol 200554170ndash174
25 Moulignier A Guiard-Schmid JB Gbadoe AH Rozen-baum W HIV-1-related spontaneous episodic hypo-thermia Neurology 200361418ndash419
26 Ruiz C Gener B Garaizar C Prats JM Episodic spon-taneous hypothermia a periodic childhood syndromePediatr Neurol 200328304ndash306
27 Johnson NC Morgan MW An unusual case of4-aminopyridine toxicity J Emerg Med 200630175ndash177
28 White KD Scoones DJ Newman PK Hypothermia inmultiple sclerosis J Neurol Neurosurg Psychiatry199661369ndash375
29 Edwards S Lennox G Robson K Whiteley A Hypo-thermia due to hypothalamic involvement in multiplesclerosis J Neurol Neurosurg Psychiatry 199661419ndash420
Neurology 69 September 18 2007 1297
DOI 10121201wnl0000275537716238e2007691293-1297 Neurology
Eduardo E BenarrochThermoregulation Recent concepts and remaining questions
This information is current as of September 17 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent69121293fullhtmlincluding high resolution figures can be found at
References
1httpwwwneurologyorgcontent69121293fullhtmlref-list-at This article cites 28 articles 19 of which you can access for free
Citations
icleshttpwwwneurologyorgcontent69121293fullhtmlotherartThis article has been cited by 4 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

late in ameliorating hypothermia in these pa-tients17 Other treatments that have been reportedto be effective in isolated cases include cyprohep-tadine (a nonselective serotonin receptorblocker) clonidine (an 2-receptor agonist)chlorpromazine (a D2 dopamine receptorblocker) and rarely antiepileptic drugs such asphenobarbital or phenytoin15 The lack of consis-tent response to these centrally acting drugs likelyreflect the multiplicity of neurochemical influ-ences that may affect thermoregulation at thelevel of the POA and manifest clinically with hy-pothermia or hyperthermia (table 2)
HYPOTHERMIA IN MS There are several reportsof hypothermia as a manifestation of MS bothduring acute relapses or chronically2829 Althoughhypothermia may reflect posterior hypothalamicinvolvement in MS in many cases no hypotha-lamic lesion is found The PAG is frequently af-fected in MS and involvement of this importantrelay of cold-response pathways may explain atleast some of the cases of hypothermia in this dis-order This is supported that the fact the PAG isalso typically affected in Wernicke encephalopa-thy a condition may also manifest withhypothermia
PERSPECTIVE There have been important ad-vances in basic science research on mechanisms ofthermoregulation but many questions regardingthe pathophysiology of human thermoregulatorydisorders still remain unanswered Neverthelessthese experimental studies provide insights andtestable hypotheses that may eventually lead tobetter therapeutic approaches to these challeng-ing disorders For example it could be hypothe-sized that acetazolamide which is effective in K
channelopathies such as episodic ataxia type 1 ortopiramate which is effective for migraine pro-phylaxis and also reduces sweat productioncould be considered as therapeutic options in pa-tients with PHH that do not respond to othertreatments Unfortunately the infrequent occur-rence of these groups of disorders makes it diffi-cult to design controlled therapeutic trials
REFERENCES1 Romanovsky AA Thermoregulation some concepts
have changed Functional architecture of the thermo-regulatory system Am J Physiol Regul Integr CompPhysiol 2007292R37ndashR46
2 Boulant JA Neuronal basis of Hammelrsquos model forset-point thermoregulation J Appl Physiol 20061001347ndash1354
3 Nagashima K Nakai S TanakaM Kanosue K Neuro-nal circuitries involved in thermoregulation AutonNeurosci 20008518ndash25
4 Mekjavic IB Eiken O Contribution of thermal andnonthermal factors to the regulation of body tempera-ture in humans J Appl Physiol 20061002065ndash2072
5 McAllen RM The cold path to BAT Am J PhysiolRegul Integr Comp Physiol 2007292R124ndashR126
6 Dimicco JA Zaretsky DV The dorsomedial hypothal-amus a new player in thermoregulation Am J PhysiolRegul Integr Comp Physiol 2007292R47ndashR63
7 Yoshida K Konishi M Nagashima K Saper CB Kano-sue K Fos activation in hypothalamic neurons duringcold or warm exposure projections to periaqueductalgray matter Neuroscience 20051331039ndash1046
8 Nakamura K Morrison SF Central efferent pathwaysmediating skin cooling-evoked sympathetic thermo-genesis in brown adipose tissue Am J Physiol RegulIntegr Comp Physiol 2007292R127ndashR136
9 CaterinaMJ Transient receptor potential ion channelsas participants in thermosensation and thermoregula-tion Am J Physiol Regul Integr Comp Physiol 2007292R64ndashR76
10 Asahina M Sakakibara R Liu Z Ito T Yamanaka Yet al The raphe magnuspallidus regulates sweat secre-tion and skin vasodilation of the cat forepaw pad apreliminary electrical stimulation study Neurosci Lett2007
11 Labar DR Mohr JP Nichols FT3rd Tatemichi TKUnilateral hyperhidrosis after cerebral infarction Neu-rology 1988381679ndash1682
12 Korpelainen JT Sotaniemi KA Myllyla VV Asym-metric sweating in stroke a prospective quantitativestudy of patients with hemispheral brain infarctionNeurology 1993431211ndash1214
13 Kim BS Kim YI Lee KS Contralateral hyperhidrosisafter cerebral infarction Clinicoanatomic correlationsin five cases Stroke 199526896ndash899
14 Smith CD A hypothalamic stroke producing recurrenthemihyperhidrosis Neurology 2001561394ndash1396
15 Kloos RT Spontaneous periodic hypothermia Medi-cine (Baltimore) 199574268ndash280
16 LeWitt PA Newman RP Greenberg HS Rocher LLCalne DB Ehrenkranz JR Episodic hyperhidrosis hy-pothermia and agenesis of corpus callosum Neurol-ogy 1983331122ndash1129
17 Klein CJ Silber MH Halliwill JR Schreiner SASuarez GA Low PA Basal forebrain malformationwith hyperhidrosis and hypothermia variant of Shapi-rorsquos syndrome Neurology 200156254ndash256
18 Magnifico F Pierangeli G Barletta G et al Paroxys-mal episodic central thermoregulatory failure Neurol-ogy 2002581300ndash1302
19 Hirayama K Hoshino Y Kumashiro H Yamamoto TReverse Shapirorsquos syndrome A case of agenesis of cor-pus callosum associated with periodic hyperthermiaArch Neurol 199451494ndash496
20 Noel P Hubert JP Ectors M Franken L Flament-Durand J Agenesis of the corpus callosum associatedwith relapsing hypothermia A clinico-pathological re-port Brain 197396359ndash368
21 Darnell RB Arbit E Reversible diencephalic dysfunc-tion episodic hyperhidrosis due to a trapped third ven-tricle Neurology 199343579ndash582
1296 Neurology 69 September 18 2007
22 Tuettenberg J Woitzik J Siegel L Thome C Episodichypothermia and hyperhidrosis after subarachnoid hem-orrhage Case illustration J Neurosurg 200399610
23 De Tanti A Gasperini G Rossini M Paroxysmal epi-sodic hypothalamic instability with hypothermia aftertraumatic brain injury Brain Inj 2005191277ndash1283
24 Fukushima K Yasaki M Kaneko K et al Nonpara-neoplastic nonherpetic limbic encephalitis with severeepisodic hypothermia a case report Eur Neurol 200554170ndash174
25 Moulignier A Guiard-Schmid JB Gbadoe AH Rozen-baum W HIV-1-related spontaneous episodic hypo-thermia Neurology 200361418ndash419
26 Ruiz C Gener B Garaizar C Prats JM Episodic spon-taneous hypothermia a periodic childhood syndromePediatr Neurol 200328304ndash306
27 Johnson NC Morgan MW An unusual case of4-aminopyridine toxicity J Emerg Med 200630175ndash177
28 White KD Scoones DJ Newman PK Hypothermia inmultiple sclerosis J Neurol Neurosurg Psychiatry199661369ndash375
29 Edwards S Lennox G Robson K Whiteley A Hypo-thermia due to hypothalamic involvement in multiplesclerosis J Neurol Neurosurg Psychiatry 199661419ndash420
Neurology 69 September 18 2007 1297
DOI 10121201wnl0000275537716238e2007691293-1297 Neurology
Eduardo E BenarrochThermoregulation Recent concepts and remaining questions
This information is current as of September 17 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent69121293fullhtmlincluding high resolution figures can be found at
References
1httpwwwneurologyorgcontent69121293fullhtmlref-list-at This article cites 28 articles 19 of which you can access for free
Citations
icleshttpwwwneurologyorgcontent69121293fullhtmlotherartThis article has been cited by 4 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

22 Tuettenberg J Woitzik J Siegel L Thome C Episodichypothermia and hyperhidrosis after subarachnoid hem-orrhage Case illustration J Neurosurg 200399610
23 De Tanti A Gasperini G Rossini M Paroxysmal epi-sodic hypothalamic instability with hypothermia aftertraumatic brain injury Brain Inj 2005191277ndash1283
24 Fukushima K Yasaki M Kaneko K et al Nonpara-neoplastic nonherpetic limbic encephalitis with severeepisodic hypothermia a case report Eur Neurol 200554170ndash174
25 Moulignier A Guiard-Schmid JB Gbadoe AH Rozen-baum W HIV-1-related spontaneous episodic hypo-thermia Neurology 200361418ndash419
26 Ruiz C Gener B Garaizar C Prats JM Episodic spon-taneous hypothermia a periodic childhood syndromePediatr Neurol 200328304ndash306
27 Johnson NC Morgan MW An unusual case of4-aminopyridine toxicity J Emerg Med 200630175ndash177
28 White KD Scoones DJ Newman PK Hypothermia inmultiple sclerosis J Neurol Neurosurg Psychiatry199661369ndash375
29 Edwards S Lennox G Robson K Whiteley A Hypo-thermia due to hypothalamic involvement in multiplesclerosis J Neurol Neurosurg Psychiatry 199661419ndash420
Neurology 69 September 18 2007 1297
DOI 10121201wnl0000275537716238e2007691293-1297 Neurology
Eduardo E BenarrochThermoregulation Recent concepts and remaining questions
This information is current as of September 17 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent69121293fullhtmlincluding high resolution figures can be found at
References
1httpwwwneurologyorgcontent69121293fullhtmlref-list-at This article cites 28 articles 19 of which you can access for free
Citations
icleshttpwwwneurologyorgcontent69121293fullhtmlotherartThis article has been cited by 4 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

DOI 10121201wnl0000275537716238e2007691293-1297 Neurology
Eduardo E BenarrochThermoregulation Recent concepts and remaining questions
This information is current as of September 17 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent69121293fullhtmlincluding high resolution figures can be found at
References
1httpwwwneurologyorgcontent69121293fullhtmlref-list-at This article cites 28 articles 19 of which you can access for free
Citations
icleshttpwwwneurologyorgcontent69121293fullhtmlotherartThis article has been cited by 4 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
![Neonatal Thermoregulation - University of · PDF fileNeonatal Thermoregulation Julia Petty. ... A care study. Journal of Neonatal Nursing. ... 5 Thermoregulation [Compatibility Mode]](https://img.pdfslide.us/doc/110x75/5aafe83f7f8b9a6b308de3c0/neonatal-thermoregulation-university-of-thermoregulation-julia-petty-a-care.jpg)

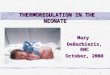














![Thermoregulation [compatibility mode] (1)](https://img.pdfslide.us/doc/110x75/58f0d50f1a28ab39538b45d7/thermoregulation-compatibility-mode-1.jpg)









