Embed Size (px)
Citation preview
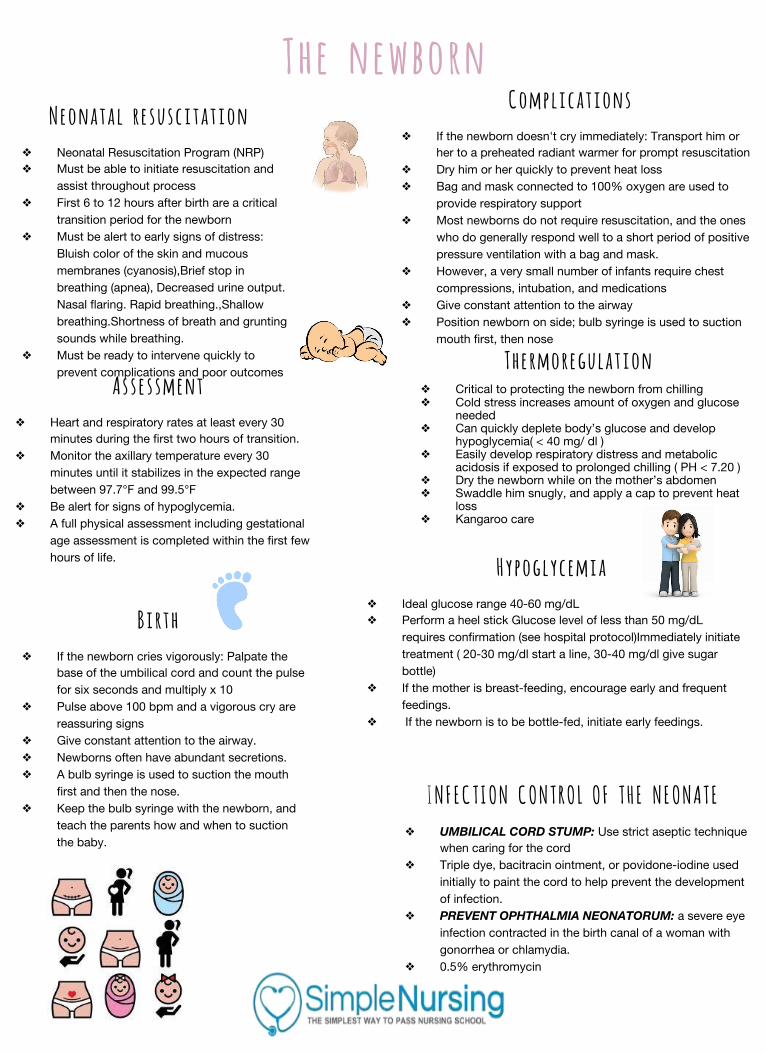
The newborn Neonatal resuscitation
❖ Neonatal Resuscitation Program (NRP)❖ Must be able to initiate resuscitation and
assist throughout process❖ First 6 to 12 hours after birth are a critical
transition period for the newborn❖ Must be alert to early signs of distress:
Bluish color of the skin and mucous membranes (cyanosis),Brief stop in breathing (apnea), Decreased urine output. Nasal flaring. Rapid breathing.,Shallow breathing.Shortness of breath and grunting sounds while breathing.
❖ Must be ready to intervene quickly to prevent complications and poor outcomes
Assessment ❖ Heart and respiratory rates at least every 30
minutes during the first two hours of transition.❖ Monitor the axillary temperature every 30
minutes until it stabilizes in the expected range between 97.7°F and 99.5°F
❖ Be alert for signs of hypoglycemia.❖ A full physical assessment including gestational
age assessment is completed within the first few hours of life.
Birth ❖ If the newborn cries vigorously: Palpate the
base of the umbilical cord and count the pulse for six seconds and multiply x 10
❖ Pulse above 100 bpm and a vigorous cry are reassuring signs
❖ Give constant attention to the airway.❖ Newborns often have abundant secretions.❖ A bulb syringe is used to suction the mouth
first and then the nose.❖ Keep the bulb syringe with the newborn, and
teach the parents how and when to suction the baby.
Complications ❖ If the newborn doesn't cry immediately: Transport him or
her to a preheated radiant warmer for prompt resuscitation❖ Dry him or her quickly to prevent heat loss❖ Bag and mask connected to 100% oxygen are used to
provide respiratory support❖ Most newborns do not require resuscitation, and the ones
who do generally respond well to a short period of positive pressure ventilation with a bag and mask.
❖ However, a very small number of infants require chest compressions, intubation, and medications
❖ Give constant attention to the airway❖ Position newborn on side; bulb syringe is used to suction
mouth first, then nose
Thermoregulation ❖ Critical to protecting the newborn from chilling❖ Cold stress increases amount of oxygen and glucose
needed❖ Can quickly deplete body’s glucose and develop
hypoglycemia( < 40 mg/ dl ) ❖ Easily develop respiratory distress and metabolic
acidosis if exposed to prolonged chilling ( PH < 7.20 ) ❖ Dry the newborn while on the mother’s abdomen❖ Swaddle him snugly, and apply a cap to prevent heat
loss❖ Kangaroo care
Hypoglycemia ❖ Ideal glucose range 40-60 mg/dL❖ Perform a heel stick Glucose level of less than 50 mg/dL
requires confirmation (see hospital protocol)Immediately initiate treatment ( 20-30 mg/dl start a line, 30-40 mg/dl give sugar bottle)
❖ If the mother is breast-feeding, encourage early and frequent feedings.
❖ If the newborn is to be bottle-fed, initiate early feedings.
INFECTION CONTROL OF THE NEONATE ❖ UMBILICAL CORD STUMP: Use strict aseptic technique
when caring for the cord❖ Triple dye, bacitracin ointment, or povidone-iodine used
initially to paint the cord to help prevent the development of infection.
❖ PREVENT OPHTHALMIA NEONATORUM: a severe eye infection contracted in the birth canal of a woman with gonorrhea or chlamydia.
❖ 0.5% erythromycin






![Neonatal Thermoregulation - University of · PDF fileNeonatal Thermoregulation Julia Petty. ... A care study. Journal of Neonatal Nursing. ... 5 Thermoregulation [Compatibility Mode]](https://img.pdfslide.us/doc/110x75/5aafe83f7f8b9a6b308de3c0/neonatal-thermoregulation-university-of-thermoregulation-julia-petty-a-care.jpg)



![Thermoregulation [compatibility mode] (1)](https://img.pdfslide.us/doc/110x75/58f0d50f1a28ab39538b45d7/thermoregulation-compatibility-mode-1.jpg)

















