Embed Size (px)
Citation preview

Therapeutics Initiative
A short history
James M Wright
March, 2016

Declaration
No financial competing interests.
Professor University of BC
Co-Managing Director of TI
Editor-in-Chief, Therapeutics Letter
Coordinating Editor, Cochrane Hypertension Group
Half-day a week outpatient Clinical Pharmacology
practice.

Therapeutics Initiative,
Founded1994(10 individuals)
Mission: To provide physicians and pharmacists with up-to-date, evidence-based, practical information on prescription drug therapy.
First Task: To become expert in assessing evidence from clinical trials of new drugs in Canada, and to provide the evidence to Pharmacare.
First policy decision: No conflicts of interest were allowed.

What happened? We became expert in critical appraisal and assessment
of evidence from clinical drug trials.
We got involved in the Cochrane Collaboration and learned their methodology.
We hired experts in Health Technology Assessment and Systematic Review.

Interventions implemented Therapeutics Letter 6 times per year posted on website
and mailed to physicians and pharmacists in BC.
Letters provided the best available evidence about the benefits and harms of drugs and drug classes.
Letters provided drug cost information.

What did the clinicians think about the Letter?
Answered by regular surveys


What was the impact on
prescribing of the first 20
Letters?Answered using a randomised controlled trial.

9
Effect of periodic letters on evidence-based
drug therapy on prescribing behaviour: a
randomized trial
Dormuth CR, Maclure M, Bassett K, Jauca C, Whiteside C,
Wright JM (CMAJ 2004; 171(9): 1057-61)
The Therapeutics Initiative is funded by a grant from the Government of British Columbia

10
Methods
Physicians:
-Study population included 499 physicians from 24 local health
areas in British Columbia, Canada
Communities:
-Paired according to the number of physicians.
-One in each pair was randomly assigned to the intervention
group and the other to the control group
Source databases:
-Physician service records and drug claims records from the
British Columbia Ministry of Health

11
Methods
Analyses:
-Incidence of newly treated patients was measured
-For each drug group studied, patients were classified as being newly treated if none of
the drugs in the group were dispensed to them in the previous year.

12
Results
Table: Characteristics of treatment and control physicians
Treatment Control
Characteristic Group (n=258) Group (n=241)
Physicians:
% General Practitioners 89.9 90.4
Average age 45.6 46.2
% Males/Females 89/11 83/17
Patients:
Average age 35.5 (75.2) 35.0 (75.3)
% Males/Females/Unknown 46/52/2 (44/52/4) 46/52/2 (44/52/4)
Avg. no. visits / MD 6402 (1322) 6660 (1340)
Results in brackets are for subset of patient population 65 and older.

13
Source: Dormuth CR, Maclure, et al. CMAJ 2004; 171(9): 1057-61

14
Interpretation
Printed letters distributed as a series regularly from a trusted
source has a modest desirable impact on prescribing to new
patients.
Further work needs to be done to determine the sustainability of
prescribing changes, and to determine what aspects of printed
letters elicit prescribing changes

What policies were implemented?
Outcomes based coverage.
Funding of new drugs was based on the best available evidence.
A new drug only became a full benefit if it represented a therapeutic advantage or a cost advantage over appropriate alternatives.
The TI assessed the evidence to determine whether there was a therapeutic advantage or disadvantage.

Examples of drug classes
affected by this policy
Non-steroidal anti-inflammatory drugs (Cox-2 selective NSAIDs).
Oral hypoglycemic drugs (glitazones and others).
Cholinesterase inhibitors for Alzheimers Disease.

Selective COX-2 inhibitors: Are they
safer? TL 39: Jan - Feb 2001
Conclusions
Patients on rofecoxib had less complicated and
symptomatic ulcers but more myocardial
infarctions than patients on naproxen.
COX-2 selective NSAIDs were associated with the
same incidence of serious adverse events as non-
selective NSAIDs.

New Drugs VI – Rosiglitazone
(Avandia®) TL 36: Jul-Aug 2000
Conclusion:
In patients with type 2 diabetes rosiglitazone
improves some surrogate markers and worsens
others.
Long-term trials are required to know whether this class
of drugs reduces morbidity and mortality outcomes.

Drugs for Alzheimer's DiseaseTL 56: Apr-Aug 2005
Conclusions
Donepezil has not been demonstrated to improve outcomes of
importance to patients and caregivers (e.g. institutionalization or
disability). Rivastigmine and galantamine have not been studied
for these outcomes.
AChE-I cause gastrointestinal, muscular, and other adverse effects
and likely increase serious adverse events.
There is no evidence that stopping AChE-I treatment is harmful.

What other policies were implemented?
Reference based pricing of equivalent drugs within a drug class.
Restricted access based on special authority criteria.
Therapeutic substitution

Reference based pricing January 1, 1997 least expensive ACE inhibitors fully
covered (captopril, quinapril, ramipril).
More expensive ACE inhibitors covered up to a maximum of $27 per month (benazepril, cilazapril, enalapril, fosinopril, lisinopril).
Patients on more expensive ACEI could pay the difference or switch.

Outcomes of reference pricing for angiotensin-
converting-enzyme inhibitors
Schneeweiss S, Walker AM, Glynn RJ, Maclure M, Dormuth C,
Soumerai SB.
N Engl J Med 2002;346:822-9

No increase in Emergency
Hospitalizations due to RP
23Schneeweiss et al. N Engl J Med 2002

Pharmacy savings
in prevalent ACEI users
$0
$10
$20
$30
$40
$50
$60A
pr-
96
May-9
6
Jun-9
6
Jul-96
Aug-9
6
Sep-9
6
Oct-
96
Nov-
96
Dec-9
6
Jan-9
7
Feb-9
7
Mar-
97
Apr-
97
May-9
7
Jun-9
7
Jul-97
Aug-9
7
Sep-9
7
Oct-
97
Nov-
97
Dec-9
7
Jan-9
8
Feb-9
8
Mar-
98
Apr-
98
Month
Av
era
ge
mo
nth
ly a
nti
-hy
pe
rte
nsiv
es
ing
red
ien
t e
xp
en
dit
ure
s p
er
pa
tie
nt
Projected pre-
policy trend
24
12 month savings:
$6,700,000
Schneeweiss et al. J Can Med Assoc, 2002

Reference pricing for ACEI conclusions
18% of patients switched to lower cost alternative.
Not associated with changes in physician visits, hospitalizations or mortality.
Cost savings to drug funder of approximately $6 million per year.

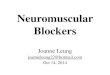
What was the impact of
these policies on drug
utilization and costs?

Source: Canadian Institute for Health Information, Drug Expenditure in Canada, 1985 to 2007 (Ottawa: CIHI, 2008)
$0
$50
$100
$150
$200
$250
$300
$350
$400
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Do
lla
rs p
er
Ca
pit
a
Year
Per Capita Pharmacare Spending on Prescription Drugs in Quebec and BC Before and After the UBCTherapeutics Initiative
Quebec
BC
Therapeutics Initiative established at the University of British Columbia (current cost = 23 cents per capita)

Canadian Rx atlas 2007
Overall per capita spending by province

Canadian Rx atlas 2007
Non-steroidal anti-inflammatory drugs

Canadian Rx atlas 2007
Oral diabetes drugs

Canadian Rx Atlas 2007
Cholinesterase inhibitors

How much did BC save on
prescription drug costs in 2007?TL 72: Nov-Dec 2008
If BC's drug utilization was the same as the Canadian average in 2007, total spending in our province would have been $701 million higher.
$455 million of this saving was due to BC residents purchasing fewer drugs, while $208 million reflects the savings from choosing lower-cost treatment options.

Why were the policies successful?
The TI did not allow any conflicts of interest.
Establishing questions for review was an iterative process.
Drug Assessment Working Group (DAWG) followed Cochrane methodology.
DAWG improved critical appraisal skills and assessing risk of bias over time.

Why were the policies successful?
Researchers were contracted to independently evaluate the impact on drug utilization and health outcomes.
Ministry of Health personnel remained committed to outcomes based coverage and other policies despite political pressures.

What did the TI team learn? All drugs with any effect have both benefits and harms.
Drugs are less effective than what we thought was true.
Drugs are more harmful than what we thought was true.
In many instances we were shocked that Health Canada had
approved the drugs for market.
In most instances drugs are marketed without knowing
that the benefits outweigh the harms in many if not all
the clinical settings where they are used.

Who were happy about this program?
Ministry of Health
Taxpayers
Most doctors
PATIENTS

Who were unhappy about the program?
The elephants.
Some doctors (specialists) who are friends of the elephants.

What should of happened? Expansion of the reference based program to new
classes of drugs eg. Statins.
Continued development of the international reputation of BC as a drug policy innovator.
Increased funding to the Therapeutics Intiative to increase the expertise and ensure the long-term future.

What Happened?In October 2007 a Pharmaceutical Task Force was announced by BC Health Minister with the following objectives:
1. Identify and strengthen patient care and choice;
2. Optimize the decision-making process for what drugs are covered under PharmaCare;
3. Improve the effectiveness of the Common Drug Review process;
4. Enhance the effectiveness, transparency and future role of the Therapeutics Initiative.

Nine member Pharmaceutical task force
Chair, Don Avison, President of the University Presidents Council. Board member LifeSciences BC.
Robert Sindelar, Dean, Faculty of Pharmaceutical Sciences, UBC. Board member LifeSciences BC.
Russell Williams, president of Canada’s Research-based Pharmaceutical Companies (Rx&D).
Susan Paish, Q.C., chief executive officer, PharmasaveDrugs (National) Ltd.
David M. Hall, chief compliance officer and senior vice president of Community Relations, AngiotechPharmaceuticals.
2 Ministry of Health members.
2 others.

PSF recommendations for TIApril 2008
#4 The Ministry of Health should establish a new Drug Review Resource Committee to carry out the drug submission review role currently performed by the Therapeutics Initiative.
#12 Subject to Recommendation #4, if the Therapeutics Initiative is maintained, action must be taken in the following areas: improve the governance, membership and accountability standards; renew and revitalize the panel of expert reviewers;

The Minister of Health accepted all the recommendations of the Pharmaceutical Task
Force and set up a mechanism for their implementation.

Academic review of TIhttp://www.pharmacology.ubc.ca/
3 member independent external panel reviewed the TI over 2 days in October 2008.
Validated the roles and activities of the TI in drug assessment, pharmacoepidemiology and education.
Recommendations:
Stable funding must be ensured. The present funding is inadequate.
3 new permanent University F-slots should be established.

What has happened? The TI’s advisory role to the BC Ministry of Health has
been severely curtailed.
The TI’s funding from the BC Ministry of Health was reduced to $550,000 per year for the Therapeutics Letter and Pharmacoepidemiology work.
The University has not created any new positions in response to the Academic Review recommendations.

What has happened? In November 2009, Don Avison confirmed that he was
recently appointed as the Canadian representative on Pfizer’s Global International Advisory Board. He did not respond to an e-mail asking what he will be paid.
Don Avison received a Leadership award from LifeSciences BC for his role as Chair of the Pharmaceutical Task Force.

What has happened? In the spring of 2012 an investigation into data access
was initiated by the BC Ministry of Health.
In June, 2012, TI data access was cut off as a result of the investigation.
In October, 2012, TI funding was suspended by the Ministry as a result of the investigation.
In October, 2013, the Ministry of Health announced that TI funding and data access be restored.

What has happened? We have been able to renew publication of the
Therapeutics Letter.
The Educational Working Group has become active delivering educational programs around the province.
It has been difficult to reestablish the full activity of the Drug Assessment Working Group because of loss of key people, decreased funding and loss of most of the function as advisor to Pharmacare.

What has happened? TI data access to allow independent exploration of data
utilization and independent research has not been reestablished.
A contract management committee oversees all activities and spending of the TI.
All attempts to negotiate increased funding and activities of the TI have been unsuccessful so far.
Funding for Cochrane Canada and the Cochrane Hypertension Group at UBC ended Sept. 2015.


Therapeutics Initiative website www.ti.ubc.ca
97 Therapeutics Letters
>30 Drug Assessment reports
References to the Pharmacoepidemiology published
papers.
Educational events, podcasts and more.

Questions????