Embed Size (px)
Citation preview

unesp
Daniela Ponce
Therapeutic Modalities: CRRT, SLED, PD
PD
BOTUCATU SCHOOL OF MEDICINE, SAO PAULO STATE, BRAZIL
16 th CRRT, San Diego, California 2011

Case Study
A 55-year-old man was victim to a massive attack by Africanized bees (>500 beestings) in a rural area in Sao Paulo, Brazil.
Day 1: On admission to hospital, widespread erythematous and painful papuleswere found on his body and he was discharged from the hospital after oralmedication.
Day 6: He was admitted to a emergency medical assistance, complaining ofedema, urine volume reduction and weakness. No laboratory evaluation wasperformed and he was discharged from hospital.
Day 10: The patient was tranferred from another hospital 24 h after admissionfor high volume vomit, urine volume decrease and altered mental status. On PE hewas somnolent, emaciated 2, pale, BP= 160/100 mmHg, HR= 105 per minute andhis lungs with basilar rales (sat=90% in spontaneuos ventilation). The otheraspects of the PE were unremarkable.

• His blood laboratory examination showed haematocrit 16%;haemoglobin, 5.9 g/dl, serum creatinine 27 mg/dl; blood ureanitrogen, 221 mg/dl; serum potassium, 7.8 mEq/l, serum pH 7.15,bic 5, total CO2 18 mmol/L.
• He was transferred to the Intensive Care Unit (ICU) andsupportive measures were started (transfusion, oxygen therapyand bicarbonate)
• APACHE 2 = 15.6 ATN-ISS= 0.41
• output urine after 6 h = 40 ml
• We are asked to evaluate him at the same day because of labexams and low urine output

Start dialylis now
Volume overload
Metabolic acidosis
Hyperkalemia
Uremic state
Which dialysis method ?
CRRT SLED iHD PD

Continuous PD using a flexible catheter and a cycler was performed
24 hours 19 cycles 2 liters/cycle 1.5% glucose
Clinical and lab improvements were observed after 2 days oftreatment, but diuresis recovery was recorded only 20 days
PD was interrupted after 23 days
Seventy-one days after the attack he had full recovery of renalfunction

1- Is it used?
2- Why to indicate it ?
3- For whom?
4- How to prescribe it?
5- Which is the ideal dose ?
6- Is it better or worsen than other methods?
7- What is the real role of PD in AKI?
Peritoneal Dialysis in AKI

BEST Study * Latin America *0
20
40
60
80
100 %
Europe **
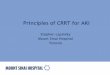
1. Is it used ?
CRRTHD
SLEDPD
* Uchino. JAMA, 2005** Ricci. NDT, 2006
SLANH***: 35% in Latin America
*** Lombardi. WCN 2007

0
20
40
60
80
1997 1998 1999 2000
HC - SP
Lima EQ. ASN, 2002
% %
HD PD CRRT
Botucatu School
Barretti P. Renal Failure, 1997Balbi AL. JBN, 2002. Balbi AL. No published
Methods of dialysis in Brazil
PD is still usedfor AKI despiteconcerns aboutits inadequacy
0
20
40
60
80
1997 2004 2006 2008 2009 2010

1- Is it used?
2- Why to indicate it ?
3- For whom?
4- How to prescribe it?
5- Which is the ideal dose ?
6- Is it better or worsen than other methods?
7- What is the real role of PD in AKI?
Peritoneal Dialysis in AKI

• simple technique
• no anticoagulation
• low risk of bleeding
• hemodynamically unstable patients
• low risk of electrolyte disorders
• less expansive than CRRT
Advantages of PD
2. Why ?

Advantages and disavantages
For a selected group of AKI

1- Is it used?
2- Why to indicate it ?
3- For whom?
4- How to prescribe it?
5- Which is the ideal dose ?
6- Is it better or worsen than other methods?
7- What is the real role of PD in AKI?
Peritoneal Dialysis in AKI


utilizar solamente em algunassituaciones hemodinâmicas
no utilizar en el catabolismo severo
Choice of dialysis method in AKI
Withoutindication
• recent abdominal or cardiothoracic surgery
• severe hyperkalemia
• severe respiratory failure
PD
• Indications and contra-indications for each method
• hemodinamic stability and hypercatalism
• nephrology experience
Unstable hemodinamic and
hypercatabolic patients?¿
No use in very unstable patients
No use in severe hypercatabolic patients

Our patient
Volume overloadMetabolic acidosis
HyperkalemiaUremic state
no respiratory failureno changes in ECGno recent surgeriesno unstable hemodinamicallysevere hypercatabolic
can be treated with PD

1- Is it used?
2- Why to indicate it ?
3- For whom?
4- How to prescribe it?
5- Which is the ideal dose ?
6- Is it better or worsen than other methods?
7- What is the real role of PD in AKI?
Peritoneal Dialysis in AKI

For decreasing complications
and improving efficciency
• flexible catheter (1 o 2 “cuffs”)
• automated method - cycler
• continuous DP

Fast exchanges h/h,sessions of 16-20 hs,2-3xx/weekly
exchanges with dweltime longer (2-6 hs)
Fast exchanges (30 min)during 8-10 hs, withresidual volum (0.5-1 l) (>solut3 clearance)
HVPD
Fast exchanges(h/h), sessions of24 h, 7xx a week


Dialysis protocols for CPD

Metabolic control and fluid balance
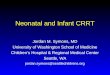
Gabriel DP. PDI, 2007

Creatinine clearance/session (ml/min) 15.8 ± 4.16Urea nitrogen clearance/session (ml/min) 17.3 ± 5.01
Prescribed Kt/V
per session 0.65
weekly 4.5
Delivered Kt/V
per session 0.55 ± 0.12a a
weekly 3.85 ± 0.62a a
Solute Reduction Index (%) 41 ± 9.9
a= p>0.05 from prescribed Kt/V
Variable Median ± SD
Dialysis dose parameters

17%
7%
86%
23%
13%
7%
57%
Complications Outcome
no complications peritonitis
mechanical
death
recovery
no recoverymethod change
CPD is an effective methodfor treating AKI patients

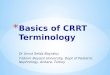
Our patient
• Continuous PD: 24 h
• High Volume PD: 38 l
• Cycler
• Flexible catheter
• There are not complications: mechanic, metabolic, infectious

Cr levels mg /dl
BUN levels mg /dl
Urine output ml/day
tempo em dias
tempo - dias
-50
50
150
250
0
2000
4000
6000
0 20 40 60 80
0
10
20
30
Follow up

Prescribed Kt/V = 0.65
K=? volume of dialysis solution prescribed in 24 hours (mL) _ 0.60 (considering the D/P relationship for dwel time between 30 and 60 min)
t = 1 treatment duration (24 h = 1 day)
V = 35l patient urea distribuition volume (Watson formule)
Weigh = 76 kg (estimated 8 kg of edema) 68 kg V = 35 l K=38 l
The number of dialysis solution exchanges in 24 hours was obtained by dividingthe K value by 2 L (infusion volume)
Total duration of 1 session: 24 hoursInflow time = 10 minOutflow time= 20 minDwell time= 45 mimGlicose concentration = 1.5 %total exchanges/session= 19Total dialysate volume= 38 lFlow rate= 26.4 ml/min
Prescription
Our patient

Calcutating Peritoneal Dialysis Dose:
Delivered Kt/V
Kt/V = [mean dialysate urea nitrogen (mg/dL) / mean serum urea nitrogen
pre andpost dialysis (mg/dL)] _ [drained 24-hour volume (mL) /patient urea
distribution volume (mL)].

Dialysis dose
delivered Kt/V UF (ml) BF (ml) session weekly session day
0,54 4,2 1170 +8800,57 4,5 1350 +6550,61 1480 +3200,63 1765 -3400,61 2205 -10900,64 2800 -18800,62 3050 -20170,64 2785 -21800,63 2240 -21900,62 2030 -18900,65 1975 -30500,64 1030 -27500,62 910 -1470

1- Is it used?
2- Why to use it ?
3- For whom?
4- How to prescribe it?
5- Which is the ideal dose ?
6- Is it better or worsen than other methods?
7- What is the real role of PD in AKI?
Peritoneal Dialysis in AKI

Ideal dialysis dose in AKI is controversial
There are not studies that evaluated the effects ofdifferent PD doses on outcome of AKI patients

• prospective and randomized study in India
• evaluated two modes of automatic PD (CPD and tidal)
• 87 patients with AKI and no severe catabolism
Total volume of dialysate per session was similar in two groups: 26 l

Results and conclusions
Pre-dialysis BUN (mg/dL) 77.9 ± 22.1 78.8 ± 8.3 0.67
Post-dialysis BUN (mg/dl) 64.7 ± 12.4 50.8 ± 11.3 0.04
KT/V (session) 0.26 ± 0.07 0.34 ± 0.14 0.001
(week) 1.8 ± 0.32 2.43 ± 0.87 0.001
SRI (%) 20.6 ± 6 28.4 ± 4 0.02
UF (L/session) 2.01 ± 0.28 2.88 ± 0.7 0.03
Total protein loss (g/session) 6.6 ± 1.2 10.5 ± 1.5 0.001
Albumin loss (g/session) 3.48 ± 2.1 6.32 ± 1.03 0.02
CPD TPD p
“Both CPD and TPD are reasonable options for mil-moderate hyper catabolic ARF. TPDprovides better clearances at the same volume. Higher protein loss in TPD was the only
limitation to its use in ARF.”

Prospective study with different doses of CPD (flexible catheter , cycler, 24 h 7 x a week)
Patients with AKI of ATN were randomly assigned to receive:
Lower intensity PD: prescribed Kt/V = 0.5 (n=60)
Higher intensity PD: prescribed Kt/V=0.8 per session (n=60)
In press
To evaluatevaluate thethe effectseffects ofof differentdifferent PD doses PD doses onon outcomeoutcome ofof AKI AKI patientspatients
This study was early interrupted because group assigned to higher intensitydialysis received lower dialysis dose than that prescribed.
Ponce D, Abrão JMG, Berbel MN, André Luis Balbi

Ä
Table 1. Peritoneal Dialysis session characteristics
Ä
Characteristics Lower intensity Higher intensity
Kt/V=0.5 Kt/V=0.8
Ä
Dialysate fluid/cycle (l) 2.0 2..0
Inflow time (min) 10 10
Outflow time (min) 20 20
Dwell time (min) 45°©60 30-45
Duration /cycle (min) 75-90 60-75
Total exchanges/session 16-19 20-24
Total dialysate volum/session 32-38 40-48
Total duration of session (h) 24 24
Flow rate mL/minute 22-26.5 27.8-33.3
Glucose (%) 1.5-4.25 1.5-4.25Ä
Ä
Ä
Ä
Ponce D, Abrão JMG, Berbel MN, Balbi AL

Patients Characterísticss
Characteristics Higher Lower p (n=31) (n=30)
Male (%) 71 65 0.58
Age (years) 64.2 ± 18.8 62.8 ± 16.2 0.32
Oliguria (%) 56 58 0.78
ATN-ISS 0.67 0.66 0.48
APACHE II 26.4 ± 6.9 24.8 ± 8.6 0.18
Sessions (number) 6.1 5.7 0.48
Pre BUN (mg/ 100 ml) 118.8± 32.6 114.2±34.8 0.78
Pre creat (mg/100 ml) 5.6 ± 1.9 5.8 ± 1.4 0.79
Cause of AKI (%)
Sepsis 48 50 0.77
Heart failure 25 22 0.58
Post-surgery 11 14 0.65
Etiology of ATN (%)
Ischemic 82 78 0.38
Mixed 16 20 0.61
Indication of dialysis (%)
Azotemia 64 66 0.78
Volume overload 20 18 0.84
Ponce D, Abrão JMG, Berbel MN, Balbi AL
Higher Lower p n=31 n=30
KT/V per session:
prescribed 0.8 0.5
delivered 0.59±0.1a 0.43±0.1 0.03weekly:
prescribed 5.6 3.5delivered 4.13±0.6a 3.43±0.2 0.03
UF per session (L) 2.41 ± 0,7 2.11 ± 0.6 0.42
a Significantly different from prescribed Kt/V (p=0.04)
Table 03. Weekly and per Session Kt/V and UKF inPatients undergoing higher and lower intensity PD dose

0
20
40
60
80
100
120
140
BUN
(mg/
dl)
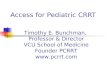
a. BUN (mg/dl)
0
1
2
3
4
5
6
7
Cr (m
g/dl
)
0
5
10
15
20
25
0
1
2
3
4
5
6
b. Creatinine (mg/dl)
c. Bicarbonate (mEq/L)d. Potassium (mEq/L)
Figure 3. Comparison of metabolic control in higher and lower-intensity peritoneal dialysis dose. Median serum levels of (a) BUN, (b)creatinine, (c) bicarbonate, (d) potassium, at the beginning of treatment and after each session.
Control metabolico

Table 4. Outcomes according to treatment group
Higher Lower p value (n=31) (n=30)
Mortality (%) 55 53 0.83Recovery of kidney function (%)* 86 86 0.97Duration of treatment (days) 6.1± 2.7 5.7 ± 2.1 0.42
* Recovery and resolution of kidney function of survivors only
Fig 2. Comparison patient survival after 30 days treatment
Ponce D, Abrão JMG, Berbel MN, Balbi AL

Conclusion
This study showed that increasing the intensity of continuous HVPD does not: :
reduce mortality or dependence on dialysis improve metabolic control among critically ill patients.
Peritoneal clearance is limited by: dialysate flow, membrane permeability, and area (KoA)
leading to a maximum delivered Kt/V of 0.6 per session
It suggests that prescribed Kt/V of 0.5 per session is enough to get a satisfactorymetabolic control and patient outcome
Ponce D, Abrão JMG, Berbel MN, Balbi AL

1- Is it used?
2- Why to use it ?
3- For whom?
4- How to prescribe it?
5- Which is the ideal dose ?
6- Is it better or worsen than other methods?
7- What is the real role of PD in AKI?
Peritoneal Dialysis in AKI


• prospective and randomized study
• 2 groups: 70 patients (PD = 36 and HF= 34)
• protocol was discontinued: mortality rate > PD (RR=3.2)
N Engl J Med 2002;347:895-902

Observations regarding results
PD
• rigid catheters
• manual exchanges
• dwell time < 15 min (70 l/day)
• no dialysis dose quantification
Daugirdas. NEJM, 2002Rao. PDI, 2003
Is not PD indicated in AKI ?

Kid Int (2008) 73,S87-S93




PD DHD p
KT/V per session:
prescribed 0.65 1.2delivered 0.53 0.79 <0.01
weekly:prescribed 4.5 7.2delivered 3.51 4.8 <0.01
UFper session (L) 2.1 ± 0,7 2.4 ± 0,7 0.39
Complications (%)infectious 18 8.5 0.21mechanical 5 18 0.13

30,0025,0020,0015,0010,005,000,00
Time ( days)
1,0
0,8
0,6
0,4
0,2
0,0
Su
rviv
al
(%)
DHD
HVPD
p = 0.48
Sobrevida en 30 días


High Volume PD x Extended Daily Hemodialysis in patients with AKI
AL Balbi, GA Brito, JMG Abrão, M Pinto, D Ponce
University Hospital, Botucatu School of Medicine, São Paulo, Brazil, 2008
• Prospective randomized trial
• 180 hemodynamically unstable AKI patients treated with HVPD or EDH
• Objectives are evaluate death within 60 days
recovery of kidney function metabolic control
From now: 64 patients in SLED and 48 patients in HVPD
Further Studies

HVPD (48)SLED (64)Characteristics
Male (%) 70.1 70.8
age (years) 66.8 ± 10 58.9 ± 18
ATN-ISS (media) 0.63 0.72
Ischemic AKI (%) 89 83
BUN (mg/dl) 91 ± 30 96 ± 25
creatinine (mg/dl) 4.8 ± 1.5 5.7 ± 3.2
Table 1: Characteristics of patients
High Volume PD x Extended Daily Hemodialysis in patients with AKI
AL Balbi, GA Brito, JMG Abrão, M Pinto, D Ponce
mortality Recovery renalfunction (survival)
0
25
50
75
100%
76,1%
69,6%
81%87%
SLED HVPD
p>0.05
Mortality rate and recovery of renal function
HVPD and EDH can be effective and similar methods
for treating AKI patients
Conclusion

1- Is it used?
2- Why to use it ?
3- For whom?
4- How to prescribe it?
5- Which is the ideal dose ?
6- Is it better or worsen than other methods?
7- What is the real role of PD in AKI?
Peritoneal Dialysis in AKI

it is an important therapeutic alternative for a selected group of patients, manly in developing countries
to overcome limitations, it must be carried in continuous and
automatic method with high volume of dialysate
prescription should be individual to achieve adequate solute and
fluid control
Kt/V =0.5 per session seems to be enough
There is room for a more frequent use of PD in AKI
In press
Ponce D, Balbi AL
Peritoneal Dialysis in Acute Kidney Injury: a Viable Alternative

André Luis Balbi
Germana Alves de Brito
Juliana Gera Abrão
Marina Nogueira Berbel
Milene Perón Rodrigues
Laudilene R Marinho
Cibele T. P. Almeida
Andréa V. Hecker
Elza Maria Januário
Ana Cristina Paulino Leite
BOTUCATU SCHOOL OF MEDICINE, SAO PAULO STATE, BRAZIL