Embed Size (px)
Citation preview
The author describes methods o j handling medication in resistant patzents. He shows us how such methods can aid psychiatrists and nonmedical staf in collaborating against barriers to eJective treatment.
Therapeutic Aspects of Medication Management
Tim Burton
Because of a number of factors, including inappropriate training, financial cutbacks, and interprofessional tensions, community mental health centers (CMHCs) are experiencing increasing difficulty in providing effective and frugal services. Although CMHCs cannot alter these forces, they can attenuate them. To do so, however, requires interprofessional coordination or team- work. Although the importance of coordination has been acknowledged (Lamb, 1971), specific methods for achieving it are not often described (Fir- man, 1982) in the literature. This chapter describes how a community mental health center in north central Oregon developed a collaborative and synergis- tic method for prescribing psychotropic medications, an important aspect of the typical psychiatrist’s consultation role. Such methods are needed to reverse the trend toward decreased psychiatric involvement in the public mental health sector (Lazare and others, 1972; Sharfstein, 1978).
Development of the Method
In 1973, after arriving in Hood River, a rural county of 14,000 people, the author began serving the local community mental health center and quickly established a norm for medicating patients: The case manager (primary thera- pist) must always be present. The results of setting this norm were immedi- ately apparent. One effect was that the case manager’s psychotherapeutic
D. L Curler (Ed ). E f ~ f t w Af tze ic for the 1980~ New Directions far Mental Health Services. no. 19 San Francisco: Joscy-Bass, September 1983 85

86
leverage multiplied. When psychiatrist, case manager, and patient- frequently his family network as well - gathered together, the meeting was found to have elements similar to those of the retribalization phenomenon described by Speck and Attneave (1973). The group ritual aspects of these meetings seemed to be important, so we named the meetings consultation ceremonies. We have used such ceremonies to reinforce norms already established at previous case manager-patient sessions. If nonproductive patterns developed (particularly transference-countertransference patterns, we found that they could he changed by what might he called directive theme interference reduction (Caplan, 1970). When the case manager simply did not understand or lacked necessary skills, the psychiatrist demonstrated appropriate treatment techniques so that the course of subsequent therapy could he shaped to solve problems more effi- ciently. All these interventions depend, of course, on the psychiatrist’s capacity to function as a consultant with a multidimensional perspective.
Theory
Problems can be viewed as pathogenic event patterns entangling mul- tiple levels of the patient’s biopsychosocial existence. Multiple coordinated interventions are required to disrupt them and to establish new patterns. Typically, pathogenic vicious cycles include distorted perceptions, irrational assumptions, maladaptive behavior, dysfunctional symptoms, and inappro- priate environmental responses, which all feed back to perpetuate the patient’s distorted perceptions.
Medications act to disrupt such cycles by altering symptoms. Since medications are active only on the biological level, they are often augmented with interventions on the psychological and social levels. The method uses framing and counterprojection as well as network restructuring to disrupt vicious cycles and to initiate and maintain virtuous cycles consisting of clear perceptions, rational assumptions, adaptive behavior, creativity, and congru- ent environmental responses.
Frunting. Framing is a familiar technique that healers and many others have known and used for centuries. For example, Tom Sawyer’s tactic of per- suading his friends that whitewashing his aunt’s fence was an artistic activity, not boring work, is classic. Watzlawick and others (1974, p. 95) provide a clear definition: “To reframe. . . means to change the conceptual and/or emo- tional setting and viewpoint in relation to which a situation is experienced and to place it in another frame which fits the ‘facts’ of the same concrete situation equally well or even better and thereby changes its entire meaning.” As we know, framing is an important aspect of hypnotic induction. For instance, to tell a patient that his uplifted arm feels heavy is to frame a naturally occurring event - fatigue - with words that shape the hypnotic experience so that the patient becomes more likely to use the hypnotist’s suggestions to shape his future behavior,
In the method that I am describing, framing is used to help patients

87
reorganize their life patterns by assigning a therapeutic meaning to medica- tions and to the interpersonal transactions associated with them. An example of assigning therapeutic meaning to medication is telling a patient who is about to receive a tricyclic antidepressant: “When your mouth begins to feel dry, it means that enough medication is being absorbed through your intes- tines to do the job we want it to do.” An example of assigning therapeutic meaning to interpersonal transactions associated with medication is when the consultation ceremony is set up to enhance the patient’s receptivity to the meaning assigned.
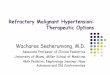
Counterprojection. Not all patients are receptive to beneficial framing. Some are preoccupied with worrisome fantasies aroused by the prospect of talking with a psychiatrist or taking pills. Indeed, the resulting anxiety can cause noncompliance, regression, and therapeutic impasses. In most cases of this nature, counterprojection is employed. Essentially, the counterprojection technique reduces the patient’s anxiety by clarifying and even neutralizing his distorted perceptions. In contrast to the usual psychoanalytic definition of projection as a mechanism of psychological defense, the definition here is interpersonal and derived from Sullivan’s term parataxic distortion. Parataxic distortion means that we perceive and respond to each other with a mixture of reality and fantasy (Sullivan, 1955). Under this definition, projections are distortions based on the patient’s historical experiences, particularly on the patient’s experiences with significant adult figures. Needless to say, some degree of counterprojection is necessary with almost every patient. Havens (1976) argues that interpersonal work with personality disorders consists pri- marily of counterprojection (see Figure 1).
A Structured Process
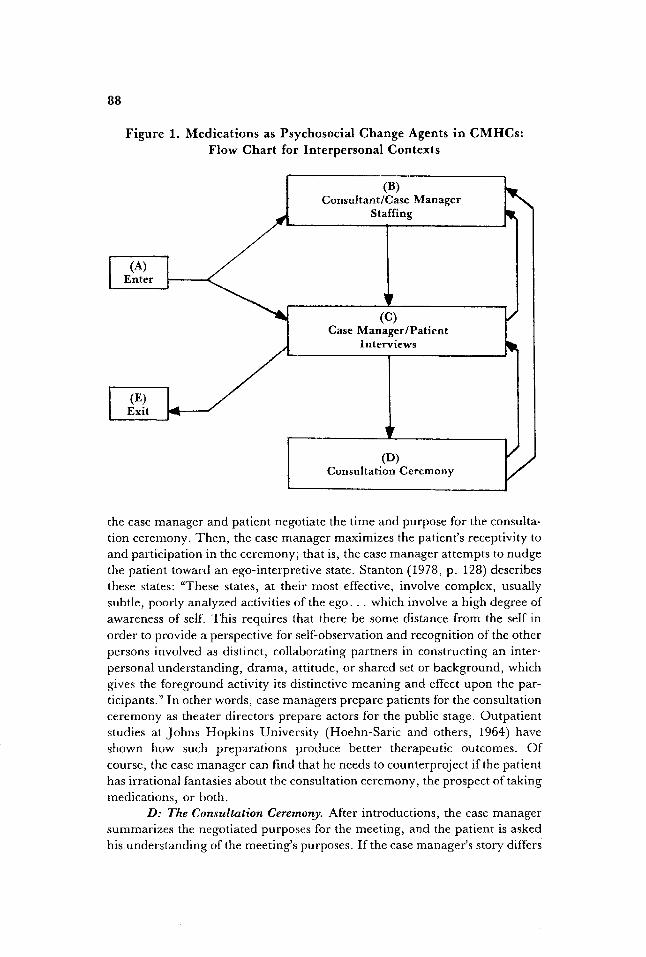
The interpersonal settings for shaping medication transactions are the consultation ceremony, the case manager-patient interviews, and the weekly all-staff meetings. These are diagrammed in Figure 1.
A: Entry. The issues of medications can arise in several ways: The patient can already be medicated, the patient can request medications, side effects can develop, and doses can need adjustment. Finally, the case manager can think that medications, consultation ceremonies, or both will be helpful.
B: Stafing. During the weekly staffing with other community mental health center personnel and the psychiatrist, strategies are devised to prepare the patient for the consultation ceremony, to introduce the topic of medica- tio‘n, and to counterproject if necessary. Family physicians frequently prescribe medications for community mental health center patients. In most instances, the psychiatrist and case manager plan a strategy and call the family physi- cian, apprise him of the plan, ask him to prescribe, and offer specific sugges- tions about the most appropriate medication and dose and about framing when he interviews the patient.
C: Case Manager-Client Interview. If medications are to be prescribed,
88
(4 Enter
Figure 1. Medications as Psychosocial Change Agents in CMHCs: Flow Chart for Interpersonal Contexts
(4 Enter
(E) Exit
t
the case manager and patient negotiate the time and purpose for the consulta- tion ceremony. Then, the case manager maximizes the patient’s receptivity to and participation in the ceremony; that is, the case manager attempts to nudge the patient toward an ego-interpretive state. Stanton (1978, p. 128) describes these states: “These states, at their most effective, involve complex, usually subtle, poorly analyzed activities of the ego. . . which involve a high degree of awareness of self. This requires that there be some distance from the self in order to provide a perspective for self-observation and recognition of the other persons involved as distinct, collaborating partners in constructing an inter- personal understanding, drama, attitude, or shared set or background, which gives the foreground activity its distinctive meaning and cffect upon the par- ticipants.” In other words, case managers prepare patients for the consultation ceremony as theater directors prepare actors for the public stage. Outpatient studies at Johns Hopkins University (Hoehn-Saric and others, 1964) have shown how such preparations produce better therapeutic outcomes. Of course, the case manager can find that he needs to counterproject if the patient has irrational fantasies about the consultation ceremony, the prospect of taking medications, or both.
D: The Consultation Ceremony. After introductions, the case manager summarizes the negotiated purposes for the meeting, and the patient is asked his understanding of the meeting’s purposes. If the case manager’s story differs

89
from the patient’s, the difference is discussed. This discussion reveals the patient’s preconceived ideas about medication. The patient self-observes and self-evaluates his participation in the previous decision, and therapeutic con- tinuity is preserved.
After any differences are resolved and the meeting’s purpose is clear, the psychiatrist typically says, “Tell me your symptoms” or asks such questions as, “How do they interfere with your life?” and “HOW have you tried to solve your problem?” Specific behavioral details are preferable to vague abstrac- tions, because vivid descriptions clarify the causal links between the patient’s social milieu; his feelings, behaviors, and thoughts; and his chemically treat- able symptoms. Detailed descriptions are preferred because they reveal the patient’s habitual language: his phraseology, metaphors, concepts. Using the patient’s own language, his semantic environment, makes negotiating a formu- lation of his problems easier. Reaching a mutually agreeable explanation for the patient’s problem seems essential, because a common understanding bridges the initial sharing of data and the subsequent medication framing. Negotiated explanations are particularly suited to chronic problems (Balint, 1957).
E: Exit. The client is discharged.
Case Examples
Four cases illustrate how this method has been applied to difficult patient problems.
Case 1. Mrs. L was a thirty-two-year-old woman who came to the community mental health center as a last resort. She complained of increas- ingly severe aches and pains all over her body, especially in the upper back and neck. Despite numerous medical workups showing no organic pathology, her suffering persisted for over a year.
After her psychodynamics and her personal language were understood, the following explanation was negotiated: “Your unassertiveness means that you cannot say no to your husband and children. This breeds frustration and anger. Because anger is unacceptable, you repress it, and your body then experiences chronic painful muscle tension, which has come to dominate your attention, making you feel more trapped and angry, causing more pain, and so on.” While she listened, her family physician was reached by telephone, and her problem was explained to him in greater physiological detail. Therapy consisted of discontinuing all previous medications and starting a low dose of neuroleptic. Drug therapy was framed as “helping you control your anger so you can learn to be more appropriately assertive.” The patient was also advised never to complain about pain to anyone, and she received assertivencss train- ing. She was discharged four months later, pain free and well.
Negotiating an explanation for this woman’s vicious cycle in words that she understood prepared her for framing designed to shift treatment from the medical arena to the more appropriate interpersonal therapy.
90
Case 2. Mr. R was a thirty-nine-year-old man who suffered from symptoms of agitation, inability to fall asleep, ruminations, depression, and social withdrawal. The precipitating event was his wife’s affair. The couple had been married for twenty-three years, and the patient suffered from an obsessive-compulsive anxiety disorder.
Marital therapy was started after initial evaluation, but therapeutic movement effectively stopped when defensive barriers escalated dramatically. Medications were indicated, yet the patient’s deprndence anxieties made him wary of taking pills. Thus, he was told that he “could not become addicted to medications; indeed, they will permit you adequate sleep, which will then give you more self-control and rationality when dealing with your marriage prob- lems.” He took perphenazine-amitriptyline. The marriage improved. After a year, medication and therapy were terminated successfully.
Patients are typically ambivalent about losing symptoms. Reinforcing the healthy intentions that coexist with unhealthy ones can therefore be impor- tant. In this example, a therapeutic impasse was overcome by counterproject- ing the patient’s dependence fantasies about medications and by framing the effect of pills so that they reinforced his working through his marital conflicts.
Case 3. Mr. T was a twenty-five-year-old man who appeared as a walk-in. He had been wandering around hitchhiking, and he was disheveled, hungry, delusional, and penniless. The initial interview spanned thirty min- utes. At the end of the interview, the patient reluctantly agreed to meet with the psychiatrist, who was working in the clinic at that moment.
An impromptu staffing was held. Since the patient was excessively vig- ilant about the issue of interpersonal control and viewed psychiatrists as threatening, it was decided that the case manager should conduct most of the meeting and that the psychiatrist would sit on the other side of the room, make comments in a disinterested manner, and offer medications in a desultory fashion. The patient’s anxiety diminished markedly, his medication delusions abated, and he took his prescribed neuroleptic.
Sometimes, framing is impossible because the patient’s irrational fan- tasies arc extremely powerful. In such cases, counterprojection is all that can be accomplished. In the example, it was used to elicit compliance with medi- cation.
Case 4. Mr. J was a forty-one-year-old chronic undifferentiated schizo- phrenic who moved to the area after quitting his lumber mill job in another state because of delusions of persecution. Committed to state hospitals several times, he harbored the usual medication ambivalence and had stopped taking his pills two months prior to decompensation.
We predicted that his ambivalence about medications would decrease and that his sense of self-control over his life would increase if he helped to determine the best medication dosage. Therefore, the following symptom list was negotiated with him: tension, not thinking straight, fears that others will attack him, excessive talk about the past, and being unable to understand
91
other people. This list has been reviewed at every follow-up visit, and com- pliance has not been problematic for four years.
Consensually defining the criteria used to evaluate the effects of medi- cations is a particularly potent framing opportunity, because the patient is more likely to cooperate and because titrating to minimal doses is easier. (Titration reduces the risk of long-term side effects, such as tardive dyskinesia.) Involving the patient’s network and making symptom lists and evaluating results can often build and maintain clearer interpersonal boun- daries between a patient and his networks.
Discussion
Clearly, the method produced some dramatic results. As it evolved, other benefits became evident. Community mental health center staff began to feel more comfortable and even adept at using medications as tools. Staff mo- rale seemed to remain on more of an even keel. Finally, staff began to view med- ications as one intervention modality, not the only modality, which helped them to maintain a broad network perspective on treatment. Some of these results can be understood as operationalizing principles that Caplan (1970) believes are im- portant for the consultant-consultee relationship: The method is coordinate with no built-in hierarchic or authoritarian tension, it involves building and using a common language (here, framing, counterprojecting, network intervening), and it works to maintain consensus as a ground rule for decision making.
One important advantage of this approach is that it makes more effi- cient use of the psychiatrists time, because once the patient has been properly medicated, the case manager assumes collaborative responsibility for medica- tion monitoring. Thus, psychiatrist and case manager often share patients for many years. We found that this served to minimize the communication gaps, thereby providing patients with the experience of feeling that the treatment team was a cohesive part of their own personal network. Another result was to decrease the time needed for follow-up drug monitoring by the psychiatrist. This gave him time for other case consultations, agency problem solving, research hospital liaison, and inservice training. Indeed, our experience is the opposite of that described by much of the literature, which points to a decreas- ing presence and increasing burnout among psychiatrists in the public sector (Eaton and Goldstein, 1977; Winslow, 1979).
Prescribing
The ideas shaping the interpersonal and psychological dimensions of any prescribing (including prescribing in this method) are eloquently expressed by Eisenberg: “Patient and doctor are together reconstructing the meaning of events in a shared mythopoesis. The effort to find meaning in life is a philo- sophical undertaking in which logic, aesthetics, and consistency provide the talismans for truth, not its objective verification. Once things fall into place;
once experience and interpretation appear to coincide; once the patient has a coherent ‘explanation’ which leaves him no longer feeling the victim of the inexplicable and the uncontrollable, the evil symptoms are, usually, exorcised” (1981, p. 245).
A coherent explanation seems necessary for good prescribing, but it alone is not sufficient. Specific skills also seem necessary, because prescribing any course of treatment is an enormously complicated process that involves many variables. (Indeed, the review by Haynes and others (1979) of just one outcome of prescribing- compliance - lists 1,422 references.)
Based on experience from this method, a review of relevant literature, and common clinical wisdom, some specific guidelines for prescribing psycho- tropic medications in community mental health clinics can be summarized. The reader is referred to several excellent review articles for specific tech- niques, particularly for techniques that focus on noninterpersonal variables.
I . Engage the patient’s network. While this is a good general principle for any treatment, prescribing specific tasks for network members is a very effec- tive method of strengthening the patient’s support system while concurrently erecting more adequate interpersonal boundaries (Cutler and Madrone, 1980).
2. Maintain continuity of care. Patients cooperate better when they interact with the same caretakers over a long period of time.
3. Negotiate mutually acceptable explanations for patient problems, for intervention strategies, for the tools to be used, and for expected treatment outcomes (Balint, 1957; Eisenberg, 1981). Gutheil (1982) calls this process participant prescribing.
4. Watch for signs and symptoms indicating failure of such negotia- tions, and take steps to correct them. Not only should we be concerned with congruent role expectations for our patients but also with whether they under- stood the specific instructions and meanings associated with medications. Often, a simple question will suffice: “Tell me what you understand of what we have agreed on.“
5. Frame medications as well as the patient’s involvement in the medi- cation transaction so that his psychological resources are enlisted and trans- formed in the treatment process.
6. Predict the setbacks, pain, anxiety, and grief that often accompany treatment of any kind. This procedure, which sometimes is called stress inocula- tion, is useful because the uncertainty associated with change can obstruct the very process of change itself.
7 . Reward specific behaviors that move patients toward graduated self-management. Following this guideline can move patients from dependence to independence. Following it requires us to assess how and to what degree patients can act dispassionately and responsibly in their own self-interests and not become overwhelmed by the change process. Specifically, we need to be alert to the rate at which interventions are made, particularly in the beginning phases of disrupting pathological patterns, so that the feelings associated with change can be contained by the patient.

93
Conclusions
Use of the methods described here should result in enhanced thera- peutic leverage, correction o r redirection of treatment strategies, fewer inter- disciplinary communication gaps, and more efficient and effective use of psy- chiatrists. Ultimately, it is the patients who will benefit from this collaborative and sensitive approach to their problems and concerns about treatment.
References
B a h t , M. The Doctor, the Patient, and His Illness. New York: International University
Caplan, G. The Theory and Practice $Mental Health Consultation. New York: Basic Books,
Cutler, D. L., and Madrone, E. “Community-Family Network Therapy in a Rural
Eaton, J . S., Jr., and Goldstein, L. S. “Psychiatry in Crisis.” AmericanJournal 4Psychi-
Eisenberg, L. “The Physician as Interpreter: Ascribing Meaning to the Illness Experi-
Firman, G. J . “The Psychiatrist-Nonmedical Psychotherapy Team: Opportunites for a
Gutheil, T. G. “The Psychology of Psychopharmacology.” Bulletin .f the Menninger
Havens, L. L. Participant Obseruation. New York: Jason Aronson, 1976. Haynes, R. B., Taylor, D. W., and Sackett, D. L. (Eds.). Compliance in Health Care.
Baltimore: Johns Hopkins University Press, 1979. Hoehn-Sarie, R., Frank, J. D., Imber, S. D., Nash, E. H . , Stone, A. R., and Battle,
C. C. “Systematic Preparation of Patients for Psychotherapy.” Journal of Psychiatric Research, 1964, 2, 267-281 ~
Lamb, H. R. “Coordination: The Key to Rehabilitation.” Hospital and Community Psychiatry, 1971, 22, 46-47.
Lazare, A , , Cohen, F. , Jacobson, A. M., and others. “The Walk-in Patient as a Custo- mer.“ AmericanJournal of Psychiatry, 1972, 42, 872-883.
Sharfstein, S. S. “Will Community Mental Health Survive in the 1980s? American Journal of Psychiatry, 1978, 135, 1363-1365.
Speck, R. V., and Attneave, C. Family Networks. New York: Vantage Books, 1973. Stanton, A. H. “The Significance of Ego-Interpretive States in Insight-Directed Psy-
Sullivan, H . S. The Interpersonal Theory of Psychiatry. New York: Norton, 1955. Watzlawick, P . , Weakland, J. H., and Fish, R. Change: Principles ofProblem Formution
Winslow, W. W. “The Changing Role of Psychiatrists in Community Mental Health
Press, 1957.
1970.
Setting.” Community Mentai Health Journal, 1980, 16, 144-155.
atv, 1977, 134, 642-645.
ence.“ Comprehensive Psychiatry, 1981, 22, 239-248.
Therapeutic Synergy.” journal of Operational Pswhiatv, 1982, 13 ( l ) , 32-36.
Clinic, 1982, 46 (4), 321-330.
chotherapy.” P.yhiatry, 1978, 41, 121-140.
and Problem Solution. New York: Norton, 1974.
Centers.” AmericanJournal .f Psychiatry, 1979, 136, 24-27.
T i m Burton, M . D., clinical assistant professor d/~sychiat?y, Oregon Health Sciences Universiy, has a priuate outpatient practice. H e is also consultant psychiatrist for the Mid-Columbia Center f o r Livin<g, Hood River, Oregon.