Embed Size (px)
Citation preview
1
Theory base See Time Out for Parents – Children with Special Needs Facilitator Guide pages FG11 to FG19 for the theoretical base for the material in Time Out for Parents – Children with ADHD. Additional notes on the theory base for the material in this course are set out in the appropriate session notes below.
Session notes Session 1 What is ADHD? Attention deficit hyperactivity disorder is a common behavioural disorder in children and young people that usually starts in early childhood, which some people will continue to have as adults. It is classified as a neurodevelopmental disorder, described as a “persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with development”. Oppositional defiant disorder Oppositional defiant disorder (ODD) often exists alongside ADHD, and is characterised by persistent ‘negative, hostile and defiant behaviour’ towards authority. It is now considered to be a sub-type of ADHD as it shares many similar features. Pathological demand avoidance (PDA) is generally seen as a separate disorder linked to ASD and extreme anxiety. ODD usually occurring in younger children, is primarily characterised by markedly defiant, disobedient and disruptive behaviour. Those with ODD as well as some children with ADHD will have difficulty in complying with even simple instructions. Deficits in attention, motor control and perception (DAMP) is a medical concept developed in the 1970’s by Lars Gillberg, a professor of child psychiatry in Sweden. It has been in clinical use in Scandinavia for about 20 years and is occasionally used in the UK by practitioners. DAMP is diagnosed on the basis of concomitant attention deficit-hyperactivity disorder and developmental coordination disorder (DCD) in children who do not have severe learning disability or cerebral palsy. The diagnostic criteria for DAMP is:
ADHD as defined by DSM IV
DCD as defined by DSM IV
The condition not being better accounted for by cerebral palsy
The condition not being associated with severe learning disability (IQ is above 50)
2
Gillberg’s use of the diagnosis DAMP is not accepted by all scholars but it is accepted that around half of all cases with ADHD have DCD, and conversely, ADHD occurs in about half of all cases of DCD Other diagnostic categories (such as ASD, ODD and depression) often apply but are not required to make a diagnosis. See Deficits in attention, motor control, and perception: a brief review for more information ADHD and autism An increasing number of children are being diagnosed as having both ADHD and autism spectrum disorder (ASD). Some people have suggested that ADHD belongs on the autistic spectrum as there can be some common features. It is clear from the genetic histories of some families that there are links between them. However, children with ADHD may have no difficulties with communication and social skills and those with ASD may have no issues with attention or hyperactivity See the National Autistic Society for further information Hyperlexia This is an exceptional ability to read, not necessarily with any understanding of what is being read. This is sometimes seen in children with ADHD. Children with ADHD can have other problems such as learning difficulties, autism, conduct disorder, anxiety and depression, neurological problems like tics, Tourette’s and epilepsy. They can also have problems with coordination and social skills. Because these conditions can cause similar behaviours a correct diagnosis can be challenging for professionals. See the Royal College of Psychiatrists for further information ADHD can present with different behaviours depending on age, setting (school, home, playground, etc.) and even motivation (for example, doing activities the child likes). See the DSM-5 or NICE or the National Autistic Society for further information on these conditions
3
Dypraxia Praxis is the word used to describe motor planning abilities. Disturbance of accurate processing of sensory information impacts on an individual’s ability to effectively plan motor response in a coordinated manner. Sensory modulation difficulties This is the capacity of the brain to regulate the degree, intensity and response to sensory input in a graded and adaptive manner so that an optimal range of arousal level, attention control, performance and adaptation to challenge can be maintained. Children with ADHD have difficultes in this area. McIntosh et al. 1999; Lane et al. 2000 Children’s developmental stages
For information on this subject, see page FG12 of the Time out for Parents Children with Special Needs facilitator manual.
History of ADHD 1845 The German psychiatrist Dr Heinrick Hoffman first described the symptoms of ADHD. He wrote and illustrated a book of poems for children entitled, Struwwelpeter. One poem, ‘The Story of Fidgety Phillip’ perfectly describes the behaviour of a child with ADHD. Dr Hoffman thought the problem was poor behaviour rather than a medical condition.
19021920 Sir George Still presented a series of lectures to the Royal College of Physicians in England in which he suggested that the cause was genetic, not poor child-rearing. His lectures started an avalanche of studies and papers from the medical community on ADHD, giving information on the cause, symptoms, diagnosis, and treatments. Historically, the origins of the concept of hyperkinetic disorder and inattention were in the idea that some disturbances of behaviour were the result of brain damage or ‘minimal brain dysfunction’ (MBD), such as were seen in the pandemic of encephalitis in the 1920s or after traumatic birth.
1937 The use of stimulant medication to treat hyperactivity was first reported.
1968 DSM-II used the term ‘hyperkinetic reaction of childhood’ to describe the symptoms.
1980s Brain damage theories continued for many years but could not be substantiated. Then, in the1980s, DSM-III and ICD-9, put to one side the aetiological theories and concentrated on the reliable description of problems at a behavioural level.
4
In the 1980 DSM-III revision, the term ‘attention-deficit disorder’ (ADD) with or without hyperactivity’ was introduced.
1987 DSM-III used the term ‘attention hyperactive disorder’.
1990 Over the past 35 years, theories about the biological basis of ADHD have suggested that it may be a neurochemical disorder. See ‘How the ADHD brain works’ below. Dr Jean Ayres, a psychologist and occupational therapist, also described sensory processing and motor planning difficulties in children with ADHD leading to poor impulse control and uninhibited behaviour. Also in 1990 positron emission tomography (PET) scans taken in a study by Zametkin found lower glucose metabolism in the brains of patients with ADHD.
1994 The DSM-IV classified ADHD and ODD under the one heading ‘attention-deficit and disruptive behaviour disorder’ which includes, ADHD, ADD and ODD.
2000 Extensive biological investigations of both ADHD and hyperkinetic disorder yielded some neuroimaging and molecular genetic associations. Neurocognitive theories have emerged; and there is a better understanding of the natural history and the risks that hyperactive behaviour imposes.
2005 Twin studies around this date showed that ADHD symptoms had quite strong genetic influences. Around 75% of various ADHD symptoms in the population are because of genetic factors. No single gene of large effect was identified in ADHD, but several DNA variants of small effect were found, each increasing the susceptibility of ADHD by a small amount.
2009 The British Psychological Society and the Royal College of Psychiatrists, in collaboration with NICE, released a set of diagnosis and treatment guidelines for ADHD.
2013 ADHD and its diagnosis and treatment have been considered controversial since the 1970s. Topics include ADHD's causes and the use of stimulant medications in its treatment. The DSM-5 (2013) now lists ADHD under the heading of ‘Neurodevelopmental Disorders’. ADHD in the DSM-5 is further defined by whether the symptoms are predominantly inattentive, predominantly hyperactive/impulsive, or combined.
5
Current thinking Current research is looking at deeper brain structure dysfunction. Studies have shown that people with ADHD have less activity in the ventral striatum (which relies heavily on D1 and D2 dopamine receptors), or the circuits on the underside of the basil ganglia that connect it to the limbic or reward system. They have disruptions in the links and activity between the basil ganglia and sensorimotor cortex.
Shaw et al., 2014 The DSM and ICD current versions, DSM-5 and ICD-10, have come to an almost identical operational definition of ADHD with a set of 18 core symptoms (see above for classification details).
What we know about ADHD Estimated prevalence rate in the
About 25% of school-aged children are thought to suffer from ADHD. In the UK, diagnostic rates are around 1% whilst in the U.S. they are 3-5%. In 2009 studies by Ford et al. found that 3.6% of boys and 0.85% of girls in Britain qualified for a diagnosis of ADHD using the American DSM guidelines. Boys are more commonly affected than girls.
A recent review by the National Centre for Biotechnology Information has shown that in girls this is a more hidden diagnosis. Girls with ADHD are more inclined to internalise symptoms so that the inattentiveness is more prominent than the hyperactivity. Also they appear to be able to develop better coping strategies than boys and mask the symptoms. They are more likely to be diagnosed with depression or an anxiety state.
To read the review see www.ncbi.nlm.nih.gov/pmc/articles/PMC4195638/
What causes ADHD? The precise causes of ADHD are still unknown but appear to be remarkably similar to those alleged to cause autism. The range of factors thought to cause ADHD range from the biological, such as genetics and brain damage during pregnancy, to the environmental, such as sensitivity to certain foodstuffs. It is thought to be an inherited condition and is closely tied to biological factors such as the size and density of various brain structures and the way that chemical reactions take place in the brain. We do not know exactly what causes these disorders. Sometimes parents feel they are to blame for not having controlled their child, but there is no evidence that poor parenting directly causes ADHD. However, it is important to note that parents play a
6
crucial role in helping and managing a child with ADHD (Royal College of Psychiatrists, Mental Health and Growing Up factsheet). “Over the past 25 years, theories about the biological basis of ADHD have suggested that the neuroanatomical location of deficits is in the frontal-basal ganglia and that this is a neurochemical disorder involving dopamine pathways which result in impaired neuropsychological functions, e.g. inhibition, executive functions, etc. This, in turn, induces a pattern of inattentive, hyperactive and impulsive behaviour.” Sidney Chu, National Association of Paediatric Occupational Therapists (NAPOT) Conference, 2002.
Diagnostic information The two diagnostic bodies are the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (latest version DSM-V, 2013) and the World Health Organisation’s International Statistical Classification of Diseases and Related Health Problems (latest version ICD-10). The 2018 update of ICD-10 now uses the term Attention-deficit, Hyperactivity Disorder rather than Hyperkinetic disorder in line with DSM V. These two classifications have come to an almost identical operational definition of ADHD with a set of 18 core symptoms There are three different types of ADHD which are referred to as ‘presentations’ based on the predominant symptom pattern for the past 6 months – predominantly inattentive presentation, predominantly hyperactive/impulsive presentations and combined presentation. There are a number of different specialists that a child may be referred to for a formal assessment, including a child psychiatrist, a specialist paediatrician or a learning disability specialist or occupational therapist with expertise in ADHD. There is no single, simple, objective medical test for diagnosing ADHD but the 18 core symptoms and the criteria for each presentation as set out by DSM V are listed below: Symptoms of predominantly inattentive presentation Diagnosed if six or more symptoms of inattention (but less than six symptoms of hyperactivity/impulsivity) have persisted for six months.
1. Often fails to give close attention to detail or makes careless mistakes in schoolwork, work or other activities
2. Often has difficulty sustaining attention in tasks or play activities (for
example, has difficulty managing sequential tasks, is messy, has disorganised work, has poor time management).

7
3. Often does not seem to listen when spoken to directly
4. Often does not follow through on instructions and fails to finish schoolwork or chores (not due to failure to understand)
5. Often has difficulty organising tasks and activities
6. Often avoids, dislikes or is reluctant to engage in tasks that require
sustained mental effort (such as schoolwork or homework)
7. Often loses things necessary for tasks or activities (e.g. toys, school assignments, pencils, books or tools)
8. Is easily distracted by extraneous stimuli
9. Is often forgetful in daily activities (for example, doing chores, errands,
keeping appointments).
Symptoms of predominantly hyperactive/impulsive presentation Diagnosed if 6 or more symptoms of hyperactivity/impulsivity (but less than 6 symptoms of inattention) have been present for 6 months. Hyperactivity
1. Often fidgets with or taps hands and feet, or squirms in seat 2. Often leaves seat in situations when remaining seated is expected (for
example, leaves their place in the classroom) 3. Often runs and climbs in situations where it is inappropriate (in adolescents or
adults, may be limited to feeling restless) 4. Often unable to play or engage in leisure activities quietly 5. Is often ‘on the go’, acting as if ‘driven by a motor’(for example, is
uncomfortable being still for an extended time in lessons or restaurants) 6. Often talks excessively
Impulsivity
7. Often blurts out answers before a question has been completed (for example, completes people’s sentences; cannot wait for their turn in conversation)
8. Often has difficulty waiting their turn
8
9. Often interrupts or intrudes on others (for example, butts into conversations or games; may start using other people’s things without asking)
Symptoms of Combined presentation All three core features are present and ADHD is diagnosed when six symptoms of hyperactivity/impulsivity and six symptoms of inattention have been observed. The disorder can be classified as mild, moderate, or severe or in ‘partial remission’ if the diagnostic criteria are not currently met. www.adhd-institute.com/assessment-diagnosis/diagnosis/ The diagnosis is made by observing the child, recognising patterns of behaviour, and obtaining reports of their behaviour at home and at school. Sometimes a computerised test may be done to aid the diagnosis. Some children also need specialised tests by a clinical or educational psychologist.
Sensory factors A person diagnosed with ADHD is thought to have an immature nervous system. More than half of children diagnosed with ADHD have sensory processing difficulties. This may include hyper-sensitivity to sound and sight, difficulty prioritising stimuli in all senses and sensory systems, difficulty blocking out non-essential sensations like background noises in order to focus sensations that are relevant (modulation), and shifting the focus of attention frequently and abruptly. Some children with ADHD are especially sensitive to sensory stimuli such as lights, sounds and textures. The environments where many of these factors interact could be extremely distracting and disturbing to them. If a child is frequently calm and only occasionally hyperactive or disruptive then it may be worth charting when and where these incidents occur to see if there is a pattern to their behaviour. Places that might over-stimulate a child include swimming pools, supermarkets and fast-food restaurants, and trips to places like these may need careful planning as a result. National Autistic Society, ADHD, environmental factors A poorly organised nervous system will ‘drive’ a child into many poorly planned movements. Ayres, J.A. 1979 Sensory sensitivities may occur in any of the senses: touch, sight, sound, smell, taste, or to balance and muscle sense.
9
Auditory sensations
Children with auditory processing disorders have normal peripheral hearing but they may be unsure about what they hear. They may be very sensitive towards sounds which are unheard by others such as humming of refrigerator, clocks ticking, or fans" or they may be hyposensitive at times appearing as if deaf.
The co-morbidity of ODD in children with ADHD is a risk factor for auditory processing problems. These children are more under-responsive to sounds. Background noise in their classroom should be minimized.
Visual sensations Sensory messages travelling from the eyes to the brain can be disrupted or slowed and the result can be observed as delayed or absent response to incoming vision.
They may be hypersensitive to bright flashing lights and notice everything around them. Those who are hyposensitive may not notice when people come into a room which can give the impression of disinterest or rudeness.
Tactile sensations Tactile defensiveness where a child will resist touch is a result of hypersensitivity. It is believed that the level of tactile defensiveness in girls with ADHD is higher than that of boys with ADHD. Children with ODD are known to be hypersensitive to touch.
Those who are hyposensitive may not be aware of being touched and often injure themselves without noticing.
Oral sensations Some children with ADHD have sensitivities to certain smells, tastes or food textures. They may be oversensitive to strong smells and tastes and can perceive them from quite far distances. They may reject or spit out certain foods. They may struggle to perceive taste which will cause them to crave strong flavours and want to smell foods or other items. Balance control and muscle sensations More than one third of children with ADHD have poor balance and coordination associated with the sensory inputs from the vestibular and proprioceptive systems.
The child who is hypersensitive will feel easily giddy and avoid movement. This child will also suffer car sickness.
The child who actively seeks intense sensations such as jumping or spinning, is trying to stimulate a hyposensitive, underactive system. These children are sensory seekers and become more organised and attend better to a task if they receive periodic movement input. These children feel the need to move in order to pay attention.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3149116/#B29
10
Sensory integration Sensory integration is the neurological process that organises sensation from one’s own body and from the environment and makes it possible to use the body effectively within the environment. It sorts, orders and eventually puts all the sensory inputs together into whole brain function. Paediatric occupational therapists can help children with sensory processing difficulties by drawing up a sensory profile and advising on appropriate sensory interventions. Treatment may include a “sensory diet,” in which the child is slowly introduced to activities in a gentle, fun way, in order to get used to a range of sensations. There are a number of strategies designed to help children with ADHD manage sensitivity to sound, light and touch, and to improve body awareness. These involve various sensory experiences – especially balance and movement – to encourage the child to interact with the environment through play and so improve learning.
Weighted blankets – can reduce anxiety and physiological stress. These are to be used with care, supervision and not for restraint (Champagne, 2008).
Ball chairs – can have a positive effect on in-seat behaviour for the children who have the most extreme vestibular-proprioceptive seeking behaviour (Bagatelle, 2010).
Chewing gum – significant positive effect on concentration performance (Tanzer, 2009) .
Ayres, J.A. 1979
How the ADHD brain works It is generally agreed among the scientific community that ADHD is a biological condition resulting from dysfunction in the brain although environmental and genetic factors also play their part. Our central nervous system receives, interprets, organises and sends messages to the rest of the body. It helps us to regard, disregard, seek out or avoid sensations to maintain or increase feelings of comfort, excitement, rest or positive interactions with objects and people. There is ongoing research into the various parts of the brain that control the sensory system, motor responses and the complex interaction of thoughts, actions and language. Gradually, neurologists and neuroscientists are uncovering the neural mechanisms that underlie ADHD
11
An imaging study of ADHD at Radboud University Nijmegen Medical Centre, The Netherlands in 2017, found that the overall brain volume of children with ADHD was smaller and that nerve tissue in different areas of the brain is smaller and thinner than other children of the same age. They often have a smaller cortex in the frontal lobe which is the part of the brain that controls many key functions in thought and action including impulse control, socialisation, reason and judgement. Positron emission tomography (PET) scans have shown differences in the brain of the person with ADHD. It would appear that there are abnormalities in the frontal cortex, basal ganglia, limbic system (containing the amygdala), brain stem and cerebellum of the person diagnosed with ADHD. The problem for these children appears to be a decrease in the metabolic activity in these areas of the brain and the links between them. This decrease in glucose metabolism is thought to result in less energy available to the attention centre in the prefrontal cortex which may leave to the person craving carbohydrates (cakes, bread and chocolate) to create a surge in glucose and better attention in the short term. People with ADHD have lower amounts of the neurotransmitters called dopamine and noradrenaline in the brain. These are chemical messengers that carry information from one nerve cells to another and play a key role in the functioning of the cortex. If you don’t get clear messages from the frontal lobe you can end up with chaotic behaviour such as reduced ability to keep still (jump around), reduced attention (look at that!) poor planning (I’m confused) disorganisation and acting without thinking – all common features of ADHD. This theory seems to be supported by the fact that stimulants work by increasing dopamine levels. For more information see How Does ADHD Work? (Part II) The frontal lobe of the cerebral cortex Is the command centre just like the boss in a large company. It is involved mainly with executive functions. These include problem-solving, paying attention, concentration, reasoning and planning. The cortex also controls the body’s sensory system, its motor responses and the complex behaviour of thoughts, actions and language. The inhibitory mechanisms of the cortex help us to restrain our behaviours; they keep us from being hyperactive, from saying things out of turn and from getting angry at inappropriate times. It has been said that 70% of the brain is there to inhibit the other 30% of the brain. Basal ganglia The basal ganglia play an important role in planning and coordinating motor movements and posture. Its major effect is to inhibit unwanted muscular activity. Disorders of the basal ganglia result in exaggerated, uncontrolled movements.
12
The limbic system The limbic system regulates emotion and memory. It directly connects the lower and higher brain functions, influencing emotions, motivation, mood and sensations of pain and pleasure. If it is over-activated, a person might have wide mood swings or quick temper outbursts. He might also be over-aroused, quick to startle, hyper-vigilant and may touch everything around him. A normally functioning limbic system would provide for normal emotional changes, normal levels of energy, normal sleep routines and normal levels of coping with stress. The limbic system is comprised of the hypothalamus, amygdala and hippocampus. The thalamus, basal ganglia and cingulate gyrus are closely connected to the limbic system. Studies have found that overall brain volume and five of the regional volumes were smaller in people with ADHD - the caudate nucleus, putamen, nucleus accumbens, Hypothalamus The hypothalamus sits under the thalamus at the top of the brain stem. Although the hypothalamus is small, it controls many critical bodily functions including the autonomic nervous system, the centre for emotional response and behaviour. It also regulates body temperature, food and water intake and the sleep-wake cycles. Hippocampus The hippocampus is very important in the transition of information from short- to long-term memory. Amygdala The amygdala appears to be responsible for the influence of emotional states on sensory inputs. When necessary, it will block ‘slow’ thinking in the cortex and move the body into action (an unthinking response). It is also thought to be responsible for face recognition. Cingulate gyrus The cingulate (meaning ‘to surround’) gyrus (meaning ‘fold’) surrounds and is connected to the parts of the inner limbic system. It serves as a conduit of messages to and from the inner limbic system. Thalamus Thalamus means ‘inner room’ in Greek as it sits deep in the brain at the top of the brain stem. It is called the gateway to the cerebral cortex as nearly all sensory inputs pass through it to the higher levels of the brain.
13
Brain stem The brain stem is the region of the brain that connects the cerebrum with the spinal cord. Motor and sensory messages travel through the brain stem allowing for the relay of signals between the brain and the spinal cord. The cerebellum The cerebellum (‘little brain’ in Latin) is a region of the brain that controls balance and coordination and is where learned movements are stored. It plays an important role in the integration of sensory perception and motor output. Many neural pathways link the cerebellum with the motor cortex, which sends information to the muscles causing them to move parts of the body (ADHD Information Gallery). The Stroop test Developed by John Ridley Stroop in1935, the stroop test is a colour-word task that demonstrates interference in the reaction time of a task. It may be used in diagnosis to measure mental vitality and flexibility. When the meaning of the word is incongruent with the colour of that word (for example, the word ‘blue’ written in the colour red) a conflict is created in brain processing. People with ADHD are slower to complete this task, highlighting their cognitive deficits in these areas since performing well requires strong attention and self-regulation capability.
Session 2 Defining attention Paying attention may sound very simple. But it’s a highly developed process with several distinct parts. Most people understand that attention plays an important role in learning. But they may not know that it’s the very first step in the learning process that occurs in the brain.
Attention is like a funnel that lets us select and take in useful information. Once the information is there, the brain can make sense of it and store it in memory.
There are three aspects to attention – being alert, selecting and sustaining and shifting focus. Children with attention issues can have problems with any or all of these parts which will affect their ability to learn. They have trouble determining where to focus attention, with maintaining attention and with shifting attention to and away from distractions.
14
Being alert This means being wide awake and well rested. A child who isn’t aware and alert may literally have his head on his desk during class. But sometimes the signs are more subtle. They can simply seem “tuned out” and appear to be staring at nothing.
Selecting and sustaining The next step is selecting what exactly to pay attention to and then continuing to pay attention to it. To some extent, people use judgment to decide what deserves attention. For instance, a student can choose to pay attention to the teacher and not the birds flying around outside.
But choice and judgment play a smaller role in this process than many people realise. For example, if the whiteboard falls off the wall, all the brains in the room will automatically focus on that. It’s basic instinct.
The same is true if a teacher stands and talks right in front of a student. That child’s brain naturally focuses on what’s taking up his immediate visual and auditory space.
Many children with attention issues want to focus on the “right” thing. But their brains may have trouble picking out what that right thing is.
The other big challenge is that even if they can pick out what’s important, they may not be able to sustain attention for a meaningful amount of time.
Shifting focus This type of flexible thinking is called, set shifting. When it comes to solving problems, set shifting allows us to see a mistake and change the way we approach a situation. It also allows us to move on from a thought or an activity to do something new. It is common for people to frequently shift attention from a task to something internal, like a thought, feeling or memory, but most of us can quickly shift back to the task. The mechanism that lets most students shift attention easily and quickly is sticky in many kids with attention issues. For example, a loud noise in the hallway will catch the attention of everyone in the classroom. But most children are able to shift their attention and then quickly shift back to the teacher.
A child with ADHD may stay focused on that loud noise out in the hallway long after his classmates have returned their attention to the teacher. By the time he tunes back in, he may have missed important information. Or he may not return his attention at all. Instead he may move on to, say, what he’s going to have for lunch
15
and what he’s doing on the weekend. In addition children with ADHD can get hyperfocus and get “stuck” in what they are doing or thinking about.
Adapted from the article How Kids Pay Attention by Peg Rosen
Home-school links Note: Facilitators should consider this recommendation from the National Institute for Clinical Excellence (NICE) and ask parents on the course if they would like them to contact their child’s school. NICE states: When parents or carers of children or young people with ADHD undertake parent-training/education programmes, the professional delivering the sessions should consider contacting the school and providing the child or young person’s teacher with written information on the areas of behavioural management covered in these sessions.
Sleep
Children need about nine to ten hours of sleep each night and a lack of sleep can negatively impact on a child’s emotions, concentration and task performance as well as affecting the wider family’s quality of life. Poor-quality sleep and lack of sleep are the top culprits when it comes to alertness issues. ADHD can lead to sleep problems and a lack of sleep can make the symptoms of ADHD worse. Sleep disorders include insomnia—problems with falling asleep or staying asleep. They can also affect a person’s ability to achieve deep, restorative sleep.
Insomnia This is a sleep disturbance resulting in difficulty falling asleep and staying asleep. People with healthy sleeping habits fall asleep in about 10 to 20 minutes. Nightmares Most children have occasional nightmares and it seems to be a normal part of growing up. Stressful things that happen during the day can turn dreams into nightmares. Simply being there to soothe your child after a nightmare will help, or you could try talking about the nightmare and making up a happy ending to the story. Snoring and breathing problems As many as 25% of children with ADHD may experience regular snoring and a small number of these may have sleep apnoea, which is characterised by struggling for breath followed by waking and gasping for air.
16
Parents also will suffer from a lack of sleep because of the bedtime challenges and interrupted nights, and effects their ability to cope with the child’s challenging behaviour, whilst causing stress among and between other family members. Research into the impact on parents of children with ADHD sleep problems found:-
• 42% of parents of children with ADHD are woken by their child before 6 a.m. • 70% of parents felt more irritable during the day • 61% of parents felt less able to cope with problems • 56% felt depressed due to the tiredness • 43% of parents said that tiredness impacted a lot on their relationships
46% said they argued with their partner more often • 20% had taken time off work in the past year due to tiredness
64% had cancelled or avoided social activities in the past six months
ADHD Sleep Seekers Research UK. 2005.
It is important for both child and parent to recognise and understand the extent of a child’s difficulty, to rule out any separate sleep disorder and to begin to find ways of making bedtimes less of a battleground.
Tips for getting a better night’s sleep Exercise Daytime exercise can make a big difference in helping children gain quality sleep at night. Encourage your child to do some light exercise such as walking, skipping, or playing a team sport every day, but avoid strenuous physical activity for a few hours before bedtime. Sleep environment Keep the bedroom dark, quiet and at a comfortable temperature. Routine Make sure your child goes to sleep at the same time each night and gets up at the same time each morning. Try to avoid over-stimulating activities during the evening before bed, such as watching television, playing a computer game or reading an exciting book. Take the television, computer, games console, etc, out of a child’s room to avoid temptation Food Try to avoid giving the child a large meal a few hours before he/she goes to bed. Try cutting out certain foods if they exacerbate the symptoms of ADHD, such as food with additives, colours, or foods high in sugar. Children should also avoid foods containing caffeine, such as cola, chocolate and tea.
17
Sleep diary A sleep diary can be a very useful assessment technique for identifying and understanding sleep problems.
ADHD medication A recent parental survey demonstrated that many treatments for ADHD begin to wear off by the late afternoon and evening. Therefore a child’s ADHD may not be well controlled during the night. Different treatments last for different lengths of time, so you may want to review your child’s medication regime with your doctor. In addition, some treatments for ADHD have been found to make it more difficult for the child to fall asleep. Seek help from your specialist doctor Because every child is different, make sure you have discussed all the treatment and medication options with your doctor, who can advise you on managing ADHD during the evening, bedtime and beyond. Sleep medication is not often used in children but sometimes your specialist may wish to discuss this with you if your child’s sleep remains a significant problem despite other management steps.
Session 3 – Hyperactivity
Hyperactivity is a classic sign of ADHD. The signs are hard to miss and they often prompt negative reactions from other people. Until you know the reason behind the behaviours, you may find yourself getting annoyed and thinking that your child is just acting up. This brain-based condition often causes children to move and talk nonstop. It’s the result of the brain’s “wiring” system working a little slower than is typical. With ADHD the brain takes a bit longer to get started and “go”. But it also has trouble putting on the brakes to “stop”. Research shows that certain parts of the brain are less active and develop more slowly in children with ADHD. One of these areas, the frontal lobe, is in charge of executive function, a group of key mental skills. Self-regulation is one of those skills.
Children with ADHD, have difficulty with self-monitoring and self-regulating their behaviour which makes it hard for them to control their hyperactive behaviour. They also have a hard time managing emotions, so they often overreact.
Self-regulation is not the quite the same as self-control although they are related. Self-control is primarily a social skill used to keep their behaviour, emotions and
18
impulses in check whilst self-regulation has to do with how we process information and emotion, and what we are able to do with them.
Children have to work out that they need to calm themselves down when they get upset. They have to learn to be flexible when expectations change, and be able to resist giving in to frustrated outbursts.
This skill develops over time. That’s why it’s fairly common to see a 4-year-old having a tantrum, but not a 12-year-old. If a 12-year-old regularly has tantrums, he likely has a problem with self-regulation.
Self-monitoring is a skill we use all the time to keep track what we’re doing. It’s a series of assessments we make along the way: How is the activity going? What’s working and what’s not? Should I make adjustments?
For example, when we make breakfast if the eggs were runny last time, we might think, “What do I need to do differently this time?”
As children mature, the frontal lobe also matures and is able to function more effectively so as they get older they can use their stronger executive skills to help manage some of their symptoms. So while children don’t actually grow out of hyperactivity the signs are less noticeable to others. They often have to work hard to keep it in check.
For information on hyperactivity, click here.
The Alert Programme “If your body is like a car engine, sometimes it runs on high, sometimes it runs on low, and sometimes it runs just right.” The Alert Programme supports the child and carers to choose appropriate strategies to help the child’s nervous system to change or maintain states of alertness, for example, a high alert state needed for school work or a more appropriate low state at bedtime. Williams, M. & Shellenberger, S. 1996
19
Behavioural theory – reward based programmes Traditional behavioural techniques such as applied behavioural analysis (Lovaas/ABA) are reward-based programmes designed to teach basic skills. Therapists use applied behavioural analysis and modification techniques to help children’s parents, carers and teachers to manage troublesome behaviours, establish healthy routines and encourage acceptable behaviour in their children. Aspects of learning that the child finds hard are broken down into small steps and are then presented in a simple and consistent way. The method relies on providing positive reinforcement so that the child feels successful and is motivated to learn more. Desired behaviours are rewarded and inappropriate behaviours are ignored or redirected. The child is taught how to pay attention, copy behaviours, imitate sounds, understand what people say, play with toys, show emotions and relate to other children. The practice of ABA is continually evolving although Baer, Wolf and Risley’s work in1968 is still used as the standard description of ABA.
Relaxation For information about the Benson method of relaxation, click here.
Session 4 – Impulsivity
The child may speak or act without thinking at times inappropriately and may have a short fuse, leading to temper tantrums.
Children with excess energy need to put that energy somewhere. Often, they’re drawn to higher-risk activities like “extreme sports.” That’s not a problem in and of itself but if the child has impulsivity they may not be aware of danger and not take even simple precautions. For them, it’s extra important to have proper training, supervision and protection for high-risk activities. Talking in advance about risks and consequences can help. .
They can have severe mood swings and be very volatile. They can have good and bad days with no real explanation. For information on impulsivity, click here.
20
‘Unthinking’ reactions Impulsive/unthinking behaviour is necessary in times of emergency. Six steps to an unthinking response:
1. Sensory data is fed to the thalamus All sensory data (except, curiously, for the sense of smell) is sent by the body first to the thalamus, which acts like a switchboard, sending it to the relevant part of the brain.
2. Data is sent to the amygdala The thalamus sends the data both to the relevant part of the cortex and also to a small part of the mid-brain called the amygdala.
3. Data sent to cortex When the information is sent to the cortex, we, of course, think about it. The problem is that sometimes there is no time to think – in fact, too much thinking can sometimes leave you dead.
4. The amygdala does a quick threat assessment The senses are compared in the amygdala with our stored fear responses. If any of these are triggered, then the amygdala has to act quickly.
5. The amygdala blocks ‘slow’ thinking If the fear response is triggered, then the amygdala floods the cortex with chemicals to stop it taking over.
6. Unthinking response The result is that we act without conscious thought. We jump out of the way of a falling branch or dive into the river to save a child.
For more information on the amygdala bypass system, click here.
Mindfulness
Mindfulness is a meditation technique that has become popular among adults with mental health problems and ADHD. There are number of papers and research projects on this topic.
Lidia Zylowska, M.D. is the author of The Mindfulness Prescription for Adult ADHD.
Mindfulness training aims to help with:
Developing better awareness of attention and learning to be less distracted.
Learning to step back and observe one’s thoughts and feeling so they don’t overly
drive our sense of self or understanding of our life. This is very helpful in learning to
have more flexible mind and controlling impulsive reactions.
21
Managing stress better by having new perspective and less emotional reactivity, but
also by replenishing the “self-regulation” tank.
Knowing when to be compassionate and accepting of ADHD symptoms, and
knowing when to encourage changing an unhelpful pattern in thinking, feeling or
actions.
To help with ‘Mindfulness of Sound, Breath, and Body’, the acronym “S.T.O.P.” is
used to help people practice mindfulness in daily life.
Each letter is a reminder to take a brief step:
S = Stop (or pause) for a moment
T = Take a deep breath
O = Observe mindfully in the moment (for example, you can notice more consciously your body sensations or what you are doing)
P = Proceed with relaxation and awareness
The last step, “proceed,” is also an invitation to use choice in your actions (for example, if you noticed you were distracted or avoiding something, you could resolve to change that). Of course, the change part is not always easy and often requires effort. But with practice (and sometimes together with medications or other ADHD tools), that choice can become easier.
I-messages In order to control what you are saying, try using assertive I-messages to communicate. These have three elements: 1. Describing the behaviour (remember to separate the behaviour from the child) 2. Describing the effects of the behaviour on yourself and others present 3. Describing how you feel, for example, “If you interrupt when I’m talking to the
class, the other pupils can’t hear what I’m saying and we all feel annoyed”
Assertive I-messages are less confrontational to the angry child and enable you to remain in control. Being passive may send the wrong message to the aggressor, possibly suggesting that you are not in control of the situation. Maines, B. & Robinson, G. 1997
22
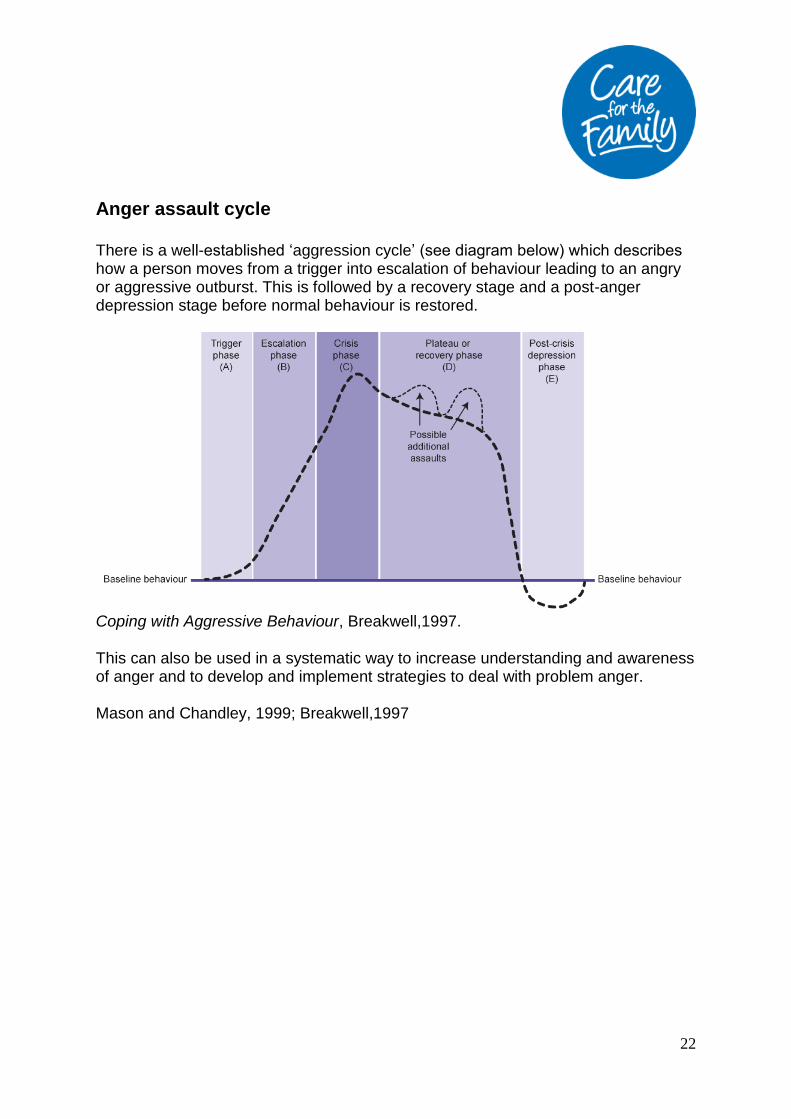
Anger assault cycle There is a well-established ‘aggression cycle’ (see diagram below) which describes how a person moves from a trigger into escalation of behaviour leading to an angry or aggressive outburst. This is followed by a recovery stage and a post-anger depression stage before normal behaviour is restored.
Coping with Aggressive Behaviour, Breakwell,1997. This can also be used in a systematic way to increase understanding and awareness of anger and to develop and implement strategies to deal with problem anger. Mason and Chandley, 1999; Breakwell,1997
23
Treatment of ADHD
In the UK, both NICE and the Scottish Intercollegiate Guidelines Network (SIGN) recommend that ADHD should be treated.
The treatment recommended for each child will depend upon their age and the severity of their symptoms. Some children will require behavioural treatments only, while others may require behavioural treatment and medication to control their symptoms adequately. The precise treatment that a child will be offered will depend on their particular needs. However, it is likely to include:
1. Advice, support and behavioural therapy
This is for both the parents and/or the child and/or their teachers. It includes specific training on how to manage the child's behaviour most effectively and promote ways of bringing out the best in them.
NICE guidelines state that healthcare professionals with training and expertise in diagnosing and managing ADHD should offer the following interventions:
Give information to parents about ADHD
Offer additional support to parents and carers of all children aged 5 years and over and young people with ADHD.
Support should be ADHD focused, can be group based and should include: education and information on the causes and impact of ADHD, advice on parenting strategies and offer of liaison with school.
Consider individual parent-training programmes for parents and carers of children with ADHD and symptoms of Oppositional Defiant Disorder when a family’s needs are too complex to be met by group-based parent-training programmes.
Consider a course of cognitive behavioural therapy (CBT) for young people with ADHD who have benefited from medication but whose symptoms are still causing a significant impairment in at least one domain, addressing the following areas: social skills with peers, problem-solving, self-control, active listening skills, dealing with and expressing feelings.
24
2. Medication
In most cases it is recommended that a combination of both medication and advice, support and behavioural therapy is the best way to manage the full range of problems experienced by those with ADHD. However, the extent to which this is possible will vary from region to region based on local resources and expertise.
Types of medication Medications used to treat ADHD are broadly divided into two groups: stimulants and non-stimulants. Stimulants These have the effect of making people feel more alert, energetic and awake. In a person suffering from ADHD, they can improve attention and reduce hyperactivity. The stimulants used in the treatment of ADHD include methylphenidate (previously commonly known by the name Ritalin) and dexamphetamine. Methylphenidate is available in different forms. Immediate-release methylphenidate is short-acting. It is used for its flexibility in dosing and can be used to determine the correct level of dose during dose changes. Slow- or modified-release
methylphenidate works for 812 hours and can be given once a day. This is more convenient and, as the child or young person need not take a dose in school, reduces the stigma attached to this disorder. Non-stimulants These medications, by their nature, do not make people alert or active. However, in ADHD, they can improve symptoms of inattention and hyperactivity. These include medications like atomoxetine. Sometimes other medications may be used to help with problems with sleep and challenging behaviours that are associated with ADHD. Melatonin (common name Circadin) is often prescribed for children who have severe sleep difficulties associated with ADHD. How they work Medications act on certain chemicals in the brain called noradrenaline. They seem to affect the parts of the brain that control attention and organise our behaviour. They do not cure ADHD; they simply help to control the symptoms of poor attention, over-activity or impulsivity. Which medication will be used and does it work? The stimulant medication, methylphenidate is usually prescribed first. The type of stimulant prescribed will depend on a number of things like the symptoms your child has, your choice of treatment, the ease of giving the medication, and even the availability and cost of the medication.
25
If methylphenidate causes unpleasant side-effects or does not work, other stimulant (dexamphetamine) or non-stimulant medications (atomoxetine) may be prescribed. Sometimes a child may respond to a different form of methylphenidate. If the medication is working, you will find that: Your child’s concentration is better. Their feelings of restlessness or over-activity are less. They control themselves better.
Sometimes school staff or teachers notice the improvement before you do. Side-effects As with most medications, there may be some unwanted effects. However, not everyone gets side-effects and most side-effects are mild and disappear with continued use. Side-effects are less likely if the dose is increased gradually when the tablets are started. Some parents worry about addiction, but there is no good evidence to suggest that this is a problem. Some of the common side-effects of methylphenidate include: Loss of appetite Difficulty falling asleep Light-headedness
Less common side-effects to look out for include: Being ‘over-focused’, quiet and staring –may be a sign that the dose is too high Anxiety, nervousness, irritability or tearfulness Tummy pains or feeling sick Headache, dizziness or drowsiness Tics or twitches If there are side-effects, the dose of medication may need to be reduced, stopped or changed. Regular checks Parents and teachers are asked to keep a record of changes in symptoms and behaviour when medication is started or the dose is changed. A specialist should contact them regularly to check how things are going. Healthcare professionals should also check for side-effects regularly and a child’s weight and height should also be regularly measured.
26
What if medication does not help? If methylphenidate or atomoxetine together with educational courses for parents and psychological therapy for the child or young person with ADHD do not help them, healthcare professionals should review the treatment so far. The dose of the medication may then be increased or dexamfetamine or another drug may be offered. How long should medication be taken? Medication should be continued for as long as it is helpful. It should be reviewed at least every year in children and young people . Healthcare professionals should work with the person to find a pattern of treatment that works best. This may include periods when medication is not taken. For further information on how to get help, click here. 3. Diet
The extracts below show that uncertainty still exists about whether or not food additives are linked to ADHD behaviour. However, it is agreed that for many children a change of diet can be beneficial. The Lancet, 2007 A study published in The Lancet in 2007 entitled ‘Diet and Attention Deficit Hyperactivity Disorder’ found a link between children’s ingestion of many commonly used artificial food colours, the preservative sodium benzoate and hyperactivity. In response to these findings, the British government took prompt action. According to the Food Standards Agency (FSA), the food regulatory agency in the UK, food manufacturers are being encouraged to voluntarily phase out the use of most artificial food colours by the end of 2009. Following the FSA’s actions, the European Commission ruled that any food products containing the ‘Southampton Six’ (the contentious colourings are: sunset yellow FCF (E110), quinoline yellow (E104), carmoisine (E122), allura red (E129), tartrazine (E102) and ponceau 4R (E124)) had to display warning labels on their packaging by 2010. NICE guidelines say that your child’s specialist should offer you advice about a good diet and regular exercise for them. If you or a healthcare professional notice any foods or drinks that seem to affect your child’s behaviour, you should be advised to keep a diary of what your child eats and drinks and their behaviour afterwards.
27
If there seems to be a link between certain foods, drinks and your child’s behaviour, you should be offered an appointment with a dietitian. There is no evidence that dietary supplements such as fatty acids (omega 3 or omega 6) or cutting out foods containing artificial colourings and other additives can help children with ADHD. For information about diet from NICE, click here.