Embed Size (px)
Citation preview

LABORATORY INVESTIGATIONANGIOPLASTY
The mechanism of transluminal angioplasty:evidence for formation of aneurysms inexperimental atherosclerosisTIMOTHY A. SANBORN, M.D., DAVID P. FAXON, M.D., CHRISTIAN HAUDENSCHILD, M.D.,SUSAN B. GO-FrSMAN, A.S., AND THOMAS J. RYAN, M.D.
ABSTRACT Quantitative histologic examination (morphometric analysis) of pressure-perfused rab-bit atherosclerotic arteries was used to determine whether compression of atheromatous material occurs
with transluminal angioplasty. Experimental atherosclerosis was developed in both iliac arteries, withtransluminal angioplasty performed on the left iliac while the right iliac served as a nondilated control.Angiography showed equal degrees of luminal narrowing before angioplasty (p = NS). Angioplastyreduced the left iliac narrowing in all animals studied. Morphometric analysis of histologic sections ofthe left and right iliac arteries disclosed significant differences in luminal and total vessel areas (p <.05), whereas arterial wall (intima and media) areas were similar (p = NS). Dilated areas oftendemonstrated marked intimal splitting with dissection into the media. At higher magnification, loss ofnuclear staining and dense layers of extracellular matrix consistent with stretching were frequentlyseen. It is concluded that the major mechanism of successful transluminal angioplasty is stretching ofthe vessel, resulting in localized aneurysm formation. Intimal splitting implies inelasticity of theneointima. No evidence of compression and remodeling of atheromatous material was disclosed in thisstudy.Circulation 68, No. 5, 1136-1140, 1983.
THE MECHANISM by which transluminal angio-plasty dilates obstructive atherosclerotic lesions is notcompletely understood. Originally, it was proposedthat the procedure remodeled the atheromatous materi-al in the arterial wall by compressing it into a smallervolume,' with release of its fluid constituents.4 Morerecently, human postmortem57 and in vivo animalstudies7'-0 investigating the histopathologic effects oftransluminal angioplasty suggest an alternative mecha-nism of intimal splitting, dissection, and stretchingrather than compression. In the present study, quanti-tative analysis of morphologic sections of pressure-
perfused dilated and control segments of rabbit iliacatherosclerotic lesions are compared to determinewhether compression of the lesion or formation of an-
eurysm represents the mechanism of successful angio-plasty.
From the Section of Cardiology, Evans Memorial Department ofClinical Research, and Department of Medicine, University Hospitaland Boston University Medical Center, Boston.
Support in part by NIH grant 1 ROLNL27512-01.Address for correspondence: Timothy A. Sanborn, M.D., Section of
Cardiology, University Hospital, 75 East Newton St., Boston, MA02118.
Received Jan. 13, 1983; revision accepted July 28, 1983.
1136
MethodsExperimental preparation and design. Atherosclerosis
was induced in the aorta and iliac arteries (left and right) ofseven 3 kg male New Zealand white rabbits. After thiopentalanesthesia, a No. 3F Fogarty catheter was passed retrogradethrough the left and right femoral artery to 20 cm, inflated toocclude the vessel, and slowly removed as described by Baum-gartner.'I Denudation of the aortic and iliac endothelia wasensured by passing the Fogarty balloon twice to 20 cm. Allanimals were subsequently placed on a 2% cholesterol dietmixed with 10% peanut oil for 6 weeks. Previous studies haveshown the development of significant diffuse iliac atherosclero-sis in animals placed on this atherogenic diet for this period.9' 10
Both iliac arteries were denuded in a similar manner to ensurethat angiographic and morphometric comparisons could bemade between the dilated (left) and nondilated (right) iliac arter-ies. After 6 weeks of the atherogenic diet, the animals wereanesthetized with thiopental and a No. 5F Swan-Ganz catheterwas inserted through the right carotid artery and advanced to theaortic bifurcation. Cineangiography was performed with 3 ml ofmeglumine diatrizoate (Renografin) as previously described tovisualize the left and right iliac arterial lesions.99 10 From afemoral arteriotomy, a Gruentzig intraoperative transluminalan-ioplasty catheter 2.5 mm in diameter was advanced retro-grade up the left femoral artery to the site of greatest iliacstenosis, inflated three times to five atmospheres for 30 sec, andremoved.9 10 This balloon size was carefully chosen to closelyapproximate the size of the least diseased portion of the proxi-mal iliac vessel to avoid overdistention. Repeat angiographywas performed immediately after angioplasty, and care was
CIRCULATION
by guest on July 14, 2017http://circ.ahajournals.org/
Dow
nloaded from

LABORATORY INVESTIGATION-ANGlOPLASTY
taken to maintain similar position of the image intensifier forboth angiograms. A I cm grid was positioned at the spine topermit calculation of the actual luminal diameter and to providecorrection for magnification differences between films. The fol-lowing day the animals were killed and the aorta and iliacvessels were surgically removed after perfusion with formalin at80 mm Hg as previously described.'2
Angiographic, histologic, and morphometric analyses.Cineangiograms taken before and after dilation were comparedon two side-by-side Vanguard projectors by measuring luminaldiameter with calipers. A change in luminal diameter of 0.4 mm(corrected for magnification) could easily be resolved by thistechnique and was considered significant. Each angiogram wasread independently by two angiographers, and discrepancieswere resolved by a subsequent simultaneous reading.
With use of the cineangiogram to identify the anatomic loca-tion of the dilated and control stenoses, the iliac vessels wereexamined histologically. Three serial sections 0.5 cm apartwere made through the dilated segment of the left iliac artery,while three serial sections taken from the nondilated stenosis ofthe right iliac artery served as controls. Sections were stainedwith hematoxylin-eosin or Verhoff-van Gieson-elastin stain andwere reviewed by at least two investigators; a consensus readingwas made as to the histologic findings. Intimal splitting wasdefined as a radial tear through the intima, dissection was de-fined as a circumferential tear along the internal elastic mem-brane, and stretching was defined as a thinning of the wall withloss of nuclear staining.
Morphometric analysis was performed by the followingmethod: Stained histologic sections were projected onto a ZeissMOP II digital image analyzer (Carl Zeiss, New York) to allowcalculation of the cross-sectional areas of the left and right iliacarterial lumina and walls (neointima plus media as demarcatedby the external elastic lamina). Total vessel cross-sectional areawas calculated by addition of the arterial wall and lumen areas.Analysis of variance and unpaired t test were used to determinestatistical significance, and a p value <.05 was accepted assignificant.
ResultsExperimental atherosclerosis. After 6 weeks on the
atherogenic diet, all seven rabbits had angiographicand histologic evidence of marked atherosclerotic dis-ease as previously reported.9 10 Their lesions were
characterized by marked intimal thickening associatedwith large accumulations offoam cells. A section froma nondilated right iliac artery used as a control is shownin figure 1.
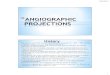
Angiography. A summary of the individual angio-graphic results before and after transluminal angio-plasty is shown for each animal in table 1. A represen-tative angiogram is displayed in figure 2. The meanluminal diameters of the left and right iliac arteriesbefore angioplasty were similar (1. I and 1.0 mm, re-spectively), indicating equal degrees of atherosclero-sis. In all seven dilated left iliac arteries a significantincrease in luminal diameter was noted after angio-plasty. The resultant mean luminal diameter was 2.3mm, which closely approximated the mean diameter ofthe more proximal segments with less marked disease(2.5 + 0.2 mm). All seven dilated left iliac arterynarrowings showed a significant increase in luminaldiameter after angioplasty. Dissection, defined as anangiographic linear density, was seen in one animal.Angiographic evidence for aneurysm formation wasseen in two animals. No evidence of extravasation ofdye, catheter perforation, or total occlusion of a vesselafter angioplasty was noted. Similar angiographic re-sults of transluminal angioplasty in this experimentalpreparation have been reported elsewhere.9 "I
Pathology. As described previously,9 10 three types ofhistologic results were seen in the dilated segments.Figure 3 is a representative example photographed atthe same magnification as the sample in figure 1.Gross splitting of the thickened intima, dissectionalong the internal elastic lamina, and thinning andbulging of the media are noted. The incidence and aqualitative assessment of the degree of neointimalsplitting, dissection along the internal elastic lamina,
FIGURE 1. Nondilated right iliac control artery.Foam cells predominate in the thickened neointimaand media. The slit along the internal elastic laminais an artifact of histologic preparation. (Originalmagnification x 50.)
Vol. 68, No. 5, November 1983 1137
by guest on July 14, 2017http://circ.ahajournals.org/
Dow
nloaded from

SANBORN et al.
TABLE 1Angiographic and histologic results
Angiographic luminal diameter (mm) Histology
Left iliac Left iliacRight iliac(control Stenosis Stenosis Nonstenotic Intimal
Rabbit segment) before TA after TA segment splitting Dissection Stretching
I 1.1 0.7 2.3 2.5 + + + + + +2 0.9 1.8 2.3 2.8 + 0 + +3 0.9 0.9 1.8 2.3 0 + 04 1.4 I.4 2.3 2.5 ++ ++ ++
5 0.9 0.9 2.3 2.3 ++ ++ +
6 1.1 1.4 1.8 2.3 + + + + +
7 0.9 0.9 2.3 2.5 ++ ++ ++
Mean 1.0 1.1 2.2 2.5SD 0.2 0.4 0.2 0.2p value NS- L .001
TA transluminal angioplasty; + local splitting, dissection, stretching; + + = marked changes; 0 no change.
and stretching are shown in table 1. None of thesechanges was noted in control segments (figure 1).Morphometric analysis of lumen, arterial wall (intimaand media), and total vessel cross-sectional areas areshown in table 2. Analysis of variance of the threesections of each dilated and control segment revealedno significant interanimal or intra-animal variance.There were significant differences in the lumen andtotal vessel cross-sectional areas between the dilatedand nondilated vessels (p < .05), while the arterialwall (intima and media) cross-sectional area was simi-lar in both groups (p = NS).
DiscussionAs originally proposed by Dotter and Judkins,' the
mechanism of transluminal dilation was attributed tocompression and local redistribution of atheromatous
material so that the atheroma functioned as a malleablesubstance. The compression of the core into a smallervolume occurs presumably by release of its fluid con-stituents.4 On the basis of histologic studies of translu-minal angioplasty in postmortem human coronary,renal, superior mesenteric, and iliac arteries, it waslater suggested that intimal splitting rather than com-pression of the atherosclerotic plaque may be themechanism of transluminal angioplasty.5 ' Indeed, invivo studies of atherosclerotic rabbit iliac arteries havedemonstrated splitting of the intimal plaque andstretching of the noninvolved portion of eccentric le-sions.7-10 In addition, histologic findings in three pa-tients who died within 3 days of transluminal angio-plasty provided additional evidence for splitting ofatherosclerotic vessels.5 Furthermore, in our recentstudy on experimental atherosclerosis,'0 release of ei-
A BFIGURE 2. Angiographic example demonstrating symmetrical disease of the left and right iliac vessels before (A), during (B),and after (C) successful angioplasty.
1138 CIRCULATION
by guest on July 14, 2017http://circ.ahajournals.org/
Dow
nloaded from

LABORATORY INVESTIGATION-ANGIOPLASTY
TABLE 2Morphometric analysis of iliac vessels
Cross-sectional areas (mm2)A
ArterialAnimal artery wall Lumen Total area
Nondilated right iliac 1.13±0.56 0.62t0.34 1.76±0.39Dilated left iliac 1.35-+O0.68 1.23±0.46 2.59-+ 0.95
p NS p < .05 p < .05
AResults are presented as mean + SD.
ther the lipid or solid contents of atheroma and emboli-zation distally was not found to represent a majormechanism of angioplasty.
In the present study, morphometric analysis of pres-sure-perfused rabbit iliac atherosclerotic vessels wasperformed to more precisely determine quantitativelywhether compression of the atheroma or stretching ofthe vessel occurred after angioplasty. The significantdifference in the luminal area between dilated and con-trol segments was expected, since angioplasty in-creased luminal diameter angiographically in all sevenanimals. Since similar degrees of atherosclerosis werepresent before dilation, the lack of a difference in arte-rial wall (intima and media) cross-sectional area indi-cates that compression of atherosclerotic material didnot occur in the animals of the present study. Rather,expansion of the vessel wall to accommodate the in-creased luminal area with localized aneurysm forma-
tion could be demonstrated both qualitatively andquantitatively. We believe that aneurysm is an appro-priate description of this vessel expansion after angio-plasty because the vessel is abnormal histologically,with the intimal splitting and a circumscribed dilationof the artery. These observations are not the result ofsampling error between individual segments, since nosignificant intra-animal or interanimal variance wasfound. In addition, since care was taken to use a bal-loon size that approximated the diameter of the leastdiseased portion of the proximal vessel, overdistensioncaused by inappropriate balloon size was avoided. Thediagram in figure 4 is a schematic representation of theproposed mechanism of angioplasty, indicating the in-timal splitting and expansion of the vessel wall withoutcompression of the atheroma.The determinants of the extent of splitting and aneu-
rysm formation remain to be established. In a prelimi-nary report in human postmortem coronary arteries,the duration of balloon inflation was found to be animportant factor in vessel diameter enlargement. 13Other factors, such as the pressure or volume of bal-loon inflation as well as the elasticity of the vesselwall, obviously play a role. If the vesssel wall is com-pliant, lumen enlargement with stretching of the vesselwall and aneurysm formation result. However, if avessel is inelastic, intimal splitting and/or dissectionmay result.
That the immediate and long-term effects of intimal
FIGURE 3. Dilated left iliac artery taken at the samemagnification as the sample in figure 1. The thick-ened neointima is fractured and separated from thestretched media, resulting in a larger lumen. (Origi-nal magnification x 50.)
Vol. 68, No. 5, November 1983 1139
by guest on July 14, 2017http://circ.ahajournals.org/
Dow
nloaded from

SANBORN et al.
FIGURE 4. Longitudinal and cross-sectional re-
views of the proposed mechanism of angioplasty.
splitting may be undesirable is implicated in a case
report of a patient dying 2 days after angioplasty. 14 Atautopsy, a fractured plaque was found with a dissect-ing hematoma almost occluding the coronary lumen.Intimal splitting with acute thrombus formation on thedisrupted arterial wall may also be the cause of acutecoronary occlusion immediately after transluminal an-
gioplasty, as evident in a report of three cases-of recan-alization of total occlusion after angioplasty with strep-tokinase. 15 The frequency of deleterious effectssecondary to intimal splitting remains to be deter-mined.
In summary, in an experimental preparation ofatherosclerosis, morphometric analysis disclosed thatdilated iliac arterial segments had significantly largerlumen and total vessel areas without a difference in thearterial wall area (intima and media) when comparedwith the nondilated iliac vessels. Thus aneurysm for-mation rather than compression and release of debrisappears to be the mechanism of transluminal angio-
plasty. Further studies are necessary to examine whatfactors provide the best possible results. Factors suchas duration of balloon inflation, pressure, and volumeas well as intrinsic vessel wall elasticity need furtherinvestigation to gain a better understanding of theircontributions to successful angioplasty.
References1. Dotter CT, Judkins MP: Transluminal treatment of atherosclerotic
obstruction. Circulation 30: 654, 19642. Leu HJ, Gruentzig A: Histopathologic aspects of transluminal re-
canalization. In Zeitler E, Gruentzig A, Schoop A, editors: Percu-
taneous vascular recanalization. Berlin, 1978, Springer-Verlag, p39
3. Lee G, Ikeda RM, Joye JA, Bogren HG, DeMaria AN, Mason DT:Evaluation of transluminal angioplasty of chronic coronary arterystenosis: value and limitations assessed in fresh human cadaverhearts. Circulation 61: 77, 1980
4. Dotter CT, Judkins MP: Transluminal dilation of atheroscleroticstenosis. Surg Gynecol Obstet 127: 794, 1968
5. Block PC, Myler RK, Stertzer S, Fallon JT: Morphology aftertransluminal angioplasty in human beings. N Engl J Med 305: 382,1981
6. Baughman KL, Pasternak RC, Fallon JT, Block PC: Transluminalcoronary angioplasty of postmortem human hearts. Am J Cardiol48: 1044, 1981
7. Castaneda-Zuniga WR, Formanek A, Tadavarthy M, Vlodaver Z,Edwards JE, Zollikofer C, Amplatz K: The mechanisms of balloonangioplasty. Diagn Radiol 135: 565, 1980
8. Block PC, Baughman KL, Pasternak RC, Fallon JT: Transluminalangioplasty: correlation of morphologic and angiographic findingsin an experimental model. Circulation 61: 778, 1980
9. Faxon DP, Weber VJ, Haudenschild C, Gottsman SB, McGovernWA, Ryan TJ: Acute effects of transluminal angioplasty in threeexperimental models of atherosclerosis. Arteriosclerosis 2: 125,1982
10. Sanborn TA, Faxon DP, Waugh D, Small DM, Haudenschild C,Gottsman SB, Ryan TJ: Transluminal angioplasty in experimentalatherosclerosis: analysis for embolization using an in vivo perfu-sion system. Circulation 66: 917, 1982
11. Baumgartner HR: The role of blood flow in platelet adhesion,fibrin deposition, and formation of mural thrombi. Microvasc Res5: 167, 1973
12. Haudenschild C, Baumgartner AR, Studer A: Significance of fix-ation procedure for preservation of arteries. Experientia (Basel) 28:828, 1972
13. Kaltenbach M, Koher G: Can prolonged application of pressureimprove the results of coronary angioplasty (TCA)? Circulation 66(supp 11): 11-123, 1982
14. Wood WG: Transluminal coronary angioplasty. N Engl J Med 306:1055, 1982
15. Schofer J, Krebber HJ, Bleifeld W, Mathey DG: Acute coronaryartery occlusion during percutaneous transluminal coronary angio-plasty: reopening by intracoronary streptokinase before emergencycoronary artery surgery to prevent myocardial infarction. Circula-tion 66: 1325, 1982
CIRCULATION
(rS 4I
1140
by guest on July 14, 2017http://circ.ahajournals.org/
Dow
nloaded from

T A Sanborn, D P Faxon, C Haudenschild, S B Gottsman and T J Ryanexperimental atherosclerosis.
The mechanism of transluminal angioplasty: evidence for formation of aneurysms in
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1983 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.68.5.1136
1983;68:1136-1140Circulation.
http://circ.ahajournals.org/content/68/5/1136the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on July 14, 2017http://circ.ahajournals.org/
Dow
nloaded from