Embed Size (px)
Citation preview

1084
intelligence, energy, and organisation on the part ofadministrators. Unfortunately these qualities arenot always forthcoming, and administration oftenlags years behind the dictates of science. Although15 years have elapsed since many of the factswhich I have described were discovered, I thinkthat I may say after constant study of the subjectand with all due consideration that mankind hashitherto not effected more than about one-tenth ofthe improvement of health which it might haveeffected already if it had put its heart into thebusiness. When I had completed my work in 1899I had fondly dreamed that a few years wouldsee the almost complete banishment of malariafrom the principal towns and cities in the
tropics-that those benign climates and thosebeautiful scenes would be almost rid at onceof a scourge which had blighted them from timeimmemorial. In this I have been disappointed.True, much has been done in certain places, as inPanama, Ismailia, Italy, West Africa, and parts ofIndia and the Malay States, and in some other
spots; but much more might have been done hadwe remained fully alive to our opportunities-andour duties. It is not the fault of science that wedo not fully utilise the gifts which she gives tous. None of us here will live to see the fullfruition of these gifts in this particular case ; butwe have at least seen the beginning and maybelieve that our children will reap the profit.But it is ever thus with science. Her slaves are
like labourers condemned to drive tunnels throughmountains-working, perhaps for years, in darknessand oppressed by the immense spissitudes of natureabove them, but always encouraged by the hopethat at any moment they may emerge into the sun-light and upon the vision of a new world. May Iconclude, as appropriate to the subject of thisaddress, with four lines which were written years agoby one who was then toiling at the researches heredescribed and in the darkness of the most utterfailure-at work, moreover, for which he had littleliking or ambition. They may encourage otherswho are now in a like case. Writing generally ofthe sublime spirit of inquiry he said :-
Thee most we honour, theeGreat Science. Hold thy way.
The end thou canst not see ;Bitt ia the end, the day.
CENTRAL MIDIVI17Es BOARD.-A special meetingof the Central Midwives Board was held at Caxton House,Westminster, on Oct. 22nd, Sir Francis H. Champneys beingin the chair. A number of midwives were struck off theroll, the following charges amongst others having been
brought forward. The patient suffering from attacks of
faintness, from rupture of the perineum, and the placentaand membranes not having been expelled within two hoursof the confinement, the midwife did not explain that thecase was one in which the attendance of a registeredmedical practitioner was required, nor did she hand to thehusband or the nearest relative or friend present the formof sending for medical help, properly filled up and signed byher, in order that this might be immediately forwarded tothe medical practitioner, as required by Rule E. 19. Themidwife being unable to make use of a clinical thermometeror to take the pulse of her patients, consequently cannotcomply with Rule E. 13. Neglect to employ the antisepticprecautions required by Rules E. 3 and 7, to wash the
patient as required by Rule E. 7, and neglect to take thepulse or temperature of the patient as required by Rules. 13.Discontinuing attendance at a time when the patient wasill and suffering. Not being scrupulously clean in person,clothing, house, and appliances as required by Rule E. 1 ;not keeping the register of cases as required by Rule E. 23.Medical aid having been sought for the patient, the midwifeneglected to send any notification thereof to the local super-vising authority, as required by Rule E. 21 (1) (a).
THE WOUNDED IN THE WAR: SOMESURGICAL LESSONS.
BY D’ARCY POWER, M.B. OXON., F.R.C.S. ENG.,SURGEON TO ST. BARTHOLOMEW’S HOSPITAL; LIEUTENANT-COLONEL
R.A.M.C. (T.F.), ATTACHED TO THE 1ST LONDON GENERAL HOSPITAL.
IT is still too early to generalise upon the surgicalmethods needed by those wounded in the presentwar. It may, however, prove useful to present a.
few of the results which have been observed in abase hospital in London. As might have beenexpected, the final results of wounds were seenbefore the earlier ones, because at first the injuredremained in the stationary hospitals until they werewell enough to travel. Now that these hospitals.are full, and the fighting is often nearer Englandthan the Allies’ bases, the type of wound is becom-ing more serious. Taking the cases in this reverseorder, then, we learnt at first that bullets, and evenpieces of shrapnel casing, often passed throughfleshy parts without doing much damage. The-points of entry and of exit were clearly seen.
Both had healed satisfactorily, and nothingremained to be done except to feed andnurse the patient for a few days before hewas discharged into a convalescent home. Inother cases the wounds of entry and exit weresuppurating, but the track which must haveexisted between the two was soundly healed. No-sinus remained, and so far it has not been neces-
sary to lay open any such track. It seems clear,therefore, that the most frequent sources of infec-tion are the skin of the patient or some subsequentcontamination. It is certainly not due to the
clothing, for in several cases pieces of shirt or putteewere removed from wounds which had healed
soundly and which had been reopened on accountof the pain they had caused. The positions of the-wounds of entrance and exit showed in many cases.that the path taken by the projectile had beenextraordinarily devious, and that the deviation was.not accounted for by the presence of any moreresistant structure such as bone.
Cases with Foreign Bodies in sitze.The wounds which were still open when the-
patient reached England were all submitted to-
radiographic examination on the assumption thatthe foreign body causing them was in situ, and)in the majority of cases this was found to becorrect. It was soon learnt, however, that there-was a vast difference between the location of theprojectile and its removal. The radiograph showedits presence, but it was often extremely difficult.and might be impossible to find it. The patient,therefore, was told that the wound would be-
explored, not that the projectile would be extracted.The difficulty lies in the fact that the patients arestrong muscular men, and that the shadowonly gives an approximate idea of the position;and depth of the projectile. It is of the utmost.importance therefore that the apparatus as wellas the X ray operator should be of first-ratequality. Very little constitutional disturbance was.produced, even when the projectile had beenin position for three or four weeks, and there-was none of the tracking or burrowing ofsuppurating sinuses which might have been ex-
pected. Pieces of the clothing, either in shreds ortorn into filaments, were found distally in nearlyevery case. They had to be looked for, as theywere often separated by a bridge of healthy tissue.In some cases where the skiagram showed that

1085
the bullet had been extensively comminuted andnumerous fragments were distributed widely inthe tissues it was thought better to leave themuntouched if they were not causing any trouble.In like manner no extensive operations were
undertaken to remove foreign bodies fromthe chest. By the time the patients arrivedin England the wounds had healed-apparentlywithout suppuration. When one side of thechest contained fluid it was treated as an
empyema by drawing off the blood-stained serousexudation, a portion of rib being removed anddrainage employed if the temperature rose or thepleural cavity refilled. It was noticed that mostof the operations undertaken for the removal ofbullets suppurated for a few days but never
dangerously. The operations were performed withthe usual precautions and were nursed in the wardsby fully trained hospital nurses, so that the suppura-tion was not attributable to any failure of surgicalor nursing technique. It was soon consideredadvisable, therefore, to isolate patients requiringsuch " clean " operations as removal of torninternal semilunar cartilages and after this pre-caution these cases uniformly did well. Amputationsat this period were rare and there were no deaths.
Severer Cases.-" nerve Concussion."The cases have become more severe as the
battles were fought nearer England. Gangrene dueto an anaerobic organism has occurred in severalcases. Early operation has been performed withsuccess, and the very great value of a free applica-tion of a 2t to 3 per cent. solution of iodinein rectified spirit has been determined. It shouldbe applied to the raw surface of the flaps atthe time of amputation, and care should be takento allow of free drainage by not putting in too many ,,sutures. A few cases of tetanus with a long incuba-tion period have occurred, but the majority of thepatients affected with this terrible disease have notcome under our care, as they have been treated atthe stationary hospitals.
It is almost a matter of common knowledge thatthe size of the skin wound bears no relation to the
severity of the injury. The lower jaw in one casewas found to be so comminuted that it had to beremoved with a Volkmann’s spoon, yet the skinwound hardly admitted a probe, and the patientmerely said that he thought his jaw was broken intwo places. It is necessary, therefore, to make adetailed examination in every case-under an anaes-thetic when possible, and with the necessary pre-paration for an immediate and adequate operation.The war, too, has revealed an interesting
series of cases which for the present mustbe called " nerve concussion," about the treat-ment and prognosis of which much has still tobe learnt. When they occur in connexion withthe spinal cord they may be the result of a blowfrom a bullet or piece of shell perhaps no nearer thanupon the pack which the soldier is carrying. Thereis no external wound, but the patient becomesparaplegic. Such a condition is analogous to
"
rail-way spine," though it is not associated with neuras-thenia at least in the early stages which have comeunder observation at the present time. A similarcondition of paralysis without any gross injury hasbeen noticed in the arms and legs apparently due tointerference with the function of one or more
nerve trunks, since exposure of the nerve does notshow that it has been anatomically damaged. It istoo soon yet to state whether recovery of func-tion is the rule or the exception in these cases.
The mental state of the patient makes nodifference to the rate of recovery. The Englishsoldier, who is naturally sanguine, heals quicklyin spite of suppuration; the Belgian is not farbehind, though he is a prey to anxiety, because hegrieves for his country, has lost sight of hisrelatives, and is in hospital in a foreign thoughfriendly land. Like a brave fellow he bears himselfin sickness as he does in health with magnificentcourage.
Surgical Methods.The net result of the work appears to show that
as in ordinary civil practice meddlesome surgery isgenerally bad surgery. Wounds need no longer beprobed, drained, and packed. Tempered with dis-cretion, it is better to wait than to operate unlessthe patient is losing ground. Considerable experi-ence, however, is required to decide when to waitand when to operate, because injuries whichappear slight superficially may conceal conditionsthat demand immediate treatment. Looking to thefact that the chief infection seems to come from thepatient’s own skin, there can be no doubt that anti-septic surgery is preferable to aseptic methods.Dry dressings must give place to compresses andfomentations wherever possible. Iodine applica-tions seem to be more effective than the solutionsof perchloride and biniodide of mercury which havebeen hitherto the more generally used. The youthand health of the patients render the prognosiseven of severe injuries correspondingly good andenable the surgeon to take waiting risks whichmight otherwise be thought hazardous. It is better,therefore, to err on the conservative rather than onthe radical side of surgery; at any rate, in theearlier stages.Chandos-street, W.
____ ______
THE INTRATRACHEAL ADMINISTRATIONOF CHLOROFORM.
BY W. DAKIN MART, B.A. CANTAB., M.R.C.S. ENG.,L.R.C.P. LOND.,
ANÆSTHETIST TO THE NOSE, EAR, AND THROAT DEPARTMENT, ROYALINFIRMARY, SHEFFIELD.
ONE hears nowadays a great deal concerning theintratracheal administration of ether and very littleconcerning the intratracheal administration ofchloroform. I have of late administered chloro-form by this method in operations on the nose andthroat performed by Mr. W. S. Kerr, honorarysurgeon to the Nose, Ear, and Throat Departmentof the Royal Infirmary, Sheffield, who has expressedhis satisfaction with the method.
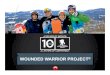
Diagram of apparatus for intratracheal administration ofchloroform. A, B. c. Taps. D, Extra opening in catheter.E, Metal collar. F, Long rubber tube (represented broken)to catheter. G, Rubber tube from Junker bellows.
The apparatus used differs from a Junker’sinhaler in that there is a cross tube connecting theentry and exit tubes. Each of these tubes carriesa tap, A, B, and c (see diagram). When A and Bare